Physical Properties, Antimicrobial Activity and In Vivo Tissue Response to Apexit Plus

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Physical Analyses
2.1.1. Flow
2.1.2. Radiopacity
2.1.3. Setting Time
2.2. Solubility
2.3. Biological Properties
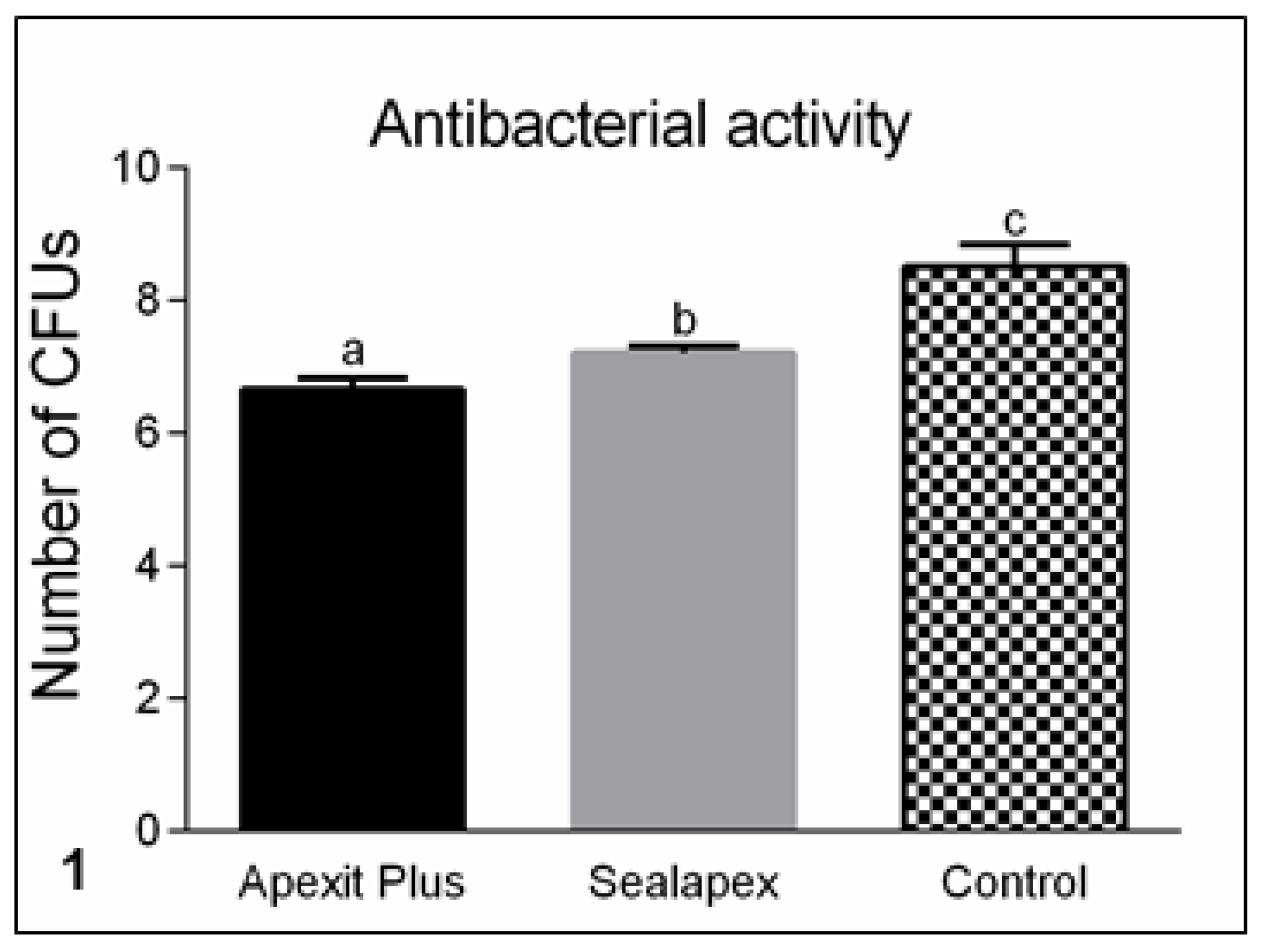
2.3.1. Antimicrobial Activity
2.3.2. Animal Experimental Procedures
2.3.3. Histological Analysis and Numerical Density of Inflammatory Cells
2.3.4. Quantification of Collagen Fibers
2.3.5. Von Kossa Histochemical Reaction
2.3.6. Von Kossa Method Combined with Immunohistochemical Detection of Alkaline Phosphatase
2.4. Statistical Analysis
3. Results
3.1. Physical Analyses
3.1.1. Flow and Radiopacity Analyses
3.1.2. Setting Time and Solubility
3.2. Biological Properties
3.2.1. Antimicrobial Activity
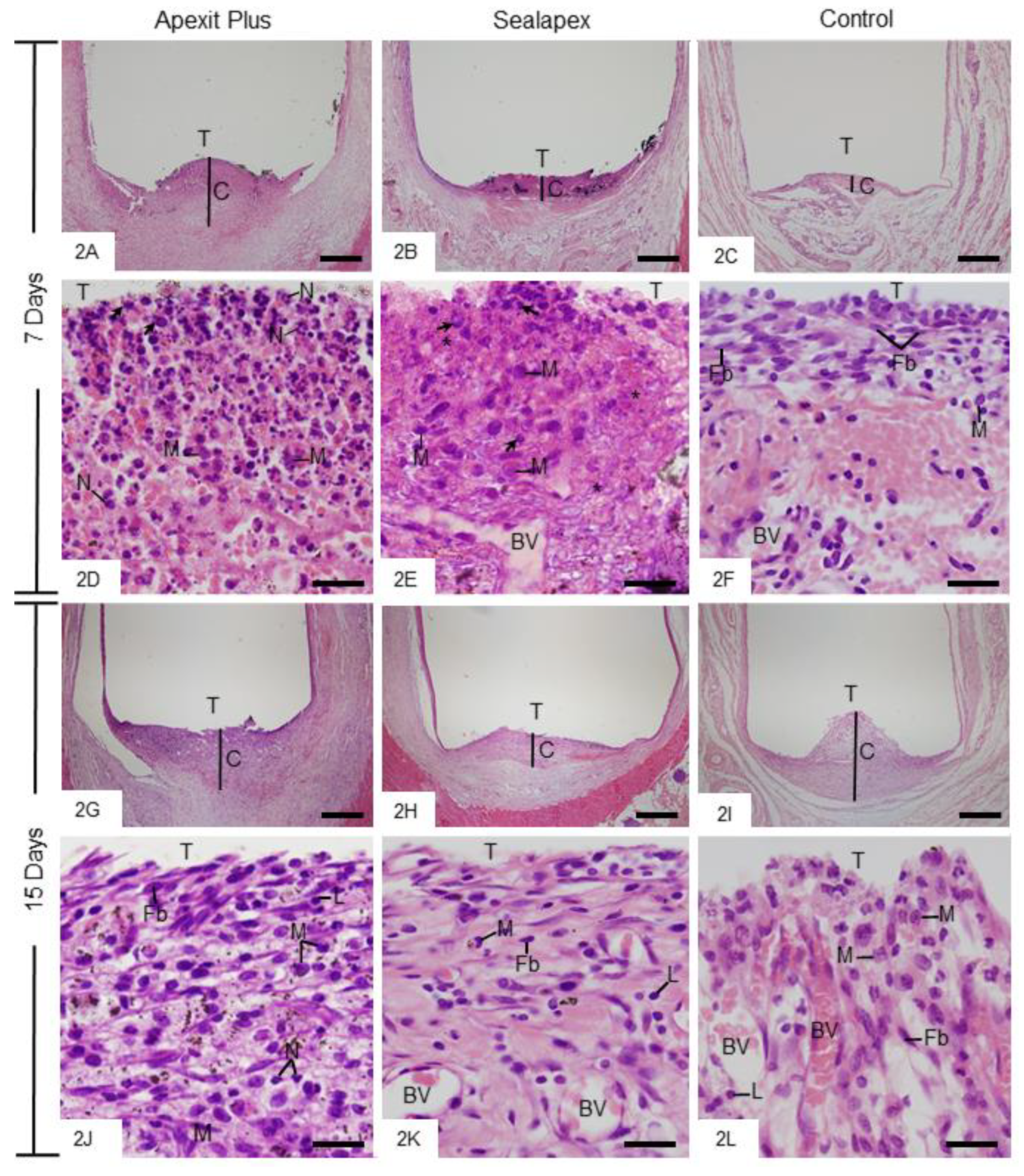
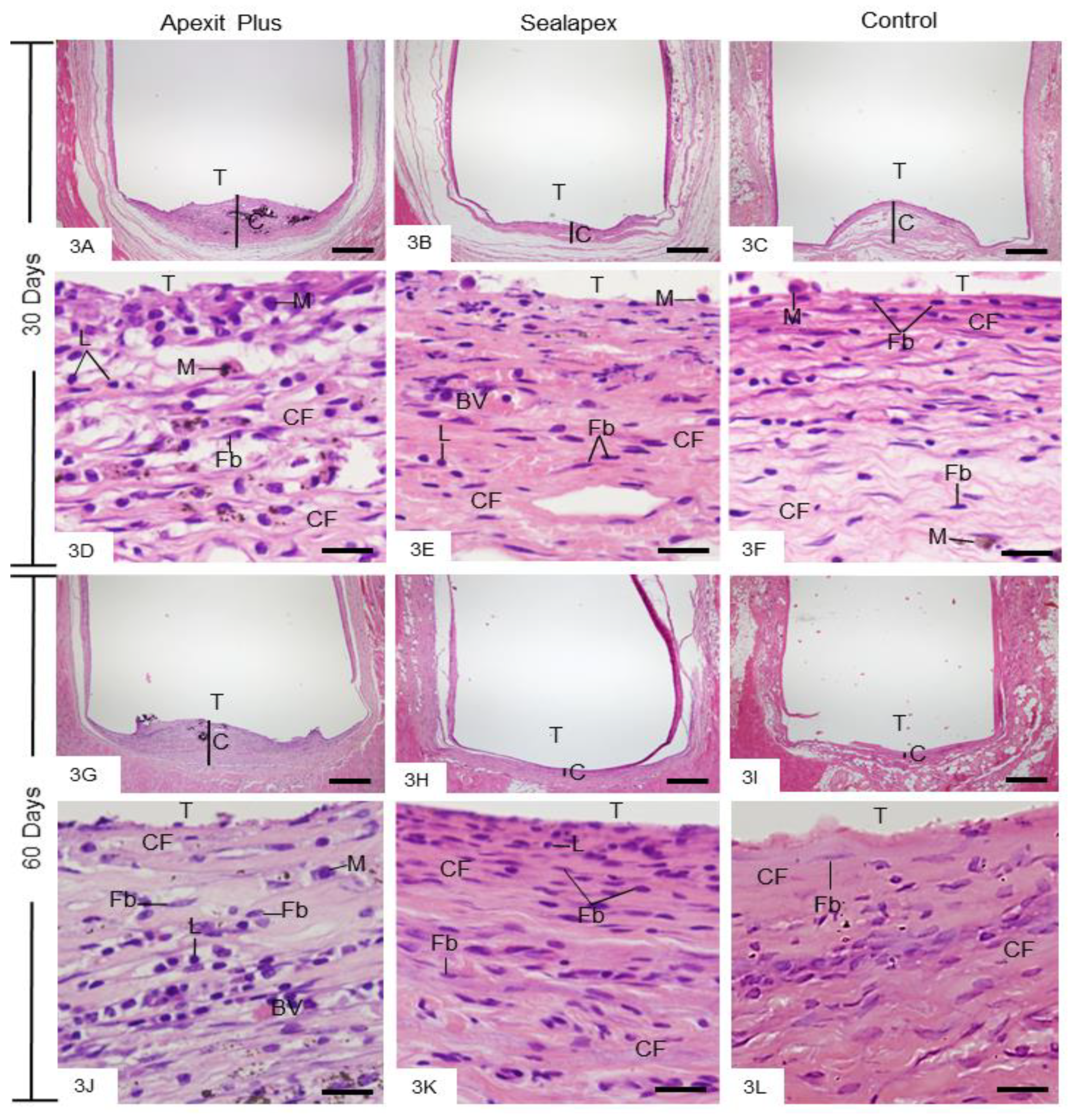
3.2.2. Morphological Analysis and Numerical Density of Inflammatory Cells
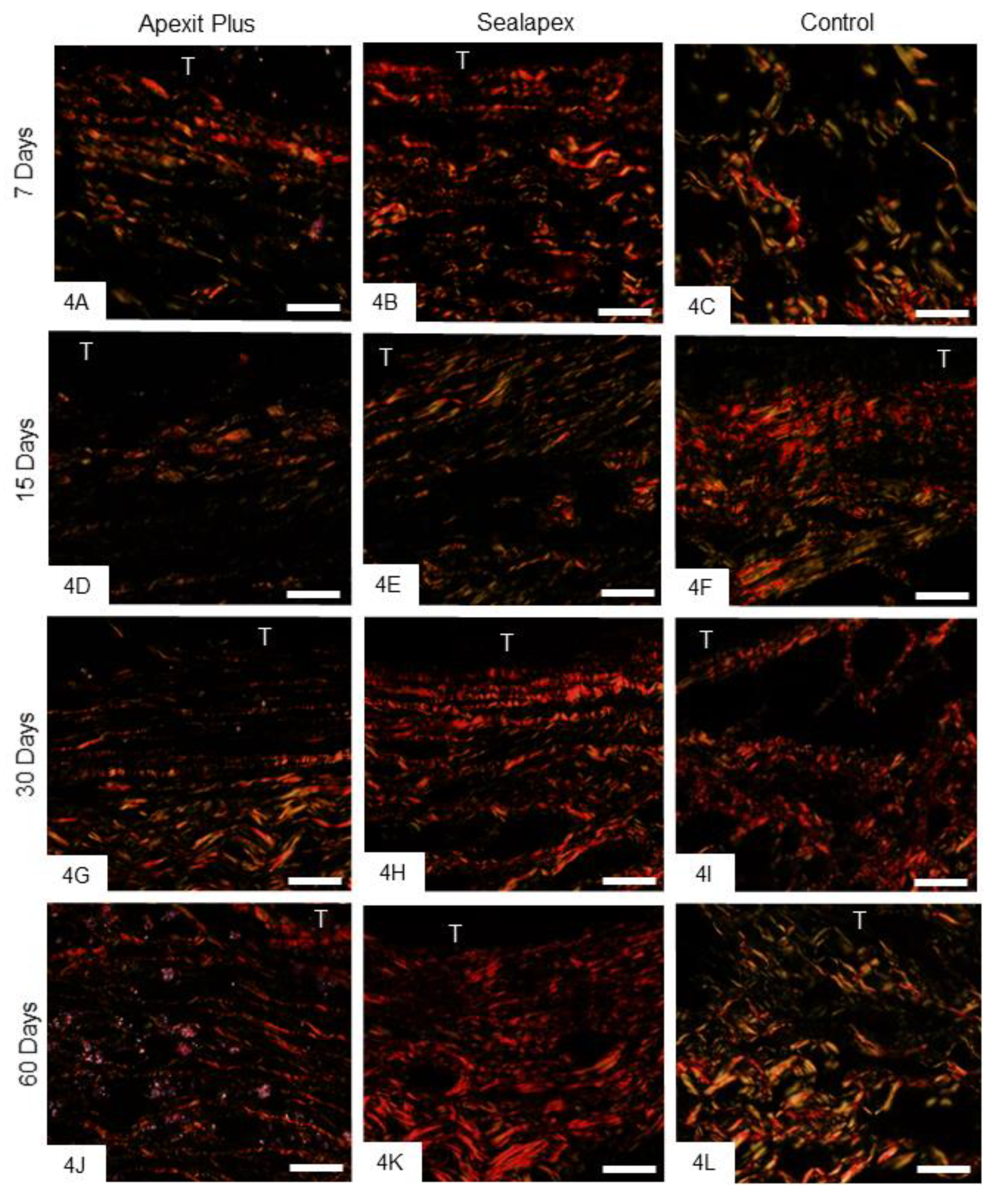
3.2.3. Birefringent Collagen
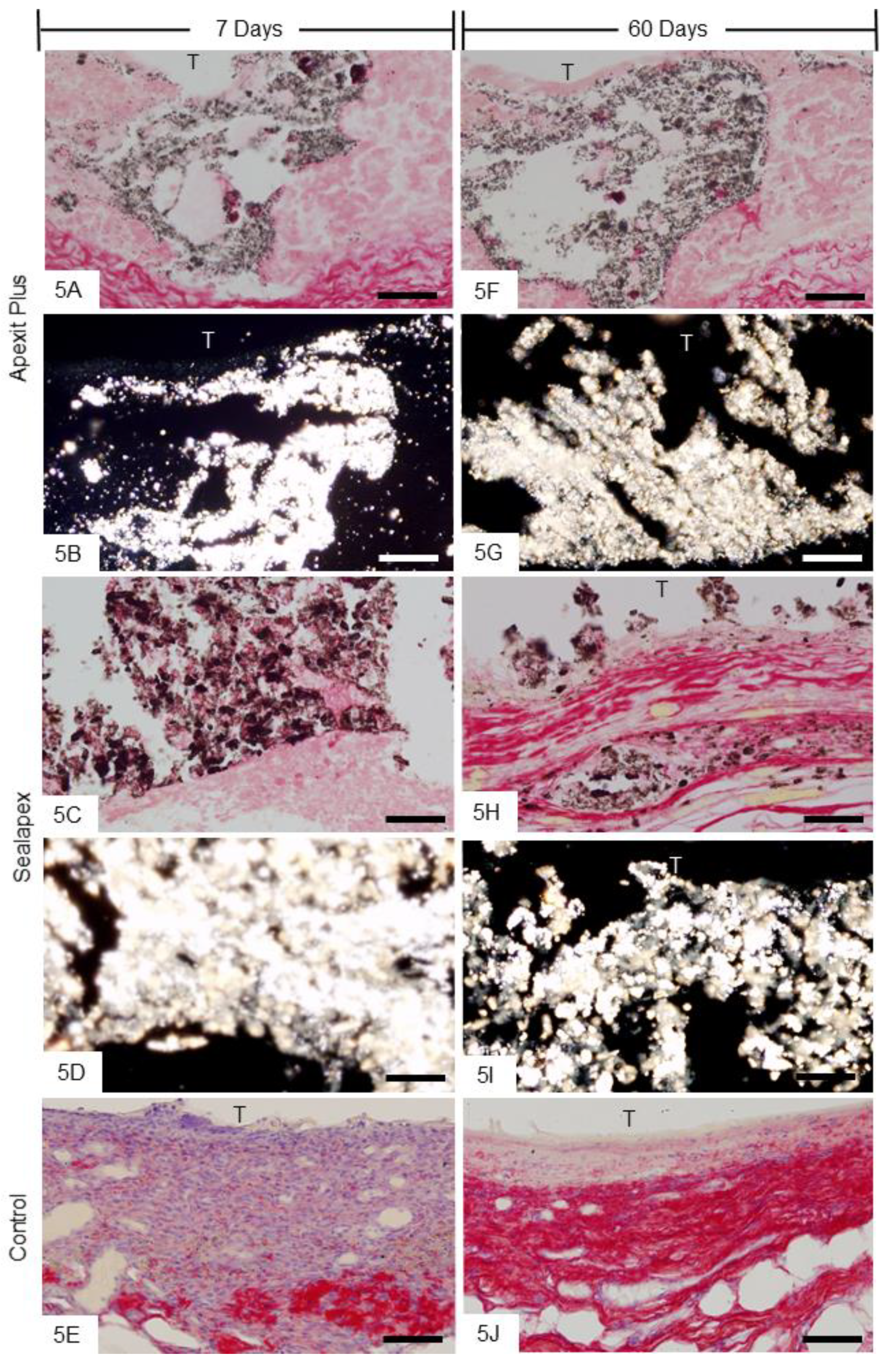
