Temperature Threshold Values of Bone Necrosis for Thermo-Explantation of Dental Implants—A Systematic Review on Preclinical In Vivo Research

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Focused Question
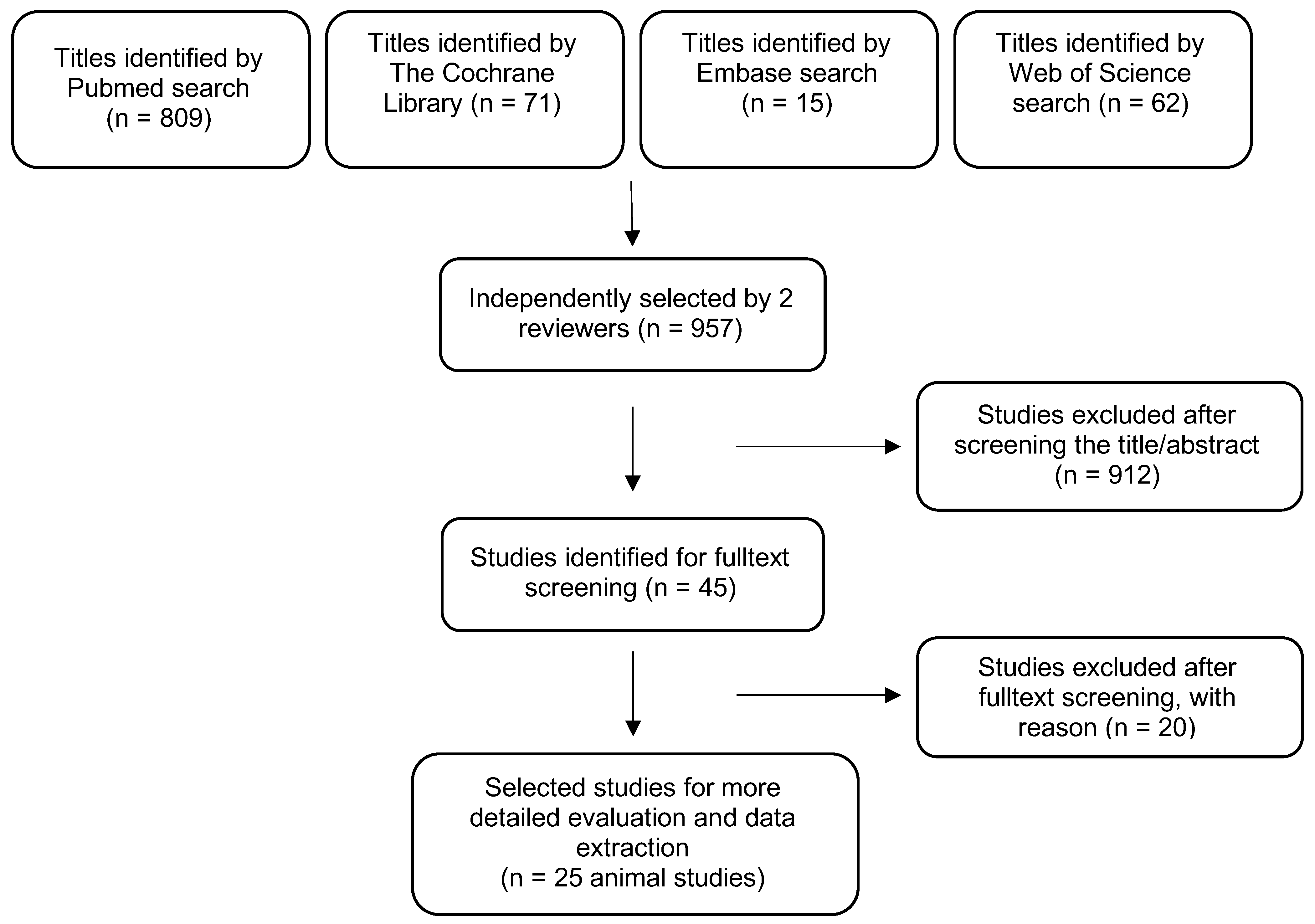
2.2. Search Strategy
2.3. Inclusion Criteria
- (1)
- In vivo animal studies
- (2)
- Studies investigating thermal bone damage by histopathology
- (3)
- Studies at all levels of evidence, except case reports and expert opinion
- (4)
- Studies reporting on at least one of the outcome measures
- (5)
- Language: German or English
2.4. Exclusion Criteria
2.5. Selection of Studies
2.6. Data Extraction
2.7. Parameters Were Classified as Follows
- (1)
- Temperature and exposure time leading to bone damage
- (2)
- Laser settings producing bone damage
- (3)
- Bone-to-implant contact ratio (BIC) around implants after thermal treatment
- (4)
- Infrabony implant pockets after thermal treatment
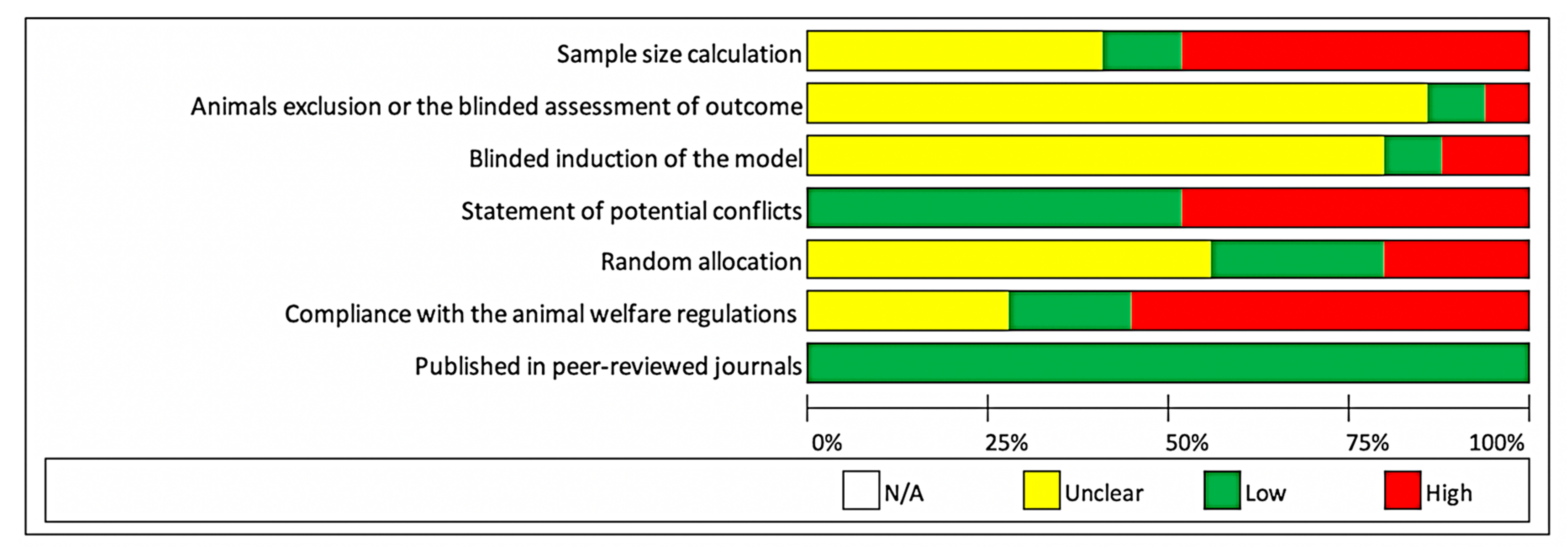
2.8. Risk of Bias in Individual Studies
2.9. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Temperature and Exposure Time Leading to Bone Damage
3.3. Laser Settings Producing Bone Damage
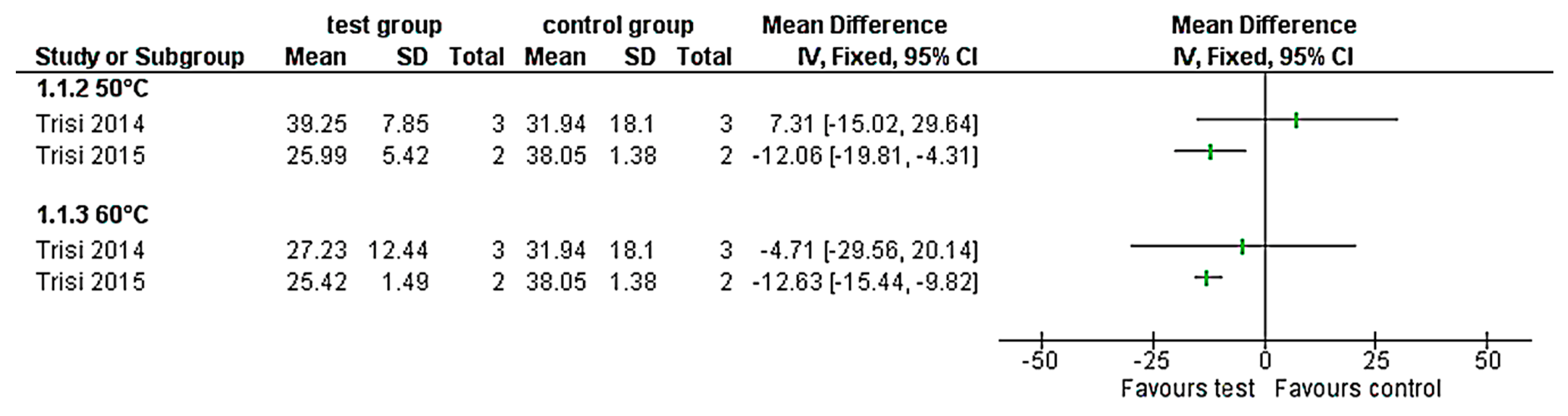
3.4. BIC around Implants after Thermal Treatment
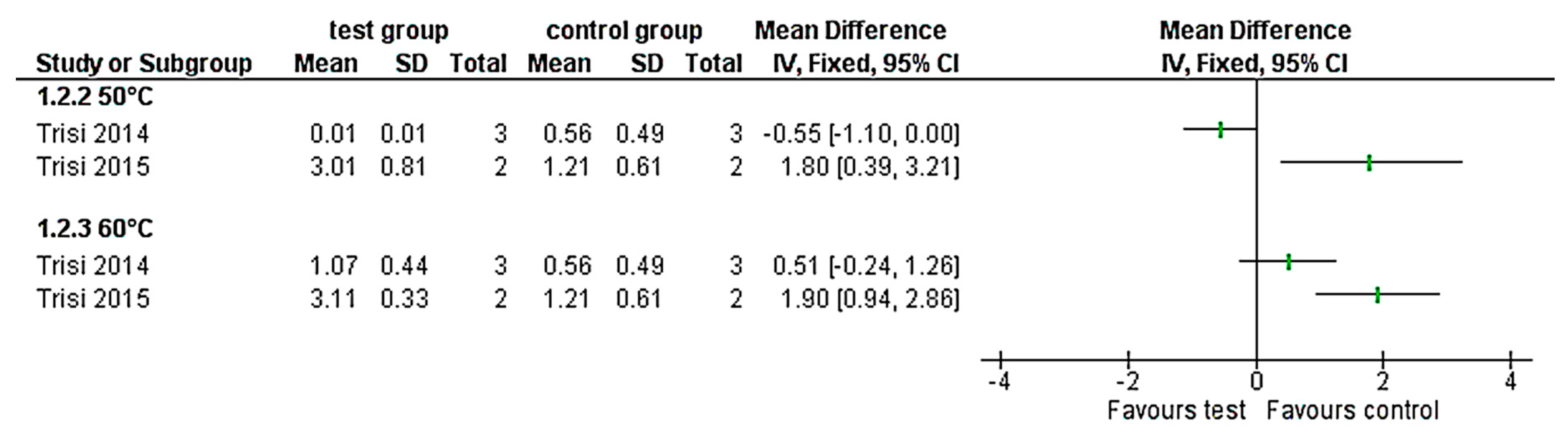
3.5. Infrabony Implant Pockets after Thermal Treatment
3.6. Risk of Bias in Individual Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Berman, A.T.; Reid, J.S.; Yanicko, D.R.; Sih, G.C.; Zimmerman, M.R. Thermally induced bone necrosis in rabbits. Relation to implant failure in humans. Clin. Orthop. Relat. Res. 1984, 284–292. [Google Scholar] [CrossRef]
- Goetz, J.E.; Robinson, D.A.; Pedersen, D.R.; Conzemius, M.G.; Brown, T.D. Cryoinsult parameter effects on the histologically apparent volume of experimentally induced osteonecrotic lesions. J. Orthop. Res. 2011, 29, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Goetz, J.E.; Pedersen, D.R.; Robinson, D.A.; Conzemius, M.G.; Baer, T.E.; Brown, T.D. The apparent critical isotherm for cryoinsult-induced osteonecrotic lesions in emu femoral heads. J. Biomech. 2008, 41, 2197–2205. [Google Scholar] [CrossRef] [PubMed]
- Paiva, K.B.S.; Granjeiro, J.M. Matrix Metalloproteinases in Bone Resorption, Remodeling, and Repair. Prog. Mol. Biol. Transl. Sci. 2017, 148, 203–303. [Google Scholar] [PubMed]
- Tawy, G.F.; Rowe, P.J.; Riches, P.E. Thermal Damage Done to Bone by Burring and Sawing With and Without Irrigation in Knee Arthroplasty. J. Arthroplast. 2016, 31, 1102–1108. [Google Scholar] [CrossRef] [PubMed]
- Fugito Junior, K.; Cortes, A.R.; de Carvalho Destro, R.; Yoshimoto, M. Comparative Study on the Cutting Effectiveness and Heat Generation of Rotary Instruments Versus Piezoelectric Surgery Tips Using Scanning Electron Microscopy and Thermal Analysis. Int. J. Oral Maxillofac. Implant. 2018, 33, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, A.; Sivolella, S.; Stocco, E.; Favero, V.; Stellini, E. Experimental Analysis of Temperature Differences During Implant Site Preparation: Continuous Drilling Technique Versus Intermittent Drilling Technique. J. Oral Implantol. 2018, 44, 46–50. [Google Scholar] [CrossRef]
