
Phase-Changing Glauber Salt Solution for Medical Applications in the 28–32 °C Interval
by
 ,
,
Linus Olson
1,2,* ,
,
Carina Lothian
3,
Ulrika Ådén
1,
Hugo Lagercrantz
1,
Nicola J. Robertson
4 and
Fredrik Setterwall
5,† 1
Department of Women’s and Children’s Health, Karolinska Institutet, 17177 Stockholm, Sweden
2
Department of Neonatology, Vietnam National Children’s Hospital, Hanoi, Vietnam
3
Neonatal Unit, Stockholm Söder Hospital, 11883 Stockholm, Sweden
4
Institute for Women’s Health, University College London, London WC1E 6HU, UK
5
Division of Energy Processes, Chemical Engineering and Technology, Royal Institute of Technology, 10044 Stockholm, Sweden
*
Author to whom correspondence should be addressed.
†
Deseased.
Materials 2021, 14(23), 7106; https://doi.org/10.3390/ma14237106
Submission received: 5 October 2021
/
Revised: 11 November 2021
/
Accepted: 16 November 2021
/
Published: 23 November 2021
Abstract
:(1) Background: The field of medicine requires simple cooling materials. However, there is little knowledge documented about phase change materials (PCM) covering the range of 28 to 40 degrees Celsius, as needed for medical use. Induced mild hypothermia, started within 6 h after birth, is an emerging therapy for reducing death and severe disabilities in asphyxiated infants. Currently, this hypothermia is accomplished with equipment that needs a power source and a liquid supply. Neonatal cooling is more frequent in low-resource settings, where ~1 million deaths are caused by birth-asphyxia. (2) Methods: A simple and safe cooling method suitable for medical application is needed for the 28 to 37.5 °C window. (3) Results: Using empirical experiments in which the ingredients in Glauber salt were changed, we studied the effects of temperature on material in the indicated temperature range. The examination, in a controlled manner, of different mixtures of NaCl, Na2SO4 and water resulted in a better understanding of how the different mixtures act and how to compose salt solutions that can satisfy clinical cooling specifications. (4) Conclusions: Our Glauber salt solution is a clinically suited PCM in the temperature interval needed for the cooling of infants suffering from asphyxia.

1. Introduction
Phase Change Materials (PCMs) are used for energy storage [1,2,3,4], heating and cooling of buildings [5,6], optimization of different residential climates [7,8,9,10], as well as cooling of computers and other telecom equipment [11]. PCM can also be used for medical purposes [12,13], which is the focus of the present investigation. For reviews of the field and relevant inventions, see the IEA Annex 17 Final report [14] and Zalba et al. [15].
1.1. Clinical Background
Newborn infants may suffer brain damage from asphyxia and oxygen deprivation during delivery. The medical term often used for this condition is Newborn Hypoxic Ischemic Encephalopathy, nHIE. By controlled therapeutic hypothermia (cooling of the human body) to a stable temperature of 33.5 ± 0.5 °C, children at risk of nHIE have been shown to have a reduced risk of death or severe disability at 18–22 months follow-up, based on several randomized, controlled investigations [16,17,18,19], after extensive pre-studies [20,21,22]. Nevertheless, there is a need to further investigate and assess several aspects of this complex therapy [19,23,24,25], and not to cool too much [26,27], as well as to clarify how the brain responds and how the effects of cooling in combination treatments, such as addition of Xenon gas, operate [28]. A key factor influencing the therapeutic effect of hypothermia is the interval between the insult and the induction of hypothermia [20,21]. To obtain maximum benefit, postnatal hypothermia should be started as soon as possible [29,30], and within 6 h after the insult [20,29]. When treatment is started as late as after 12 h, only limited effects should be expected. A meta-analysis stresses the need for further studies, and specifically points to the need to study earlier initiation of hypothermia [23,24]. Conventional cooling to prevent nHIE is based on circulating cool water and requires electricity. To allow fast initiation of cooling, e.g., during transport of patients, as well as to provide a system that is independent of both water and electricity, PCMs have been considered. PCMs melt within given temperature ranges, and are used, for example, for thermal energy storage [1,2,31,32].
1.2. PCM Background
Thermal energy can be stored in multiple ways. In PCM, the latent heat of the material is used [5]. Each time a material changes phase between solid, liquid and gas, heat is disseminated or taken up. Ice constitutes a simple form of PCM, used since the beginning of modern history [33]. Its PCM characteristics can be exemplified by the fact that the amount of energy needed to melt 1 kg of ice is 80 times larger than the energy needed to increase the temperature of the same amount of ice by 1 degree [31]. However, ice undergoes its phase change at a temperature that is unsuitable for the cooling of infants. Other more commonly used PCMs are often based on waxes (fatty acid and ester or paraffins, such as octadecane), eutectic salt mixtures, and salt hydrates. Figure 1. PCMs for our purpose should have phase change temperatures that allow them to be used to cool babies via direct skin contact, and should also be rechargeable (i.e., re-frozen) at room temperature. Advantages of PCMs include the ability to maintain a constant temperature during the phase change, thus minimizing fluctuations and providing better stability in the energy exchange process. PCMs also have a high energy storage density, making them ideal for objects that need to be constantly cooled or heated for a prolonged period by energy removal or delivery, respectively.
Progress in absorption systems (a subset of systems for heating and cooling of buildings) has included peak temperature shaving of systems that generate too much heat or cold during limited time periods. In recent decades, there have been evolutions in the research field, including passive cooling of buildings [13,15], energy saving methods, absorption systems (a subset of heating and cooling buildings). One way to solve this problem is to microencapsulate PCMs, allowing the mixing of PCMs with other materials or the flux of PCMs [34,35,36]. In addition to common buildings, potential uses for PCMs include heating and cooling of greenhouses to adjust climate and improve production, the multiple needs for heating and cooling in the medical world, transportation and conservation storage containers, and in computers and other telecom equipment [10].
The energy density in sensible heat storage materials is given by the temperature range and the heat capacity of the storage material [37]. The temperature range depends on the application at hand, and is limited by the temperature of the storage material as well as the temperature of the heat source, in our case the infant. The energy density, in our case the capacity to remove heat from a newborn baby, is highest when using a PCM with a phase change temperature similar to the desired cooling temperature [15,38,39,40].
Within a given temperature interval ∇T = T2−T1, the sensible and latent stored heat Qlat can be calculated as:
where Hls is the heat of the fusion at the phase change temperature Tls.
Qlat = T1∫T2 cp × dT + Hls
The attainable temperature difference ∇T is dependent on the charging temperature Tc, given by the heat source. Depending upon whether the temperature of the energy source is higher or lower than the ambient temperature, the storage material will work as a heat or a cold sink. This means that insulation of the storage is needed to protect the storage material from losses over time. Preliminary results of studies were presented at the Annex 17 meetings, and a summary is found in the IEA final report, as well as in [14]. The general idea behind the current paper was first presented at the IEATA conference in 2004 in Arvika, Sweden [38]. Preliminary studies were performed in China and Turkey [41], and preliminary medical conclusions were drawn in Stockholm, Sweden on the basis of animal experiments [39].
1.3. Experimental Background
The PCMs intended for our purposes are solid at room temperature; when in contact with a warmer object, these PCMs absorb and store heat, ultimately liquefying. Conversely, liquid PCMs can solidify when giving off heat, thus working as heat buffers and stabilizing the temperature of objects in contact with them. The objective of this study was to evaluate different mixtures of Glauber salt (named after Johann Rudolf Glauber, who discovered it in 1625), in order to develop a mixture with a temperature range of 28–32 °C that is suitable for the medical field. The material should also be such that no outside force would be needed to start or stop the energy transfer process between the PCM and the object to be cooled or heated. It should also be independent of electric power and water in terms of reversing the phase transition.