3.2.4. Von Kossa Histochemical Method and Analysis under Polarized Light Microscope
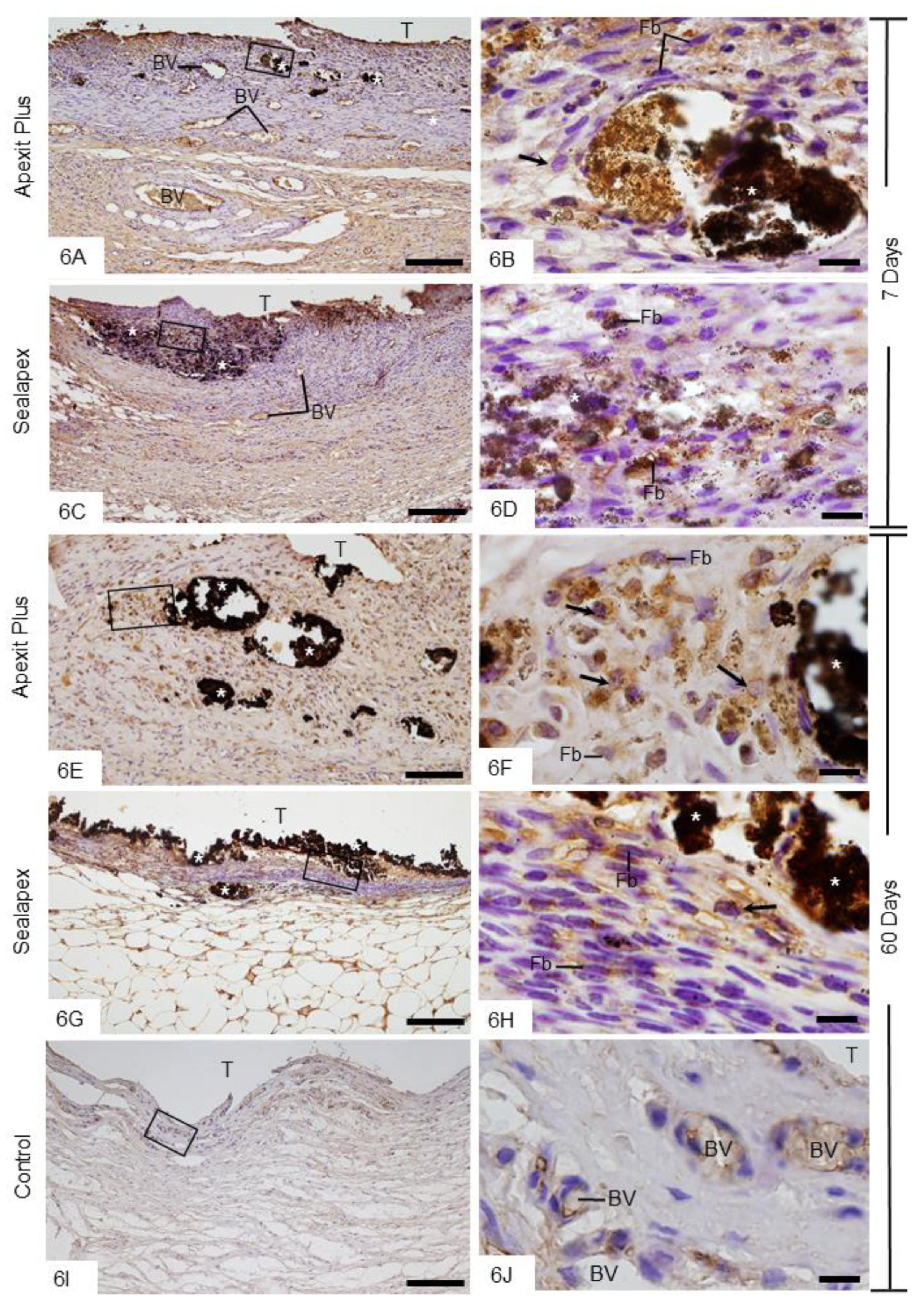
3.2.5. Von Kossa Method Combined with Immunohistochemical Detection of ALP
4. Discussion
4.1. Physical Properties
4.2. Biological Properties
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethical Approval
References
- Rezende, G.C.; Massunari, L.; Queiroz, I.O.; Gomes-Filho, J.E.; Jacinto, R.C.; Lodi, C.S.; Dezan-Junior, E. Antimicrobial action of calcium hydroxide-based endodontic sealers after setting, against E. faecalis biofilm. Braz. Oral Res. 2016, 30, e38. [Google Scholar] [CrossRef]
- Poggio, C.; Trovati, F.; Ceci, M.; Colombo, M.; Pietrocola, G. Antibacterial activity of different root canal sealers against Enterococcus faecalis. J. Clin. Exp. Dent. 2017, 1, e743–e748. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ballullaya, S.V.; Vinay, V.; Thumu, J.; Devalla, S.; Bollu, I.P.; Balla, S. Stereomicroscopic dye Leakage measurement of six different root canal sealers. J. Clin. Diag. Res. 2017, 11, 65–68. [Google Scholar] [CrossRef]
