
miRNA-146a and miRNA-126 as Potential Biomarkers in Patients with Coronary Artery Disease and Generalized Periodontitis

 , , , and
, , , and 
Abstract
1. Introduction
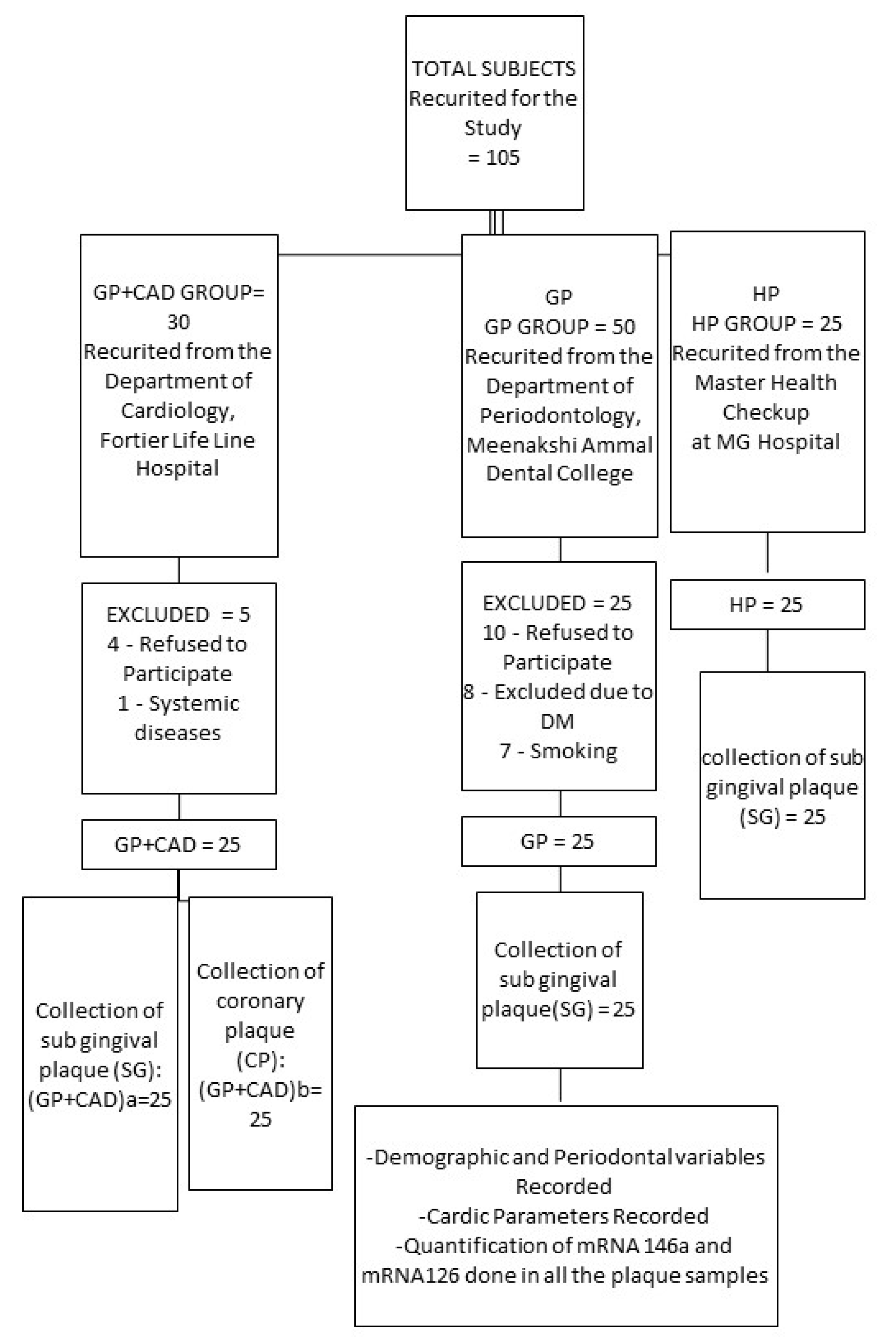
2. Materials and Methods
3. Statistical Analysis
4. Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Luan, X.; Zhou, X.; Naqvi, A.; Francis, M.; Foyle, D.; Nares, S.; Diekwisch, T.G.H. MicroRNAs and immunity in periodontal health and disease. Int. J. Oral Sci. 2018, 10, 24. [Google Scholar] [CrossRef]
- Costa, K.; Câmara, P.; Robbs, B.; Pascoal, A.; Pascoal, V. Possibles Meschanisms Of Action Of MicroRNA In Periodontal Disease. Rev. Bras. Odontol. 2019, 76, 1. [Google Scholar] [CrossRef]
- Mahendra, J.; Mahendra, L.; Felix, J.; Romanos, G. Prevelance of periodontopathogenic bacteria in subgingival biofilm and atherosclerotic plaques of patients undergoing coronary revascularization surgery. J. Indian Soc. Periodontol. 2013, 17, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Malik, R.; Mushtaque, R.S.; Siddiqui, U.A.; Younus, A.; Aziz, M.A.; Humayun, C.; Mansoor, K.; Latif, M.A.; Waheed, S.; Assad, S.; et al. Association Between Coronary Artery Disease and MicroRNA: Literature Review and Clinical Perspective. Cureus 2017, 9, e1188. [Google Scholar] [CrossRef] [PubMed]
- Kebschull, M.; Papapanou, P.N. Mini but mighty: Micro RNAs in the pathobiology of periodontal disease. Periodontology 2000 2015, 69, 201–220. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.-F.; Shu, R.; Jiang, S.-Y.; Liu, D.-L.; Ni, J.; Zhang, X.-L. MicroRNA-146 inhibits pro-inflammatory cytokine secretion through IL-1 receptor-associated kinase 1 in human gingival fibroblasts. J. Inflamm. 2013, 10, 20. [Google Scholar] [CrossRef]
- Sun, X.; Zhang, M.; Sanagawa, A.; Mori, C.; Ito, S.; Iwaki, S.; Satoh, H.; Fujii, S. Circulating microRNA-126 in patients with coronary artery disease: Correlation with LDL cholesterol. Thromb. J. 2012, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- Hansen, T.F.; Christensen, R.d.P.; Andersen, R.F.; Sørensen, F.B.; Johnsson, A.; Jakobsen, A. MicroRNA-126 and epidermal growth factor-like domain 7–an angiogenic couple of importance in metastatic colorectal cancer. Results from the Nordic ACT trial. Br. J. Cancer 2013, 109, 1243–1251. [Google Scholar] [CrossRef]
- Wang, S.; Aurora, A.B.; Johnson, B.A.; Qi, X.; McAnally, J.; Hill, J.A.; Richardson, J.A.; Bassel-Duby, R.; Olson, E.N. The Endothelial-Specific MicroRNA miR-126 Governs Vascular Integrity and Angiogenesis. Dev. Cell 2008, 15, 261–271. [Google Scholar] [CrossRef]