2. Materials and Methods
For medical uses, the studied PCMs should meet a list of 10 important criteria, described in Table 1.
These criteria eliminate all highly toxic materials, as well as compounds with very slow energy transfer characteristics or very low energy storage capacity. Based on these criteria, and discussions with expertise in material physics from the Royal Institute of Technology in Stockholm, we selected Glauber salt in different forms for further study. In reaching this decision, we took into account the mixture-processing expertise available to our project through PCM producers TST AB Sweden and its subsidiary, Climator AB (a PCM producer in Sweden) and Rubitherm. A shared knowledge protocol was established, which included the intention to produce test amounts of suitable PCMs for medical use.
We used a T-History-like method [42,43] to evaluate the findings. To generate the different materials, we used the well-known Glauber salt Na2SO4 10H2O, which has a phase change temperature point of 32 °C, and mixed it with NaCl, in an attempt to change the temperature stabilization point and produce PCM that would have a lower set point, e.g., at 30 °C. For equipment see Appendix A.
The mixtures were constructed as follows: a well-defined amount of Na2SO4, 10.33 g, was first measured. Next, NaCl was added. The salt combination was then mixed with water to obtain the desired NaCl and Na2SO4 mixtures. The amount of NaCl was varied so that, on a dry weight basis, the percentage of NaCl was between 1.5 and 7% in 0.5% increments. The solution was stirred while being heated until all salts were completely dissolved. To stabilize the solution and make it more convenient to handle in future commercial applications, 1–5 g of cethyl methyl cellulose (CMC) was added as a gelifier agent. The CMC also allowed different salt hydride products to bind different amounts of water, during different stages of the phase change to avoid separation due to gravity. Likewise, the presence of CMC was also expected to keep the NaCl better distributed within the solution. The complete solution was then poured into glass test tubes for experimental usage. The temperatures of the glass tubes were monitored (DacPad, National Instruments, Austin, TX, USA) using temperature probes placed in the middle of the test solutions in the glass tubes and connected to a data logger. The glass test tubes were repeatedly cooled and heated using a water bath (Lauda RE106 with heater, The Lab World Group, Hudson, MA, USA) /cooler Lauda E100, (The Lab World Group, Hudson, MA, USA). The temperature signals were stored and monitored using a computer with appropriate software (Medical Cooling, Labview, version 8.2) (configured using Labview). The system allowed temperature control, control of sampling rates (time between measurements), and the use of up to four input channels. A monitor was used to display temperature curves in real time, to help evaluate the results and to aid storage of results. The four different channels were used to measure glass test tubes with contents as follows: channel 1: jellified water (control); channel 2: water; channel 3: experimental PCM mixture of interest; channel 4: known PCM mixture for calibration of the experiment. The experimental setup with test tubes in a water bath is schematically shown in Figure 2.
For each mixture we heated the glass test tubes (10 mL) in a water bath to 45 °C and then lowered them to 5 °C and then cycled this procedure at least 3 times. This strategy was used to ensure the elimination of any problems of non-homogeneous mixtures and the risks of crystallization irregularities of different mixtures such as the presence of Na2SO4 7H2O instead of Na2SO4 10H2O, and other faults that might compromise reproducibility. Because of the relatively fast temperature changes of the water bath, we added semitransparent insulation sheets around the test tubes to slow down the temperature change process of the PCM somewhat. This also helped prevent glass tubes closer to the heat source from heating up faster than tubes further away.
3. Results
Adding different amounts of NaCl was found to modify the melting temperature of the test solutions (Figure 3). From a melting point of 32 °C in the absence of NaCl, additions of up to 5% NaCl decreased the melting point of the mixture to about 25 °C, while further additions of NaCl had little effect on the melting point. We visualized the samples melting points, dissolution/crystallization point as well as usage of the T-history over time in figure after the first two runs (to avoid initial mixing interfering with results).
The salt solutions have temperature change curves that differ from the water curve when warmed up to about 28 °C, and that flattens out briefly around 30–32 °C, depending on the mixture. This flattening occurs when the salt takes up energy from the surroundings before being heated again as expected. This is illustrated in the first part of the curves in Figure 4. When being cooled, the different materials were less diverse, but even here a small variation in the slope of the curves could be noted, as seen in the right part of Figure 4. In mixtures with a small percentage of NaCl, there was a risk for crystallization with 7 instead of the intended 10 H2O molecules. When temperatures were lowered to 5°, this caused a temporary rise of temperature to 10 or 12 °C instead of a smooth curve (here seen as a peek in Figure 4 in the very end). The salt then acted in a non-regulated way until the solution was heated up again. All curves can be plotted into a phase–temperature diagram for water NaCl Na2SO4 mixture. Such a diagram is shown in Figure 5.
Our results in the area of 0–10% NaCl in a solution of 30% Na2SO4 (5g Na2SO4, H2O, 0.833 g CMC) confirm previously published phase diagrams for temperature vs. salt composition (Figure 5b (25 °C)). We allowed a 0.2–0.3-degree tolerance between measurements, because the reliability of the water bath servo control was ±0.2 °C, and in order to cope with other forms of variability, such as forms of crystallization. If a particular salt solution is dissolved with a 7- instead of 10-crystal water configuration, the next cycle will be affected. Additionally, our sample rate was set to every 10 s (to keep data files manageable). Therefore, curves shown in the figures may not reveal small variations occurring between temperature measurements and cycles. Comparing our data to Figure 6, our curve does not appear to fit the published diagram so well. This is due to our curve seeming to plateau, but as indicated in the curve drawn on top, the curve actually continues descending when higher amounts of NaCl is mixed into the solution. This is known, because other mixtures on the market for Glauber salt contains more NaCl, e.g., ClimSelC 21 from Climator. The faulty point at 2% might be due to a faulty probe, but since the curve is not a straight line superimposing the different diagrams from Figure 6, as well as other similar curves, suggests our double bent one might have hit a low point in our measurements. By altering the amount of CMC within limits of 3 to 8%, it was possible to alter the viscosity of the gel. However, as long as the difference in concentration between the two salts did not change, the behavior of the curve did not change much. Thus, depending on the specifications for a certain application, one can alter viscosity to adapt to specific needs. However, if the thickness of the gel is altered too much, PCM compositions with low amounts of NaCl might become inhomogeneous, leading to different behavior in different compartments.
4. Discussion
The investigation of different mixtures of NaCl, Na2SO4 and water in a controlled way resulted in a better understanding of how these different mixtures act in terms of phase change characteristics when subjected to rising and falling temperatures. This has made it possible for us to identify a particular composition of salts that can be reproduced to fulfill the specifications of medical needs.
The risk of small particles interfering with the procedure and material properties is higher when the mixture contains smaller amounts of NaCl in the solution. The risk of the anhydrite solution was avoided in our experiments by positioning our mixture of interest to the left of the normal Glauber salt mixture seen in the concentration–weight fraction of the Na2SO4 diagram (Figure 6).
The anhydrite could have caused problems, since variation of NaCl content would then be of less importance in the behavior of the mixture in our temperature interval. Using 30% Na2SO4 as the base for our mixture, we were able to avoid sodium sulfate deposition, which could otherwise cause additional problems at all stages. Any deposition precipitate in the mixture would act as a foreign particle, which would increase the risk of crystallization at temperatures other than the desired ones, as well as altered amounts of different chemicals in the mixture, available to react as planned in the remaining solution. An uncontrolled process could lead to more or less cooling, and to more or less deposition, further adding to an unstable situation. Some of this has been described, and solutions have been suggested, by Mehling and Cabeza [44]. One way to solve this problem is to microencapsulate PCM, allowing the mixing of PCM with other materials or flux of PCM. However, we mixed Na2SO4, NaCl and CMC to find new materials in our desired temperature range; findings that have not previously been reported.