- Piattelli, A.; Piattelli, M.; Mangano, C.; Scarano, A. A histologic evaluation of eight cases of failed dental implants: Is bone overheating the most probable cause? Biomaterials 1998, 19, 683–690. [Google Scholar] [CrossRef]
- Massei, G.; Szmukler-Moncler, S. Thermo-explantation. a novel approach to remove osseointegrated implants. Eur. Cells Mater. 2004, 7 (Suppl. 2), 48. [Google Scholar]
- Cunliffe, J.; Barclay, C. Removal of a dental implant: An unusual case report. J. Dent. Implant. 2011, 1, 22–25. [Google Scholar] [CrossRef]
- Worni, A.; Marchand, L.; Sailer, I.; Cornish, D.; Hicklin, S.P. Explantation of an Osseointegrated Titanium Implant Using Laser-Induced Thermo-necrosis: A Case Report. Int. J. Oral Maxillofac. Implant. 2018, 33, e151–e155. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, A.R.; Albrektsson, T. Temperature threshold levels for heat-induced bone tissue injury: A vital-microscopic study in the rabbit. J. Prosthet. Dent. 1983, 50, 101–107. [Google Scholar] [CrossRef]
- Eriksson, R.A.; Albrektsson, T. The effect of heat on bone regeneration: An experimental study in the rabbit using the bone growth chamber. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 1984, 42, 705–711. [Google Scholar] [CrossRef]
- Eriksson, R.A.; Albrektsson, T.; Magnusson, B. Assessment of bone viability after heat trauma. A histological, histochemical and vital microscopic study in the rabbit. Scand. J. Plast. Reconstr. Surg. 1984, 18, 261–268. [Google Scholar] [CrossRef]
- Stubinger, S.; Ghanaati, S.; Saldamli, B.; Kirkpatrick, C.J.; Sader, R. Er:YAG laser osteotomy: Preliminary clinical and histological results of a new technique for contact-free bone surgery. Eur. Surg. Res. 2009, 42, 150–156. [Google Scholar] [CrossRef]
- De Cremer, K.; Braem, A.; Gerits, E.; De Brucker, K.; Vandamme, K.; Martens, J.A.; Michiels, J.; Vleugels, J.; Cammue, B.P.; Thevissen, K. Controlled release of chlorhexidine from a mesoporous silica-containing macroporous titanium dental implant prevents microbial biofilm formation. Eur. Cell. Mater. 2017, 33, 13–27. [Google Scholar] [CrossRef]
- Trisi, P.; Berardini, M.; Falco, A.; Vulpiani, M.P. Effect of temperature on the dental implant osseointegration development in low-density bone: An in vivo histological evaluation. Implant. Dent. 2015, 24, 96–100. [Google Scholar] [CrossRef]
- Trisi, P.; Berardini, M.; Falco, A.; Vulpiani, M.P.; Masciotra, L. Effect of 50 to 60 degrees C heating on osseointegration of dental implants in dense bone: An in vivo histological study. Implant. Dent. 2014, 23, 516–521. [Google Scholar] [CrossRef][Green Version]
- Rayan, G.M.; Pitha, J.V.; Edwards, J.S.; Everett, R.B. Effects of CO2 laser beam on cortical bone. Lasers. Surg. Med. 1991, 11, 58–61. [Google Scholar] [CrossRef]
- Mohlhenrich, S.C.; Modabber, A.; Steiner, T.; Mitchell, D.A.; Holzle, F. Heat generation and drill wear during dental implant site preparation: Systematic review. Br. J. Oral Maxillofac. Surg. 2015, 53, 679–689. [Google Scholar] [CrossRef]