- Pawinska, M.; Szczurko, G.; Kierklo, A.; Sidun, J. A laboratory study evaluating the pH of various modern root canal filling materials. Adv. Clin. Exp. Med. 2017, 26, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Bueno, C.R.; Valentim, D.; Marques, V.A.; Gomes-Filho, J.E.; Cintra, L.T.; Jacinto, R.C.; Dezan-Junior, E. Biocompatibility and biomineralization assessment of bioceramic-, epoxy-, and calcium hydroxide-based sealers. Braz. Oral Res. 2016, 14, e81. [Google Scholar] [CrossRef] [PubMed]
- Marín-Bauza, G.A.; Silva-Sousa, Y.T.; da Cunha, S.A.; Rached-Junior, F.J.; Bonetti-Filho, I.; Sousa-Neto, M.D.; Miranda, C.E. Physicochemical properties of endodontic sealers of different bases. J. Appl. Oral Sci. 2012, 20, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Schafer, E.; Zandbiglari, T. Solubility of root-canal sealers in water and artificial saliva. Int. Endod. J. 2003, 36, 660–669. [Google Scholar] [CrossRef]
- Borges, R.P.; Sousa-Neto, M.D.; Versiani, M.A.; Rached-Junior, F.A.; De-Deus, G.; Miranda, C.E.; Pecora, J.D. Changes in the surface of four calcium silicate-containing endodontic materials and an epoxy resin-based sealer after a solubility test. Int. Endod. J. 2012, 45, 419–428. [Google Scholar] [CrossRef]