Clinically, controlled cooling with circulating water has become a standard treatment of newborn infants at risk of brain damage due to oxygen deprivation. Accumulating clinical experience with excessively cooled children or infants suggests that prolonged periods with unstable temperatures may aggravate brain damage. [18,19,26]. In infants in need of cooling, rectal temperatures may vary from 31 to 38 °C during the initial day of treatment, due to intrinsic temperature regulation mechanisms and environmental factors. These factors may continue to cause fluctuations in temperature that might hamper the final effect of the hypothermia, and therefore, a stable temperature should be maintained throughout the treatment period. On the basis of animal work, it is also known that rewarming too rapidly might have negative effects on neurological outcome. It is, therefore, a significant advantage that PCM mattresses avoid these extreme variations, and that the target temperature remains stable during the entire cooling period. In animal experiments, we have demonstrated that PCM acts like an energy buffer, leading to fewer temperature fluctuations, and hence a more stable temperature, since our salt hybrid gives energy back to the animal when the temperature is too low and absorbs energy when the temperature is above the phase change temperature [45]. Our experimental use of PCM mattresses (Figure 7 and Figure 8) is supported by another advantage of using PCMs for cooling: the inability of a temperature undershoot occurring during the intended cooling period, eliminating such problems originating from human error when manually regulating the temperature of the cooling.
Medical use of the knowledge obtained in this study could help avoid unstable temperatures, which cause harm (swing of temperatures has been known to counteract the hypothermia) [46], and can cool down or obtain temperatures in a simple way, also making it useful for the transport of patients to hospitals, where treatment can be continued. It can also help when starting treatment of newborns at risk of hypoxic ischemic encephalopathy or asphyxia within the 6 h treatment start window in order to prevent brain or organ injuries in remote places [47]. A mattress with PCM does not require an electricity source or water during transport to a high-level centers where newborns can be treated in the same way as the standard state of treatment in western societies.
The material knowledge can also be used to keep patients of different ages within a normal temperature interval in areas with high outside temperatures, highly variable temperatures, or during transport, as well as together with textiles with encapsulated PCM [48,49,50]. These textiles can then be used in blankets or for the staff to maintain normothermia during transport in warm countries.
Further studies into the use of PCM may lead to applications in different medical disciplines, as well as for the transport of samples or isolates (human, animal and environment samples/isolates), including bacteria and virus samples, blood samples, vaccines, etc. [51]. A Glauber solution seems to be a promising way forward for medical use.
5. Conclusions
A PCM solution, in our case a Glauber salt solution, can function as a medically well-suited phase change material in the temperature interval needed for cooling of infants suffering from oxygen deprivation during birth or within 6 h. Such a Glauber salt mixture should keep the set rectal temperature of the infant at 33–34 ± 0.5 °C. We confirmed and tested different amounts of NaCl added to the Glauber salt mixture and found that by altering the percentage we could construct PCMs for all the specified temperatures in the interval of 20–32 °C. By using only 30% instead of the normal amount of Glauber salt (Na2SO4 × 10 H2O) as our starting material, we could avoid problems caused by sulfate anhydrites as well as precipitates in the solution. In this way, we also obtained a more liquid mixture in which all components involved could be better mixed before adding CMC. We were thus able to study the involvement of different amounts of NaCl better than if we would have chosen a higher relative amount of Na2SO4. Based on the present results, we are confident that optimal mixtures can be developed for cooling and heating purposes, not the least in the medical field.
From a medical point of view, we were interested in the development of technically simple solutions to the problem of brain cooling, applicable in remote sites and countries lacking advanced medical resources [46,52,53]. Such a solution should allow treatment soon after birth and improve the possibility of already starting safe cooling during transportation. A single mattress can be used repeatedly at least 50 times. Clinical use of the knowledge in this article led us to produce a mattress in Sweden and use a PCM mattress in Vietnam and Sweden. This also tests whether the knowledge obtained about PCM worked as expected in a climate where higher temperatures are occurring than in Europe, and larger temperature swings exist. The mattress was used and seemed to work as well as or better than other methods for hypothermia treatment of children with HIE [47]. Additionally, globally, e.g., in India, PCM mattresses have been successfully used even though there were problems when temperatures went over 33 °C [52,54,55,56]. The general conclusion is that PCMs are very useful for medical applications both in high- and in low–middle-income settings, in hospitals and during transportation, and can be used if the material is constructed correctly for the intended temperature or temperature interval in many situations where steady controlled cooling is needed.
Author Contributions
Conceptualization, L.O., C.L. and F.S.; methodology, L.O., C.L. and F.S; software, L.O. and F.S.; validation, L.O. and N.J.R.; formal analysis, F.S.; investigation, L.O. and F.S; resources, C.L.; data curation, L.O.; writing—original draft preparation, L.O.; writing—review and editing, L.O., C.L., U.Å., H.L., N.J.R. and F.S.; visualization, L.O. and N.J.R.; supervision, U.Å., H.L. and F.S.; project administration, H.L. and F.S.; funding acquisition, L.O., U.Å., H.L. and N.J.R. All authors have read and agreed to the published version of the manuscript.
Funding
The study’s medical part was funded by The Swedish and British Medical Research Council, Stiftelsen Barncentrum and Air products. The rest of the study was supported in part by generous grants from Vinnova and by in-kind time, by the different authors from Karolinska Institutet and University College London.
Institutional Review Board Statement
Not applicable. (The study only concerns materials and all references to other independent studies has their own ethical permits but was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Boards where they take or took place).
Informed Consent Statement
Informed written consent was obtained from all subjects involved in the photos. No patient data is used or presented in this article (since that is an independent follow up studies, with its own ethical permits) so no other informed consent has been needed.
Data Availability Statement
All study data can be asked for by the Corresponding Author.
Acknowledgments
We would like to thank: Viktoria Martin at KTH for her support. Climator AB for supplying us with important technical data for cooling, and especially Rolf Ulvengren * who supported our project and suggested improvements in the start. The authors thank TST and Medical Cooling Sweden for supplying the PCM mattress used in this study. * Deceased.