- Clattenburg, R.; Cohen, J.; Conner, S.; Cook, N. Thermal properties of cancellous bone. J. Biomed. Mater. Res. 1975, 9, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Leunig, M.; Hertel, R. Thermal necrosis after tibial reaming for intramedullary nail fixation. A report of three cases. J. Bone Jt. Surg. Br. 1996, 78, 584–587. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Sena, E.; van der Worp, H.B.; Howells, D.; Macleod, M. How can we improve the pre-clinical development of drugs for stroke? Trends Neurosci. 2007, 30, 433–439. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Arnoldi, J.; Henry, P.; Procter, P.; Robioneck, B.; Jonsson, A. In vivo tissue response to ultrasound assisted application of biodegradable pins into cortical and cancellous bone structures: A histological and densitometric analysis in rabbits. J. Biomater. Sci. Polym. Ed. 2012, 23, 663–676. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Delgado-Pena, J.; Mate-Sanchez, J.E.; Mareque Bueno, J.; Delgado-Ruiz, R.A.; Romanos, G.E. Novel hybrid drilling protocol: Evaluation for the implant healing--thermal changes, crestal bone loss, and bone-to-implant contact. Clin. Oral Implant. Res. 2015, 26, 753–760. [Google Scholar] [CrossRef]
- Conzemius, M.G.; Brown, T.D.; Zhang, Y.; Robinson, R.A. A new animal model of femoral head osteonecrosis: One that progresses to human-like mechanical failure. J. Orthop. Res. 2002, 20, 303–309. [Google Scholar] [CrossRef]
- Eriksson, A.; Albrektsson, T.; Grane, B.; McQueen, D. Thermal injury to bone. A vital-microscopic description of heat effects. Int. J. Oral Surg. 1982, 11, 115–121. [Google Scholar] [CrossRef]
- Fan, M.; Peng, J.; Wang, A.; Zhang, L.; Liu, B.; Ren, Z.; Xu, W.; Sun, J.; Xu, L.; Xiao, D.; et al. Emu model of full-range femoral head osteonecrosis induced focally by an alternating freezing and heating insult. J. Int. Med. Res. 2011, 39, 187–198. [Google Scholar] [CrossRef] [PubMed]
- Lundskog, J. Heat and bone tissue. An experimental investigation of the thermal properties of bone and threshold levels for thermal injury. Scand. J. Plast. Reconstr. Surg. 1972, 9, 1–80. [Google Scholar] [PubMed]
- Lye, K.W.; Lee, S.; Tideman, H.; Merkx, M.A.; Jansen, J.A. Temperature changes in a cemented mandibular endoprosthesis: In vitro and in vivo studies. Int. J. Oral Maxillofac. Surg. 2011, 40, 86–93. [Google Scholar] [CrossRef]
- Mai, R.; Lauer, G.; Pilling, E.; Jung, R.; Leonhardt, H.; Proff, P.; Stadlinger, B.; Pradel, W.; Eckelt, U.; Fanghanel, J.; et al. Bone welding—A histological evaluation in the jaw. Ann. Anat. 2007, 189, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Martins, G.L.; Puricelli, E.; Baraldi, C.E.; Ponzoni, D. Bone healing after bur and Er:YAG laser ostectomies. J. Oral Maxillofac. Surg. Off. J. Am. Assoc. Oral Maxillofac. Surg. 2011, 69, 1214–1220. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Hossain, M.; Watanabe, H.; Tokonabe, H.; Matsumoto, N.; Matsumoto, K. Morphological changes of rat mandibular bone with ArF excimer laser in vivo. J. Clin. Laser Med. Surg. 1999, 17, 145–149. [Google Scholar] [CrossRef]