- Ross, R. Atherosclerosis—An Inflammatory Disease. N. Engl. J. Med. 1999, 340, 115–126. [Google Scholar] [CrossRef]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar]
- Fischman, S.L. Current status of indices of plaque. J. Clin. Periodontol. 1986, 13, 371–374. [Google Scholar] [CrossRef] [PubMed]
- Schmittgen, T.D.; Livak, K.J. Analyzing real-time PCR data by the comparative CT method. Nat. Protoc. 2008, 3, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- Oppermann, R.V. An overview of the epidemiology of periodontal diseases in Latin America. Braz. Oral Res. 2007, 21, 8–15. [Google Scholar] [CrossRef]
- Lamon-Fava, S.; Wilson, P.W.; Schaefer, E.J. Impact of body mass index on coronary heart disease risk factors in men and women. The Framingham Offspring Study. Arterioscler. Thromb. Vasc. Biol. 1996, 16, 1509–1515. [Google Scholar] [CrossRef]
- Flint, A.J.; Rexrode, K.M.; Hu, F.B.; Glynn, R.J.; Caspard, H.; Manson, J.E.; Willett, W.C.; Rimm, E.B. Body mass index, waist circumference, and risk of coronary heart disease: A prospective study among men and women. Obes. Res. Clin. Pract. 2010, 4, e171–e181. [Google Scholar] [CrossRef] [PubMed]
- Schultz, W.M.; Kelli, H.M.; Lisko, J.C.; Varghese, T.; Shen, J.; Sandesara, P.; Quyyumi, A.A.; Taylor, H.A.; Gulati, M.; Harold, J.G.; et al. Socioeconomic Status and Cardiovascular Outcomes. Circulation 2018, 137, 2166–2178. [Google Scholar] [CrossRef]
- de Mestral, C.; Stringhini, S. Socioeconomic Status and Cardiovascular Disease: An Update. Curr. Cardiol. Rep. 2017, 19, 115. [Google Scholar] [CrossRef]
- Mattila, K.J.; Nieminen, M.S.; Valtonen, V.V.; Rasi, V.P.; Kesaniemi, Y.A.; Syrjala, S.L.; Jungell, P.S.; Isoluoma, M.; Hietaniemi, K.; Jokinen, M.J. Association between dental health and acute myocardial infarction. BMJ 1989, 298, 779–781. [Google Scholar] [CrossRef]
- Bokhari, S.A.H.; Khan, A.A.; Butt, A.K.; Hanif, M.; Izhar, M.; Tatakis, D.N.; Ashfaq, M. Periodontitis in coronary heart disease patients: Strong association between bleeding on probing and systemic biomarkers. J. Clin. Periodontol. 2014, 41, 1048–1054. [Google Scholar] [CrossRef]
- Tang, K.; Lin, M.; Wu, Y.; Yan, F. Alterations of serum lipid and inflammatory cytokine profiles in patients with coronary heart disease and chronic periodontitis: A pilot study. J. Int. Med. Res. 2011, 39, 238–248. [Google Scholar] [CrossRef]
- Desvarieux, M.; Demmer, R.T.; Jacobs, D.R.; Rundek, T.; Boden-Albala, B.; Sacco, R.L.; Papapanou, P.N. Periodontal bacteria and hypertension: The oral infections and vascular disease epidemiology study (INVEST). J. Hypertens. 2010, 28, 1413–1421. [Google Scholar] [CrossRef]