Conflicts of Interest
Linus Olson, Carina Lothian and Fredrik Setterwall were shareholders in Medical Cooling Sweden AB. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Appendix A
Equipment Used
| Heated bath | Lauda RE106 with heater/cooler Lauda E100 |
| Computer | Fujitsu-Siemens Scaleo L with software: National Instrument Labview 8.2 |
| Dacpad | NI SC-2345 with termoprobes T100 elements K-Coupled |
| Scale | Presica BJ210C |
| Salt: NaCl | Falksalt, >99% without Ion-supplement |
| Na2SO4 | Merck, Sodium Sulfate Lot Ta518349843 |
| Water | Regular tap water. |
| Stirring rod | Bamboo rod |
| Mixing bowl | Plastic food cup |
References
- El-Sebaii, A.A.; Al-Ghamdi, A.A.; Al-Hazmi, F.S.; Faidah, A.S. Thermal performance of a single basin solar still with PCM as a storage medium. Appl. Energy 2009, 86, 1187–1195. [Google Scholar] [CrossRef]
- Joulin, A.; Younsi, Z.; Zalewski, L.; Lassue, S.; Rousse, D.R.; Cavrot, J.-P. Experimental and numerical investigation of a phase change material: Thermal-energy storage and release. Appl. Energy 2011, 88, 2454–2462. [Google Scholar] [CrossRef]
- Martin, V.; He, B.; Setterwall, F. Direct contact PCM-water cold storage. Appl. Energy 2010, 87, 2652–2659. [Google Scholar] [CrossRef]
- Wang, W.; Yang, X.; Fang, Y.; Ding, J.; Yan, J. Preparation and thermal properties of polyethylene glycol/expanded graphite blends for energy storage. Appl. Energy 2009, 86, 1479–1483. [Google Scholar] [CrossRef]
- Medrano, M.; Yilmaz, M.O.; Nogues, M.; Martorell, I.; Roca, J.; Cabeza, L.F. Experimental evaluation of commercial heat exchangers for use as PCM thermal storage systems. Appl. Energy 2009, 86, 2047–2055. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, Y.; Xiao, W.; Zeng, R.; Zhang, Q.; Di, H. Review on thermal performance of phase change energy storage building envelope. Chin. Sci. Bull. 2009, 54, 920–928. [Google Scholar] [CrossRef] [Green Version]
- Borreguero, A.M.; Sanchez, M.L.; Valverde, J.L.; Carmona, M.; Rodriguez, J.F. Thermal testing and numerical simulation of gypsum wallboards incorporated with different PCMs content. Appl. Energy 2011, 88, 930–937. [Google Scholar] [CrossRef]
- Eicker, U. Cooling strategies, summer comfort and energy performance of a rehabilitated passive standard office building. Appl. Energy 2010, 87, 2031–2039. [Google Scholar] [CrossRef]
- Tzivanidis, C.; Antonopoulos, K.A.; Gioti, F. Numerical simulation of cooling energy consumption in connection with thermostat operation mode and comfort requirements for the Athens buildings. Appl. Energy 2011, 88, 2871–2884. [Google Scholar] [CrossRef]
- Xiao, W.; Wang, X.; Zhang, Y.P. Analytical optimization of interior PCM for energy storage in a lightweight passive solar room. Appl. Energy 2009, 86, 2013–2018. [Google Scholar] [CrossRef]
- Weng, Y.-C.; Cho, H.-P.; Chang, C.-C.; Chen, S.-L. Heat pipe with PCM for electronic cooling. Appl. Energy 2011, 88, 1825–1833. [Google Scholar] [CrossRef]
- Chou, C.; Tochihara, Y.; Kim, T. Physiological and subjective responses to cooling devices on firefighting protective clothing. Eur. J. Appl. Physiol. 2008, 104, 369–374. [Google Scholar] [CrossRef]
- Mondieig, D.; Rajabalee, F.; Laprie, A.; Oonk, H.A.J.; Calvet, T.; Angel Cuevas-Diarte, M. Protection of temperature sensitive biomedical products using molecular alloys as phase change material. Transfus. Apher. Sci. 2003, 28, 143–148. [Google Scholar] [CrossRef] [Green Version]
- Hauer, A.; Mehling, H.; Schossig, P.; Yamaha, M.; Cabeza, L.; Martin, V.; Setterwall, F.; Expertgroup IEA. Implementing Agreement on Energy Conservation through Energy Storage; Annex 17; Eces, I., Ed.; International Energy Agency: Arvika, Sweden, 2008; pp. 1–132. [Google Scholar]
- Zalba, B.; Marin, J.M.; Cabeza, L.F.; Mehling, H. Review on thermal energy storage with phase change: Materials, heat transfer analysis and applications. Appl. Therm. Eng. 2003, 23, 251–283. [Google Scholar] [CrossRef]
- Gluckman, P.D.; Wyatt, J.S.; Azzopardi, D.; Ballard, R.; Edwards, A.D.; Ferriero, D.M.; Polin, R.A.; Robertson, C.M.; Thoresen, M.; Whitelaw, A.; et al. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: Multicentre randomised trial. Lancet 2005, 365, 663–670. [Google Scholar] [CrossRef]
- Shankaran, S.; Laptook, A.R.; Ehrenkranz, R.A.; Tyson, J.E.; McDonald, S.A.; Donovan, E.F.; Fanaroff, A.A.; Poole, W.K.; Wright, L.L.; Higgins, R.D.; et al. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N. Engl. J. Med. 2005, 353, 1574–1584. [Google Scholar] [CrossRef] [PubMed]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Rüdiger, M.; Skåre, C.; Szczapa, T.; Te Pas, A.; Trevisanuto, D.; et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. Resuscitation 2021, 161, 291–326. [Google Scholar] [CrossRef]
- Azzopardi, D.; Strohm, B.; Edwards, A.D.; Halliday, H.; Juszczak, E.; Levene, M.; Thoresen, M.; Whitelaw, A.; Brocklehurst, P. Treatment of asphyxiated newborns with moderate hypothermia in routine clinical practice: How cooling is managed in the UK outside a clinical trial. Arch. Dis. Child. Fetal Neonatal Ed. 2009, 94, F260–F264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Colbourne, F.; Corbett, D. Delayed postischemic hypothermia: A six month survival study using behavioral and histological assessments of neuroprotection. J. Neurosci. 1995, 15, 7250–7260. [Google Scholar] [CrossRef] [Green Version]
- Taylor, D.L.; Mehmet, H.; Cady, E.B.; Edwards, A.D. Improved neuroprotection with hypothermia delayed by 6 h following cerebral hypoxia-ischemia in the 14-day-old rat. Pediatr. Res. 2002, 51, 13–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thoresen, M.; Penrice, J.; Lorek, A.; Cady, E.; Wylezinska, M.; Kirkbride, V. Mild Hypothermia following severe transient hypoxia-ischaemia ameliorates delayed cerebral energy failure in the newborn piglet. Pediatr. Res. 1995, 37, 667–670. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, S. Whole-body hypothermia for neonatal hypoxic-ischemic encephalopathy reduces mortality into childhood. J. Pediatr. 2012, 161, 968–969. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, S.; Hunt, R.; Tarnow-Mordi, W.; Inder, T.; Davis, P. Cooling for newborns with hypoxic ischaemic encephalopathy. Cochrane Database Syst. Rev. 2007, 4, CD003311. [Google Scholar]
- Nair, J.; Kumar, V.H.S. Current and Emerging Therapies in the Management of Hypoxic Ischemic Encephalopathy in Neonates. Children 2018, 5, 99. [Google Scholar] [CrossRef] [Green Version]
- Olson, L.; Faulkner, S.; Lundströmer, K.; Kerenyi, A.; Kelen, D.; Chandrasekaran, M.; Ådén, U.; Olson, L.; Golay, X.; Lagercrantz, H.; et al. Comparison of Three Hypothermic Target Temperatures for the Treatment of Hypoxic Ischemia: mRNA Level Responses of Eight Genes in the Piglet Brain. Transl. Stroke Res. 2012, 4, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Worner, J.; Oddo, M. Too cold may not be so cool: Spontaneous hypothermia as a marker of poor outcome after cardiac arrest. Crit. Care 2010, 14, 1002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rüegger, C.M.; Davis, P.G.; Cheong, J.L. Xenon as an adjuvant to therapeutic hypothermia in near-term and term newborns with hypoxic-ischaemic encephalopathy. Cochrane Database Syst. Rev. 2018, 8, Cd012753. [Google Scholar] [CrossRef]
