
Vital Pulp Therapy in Aesthetic Zone-Identifying the Biomaterial That Reduces the Risk of Tooth Discolouration


Abstract
:1. Introduction
2. Materials and Methods
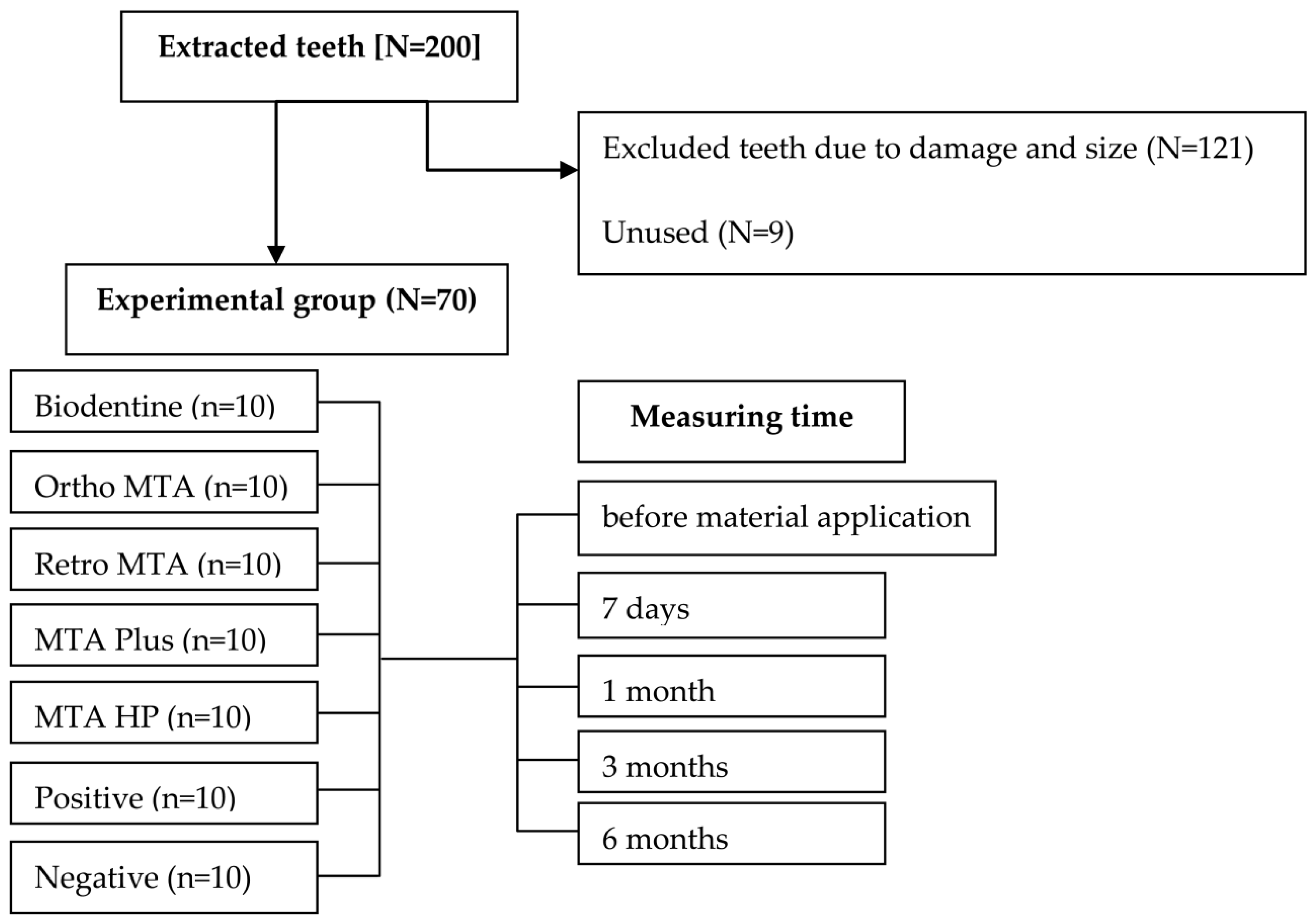
2.1. Sample Preparation
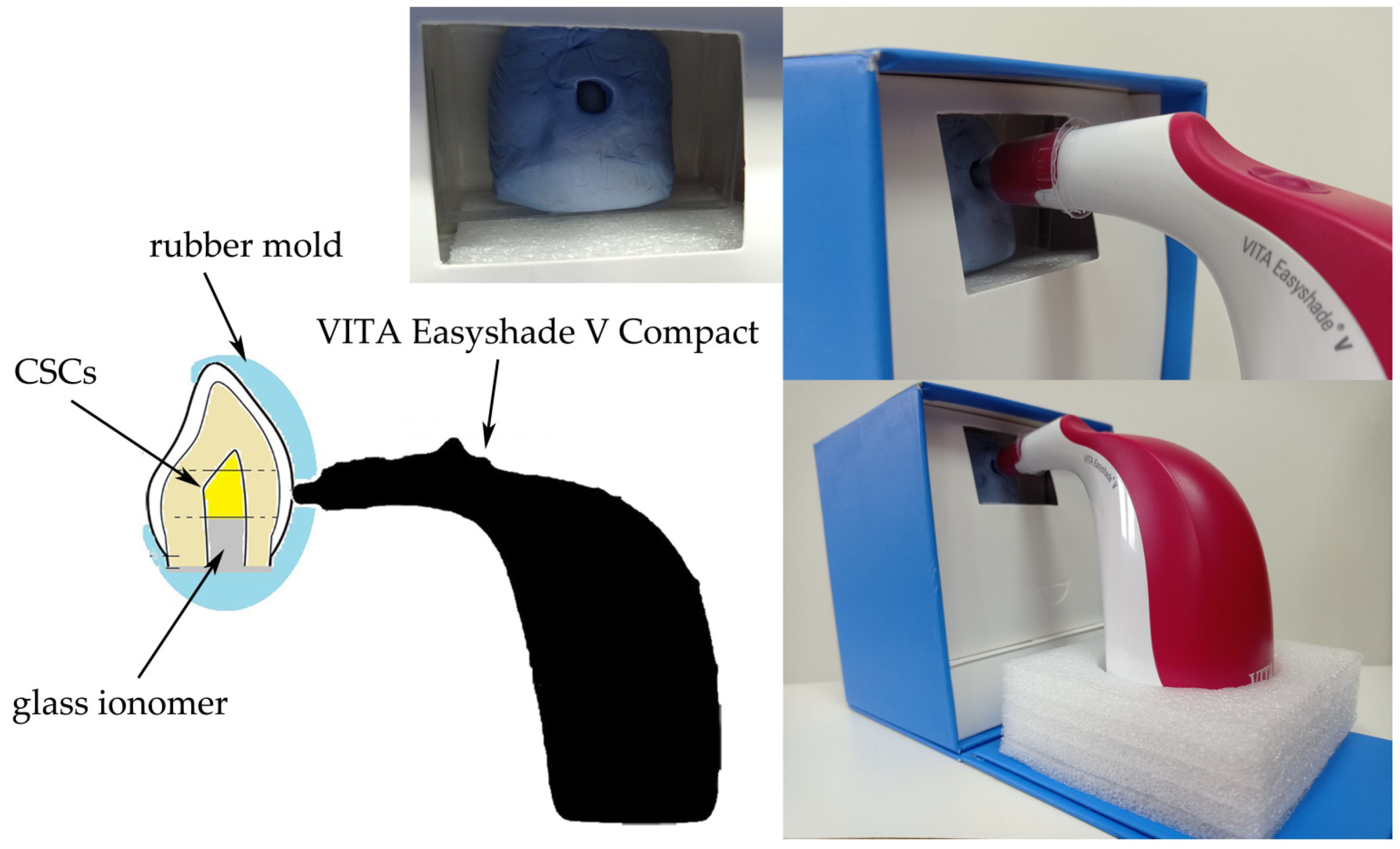
2.2. Measuring Tooth Discolouration
2.3. Statistical Analyses
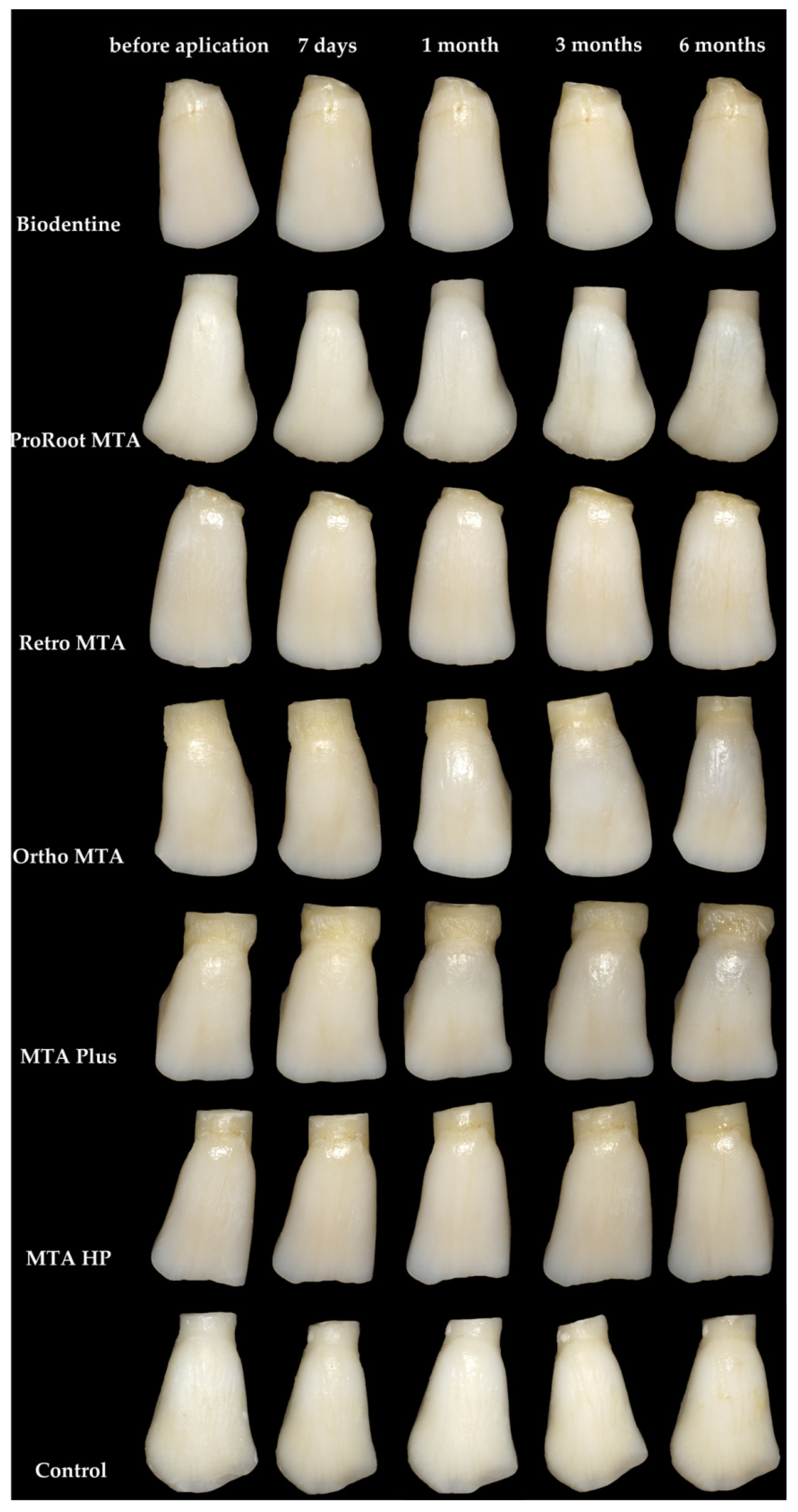
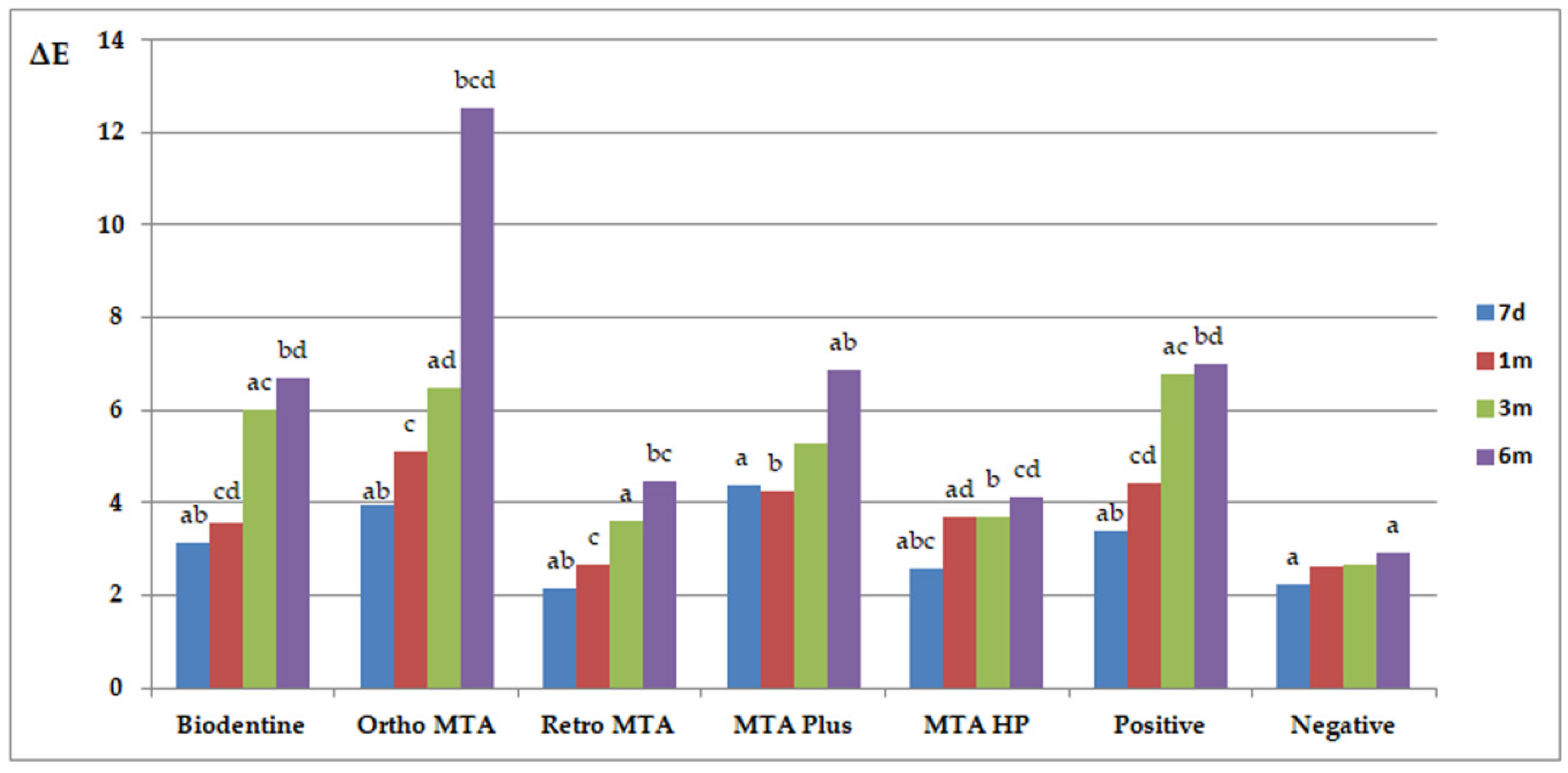
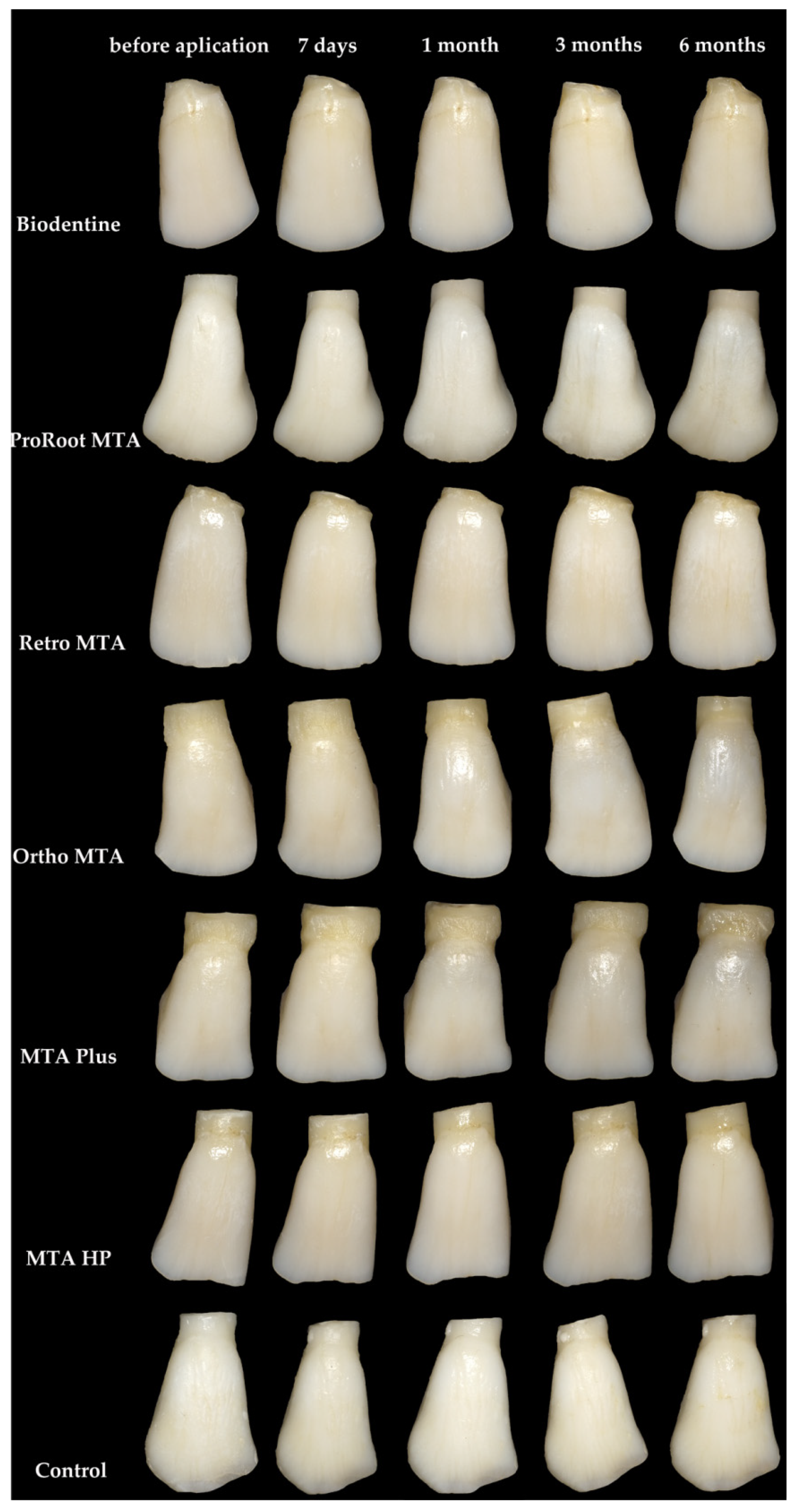