- Szczurko, G.; Pawinska, M.; Luczaj-Cepowicz, E.; Kierklo, A.; Marczuk-Kolada, G.; Holownia, A. Effect of root canal sealers on human periodontal ligament fibroblast viability: Ex vivo study. Odontology 2018, 106, 245–256. [Google Scholar] [CrossRef]
- Konjhodzic-Prcic, A.; Jakupovic, S.; Hasic-Brankovic, L.; Vukovic, A. Evaluation of biocompatibility of root canal sealers on L929 fibroblasts with Multiscan EX Spectrophotometer. Acta Inform. Med. 2015, 23, 135–137. [Google Scholar] [CrossRef]
- Vanapatla, A.; Vemisetty, H.; Punna, R.; Veeramachineni, C.; Venkata, R.P.; Muppala, J.N.; Dandolu, R. Comparative evaluation of antimicrobial effect of three endodontic sealers with and without antibiotics—An in vitro study. J. Clin. Diag. Res. 2016, 10, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Slutzky-Goldberg, I.; Slutzky, H.; Solomonov, M.; Moshonov, M.; Weiss, E.I.; Matalon, S. Antibacterial properties of four endodontic sealers. J. Endod. 2008, 34, 735–738. [Google Scholar] [CrossRef] [PubMed]