- Pourzarandian, A.; Watanabe, H.; Aoki, A.; Ichinose, S.; Sasaki, K.M.; Nitta, H.; Ishikawa, I. Histological and TEM examination of early stages of bone healing after Er:YAG laser irradiation. Photomed. Laser Surg. 2004, 22, 342–350. [Google Scholar] [CrossRef]
- Rayan, G.M.; Stanfield, D.T.; Cahill, S.; Kosanke, S.D.; Kopta, J.A. Effects of rapid pulsed CO2 laser beam on cortical bone in vivo. Lasers Surg. Med. 1992, 12, 615–620. [Google Scholar] [CrossRef]
- Rouiller, C.; Majno, G. Morphological and chemical studies of bones after the application of heat. Beitr. Zur Pathol. Anat. Und Zur Allg. Pathol. 1953, 113, 100–120. [Google Scholar]
- Stubinger, S.; Nuss, K.; Pongratz, M.; Price, J.; Sader, R.; Zeilhofer, H.F.; von Rechenberg, B. Comparison of Er:YAG laser and piezoelectric osteotomy: An animal study in sheep. Lasers Surg. Med. 2010, 42, 743–751. [Google Scholar] [CrossRef]
- Thompson, H.C. Effect of drilling into bone. J. Oral Surg. 1958, 16, 22–30. [Google Scholar] [PubMed]
- Tillotson, C.L.; Rosenberg, A.E.; Rosenthal, D.I. Controlled thermal injury of bone. Report of a percutaneous technique using radiofrequency electrode and generator. Invest. Radiol. 1989, 24, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, C.; Matsumoto, K. In vivo study of the healing processes that occur in the jaws of rabbits following perforation by an Er,Cr:YSGG laser. Lasers Med. Sci. 2005, 20, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Uoshima, K.; Oda, K.; Maeda, T. Influence of heat stress to matrix on bone formation. Clin. Oral Implant. Res. 2009, 20, 782–790. [Google Scholar] [CrossRef]
- Yoshino, T.; Aoki, A.; Oda, S.; Takasaki, A.A.; Mizutani, K.; Sasaki, K.M.; Kinoshita, A.; Watanabe, H.; Ishikawa, I.; Izumi, Y. Long-term histologic analysis of bone tissue alteration and healing following Er:YAG laser irradiation compared to electrosurgery. J. Periodontol. 2009, 80, 82–92. [Google Scholar] [CrossRef]
- Jacobs, R.L.; Ray, R.D. The effect of heat on bone healing. A disadvantage in the use of power tools. Arch. Surg. 1972, 104, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Pallan, F.G. Histological changes in bone after insertdon of skeletal fixation pins. J. Oral Surg. Anesth. Hosp. Dent. Serv. 1960, 18, 400–408. [Google Scholar]
- Pandey, R.K.; Panda, S.S. Drilling of bone: A comprehensive review. J. Clin. Orthop. Trauma 2013, 4, 15–30. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Reasons of Exclusion |
|---|---|
| Gholampour and Deh 2019 | No histological evaluation |
| Fuchsberger 1988 | No histological evaluation |
| Fontana et al., 2004 | No histological evaluation |
| Connor and Hynynen 2004 | No histological evaluation |
| Baker et al., 2011 | No histological evaluation |
| Bonfield and Li 1968 | No histological evaluation |
| Barnett 2001 | No requested outcome measures |
| Myers et al., 1980 | No requested outcome measures |
| Dolan et al., 2012 | No requested outcome measures |