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Santos, J.; Pereira, J.; Marques, A.; Sequeira, D.; Friedman, S. Vital pulp therapy in permanent mature posterior teeth with symptomatic irreversible pulpitis: A systematic review of treatment outcomes. Med. Kaunas 2021, 57, 573. [Google Scholar] [CrossRef]
- Ricucci, D.; Siqueira, J.F.; Li, Y.; Tay, F.R. Vital pulp therapy: Histopathology and histobacteriology-based guidelines to treat teeth with deep caries and pulp exposure. J. Dent. 2019, 86, 41–52. [Google Scholar] [CrossRef] [PubMed]
- Naseri, M.; Khayat, A.; Zamaheni, S.; Shojaeian, S. Correlation between histological status of the pulp and its response to sensibility tests. Iran. Endod. J. 2017, 12, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Ghoddusi, J.; Forghani, M.; Parisay, I. New approaches in vital pulp therapy in permanent teeth. Iran. Endod. J. 2014, 9, 15–22. [Google Scholar] [PubMed]
- Palma, P.J.; Marques, J.A.; Antunes, M.; Falacho, R.I.; Sequeira, D.; Roseiro, L.; Santos, J.M.; Ramos, J.C. Effect of restorative timing on shear bond strength of composite resin/calcium silicate-based cements adhesive interfaces. Clin. Oral Investig. 2021, 25, 3131–3139. [Google Scholar] [CrossRef] [PubMed]
- American Association of Endodontists Glossary of Endodontic Terms, 9th ed., Chicago, IL, USA. Available online: http://www.aae.org/clinical-resources/aae-glossary-of-endodontic-terms.aspx (accessed on 11 February 2020).