- International Organization for Standardization. Biological Evaluation of Medical Devices. Part 6: Tests for Local Effects after Implantation; ISO: Geneva, Switzerland, 2016; pp. 10993–10996. [Google Scholar]
- Gomes-Filho, J.E.; Bernabé, P.F.; Nery, M.J. Reaction of rat connective tissue to a new calcium hydroxide-based sealer. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2008, 106, e71–e76. [Google Scholar] [CrossRef] [PubMed]
- Viola, N.V.; Guerreiro-Tanomaru, J.M.; da Silva, G.F.; Sasso-Cerri, E.; Tanomaru-Filho, M.; Cerri, P.S. Biocompatibility of an experimental MTA sealer implanted in the rat subcutaneous: Quantitative and immunohistochemical evaluation. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 1773–1781. [Google Scholar] [CrossRef]
- Silva, G.F.; Bosso, R.; Ferino, R.V.; Tanomaru-Filho, M.; Bernardi, M.I.; Guerreiro-Tanomaru, J.M.; Cerri, P.S. Microparticulated and nanoparticulated zirconium oxide added to calcium silicate cement: Evaluation of physicochemical and biological properties. J. Biomed. Mater. Res. A 2014, 102, 4336–4345. [Google Scholar] [CrossRef]
- Holtz, K.M.; Kantrowitz, E.R. The mechanism of the alkaline phosphatase reaction: Insights from NMR, crystallography and site-specific mutagenesis. FEBS Letters. 1999, 462, 7–11. [Google Scholar] [CrossRef]
- Golub, E.E.; Boesze-Battaglia, K. The role of alkaline phosphatase in mineralization. Curr. Opi. Orthop. 2007, 18, 444–448. [Google Scholar] [CrossRef]
- Dental Root Canal Sealing Materials; International Standards Organization: Geneva, Switzerland, 2012; ISO 6876.
- Laboratory Testing Methods: Endodontic Filling and Sealing Materials; American National Standard Institute/America Dental Association: Chicago, IL, USA, 2000; ANSI/ADA 57.
- Hungaro-Duarte, M.A.; de Oliveira, E.; Kadre, G.D.; Vivan, R.R.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; de Moraes, I.G. Radiopacity of portland cement associated with different radiopacifying agents. J. Endod. 2009, 35, 737–740. [Google Scholar] [CrossRef]
- Standard Test Method for Time and Setting of Hydraulic-Cement Paste; ASTM: West Conshohocken, PA, USA, 2000.