- Thoresen, M.; Tooley, J.; Liu, X.; Jary, S.; Fleming, P.; Luyt, K.; Jain, A.; Cairns, P.; Harding, D.; Sabir, H. Time is brain: Starting therapeutic hypothermia within three hours after birth improves motor outcome in asphyxiated newborns. Neonatology 2013, 104, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Walloe, L.; Hjort, N.L.; Thoresen, M. Start cooling as soon as possible. Acta Paediatr. 2019, 108, 771. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hauer, A.; Mehling, H.; Schossig, P.; Yamaha, M.; Cabeza, L.; Martin, V.; Setterwall, F. Advanced thermal energy storage through Phase Change Materials and Chemical Reactions-Feasibility studies and demostration projects, Final report. In Implementing Agreement on Energy Conservation through Energy Storage; Annex 17; Agency, I.E., Ed.; International Energy Agency: Arvika, Sweden, 2009; pp. 1–136. [Google Scholar]
- Wang, W.L.; Yang, X.X.; Fang, Y.T.; Ding, J.; Yan, J.Y. Enhanced thermal conductivity and thermal performance of form-stable composite phase change materials by using beta-Aluminum nitride. Appl. Energy 2009, 86, 1196–1200. [Google Scholar] [CrossRef]
- Muir, I.H.; Bishop, P.A.; Ray, P. Effects of a novel ice-cooling technique on work in protective clothing at 28 degrees C, 23 degrees C, and 18 degrees C WBGTs. Am. Ind. Hyg. Assoc. J. 1999, 60, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Yim, Y.J.; Lee, J.W.; Heo, Y.J.; Park, S.J. Carbon-Filled Organic Phase-Change Materials for Thermal Energy Storage: A Review. Molecules 2019, 24, 2055. [Google Scholar] [CrossRef] [Green Version]
- Yinping, Z.; Yi, J. A simple method, the-history method, of determining the heat of fusion, specific heat and thermal conductivity of phase-change materials. Meas. Sci. Technol. 1999, 10, 201. [Google Scholar] [CrossRef]
- Chen, B.; Wang, X.; Zeng, R.; Zhang, Y.; Wang, X.; Niu, J.; Li, Y.; Di, H. An experimental study of convective heat transfer with microencapsulated phase change material suspension: Laminar flow in a circular tube under constant heat flux. Exp. Therm. Fluid Sci. 2008, 32, 1638–1646. [Google Scholar] [CrossRef]
- Günther, E.; Heibler, S.; Mehling, H.; Redlich, R. Enthalpy of Phase Change Materials as a Function of Temperature: Required Accuracy and Suitable Measurement Methods. Int. J. Thermophys. 2009, 30, 1257–1269. [Google Scholar] [CrossRef]
- Olson, L. Cooling of newborns with PCMs. In IEATA, PCM Future; IEATA: Arvika, Sweden, 2004. [Google Scholar]
- Olson, L. Cooling with phase changing material. In Neonatal Brain and Epigenetics Workshop; Karolinska Institutet: Stockholm, Sweden, 2011. [Google Scholar]
- Sharma, A.; Tyagi, V.V.; Chen, C.R.; Buddhi, D. Review on thermal energy storage with phase change materials and applications. Renew. Sustain. Energy Rev. 2009, 13, 318–345. [Google Scholar] [CrossRef]
- Olson, L. PCM for medical applications. In Annex 17; IEATA: Ankara, Turkey, 2005; Beijing, China, 2006. [Google Scholar]
- Hong, H.; Kim, S.K.; Kim, Y.-S. Accuracy improvement of T-history method for measuring heat of fusion of various materials. Int. J. Refrig. 2004, 27, 360–366. [Google Scholar] [CrossRef]
- Peck, J.H.; Kim, J.-J.; Kang, C.; Hong, H. A study of accurate latent heat measurement for a PCM with a low melting temperature using T-history method. Int. J. Refrig. 2006, 29, 1225–1232. [Google Scholar] [CrossRef]
- Mehling, H.; Cabeza, L.F. Heat and cold storage with PCM an up to date introduction into basics and applications. In Heat and Mass Transfer; Springer: Berlin/Heidelberg, Germany, 2008; Volume 308. [Google Scholar]
- Iwata, S.; Iwata, O.; Olson, L.; Kapetanakis, A.; Kato, T.; Evans, S.; Araki, Y.; Kakuma, T.; Matsuishi, T.; Setterwall, F.; et al. Therapeutic hypothermia can be induced and maintained using either commercial water bottles or a “phase changing material” mattress in a newborn piglet model. Arch. Dis. Child. 2009, 94, 387–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hallberg, B.; Olson, L.; Bartocci, M.; Edqvist, I.; Blennow, M. Passive induction of hypothermia during transport of asphyxiated infants: A risk of excessive cooling. Acta Paediatr. 2009, 98, 942–946. [Google Scholar] [CrossRef]
- Tran, H.T.T.; Le, H.T.T.; Tran, H.T.P.; Khu, D.T.K.; Lagercrantz, H.; Tran, D.M.; Winbladh, B.; Hellström-Westas, L.; Alfvén, T.; Olson, L. Hypothermic treatment for neonatal asphyxia in low-resource settings using phase-changing material-An easy to use and low-cost method. Acta Paediatr. 2021, 110, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Hu, Y.; Hou, Y.; Shen, X.; Xu, G.; Dai, L.; Zhou, J.; Liu, Y.; Cai, K. Phase-change material filled hollow magnetic nanoparticles for cancer therapy and dual modal bioimaging. Nanoscale 2015, 7, 9004–9012. [Google Scholar] [CrossRef]
- Wu, J.; Hu, R.; Zeng, S.; Xi, W.; Huang, S.; Deng, J.; Tao, G. Flexible and Robust Biomaterial Microstructured Colored Textiles for Personal Thermoregulation. ACS Appl. Mater. Interfaces 2020, 12, 19015–19022. [Google Scholar] [CrossRef] [PubMed]
- Yan, Y.; Li, W.; Zhu, R.; Lin, C.; Hufenus, R. Flexible Phase Change Material Fiber: A Simple Route to Thermal Energy Control Textiles. Materials 2021, 14, 401. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Long, J.; Du, Y.; Zhou, J.; Wang, Y.; Miao, Z.; Liu, Y.; Xu, S.; Cao, S. Recyclable low-temperature phase change microcapsules for cold storage. J. Colloid Interface Sci. 2020, 564, 286–295. [Google Scholar] [CrossRef] [PubMed]
- Thayyil, S.; Costello, A.; Shankaran, S.; Robertson, N.J. Therapeutic hypothermia for neonatal encephalopathy implications for neonatal units in India. Indian Pediatr. 2009, 46, 283–289. [Google Scholar] [PubMed]
- Robertson, N.J.; Nakakeeto, M.; Hagmann, C.; Cowan, F.M.; Acolet, D.; Iwata, O.; Allen, E.; Elbourne, D.; Costello, A.; Jacobs, I. Therapeutic hypothermia for birth asphyxia in low-resource settings: A pilot randomised controlled trial. Lancet 2008, 372, 801–803. [Google Scholar] [CrossRef]
- Montaldo, P.; Pauliah, S.S.; Lally, P.J.; Olson, L.; Thayyil, S. Cooling in a low-resource environment: Lost in translation. Semin. Fetal Neonatal Med. 2015, 20, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Thayyil, S.; Bhutta, Z.A.; Ramji, S.; Costello, A.M.; Robertson, N. J Global application of therapeutic hypothermia to treat perinatal asphyxial encephalopathy. Int. Health 2010, 2, 79–81. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.; Abiramalatha, T.; Bhat, V.; Varanattu, M.; Rao, S.; Wazir, S.; Lewis, L.; Balakrishnan, U.; Murki, S.; Mittal, J.; et al. Phase Changing Material for Therapeutic Hypothermia in Neonates with Hypoxic Ischemic Encephalopathy—Multi-centric Study. Indian Pediatr. 2018, 55, 201–205. [Google Scholar] [CrossRef]
Figure 1.
Available phase changing materials and the relation between melting temperature and heat of fusion from these materials.
Figure 1.
Available phase changing materials and the relation between melting temperature and heat of fusion from these materials.

Figure 2.