- Qudeimat, M.A.; Alyahya, A.; Hasan, A.A. Mineral trioxide aggregate pulpotomy for permanent molars with clinical signs indicative of irreversible pulpitis: A preliminary study. Int. Endod. J. 2017, 50, 126–134. [Google Scholar] [CrossRef]
- Taha, N.A.; Ahmad, M.B.; Ghanim, A. Assessment of Mineral Trioxide Aggregate pulpotomy in mature permanent teeth with carious exposures. Int. Endod. J. 2017, 50, 117–125. [Google Scholar] [CrossRef]
- Meza, G.; Urrejola, D.; Saint Jean, N.; Inostroza, C.; López, V.; Khoury, M.; Brizuela, C. Personalized cell therapy for pulpitis using autologous dental pulp stem cells and leukocyte platelet-rich fibrin: A case report. J. Endod. 2019, 45, 144–149. [Google Scholar] [CrossRef]
- Fagogeni, I.; Metlerska, J.; Lipski, M.; Falgowski, T.; Maciej, G.; Nowicka, A. Materials used in regenerative endodontic procedures and their impact on tooth discoloration. J. Oral Sci. 2019, 61, 379–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tetè, G.; D’Orto, B.; Nagni, M.; Agostinacchio, M.; Polizzi, E.; Agliardi, E. Role of induced pluripotent stem cells (IPSCS) in bone tissue regeneration in dentistry: A narrative review. J. Biol. Regul. Homeost. Agents 2020, 34, 1–10. [Google Scholar] [PubMed]
- Duncan, H.F.; Cooper, P.R.; Smith, A.J. Dissecting dentine-pulp injury and wound healing responses: Consequences for regenerative endodontics. Int. Endod. J. 2019, 52, 261–266. [Google Scholar] [CrossRef] [Green Version]
- Huang, G.T.; Liu, J.; Zhu, X.; Yu, Z.; Li, D.; Chen, C.A.; Azim, A.A. Pulp/dentin regeneration: It should be complicated. J. Endod. 2020, 46, S128–S134. [Google Scholar] [CrossRef]
- Paula, A.B.; Laranjo, M.; Marto, C.-M.; Paulo, S.; Abrantes, A.M.; Casalta-Lopes, J.; Marques-Ferreira, M.; Botelho, M.F.; Carrilho, E. Direct pulp capping: What is the most effective therapy?—Systematic review and meta-analysis. J. Evid. Based. Dent. Pract. 2018, 18, 298–314. [Google Scholar] [CrossRef]
- Prosser, H.J.; Groffman, D.M.; Wilson, A.D. The effect of composition on the erosion properties of calcium hydroxide cements. J. Dent. Res. 1982, 61, 1431–1435. [Google Scholar] [CrossRef]
- Hilton, T.J.; Ferracane, J.L.; Mancl, L. Northwest practice-based research collaborative in evidence-based dentistry (NWP). comparison of CaOH with MTA for direct pulp capping: A PBRN randomized clinical trial. J. Dent. Res. 2013, 92, 16S–22S. [Google Scholar] [CrossRef] [Green Version]
- Holland, R.; De Souza, V.; Murata, S.S.; Nery, M.J.; Bernabé, P.F.; Filho, J.A.O.; Junior, E.D. Healing process of dog dental pulp after pulpotomy and pulp covering with mineral trioxide aggregate or Portland cement. Braz. Dent. J. 2001, 12, 109–113. [Google Scholar] [PubMed]
- Eidelman, E.; Holan, G.; Fuks, A.B. Mineral trioxide aggregate vs. formocresol in pulpotomized primary molars: A preliminary report. Pediatr. Dent. 2001, 23, 15–18. [Google Scholar] [PubMed]
- Camilleri, J. Modification of mineral trioxide aggregate. Physical and mechanical properties. Int. Endod. J. 2008, 41, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, J. The chemical composition of mineral trioxide aggregate. J. Conserv. Dent. 2008, 11, 141–143. [Google Scholar] [CrossRef] [PubMed]
- Gomes-Cornélio, A.L.; Rodrigues, E.M.; Mestieri, L.B.; Falcoski Tde, O.; Soares, C.P.; Guerreiro-Tanomaru, J.M.; Rossa, C.J.; Tanomaru, M.F. Cytotoxicity and genotoxicity of calcium silicate-based cements on an osteoblast lineage. Braz. Oral Res. 2016, 30, S1806-83242016000100247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torabinejad, M.; Parirokh, M. Mineral trioxide aggregate: A comprehensive literature review--part II: Leakage and biocompatibility investigations. J. Endod. 2010, 36, 190–202. [Google Scholar] [CrossRef]
- Parirokh, M.; Torabinejad, M. Mineral trioxide aggregate: A comprehensive literature review--Part III: Clinical applications, drawbacks, and mechanism of action. J. Endod. 2010, 36, 400–413. [Google Scholar] [CrossRef]