- Raitoharju, E.; Lyytikäinen, L.-P.; Levula, M.; Oksala, N.; Mennander, A.; Tarkka, M.; Klopp, N.; Illig, T.; Kähönen, M.; Karhunen, P.J.; et al. miR-21, miR-210, miR-34a, and miR-146a/b are up-regulated in human atherosclerotic plaques in the Tampere Vascular Study. Atherosclerosis 2011, 219, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Yagnik, K.; Mahendra, J.; Kurian, V.M. The Periodontal-Cardiovascular alliance: Evaluation of miRNA-146a in subgingival plaque samples of chronic periodontitis patients with and without coronary heart disease. J. Investig. Clin. Dent. 2019, 10, e12442. [Google Scholar] [CrossRef] [PubMed]
- Motedayyen, H.; Ghotloo, S.; Saffari, M.; Sattari, M.; Amid, R. Evaluation of MicroRNA-146a and Its Targets in Gingival Tissues of Patients With Chronic Periodontitis. J. Periodontol. 2015, 86, 1380–1385. [Google Scholar] [CrossRef]
- Wu, Y.; Song, L.-T.; Li, J.-S.; Zhu, D.-W.; Jiang, S.-Y.; Deng, J.-Y. MicroRNA-126 Regulates Inflammatory Cytokine Secretion in Human Gingival Fibroblasts Under High Glucose via Targeting Tumor Necrosis Factor Receptor Associated Factor 6. J. Periodontol. 2017, 88, e179–e187. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Lian, Y.; Wen, X.; Guo, J.; Wang, Z.; Jiang, S.; Hu, Y. Expression of miR-126 and its potential function in coronary artery disease. Afr. Health Sci. 2017, 17, 474–480. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Li, Y.; Zhou, Q.; Pei, C.; Liu, B.; Li, M.; Fang, L.; Sun, Y.; Li, Y.; Meng, S. Hyperglycemia and Advanced Glycation End Products Regulate miR-126 Expression in Endothelial Progenitor Cells. J. Vasc. Res. 2016, 53, 94–104. [Google Scholar] [CrossRef]
- Wu, F.; Yang, Z.; Li, G. Role of specific microRNAs for endothelial function and angiogenesis. Biochem. Biophys. Res. Commun. 2009, 386, 549–553. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Median (I Quartile, III Quartile) | F | P | ||
|---|---|---|---|---|---|
| GP+CAD | GP | HP | |||
| Age(years) | 59.00 | 51.00 | 50.00 | 5.18 | 0.07 NS |
| Height | 166.00 | 164.00 | 163.00 | 0.05 | 0.97 NS |
| Weight | 66.00 | 64.00 | 58.00 | 8.36 | 0.01 |
| BMI (kg/m2) | 24.00 | 24.52 | 21.36 | 8.55 | 0.01 * |
| Income (Rs) | 30,000.00 | 26,000.00 | 30,000.00 | 0.85 | 0.65 NS |
| PI | 2.00 | 2.19 | 0.83 | 49.02 | 0.00 * |
| BOP | 0.64 | 73.90 | 43.80 | 62.78 | 0.00 * |
| PPD(mm) | 6.15 | 6.43 | 2.34 | 50.19 | 0.00 * |
| CAL(mm) | 7.80 | 6.76 | 2.34 | 52.13 | 0.00 * |
| TC (mg/dL) | 176.00 | 172.00 | 175.00 | 0.39 | 0.82 NS |
| HDL (mg/dL) | 32.00 | 53.00 | 52.00 | 29.23 | 0.83 NS |
| LDL (mg/dL) | 90.00 | 97.00 | 97.00 | 0.00 | 0.99 NS |
| TG (mg/dL) | 128.00 | 107.00 | 106.00 | 2.59 | 0.27 NS |