Schematic illustration of experimental setup for monitoring temperature characteristics of different PCM mixtures (yellow) in a water bath with temperatures cycling between 5 and 45 °C. A temperature probe is located in the material to be tested. The test tube has a thin outside insulation (not shown) to dampen speed of temperature changes (see text). The water bath contains a heater, and a stirrer. The stirrer also carries a temperature probe, such that both the heater and the stirrer rpm is controlled by water temperature and temperature changes. Control test tubes (not shown) contain water, jellified water or a known PCM mixture.
Figure 2.
Schematic illustration of experimental setup for monitoring temperature characteristics of different PCM mixtures (yellow) in a water bath with temperatures cycling between 5 and 45 °C. A temperature probe is located in the material to be tested. The test tube has a thin outside insulation (not shown) to dampen speed of temperature changes (see text). The water bath contains a heater, and a stirrer. The stirrer also carries a temperature probe, such that both the heater and the stirrer rpm is controlled by water temperature and temperature changes. Control test tubes (not shown) contain water, jellified water or a known PCM mixture.

Figure 3.
Effect of adding different concentrations of NaCl on melting temperature of PCM. In the absence of NaCl, the melting point (red) is 32 °C. Adding increasing amounts of NaCl decreases the melting temperature to approximately 25 °C when 5% NaCl is added. Further additions of NaCl do not appear to cause further decrease of the melting point. The approximated curve (blue) does not illustrate the possibility that there may be further complexity of the melting point temperatures in the 1.5–3.0% NaCl range, due to the technical limitations of our experimental set up. However, the correlation is significant.
Figure 3.
Effect of adding different concentrations of NaCl on melting temperature of PCM. In the absence of NaCl, the melting point (red) is 32 °C. Adding increasing amounts of NaCl decreases the melting temperature to approximately 25 °C when 5% NaCl is added. Further additions of NaCl do not appear to cause further decrease of the melting point. The approximated curve (blue) does not illustrate the possibility that there may be further complexity of the melting point temperatures in the 1.5–3.0% NaCl range, due to the technical limitations of our experimental set up. However, the correlation is significant.

Figure 4.
Heating–cooling curves for different mixtures of NaCl and Na2SO4 in water with CMC added as stabilizing gelifier. The PCM mixtures are compared to water, also gelified by CMC (purple). During heating, all three PCM mixtures differ from water by having a lesser slope and also by brief periods of energy take up at around 30–32 °C (1% NaCl, blue curve is partly hidden). During cooling, there is less diversity, although the slopes of the PCM curves are less steep than that of water. Please note that lowering the bath temperature to 5 °C caused a temporary increase of temperature in PCM containing 1% NaCl (blue).
Figure 4.
Heating–cooling curves for different mixtures of NaCl and Na2SO4 in water with CMC added as stabilizing gelifier. The PCM mixtures are compared to water, also gelified by CMC (purple). During heating, all three PCM mixtures differ from water by having a lesser slope and also by brief periods of energy take up at around 30–32 °C (1% NaCl, blue curve is partly hidden). During cooling, there is less diversity, although the slopes of the PCM curves are less steep than that of water. Please note that lowering the bath temperature to 5 °C caused a temporary increase of temperature in PCM containing 1% NaCl (blue).
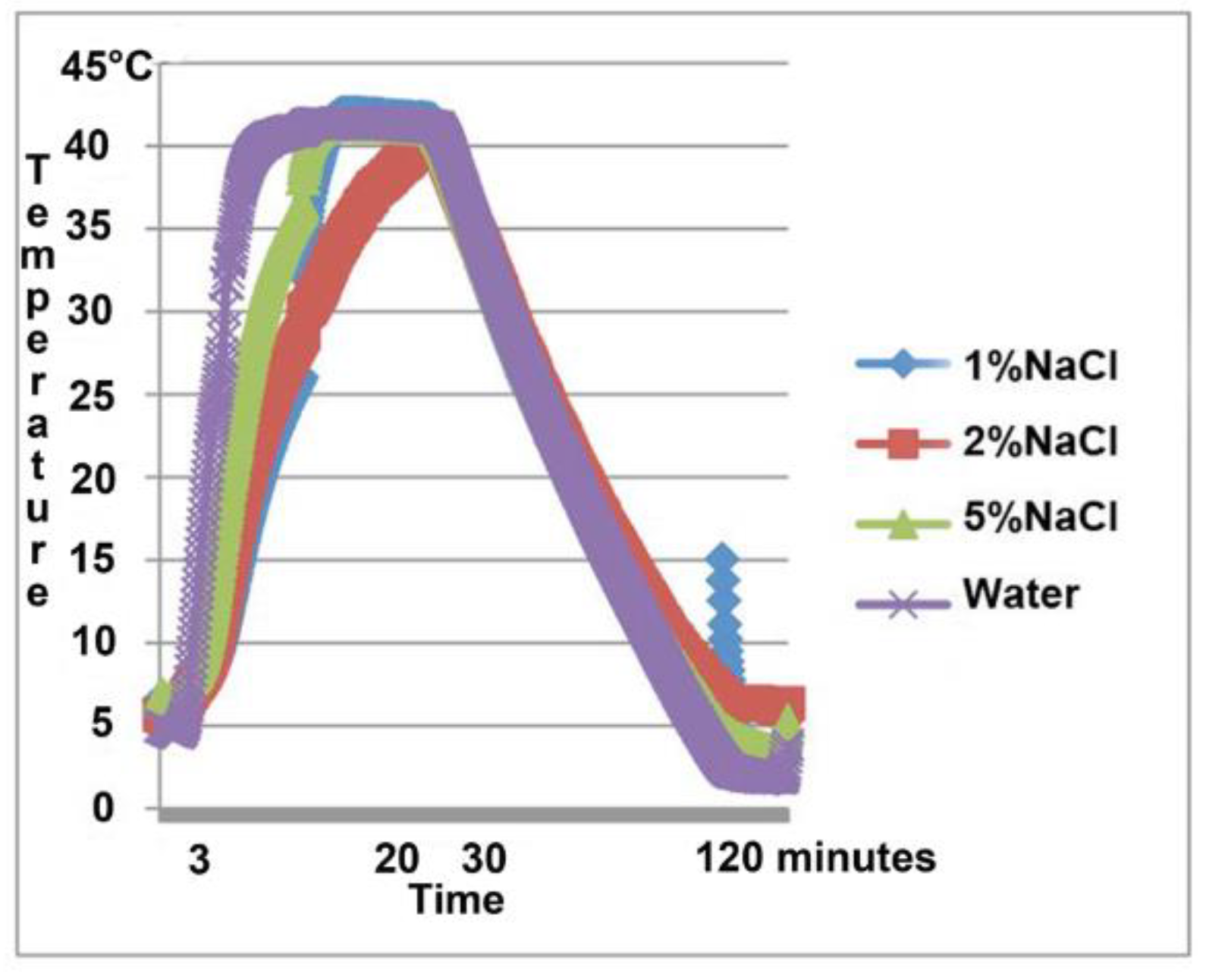
Figure 5.
Phase diagrams for the system NACl-Na2SO4- H2O at 17.5 (a) and 25 °C (b). From Mullin, J.W.: Crystallization, Fourth Edition, Reed Educational and Professional Ltd. Reproduced with permission from Butterworth-Heinemann, Oxford. Please note that the B-C curve descends with increasing amounts of NaCl. Na = Natrium, S = sulfite, Cl = Clorine, H = helium, O = Oxygen.
Figure 5.
Phase diagrams for the system NACl-Na2SO4- H2O at 17.5 (a) and 25 °C (b). From Mullin, J.W.: Crystallization, Fourth Edition, Reed Educational and Professional Ltd. Reproduced with permission from Butterworth-Heinemann, Oxford. Please note that the B-C curve descends with increasing amounts of NaCl. Na = Natrium, S = sulfite, Cl = Clorine, H = helium, O = Oxygen.