- Nowicka, A.; Wilk, G.; Lipski, M.; Kołecki, J.; Buczkowska-Radlińska, J. Tomographic evaluation of reparative dentin formation after direct pulp capping with Ca(OH)2, MTA, Biodentine, and dentin bonding system in human teeth. J. Endod. 2015, 41, 1234–1240. [Google Scholar] [CrossRef]
- Możyńska, J.; Metlerski, M.; Lipski, M.; Nowicka, A. Tooth discoloration induced by different calcium silicate-based cements: A systematic review of in vitro studies. J. Endod. 2017, 43, 1593–1601. [Google Scholar] [CrossRef] [PubMed]
- Dawood, A.E.; Parashos, P.; Wong, R.H.K.; Reynolds, E.C.; Manton, D.J. Calcium silicate-based cements: Composition, properties, and clinical applications. J. Investig. Clin. Dent. 2017, 8, e12195. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Siboni, F.; Primus, C.M.; Prati, C. Ion release, porosity, solubility, and bioactivity of MTA Plus tricalcium silicate. J. Endod. 2014, 40, 1632–1637. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, B.M.; Prati, C.; Duarte, M.A.H.; Bramante, C.M.; Gandolfi, M.G. Physicochemical properties of calcium silicate-based formulations MTA Repair HP and MTA Vitalcem. J. Appl. Oral Sci. 2018, 26, e2017115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International Commission on Illumination. Recommendations on Uniform Color Spaces, Color—Difference Equations, Psychometric Color Terms; Bureau Central de la CIE: Paris, France, 1978; p. 1913. [Google Scholar]
- Karamouzos, A.; Papadopoulos, M.A.; Kolokithas, G.; Athanasiou, A.E. Precision of in vivo spectrophotometric colour evaluation of natural teeth. J. Oral Rehabil. 2007, 34, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Cazzaniga, G.; Ottobelli, M.; Ionescu, A.C.; Paolone, G.; Gherlone, E.; Ferracane, J.L.; Brambilla, E. In vitro biofilm formation on resin-based composites after different finishing and polishing procedures. J. Dent. 2017, 67, 43–52. [Google Scholar] [CrossRef]
- Polizzi, E.; Tetè, G.; Targa, C.; Salviato, B.; Ferrini, F.; Gastaldi, G. Evaluation of the effectiveness of the use of the diode laser in the reduction of the volume of the edematous gingival tissue after causal therapy. Int. J. Environ. Res. Public Health 2020, 17, 6192. [Google Scholar] [CrossRef]
- Vallés, M.; Roig, M.; Duran-Sindreu, F.; Martínez, S.; Mercadé, M. Color stability of teeth restored with biodentine: A 6-month in vitro study. J. Endod. 2015, 41, 1157–1160. [Google Scholar] [CrossRef] [PubMed]
- Ramos, J.C.; Palma, P.J.; Nascimento, R.; Caramelo, F.; Messias, A.; Vinagre, A.; Santos, J.M. 1-year in vitro evaluation of tooth discoloration induced by 2 calcium silicate-based cements. J. Endod. 2016, 42, 1403–1407. [Google Scholar] [CrossRef] [PubMed]
- Schmalz, G.; Hiller, K.A.; Nunez, L.J.; Stoll, J.; Weis, K. Permeability characteristics of bovine and human dentin under different pretreatment conditions. J. Endod. 2001, 27, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Tagami, J.; Tao, L.; Pashley, D.H.; Horner, J.A. The permeability of dentine from bovine incisors in vitro. Arch. Oral Biol. 1989, 34, 773–777. [Google Scholar] [CrossRef]
- Kang, S.H.; Shin, Y.S.; Lee, H.S.; Kim, S.O.; Shin, Y.; Jung, I.Y.; Song, J.S. Color changes of teeth after treatment with various mineral trioxide aggregate-based materials: An ex vivo study. J. Endod. 2015, 41, 737–741. [Google Scholar] [CrossRef]
- Lenherr, P.; Allgayer, N.; Weiger, R.; Filippi, A.; Attin, T.; Krastl, G. Tooth discoloration induced by endodontic materials: A laboratory study. Int. Endod. J. 2012, 45, 942–949. [Google Scholar] [CrossRef]
- Jang, J.H.; Kang, M.; Ahn, S.; Kim, S.; Kim, W.; Kim, Y.; Kim, E. Tooth discoloration after the use of new pozzolan cement (Endocem) and mineral trioxide aggregate and the effects of internal bleaching. J. Endod. 2013, 39, 1598–1602. [Google Scholar] [CrossRef]