| Petersohn et al., 2008 | No requested outcome measures |
| Posen et al., 1965 | No requested outcome measures |
| Ivanenco et al., 2002 | Only in vitro analysis |
| Lai et al., 2011 | Only in vitro analysis |
| Van Egmod et al., 1994 | Only in vitro analysis |
| Ryan et al., 1991 | Only in vitro analysis |
| Danckwardt-Lillistrom 1969 | Only in vitro analysis |
| Matthews et al., 1984 | Only in vitro analysis |
| Franssen et al., 2008 | No thermal values |
| Carvalho et al., 2011 | No thermal values |
| Stubinger et al., 2009 | No animal study |
| N | Author, Year | Species | Bone Area | N Animals | Thermal Application | Temperature Measurement System and Location | Temperature Max. in °C | Time | Effect on Bone | Follow up Time | BIC% |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Fan et al., 2011 | Emu | Femoral head cortical and cancellous | 20 | Liquid nitrogen and radiofrequency heating | Cryoprobe with external control system | −273 | 9 m nitrogen and 5 m heat | Necrosis | 16 w | n.s. |
| 2 | Conzemius et al., 2002 | Emu | Femoral head cortical and cancellous | 22 | Pressurized liquid nitrogen | n.s. | −196 | 15 s | Necrosis | 6 w | n.s. |
| 3 | Goetz et al., 2011 | Emu | Femoral head cortical and cancellous | 28 | Kirschner wire | Cryoprobe with two thermocouples at the exposed tip and one on the resistance-heated shaft | −50 | 9 m | 1410 necrosis volume (mm2) | 1 w | n.s. |
| −40 | 9 m | 1190 necrosis volume (mm2) | 1 w | n.s. | |||||||
| −30 | 9 m | 1000 necrosis volume (mm2) | 1 w | n.s. | |||||||
| −20 | 9 m | 700 necrosis volume (mm2) | 1 w | n.s. | |||||||
| −10 | 9 m | 400 necrosis volume (mm2) | 1 w | n.s. | |||||||
| 4 | Lye et al., 2011 | Monkey | Mandible cortical and cancellous | 6 | Cemented endoprothesis | One external thermocouple at the test location | 33.0 | 11 m | No thermal damage | 3 m | n.s. |
| 5 | Yoshida et al., 2009 | Rat | Calvaria cortical | 120 | Thermosimulator | Device with internal thermocouple | 37 | 15 m | Control, TRAP-positive cells were reduced | 1 w, 3 w and 5 w | n.s. |
| 43 | 15 m | TRAP-positive cells and ALP-positive cells were mostly absent on the bone surface after 1 w | 1 w, 3 w and 5 w | n.s. | |||||||
| 45 | 15 m | Rising average of dead osteocyte layers | 1 w, 3 w and 5 w | n.s. | |||||||
| 48 | 15 m | Apoptotic osteocytes were detected, high count dead osteocytes, no bone necrosis | 1 w, 3 w and 5 w | n.s. | |||||||
| 6 | Calvo-Guirado et al., 2015 | Dog | Mandible cortical and cancellous | 6 | Implant drill | Two external thermocouples next to the drill hole | 38.9 | up to 4 m | No thermal damage | 1 m | mean 43.1% SD 2.80 |
| 3 m | mean 64% SD 3.30 | ||||||||||
| 7 | Mai et al., 2007 | Sheep | Mandible cortical and cancellous | 12 | Frictional heat pins | n.s. | 40 | 4 h | No thermal bone damage | 2 w and 9 w | n.s. |
| 8 | Eriksson et al., 1984 | Rabbit | Fibula cortical and cancellous | 10 | Heated saline solution | External thermocouple in the Thermostat | 50 | 1 m | No thermal bone damage | n.s. | n.s. |