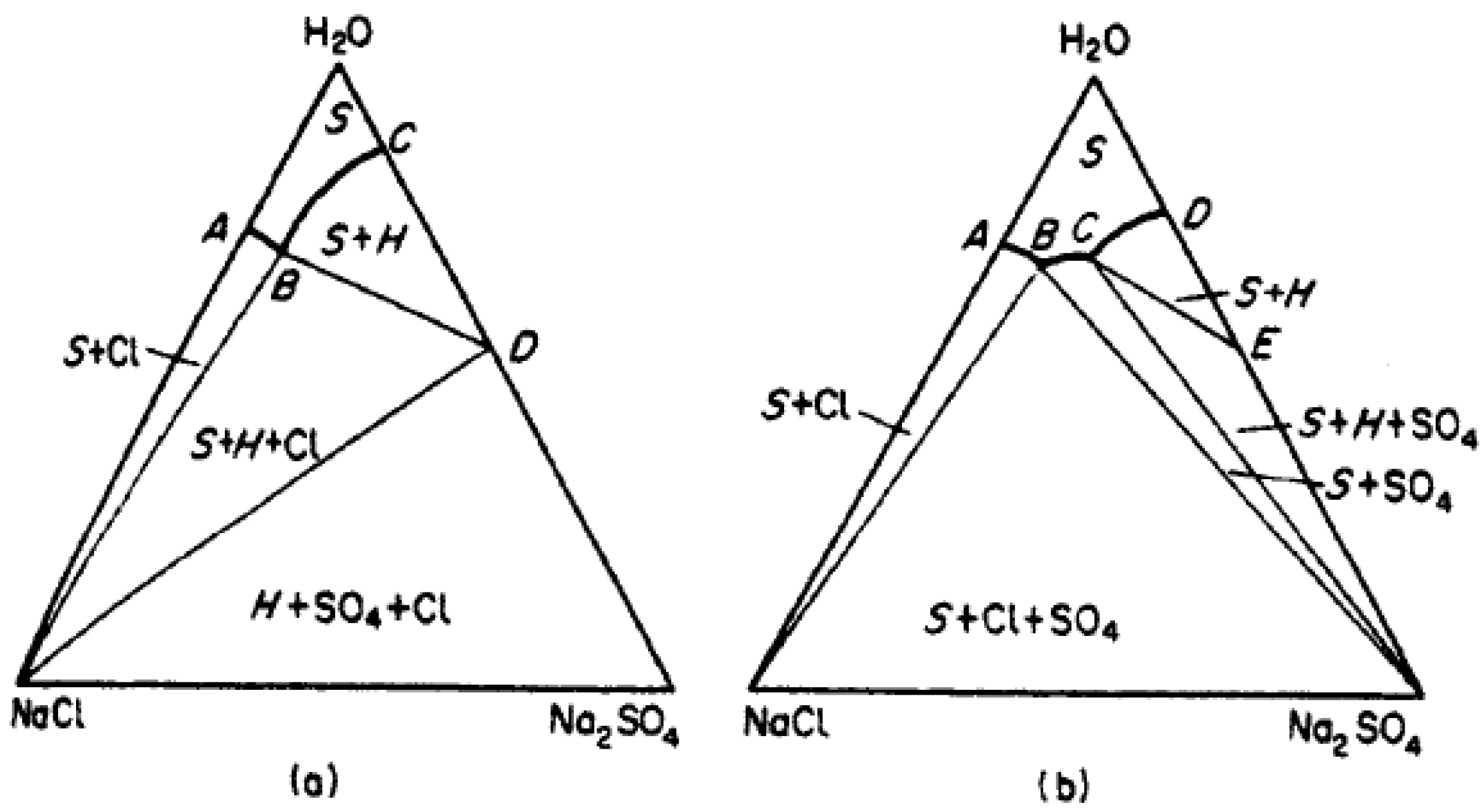
Figure 6.
Enthalpy–concentration weight fraction temperature diagram from Mullin, J.W.: Crystallization, Fourth Edition, Reed Educational and Professional Ltd. Reproduced with permission from Butterworth–Heinemann, Oxford. There is risk of sulfate anhydrite and deposition to the right of the vertical line spanning the whole diagram. Location in this diagram of our experimental trials and % of water content in the solution are indicated by arrows. The red arrow shows how moving in the area of interest can effect where we are in diagram.
Figure 6.
Enthalpy–concentration weight fraction temperature diagram from Mullin, J.W.: Crystallization, Fourth Edition, Reed Educational and Professional Ltd. Reproduced with permission from Butterworth–Heinemann, Oxford. There is risk of sulfate anhydrite and deposition to the right of the vertical line spanning the whole diagram. Location in this diagram of our experimental trials and % of water content in the solution are indicated by arrows. The red arrow shows how moving in the area of interest can effect where we are in diagram.
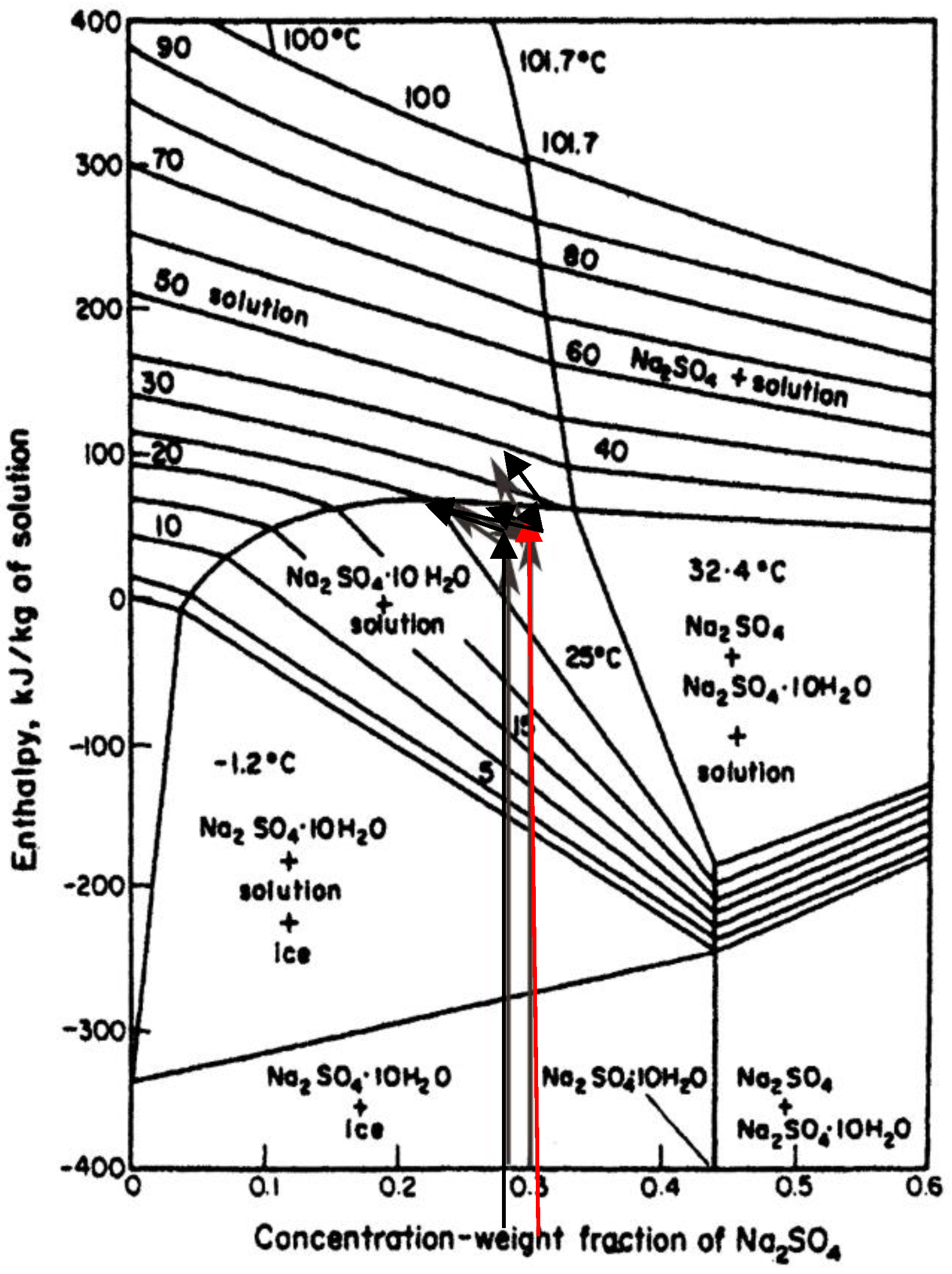
Figure 7.