- Ioannidis, K.; Mistakidis, I.; Beltes, P.; Karagiannis, V. Spectrophotometric analysis of coronal discolouration induced by grey and white MTA. Int. Endod. J. 2013, 46, 137–144. [Google Scholar] [CrossRef]
- Shokouhinejad, N.; Nekoofar, M.H.; Pirmoazen, S.; Shamshiri, A.R.; Dummer, P.M. Evaluation and comparison of occurrence of tooth discoloration after the application of various calcium silicate-based cements: An ex vivo study. J. Endod. 2016, 42, 140–144. [Google Scholar] [CrossRef]
- Aguiar, B.A.; Frota, L.M.A.; Taguatinga, D.T.; Vivan, R.R.; Camilleri, J.; Duarte, M.A.H.; de Vasconcelos, B.C. Influence of ultrasonic agitation on bond strength, marginal adaptation, and tooth discoloration provided by three coronary barrier endodontic materials. Clin. Oral Investig. 2019, 23, 4113–4122. [Google Scholar] [CrossRef]
- Beatty, H.; Svec, T. Quantifying coronal tooth discoloration caused by Biodentine and EndoSequence Root Repair Material. J. Endod. 2015, 41, 2036–2039. [Google Scholar] [CrossRef]
- Dettwiler, C.A.; Walter, M.; Zaugg, L.K.; Lenherr, P.; Weiger, R.; Krastl, G. In vitro assessment of the tooth staining potential of endodontic materials in a bovine tooth model. Dent. Traumatol. 2016, 32, 480–487. [Google Scholar] [CrossRef]
- Kohli, M.R.; Yamaguchi, M.; Setzer, F.C.; Karabucak, B. Spectrophotometric analysis of coronal tooth discoloration induced by various bioceramic cements and other endodontic materials. J. Endod. 2015, 41, 1862–1866. [Google Scholar] [CrossRef]
- Metlerska, J.; Dammaschke, T.; Lipski, M.; Fagogeni, I.; Machoy-Mokrzyńska, A.; Nowicka, A. Effect of citric acid on color changes of calcium silicate-based cements an in vitro study. Appl. Sci. 2021, 11, 2339. [Google Scholar] [CrossRef]
- Camilleri, J.; Borg, J.; Damidot, D.; Salvadori, E.; Pilecki, P.; Zaslansky, P.; Darvell, B.W. Colour and chemical stability of bismuth oxide in dental materials with solutions used in routine clinical practice. PLoS ONE 2020, 15, e0240634. [Google Scholar] [CrossRef] [PubMed]
- Vallés, M.; Mercadé, M.; Duran-Sindreu, F.; Bourdelande, J.L.; Roig, M. Color stability of white mineral trioxide aggregate. Clin. Oral Investig. 2013, 17, 1155–1159. [Google Scholar] [CrossRef]
- Marciano, M.A.; Duarte, M.A.; Camilleri, J. Dental discoloration caused by bismuth oxide in MTA in the presence of sodium hypochlorite. Clin. Oral Investig. 2015, 19, 2201–2209. [Google Scholar] [CrossRef]
- Berger, T.; Baratz, A.Z.; Gutmann, J.L. In vitro investigations into the etiology of mineral trioxide tooth staining. J. Conserv. Dent. 2014, 17, 526–530. [Google Scholar] [CrossRef] [Green Version]
- Camilleri, J.; Montesin, F.E.; Papaioannou, S.; McDonald, F.; Pitt Ford, T.R. Biocompatibility of two commercial forms of mineral trioxide aggregate. Int. Endod. J. 2004, 37, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Palma, P.J.; Marques, J.A.; Santos, J.; Falacho, R.I.; Sequeira, D.; Diogo, P.; Caramelo, F.; Ramos, J.C.; Santos, J.M. Tooth discoloration after regenerative endodontic procedures with calcium silicate-based cements—An ex vivo study. Appl. Sci. 2020, 10, 5793. [Google Scholar] [CrossRef]
- Felman, D.; Parashos, P. Coronal tooth discoloration and white mineral trioxide aggregate. J. Endod. 2013, 39, 484–487. [Google Scholar] [CrossRef] [PubMed]
- Capparè, P.; Tetè, G.; Sberna, M.T.; Panina-Bordignon, P. The emerging role of stem cells in regenerative dentistry. Curr. Gene Ther. 2020, 20, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Fagogeni, I.; Falgowski, T.; Metlerska, J.; Lipski, M.; Górski, M.; Nowicka, A. Efficiency of teeth bleaching after regenerative endodontic treatment: A systematic review. J. Clin. Med. 2021, 10, 316. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Material | Manufacturer | Ingredients-Radiopacifer | Mixing |
|---|---|---|---|