| 9 | Lundskog 1972 | Rabbit | Tibia cortical and cancellous | n.s. | Electric thermal probe | Infrared thermography | 50 | 30 s | Threshold necrosis | n.s. | n.s. |
| N | Author, Year | Species | Bone Area | N Animals | Thermal Application | Temperature Measurement System and Location | Temperature Max. in °C | Time | Effect on Bone | Follow up Time | BIC% | Infrabony Pockets Implant |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 10 | Eriksson and Albrektsson 1983 | Rabbit | Tibia cortical and cancellous | 15 | Heated implant chamber | Thermocouple inserted in the chamber with direct contact to the observed bone | 47 | 1 m | Hyperemia, no vessel long term effects, 2 d slower fat cell resorption, slower new fat cell formation, slower bone resorption after 30 d and remodeling | up to 4 w | n.s. | n.s. |
| 47 | 5 m | Hyperemia, 5 d vessel diameter increase, 2 d fat cell resorption, 3 w new fat cell formation and bone resorption, 30 d up to 30% bone resorption and remodeling | up to 4 w | n.s. | n.s. | |||||||
| 50 | 1 m | Hyperemia, 41° blood flow increase, 50° blood flow stop, 2 d fat cell resorption, 10 d revascularization, 3 w new fat cell formation and bone resorption | up to 4 w | n.s. | n.s. | |||||||
| 55–70 | 30 s | Necrosis | n.s. | n.s. | n.s. | |||||||
| 11 | Eriksson et al., 1982 | Rabbit | Tibia cortical and cancellous | 5 | Heated implant chamber | Thermocouple inserted in the chamber with direct contact to the observed bone | 53 | 1 m | Stop of blood flow up to 3–4 w revascularization, after 2 d connective tissue injury, 6–8 w formation of new fat cells, after 5 w bone remodeling and osteogenesis | up to 10 w | n.s. | n.s. |
| 12 | Thompson 1958 | Dog | Mandible cortical and cancellous | n.s. | Frictional heat pins | Infrared thermography | 40–67 | n.s. | Osteocyte degeneration and hyperemia | n.s. | n.s. | n.s. |
| 13 | Berman et al., 1984 | Rabbit | Tibia cortical | 18 | Heated isotonic fluid | Internal thermocouple in the bath | 45–55 | 1 m | Inflammation and fibrous tissue scar | 1, 2 and 3 w | n.s. | n.s. |
| 70 | 1 m | Necrosis | 1, 2 and 3 w | n.s. | n.s. | |||||||
| 14 | Rouiller 1953 | Rabbit | Calvaria, metatarsi and Radii cortical | 27 | Heated metal | n.s. | 46 | 5 m | Proliferation | 24 h | n.s. | n.s. |
| 55 | 1 m | Threshold necrosis | 24 h | n.s. | n.s. | |||||||
| 15 | Tillotson et al., 1989 | Dog | Femur cortical and cancellous | 4 | Radiofrequency electrodes | Thermocouple at the tip of the probe | 80 | up to 4 m | Bone necrosis diameter 0.9. 1.3 cm, muscle necrosis | 6 w | n.s. | n.s. |
| 16 | Trisi et al., 2015 | Sheep | Iliac crest cancellous | 2 | Heated electronic device | Internal thermocouple in the device | 50 | 1 m | Peri-implant bone loss, low density bone is more subject to heat-induced injury | 2 m | n.s. | n.s. |
| 60 | 1 m | Peri-implant bone loss, influence on the osseointegration | 2 m | n.s. | n.s. | |||||||
| 17 | Trisi et al., 2014 | Sheep | Mandible cortical | 3 | Heated electronic device | Internal thermocouple in the device | 50 | 1 m | No bone resorption, no threshold to heat-induced injury | 2 m | mean 25.99% SD 5.42 | mean 3.01 SD 0.81 |