An asphyxia piglet on a PCM 32 mattress with a gel mattress cover continuously cooled to 33.5 °C. From a study Iwata et al. [45].
Figure 7.
An asphyxia piglet on a PCM 32 mattress with a gel mattress cover continuously cooled to 33.5 °C. From a study Iwata et al. [45].
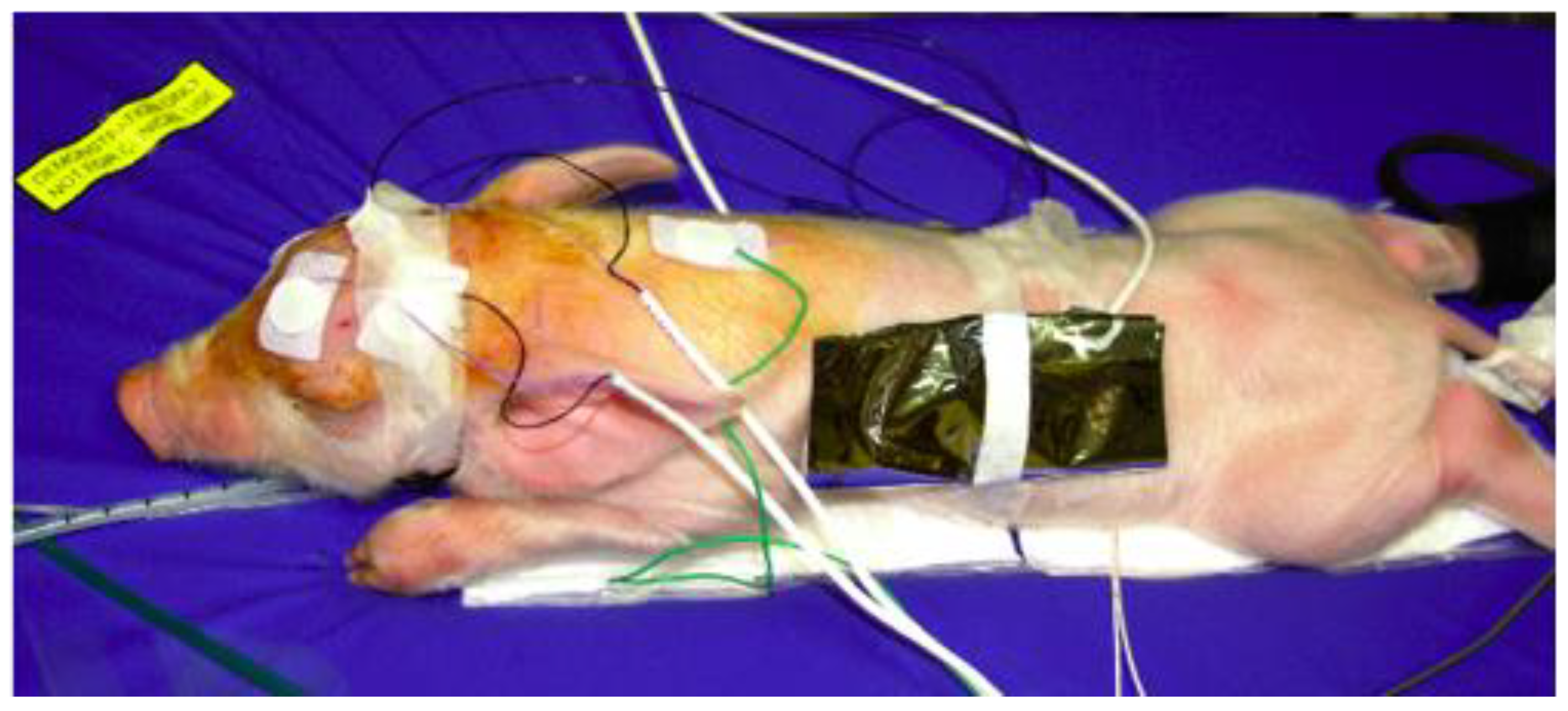
Figure 8.
Baby being cooled on a PCM-mattress (blue) in a neonatal ward. With permission from the parents. The mattress contains PCM and a layer of soft material.
Figure 8.
Baby being cooled on a PCM-mattress (blue) in a neonatal ward. With permission from the parents. The mattress contains PCM and a layer of soft material.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
PCM criteria needed for medical applications such as cooling of infants and children suffering from oxygen deprivation.
Table 1.
PCM criteria needed for medical applications such as cooling of infants and children suffering from oxygen deprivation.
| No. | Criterion | What Needs to Be Done |
|---|---|---|
| 1. | Must deliver controlled set temperature that gives the cooled object a temperature of 33.5–34.5 °C. | New mixtures that can deliver the temperatures the medical market asks for. |
| 2. | Must be non-toxic. | The ingredients in the solution need to be tested for toxicity or the material needs to be securely encapsulated. |
| 3. | Must not expand or in any other way cause injuries to the intended target. | Needs to be tested for each solution in a helicopter test. |
| 4. | Must have a rapid cooling effect but with no cooling undershoot. | Needs to be tested. |
| 5. | Should be stable for at least 72 h. | If cooling time is shorter, a fast change should be possible without problems for staff or patient. |
| 6. | Be of low cost. | Enables use in developing countries |
| 7. | No interbatch variability. | Each mixture needs to be tested to fulfill criteria. |
| 8. | Able to cycle through cooling phase change at least 100 times. | Needs to be tested. |
| 9. | Effective without electricity or water supply is a major advantage. | Choose PCM as the cooling agent. |
| 10. | Reversed phase change no longer than 4 h. | Reversed cycle needed to be tested. |
| 11. | Magnetic resonance imaging compatible. | No metallic or magnetic compounds can be involved in end-product. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Olson, L.; Lothian, C.; Ådén, U.; Lagercrantz, H.; Robertson, N.J.; Setterwall, F. Phase-Changing Glauber Salt Solution for Medical Applications in the 28–32 °C Interval. Materials 2021, 14, 7106. https://doi.org/10.3390/ma14237106
AMA Style
Olson L, Lothian C, Ådén U, Lagercrantz H, Robertson NJ, Setterwall F. Phase-Changing Glauber Salt Solution for Medical Applications in the 28–32 °C Interval. Materials. 2021; 14(23):7106. https://doi.org/10.3390/ma14237106
Chicago/Turabian StyleOlson, Linus, Carina Lothian, Ulrika Ådén, Hugo Lagercrantz, Nicola J. Robertson, and Fredrik Setterwall. 2021. "Phase-Changing Glauber Salt Solution for Medical Applications in the 28–32 °C Interval" Materials 14, no. 23: 7106. https://doi.org/10.3390/ma14237106
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.