| RBS (mg/dL) | 142.00 | 103.00 | 102.00 | 30.23 | 0.00 * |
| BP(mmHg) | 105.00 | 90.00 | 93.33 | 20.62 | 0.00 * |
| (a) | ||||
|---|---|---|---|---|
| MicroRNA-146a Levels | Mean ± Std Dev | F-Value | p-Value | |
| (GP+CAD)a | 2.55 ± 0.74 | |||
| GP | 2.24 ± 0.54 | |||
| HP | 1.21 ± 0.25 | 39.83 | <0.001 * | |
| (b) | ||||
| Variables | Groups | Mean Difference | p-Value | |
| (GP+CAD)a | GP significance—p < 0.05 | 0.31 | 0.123 NS | |
| MicroRNA-146a | HP | 1.33 | <0.001 * | |
| GP | HP | 1.02 | <0.001 * | |
| (a) | |||||
|---|---|---|---|---|---|
| MicroRNA 126 Levels | Mean ± Std dev | F-Value | p-Value | ||
| (GP+CAD)a | 1.36 ± 0.41 | 60.981 | <0.001 * | ||
| GP | 1.84 ± 0.69 | ||||
| HP | 3.21 ± 0.70 | ||||
| (b) | |||||
| Variables | Groups | Mean Difference | p-Value | ||
| MicroRNA-126 | (GP+CAD)a | GP | −0.48 | 0.19 NS | |
| HP | −1.85 | <0.001 * | |||
| GP | HP | −1.37 | <0.001 * | ||
| (GP+CAD)a (Subgingival Plaque Sample) | (GP+CAD)b | r-Value | p-Value |
|---|---|---|---|
| microRNA-146a | micro RNA-146a | −2.40 | 0.24 NS |
| microRNA-126 | micro RNA-126 | 0.12 | 0.57 NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahendra, J.; Mahendra, L.; Fageeh, H.N.; Fageeh, H.I.; Ibraheem, W.; Abdulkarim, H.H.; Kanakamedala, A.; Prakash, P.; Srinivasan, S.; Balaji, T.M.; et al. miRNA-146a and miRNA-126 as Potential Biomarkers in Patients with Coronary Artery Disease and Generalized Periodontitis. Materials 2021, 14, 4692. https://doi.org/10.3390/ma14164692
Mahendra J, Mahendra L, Fageeh HN, Fageeh HI, Ibraheem W, Abdulkarim HH, Kanakamedala A, Prakash P, Srinivasan S, Balaji TM, et al. miRNA-146a and miRNA-126 as Potential Biomarkers in Patients with Coronary Artery Disease and Generalized Periodontitis. Materials. 2021; 14(16):4692. https://doi.org/10.3390/ma14164692
Chicago/Turabian StyleMahendra, Jaideep, Little Mahendra, Hytham N. Fageeh, Hammam Ibrahim Fageeh, Wael Ibraheem, Hesham H. Abdulkarim, Anilkumar Kanakamedala, Prashanthi Prakash, Sruthi Srinivasan, Thodur Madapusi Balaji, and et al. 2021. "miRNA-146a and miRNA-126 as Potential Biomarkers in Patients with Coronary Artery Disease and Generalized Periodontitis" Materials 14, no. 16: 4692. https://doi.org/10.3390/ma14164692
APA StyleMahendra, J., Mahendra, L., Fageeh, H. N., Fageeh, H. I., Ibraheem, W., Abdulkarim, H. H., Kanakamedala, A., Prakash, P., Srinivasan, S., Balaji, T. M., Varadarajan, S., Jagannathan, R., & Patil, S. (2021). miRNA-146a and miRNA-126 as Potential Biomarkers in Patients with Coronary Artery Disease and Generalized Periodontitis. Materials, 14(16), 4692. https://doi.org/10.3390/ma14164692