| 60 | 1 m | Peri-implant bone loss | 2 m | mean 25.42% SD 1.49 | mean 3.11 SD 0.33 | |||||||
| 18 | Arnoldi et al., 2012 | Rabbit | Femur cortical and cancellous | 10 | Ultrasonic energy pins | None | 180–190 | several seconds | —5 d cortical sites were more sensitive compared to cancellous sites, —4 w. No signs of tissue degeneration, new bone formation | 5 d and 4 w | mean 39.25% SD 7.85 | mean 0.01 SD 0.01 |
| mean 27.23% SD 12.44 | mean 1.07 SD 0.44 |
| N | Author, Year | Species | Bone Area | N of Animals | Thermal Application | Temperature Measurement System | Laser Settings | Exposure Time | Effect on Bone | Follow up |
|---|---|---|---|---|---|---|---|---|---|---|
| 19 | Martins et al., 2011 | Rat | Mandible cortical | 20 | Er:YAG laser (cooled) | n.s. | 300 mJ/6 Hz, 350 mJ/6 Hz, and 400 mJ/6 Hz | 10 s | Similar healing pattern, 7 d thermal damage with thin layer of surface carbonization, 60 d amorphous layer persisted, 90 d no residual thermal damage was observed | up to 90 d |
| 20 | Nakamura et al., 1999 | Rat | Mandible cortical | 30 | Excimer laser | n.s. | 1.0 J/pulse and 10 Hz, 0.12 W, wavelength 193 nm (pulse duration 10–12 nsec, energy density 270 J/cm2 for 90 s with 34 °C and 360 J/cm2 for 120 s with 45 °C) | 90 s and 120 s | Neither carbonization nor necrotic zone was observed at the surrounding tissue. Some vacuolar degeneration of osteocyte adjacent to the defect was observed. Minimal thermal damage. | directly after irrigation |
| 21 | Pourzarandian et al., 2004 | Rat | Calvaria cortical | 24 | Er:YAG laser (cooled) | n.s. | 100 mJ/pulse and 10 Hz, 1 W, wavelength 2.94 μm (pulse duration of 200 μs) | 1.6 mm/s | —10 min a granular precipitate, red blood cells in aggregates of varying density predominant, thin fibrillar strands and inflammatory cells between cell aggregates. | up to 14 d |
| —6 h many polymorphonuclear leukocytes, —1 d decrease in the number of red blood cells. Polymorphonuclear leukocytes and macrophages. | ||||||||||
| —3 d maturation of the fibrin clot, and a reduced red blood cell population. The polymorphonuclear leukocyte population increased and fibroblasts. Phagocytosis and angiogenesis. | ||||||||||
| —7 d cell-rich granulation tissue contained fibroblasts, and clusters of osteoblasts closely adapted to the bone, spots of mineralization identified, collagen fibrils surrounding osteoblasts. | ||||||||||
| —14 d new bone formation. | ||||||||||
| CO2 laser (not cooled) | n.s. | 4 W, continuous wavelength of 10.6 μm | 2.5 mm/sec | —10 m a carbonized layer with microcracks and porosities, a zone of thermal necrosis. | up to 14 d | |||||
| —6 h many polymorphonuclear leukocytes. | ||||||||||
| —1 d the population of polymorphonuclear leukocytes increased. | ||||||||||
| —3 d polymorphonuclear leukocytes predominant, proceeding to clear the necrotic or carbonized material. Healing started | ||||||||||
| —7 d fibrillar strands organized. | ||||||||||
| —14 d carbonized tissue still covered the treated surface. spots of mineralization, percentage of the area of new | ||||||||||