- Mendes, A.T.; Silva, P.B.D.; Só, B.B.; Hashizume, L.N.; Vivan, R.R.; Rosa, R.A.D.; Duarte, M.A.H.; Só, M.V.R. Evaluation of physicochemical properties of new calcium silicate-based sealer. Braz. Dent. J. 2018, 29, 536–540. [Google Scholar] [CrossRef]
- Arias-Moliz, M.T.; Ruiz-Linares, M.; Cassar, G.; Ferrer-Lugue, C.M.; Baca, P.; Ordinola-Zapata, R.; Camilleri, J. The effect of benzalkonium chloride additions to AH Plus sealer. Antimicrobial, physical and chemical properties. J. Dent. 2015, 43, 846–854. [Google Scholar] [CrossRef]
- Silva, G.F.; Tanomaru-Filho, M.; Bernardi, M.I.; Guerreiro-Tanomaru, J.M.; Cerri, P.S. Niobium pentoxide as radiopacifying agent of calcium silicate-based material: Evaluation of physicochemical and biological properties. Clin. Oral Investig. 2015, 19, 2015–2025. [Google Scholar] [CrossRef] [PubMed]
- Saraiva, J.A.; da Fonseca, T.S.; da Silva, G.F.; Sasso-Cerri, E.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Cerri, P.S. Reduced interleukin-6 immunoexpression and birefringent collagen formation indicate that MTA Plus and MTA Fillapex are biocompatible. Biomed. Mater. 2018, 20, 035002. [Google Scholar] [CrossRef] [PubMed]
- Benetti, F.; Gomes-Filho, J.E.; de Araujo Lopes, J.M.; Barbosa, J.G.; Jacinto, R.C.; Cintra, L.T.A. In vivo biocompatibility and biomineralization of calcium silicate cements. Eur. J. Oral Sci. 2018, 126, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Laghios, C.D.; Benson, B.W.; Gutmann, J.L.; Cutler, C.W. Comparative radiopacity of tetracalcium phosphate and other root-end filling materials. Int. Endod. J. 2000, 33, 311–315. [Google Scholar] [CrossRef]
- Xuereb, M.; Vella, P.; Damidot, D.; Sammut, C.V.; Camilleri, J. In situ assessment of the setting of tricalcium silicate-based sealers using a dentin pressure model. J. Endod. 2015, 41, 111–124. [Google Scholar] [CrossRef]
- Cañadas, P.S.; Berástegui, E.; Gaton-Hernández, P.; Silva, L.A.; Leite, G.A.; Silva, R.S. Physicochemical properties and interfacial adaptation of root canal sealers. Braz. Dent. J. 2014, 25, 435–441. [Google Scholar] [CrossRef]
- Ørstavik, D.; Nordahl, I.; Tibballs, J.E. Dimensional change following setting of root canal sealer materials. Dent. Mater. 2001, 17, 512–519. [Google Scholar] [CrossRef]
- Caicedo, R.; von Fraunhofer, J.A. The properties of endodontic sealer cements. J. Endod. 1988, 14, 527–534. [Google Scholar] [CrossRef]
- Viapiana, R.; Flumignan, D.L.; Guerreiro-Tanomaru, J.M.; Camilleri, J.; Tanomaru-Filho, M. Physicochemical and mechanical properties of zirconium oxide and niobium oxide modified Portland cement-based experimental endodontic sealers. Int. Endod. J. 2014, 47, 437–448. [Google Scholar] [CrossRef]
- Guerreiro-Tanomaru, J.M.; Morgental, R.D.; Flumignan, D.L.; Gasparini, F.; Oliveira, J.E.; Tanomaru-Filho, M. Evaluation of pH, available chlorine content, and antibacterial activity of endodontic irrigants and their combinations against Enterococcus faecalis. Oral Sur. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 112, 132–135. [Google Scholar] [CrossRef]
- Vazquez-Garcia, F.; Tanomaru-Filho, M.; Chávez-Andrade, G.M.; Bosso-Martelo, R.; Basso-Bernardi, M.I.; Guerreiro-Tanomaru, J.M. Effect of silver nanoparticles on physicochemical and antibacterial properties of calcium silicate cements. Braz. Dent. J. 2016, 27, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Zordan-Bronzel, C.L.; Tanomaru-Filho, M.; Rodrigues, E.M.; Chávez-Andrade, G.M.; Faria, G.; Guerreiro-Tanomaru, J.M. Cytocompatibility, bioactive potential and antimicrobial activity of an experimental calcium silicated-based endodontic sealer. Int. Endod. J. 2019, 31, 1–8. [Google Scholar]