| Biodentine | Septodont, Saint-Maur-des-Fossés Cedex, France | powder: tricalcium silicate, dicalcium silicate, calcium carbonate and oxide filler, iron oxide shade, and zirconium oxide liquid: calcium chloride as accelerator, hydrosoluble polymer water-reducing agent, water | 0.7 g capsule of powder + 5 drops of liquid (30 s; 4000–4200 rpm) |
| Ortho MTA | BioMTA, Seoul, Korea | calcium carbonate, silicon dioxide, aluminium oxide, and dibismuth trioxide | 0.2 g pouches of powder + 2 drops of water (mixed manually) |
| Retro MTA | BioMTA, Seoul, Korea | calcium carbonate, silicon dioxide, aluminium oxide, and calcium zirconia complex | 0.3 g pouches of powder + 3 drops of water (mixed manually) |
| MTA Plus | Avalon Biomed Inc, by Prevest Denpro Limited, Jammu, India | powder: tricalcium silicate, dicalcium silicate, bismuth oxide, calcium sulfate, and silica liquid: hydrated polymer gel | Powder + liquid (mixed manually) |
| MTA Repair HP | Angelus, Londrina, PR, Brazil | powder: tricalcium silicate, dicalcium silicate, tricalcium aluminate, calcium oxide, and calcium tungstate liquid: water and plasticizer | 0.085 g capsules of powder + 2 drops of liquid (mixed manually) |
| ProRoot MTA | Dentsply, Tulsa, OK, USA | tricalcium silicate, dicalcium silicate, tricalcium aluminate, tetracalcium aluminoferrite, free calcium oxide, and bismuth oxide | 0.5 g pouches of powder + pre-measured unit dose of water (mixed manually) |
| Ortho MTA | Retro MTA | MTA Plus | MTA HP | Positive | Negative | ||
|---|---|---|---|---|---|---|---|
| Biodentine | 7 d | 0.0202 | |||||
| 1 m | |||||||
| 3 m | 0.0321 | 0.0230 | 0.0020 | ||||
| 6 m | 0.0348 | 0.0231 | 0.0017 | ||||
| Ortho MTA | 7 d | ||||||
| 1 m | 0.0178 | ||||||
| 3 m | 0.0065 | 0.0003 | |||||
| 6 m | 0.0420 | 0.0021 | 0.0331 | 0.0007 | |||
| Retro MTA | 7 d | 0.0124 | |||||
| 1 m | 0.0311 | 0.0049 | 0.0423 | 0.0174 | |||
| 3 m | 0.0494 | 0.0267 | 0.0100 | ||||
| 6 m | 0.0034 | 0.0021 | 0.0095 | ||||
| MTA Plus | 7 d | 0.0336 | 0.0080 | ||||
| 1 m | 0.0000 | ||||||
| 3 m | 0.0071 | 0.0001 | |||||
| 6 m | 0.0218 | 0.0019 | |||||
| MTA HP | 7 d | ||||||
| 1 m | 0.0129 | 0.0000 | |||||
| 3 m | 0.0067 | 0.0001 | |||||
| 6 m | 0.0000 | 0.0002 | |||||
| Positive | 7 d | 0.0383 | |||||
| 1 m | 0.0027 | ||||||
| 3 m | 0.0007 | ||||||
| 6 m | 0.0000 | ||||||
| Material | Colour Scale | Study Time | |||
|---|---|---|---|---|---|
| 7 d | 1 m | 3 m | 6 m | ||
| Biodentine | A | 10 | 10 | 7 | 2 |
| B | 0 | 0 | 3 | 8 | |
| C | 0 | 0 | 0 | 0 | |
| Ortho MTA | A | 10 | 3 | 0 | 0 |
| B | 0 | 0 | 0 | 0 | |
| C | 0 | 7 | 10 | 10 | |
| Retro MTA | A | 10 | 10 | 10 | 10 |
| B | 0 | 0 | 0 | 0 | |
| C | 0 | 0 | 0 | 0 | |
| MTA Plus | A | 10 | 10 | 3 | 1 |
| B | 0 | 0 | 0 | 0 | |
| C | 0 | 0 | 7 | 9 | |
| MTA Repair HP | A | 10 | 10 | 10 | 10 |
| B | 0 | 0 | 0 | 0 | |
| C | 0 | 0 | 0 | 0 | |
| Positive | A | 10 | 9 | 5 | 0 |
| B | 0 | 0 | 0 | 0 | |
| C | 0 | 1 | 5 | 10 | |
| Negative | A | 10 | 10 | 10 | 10 |
| B | 0 | 0 | 0 | 0 | |
| C | 0 | 0 | 0 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Metlerska, J.; Fagogeni, I.; Metlerski, M.; Nowicka, A. Vital Pulp Therapy in Aesthetic Zone-Identifying the Biomaterial That Reduces the Risk of Tooth Discolouration. Materials 2021, 14, 6026. https://doi.org/10.3390/ma14206026
Metlerska J, Fagogeni I, Metlerski M, Nowicka A. Vital Pulp Therapy in Aesthetic Zone-Identifying the Biomaterial That Reduces the Risk of Tooth Discolouration. Materials. 2021; 14(20):6026. https://doi.org/10.3390/ma14206026
Chicago/Turabian StyleMetlerska, Joanna, Irini Fagogeni, Marcin Metlerski, and Alicja Nowicka. 2021. "Vital Pulp Therapy in Aesthetic Zone-Identifying the Biomaterial That Reduces the Risk of Tooth Discolouration" Materials 14, no. 20: 6026. https://doi.org/10.3390/ma14206026
APA StyleMetlerska, J., Fagogeni, I., Metlerski, M., & Nowicka, A. (2021). Vital Pulp Therapy in Aesthetic Zone-Identifying the Biomaterial That Reduces the Risk of Tooth Discolouration. Materials, 14(20), 6026. https://doi.org/10.3390/ma14206026