| —bone formation of Er:YAG laser and no significant new bone formation of CO2 laser. | ||||||||||
| 22 | Rayan et al., 1992 | Rabbit | Femur cortical and cancellous | 20 | CO2 laser (not cooled) | n.s. | 20 W, 2 kHz spike pulse for 10 s. The pulse duration is 0.1 ms | 10 s | 4- and 6-week bony healing. Superficial zone on the inner cortex carbonization, residuals from vaporized tissue. bone resorption. encapsulated by reactive cells, evidence of new bone formation, deeper region of cellular thermal damage and bone necrosis but without vaporization. Active resorption by osteoclasts, histologic changes had less than 40 pm | 4 w and 6 w |
| 23 | Stubinger et al., 2011 | Sheep | Tibia cortical an cancellous | 24 | Er:YAG laser (cooled) | n.s. | 1000 mJ/pulse and 12 Hz, energy density 157 J/cm2 (pulse duration of 300 μs, applied water spray level was 40–50 mL/m) | 2 mon 245.33 s SD 29.9.3 mon 211.17 s SD 45.1 | No thermal damage | 2 mon and 3 mon |
| 24 | Wang et al., 2005 | Rabbit | Mandible and maxilla cortical | 12 | Er:YAG laser (cooled) | n.s. | 20 Hz, 2 W (emitting at 2.78 lm, pulsed with a duration of 140–200 ls, tip used was 400 lm in diameter and 8.0 mm in length) | 10 s | 70–90 micron bone necrosis (mean 30) | directly after irrigation |
| 25 | Yoshida et al., 2009 | Rat | Calvaria cortical | 30 | Contact Er:YAG laser (not cooled) | n.s. | 115 mJ/pulse and 10 Hz. Contact focused irradiation (energy density: 40.7 J/cm2/pulse) | 1 cm per 3 s | No major thermal changes were noted around the ablation defect | up to 6 m |
| Non-contact Er:YAG laser (not cooled) | n.s. | 115 mJ/pulse and 10 Hz. Non-contact defocused irradiation (6.6 J/cm2/pulse) | 1 cm per 3 s | No major thermal changes were noted around the ablation defect | up to 6 m |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kniha, K.; Heussen, N.; Weber, E.; Möhlhenrich, S.C.; Hölzle, F.; Modabber, A. Temperature Threshold Values of Bone Necrosis for Thermo-Explantation of Dental Implants—A Systematic Review on Preclinical In Vivo Research. Materials 2020, 13, 3461. https://doi.org/10.3390/ma13163461
Kniha K, Heussen N, Weber E, Möhlhenrich SC, Hölzle F, Modabber A. Temperature Threshold Values of Bone Necrosis for Thermo-Explantation of Dental Implants—A Systematic Review on Preclinical In Vivo Research. Materials. 2020; 13(16):3461. https://doi.org/10.3390/ma13163461
Chicago/Turabian StyleKniha, Kristian, Nicole Heussen, Eugenia Weber, Stephan Christian Möhlhenrich, Frank Hölzle, and Ali Modabber. 2020. "Temperature Threshold Values of Bone Necrosis for Thermo-Explantation of Dental Implants—A Systematic Review on Preclinical In Vivo Research" Materials 13, no. 16: 3461. https://doi.org/10.3390/ma13163461
APA StyleKniha, K., Heussen, N., Weber, E., Möhlhenrich, S. C., Hölzle, F., & Modabber, A. (2020). Temperature Threshold Values of Bone Necrosis for Thermo-Explantation of Dental Implants—A Systematic Review on Preclinical In Vivo Research. Materials, 13(16), 3461. https://doi.org/10.3390/ma13163461