- Kim, R.J.; Shin, J.H. Cytotoxicity of a novel mineral trioxide aggregate-based root canal sealer. Dent. Mater. J. 2014, 33, 313–318. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Martinho, F.C.; Camargo, S.E.A.; Fernandes, A.M.M.; Campos, M.S.; Prado, R.F.; Camargo, C.H.R.; Valera, M.C. Comparison of cytotoxicity, genotoxicity and immunological inflammatory biomarker activity of several endodontic sealers against immortalized human pulp cells. Int. Endod. J. 2018, 51, 41–57. [Google Scholar] [CrossRef] [PubMed]
- Silva, G.F.; Guerreiro-Tanomaru, J.M.; da Fonseca, T.S.; Bernardi, M.I.B.; Sasso-Cerri, E.; Tanomaru-Filho, M.; Cerri, P.S. Zirconium oxide and niobium oxide used as radiopacifiers in a calcium silicate-based material stimulate fibroblast proliferation and collagen formation. Int. Endod. J. 2017, 50 (Suppl. 2), e95–e108. [Google Scholar] [CrossRef]
- Gandolfi, M.G.; Taddei, P.; Modena, E.; Siboni, F.; Prati, C. Biointeractivity-related versus chemi/physisorption-related apatite precursor-forming ability of current root end filling materials. J. Biomed. Mater. Res. B Appl. Biomater. 2013, 101, 1107–1123. [Google Scholar] [CrossRef]
- Chang, S.W.; Lee, S.Y.; Kang, S.K.; Kum, K.Y.; Kim, E.C. In vitro biocompatibility, inflammatory response, and osteogenic potential of 4 root canal sealers: Sealapex, Sankin apatite root sealer, MTA Fillapex, and iRoot SP root canal sealer. J. Endod. 2014, 40, 1642–1648. [Google Scholar] [CrossRef]
- Gallo, R.L.; Dorschner, R.A.; Takashima, S.; Klagsbrun, M.; Eriksson, E.; Bernfield, M. Endothelial cell surface alkaline phosphatase activity is induced by IL-6 released during wound repair. J. Investig. Dermatol. 1997, 109, 597–603. [Google Scholar] [CrossRef][Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sealers | Flow Test | Radiopacity |
|---|---|---|
| Apexit Plus | 25.69 ± 1.12 a | 3.44 ± 0.32 a |
| Sealapex | 20.93 ± 1.12 b | 6.82 ± 0.68 b |
| Sealers | Setting Time | Solubility |
|---|---|---|
| Initial Final | Final (%) | |
| Apexit Plus | 298 ± 13.51 a 1062 ± 17.62 a | −1.333 ± 0.2364 a |
| Sealapex | 1181 ± 14.32 b 1268 ± 22.80 b | −6.952 ± 1.302 b |
| Apexit Plus | Sealapex | Control | ||
|---|---|---|---|---|
| 7 days | ICs BC | 580 ± 145 a;1 27.4 ± 2.4 a;1 | 425 ± 71 b;1 32.5 ± 1.8 b;1 | 327 ± 45 c;1 30.0 ± 1.7 ab;1 |
| 15 days | ICs BC | 445 ± 35 a;2 28.6±1.4 a;1 | 377 ± 38 a;1 35.7 ± 5.3 b;1 | 181 ± 30 b;2 39.3 ± 3.0 b;2 |
| 30 days | ICs BC | 413 ± 30 a;2 32.0 ± 2.3 a;2 | 322 ± 32 a;1 44.6 ± 5.5 b;2 | 156 ± 30 b;2 42.6 ± 2.7 b;2 |
| 60 days | ICs BC | 300 ± 31 a;3 34.0 ± 1.2 a;2 | 204 ± 21 a;2 49.1 ± 4.7 b;2 | 93 ± 45 b;2 54.2 ± 3.8 b;3 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoshino, R.A.; Silva, G.F.d.; Delfino, M.M.; Guerreiro-Tanomaru, J.M.; Tanomaru-Filho, M.; Sasso-Cerri, E.; Bonetti Filho, I.; Cerri, P.S. Physical Properties, Antimicrobial Activity and In Vivo Tissue Response to Apexit Plus. Materials 2020, 13, 1171. https://doi.org/10.3390/ma13051171
Hoshino RA, Silva GFd, Delfino MM, Guerreiro-Tanomaru JM, Tanomaru-Filho M, Sasso-Cerri E, Bonetti Filho I, Cerri PS. Physical Properties, Antimicrobial Activity and In Vivo Tissue Response to Apexit Plus. Materials. 2020; 13(5):1171. https://doi.org/10.3390/ma13051171
Chicago/Turabian StyleHoshino, Roberto Alameda, Guilherme Ferreira da Silva, Mateus Machado Delfino, Juliane Maria Guerreiro-Tanomaru, Mario Tanomaru-Filho, Estela Sasso-Cerri, Idomeo Bonetti Filho, and Paulo Sérgio Cerri. 2020. "Physical Properties, Antimicrobial Activity and In Vivo Tissue Response to Apexit Plus" Materials 13, no. 5: 1171. https://doi.org/10.3390/ma13051171
APA StyleHoshino, R. A., Silva, G. F. d., Delfino, M. M., Guerreiro-Tanomaru, J. M., Tanomaru-Filho, M., Sasso-Cerri, E., Bonetti Filho, I., & Cerri, P. S. (2020). Physical Properties, Antimicrobial Activity and In Vivo Tissue Response to Apexit Plus. Materials, 13(5), 1171. https://doi.org/10.3390/ma13051171