Abstract
Carbapenem-resistant Enterobacteriaceae (CRE) and vancomycin-resistant Enterococci (VRE) have emerged as multidrug-resistant (MDR) pathogens associated with periprosthetic joint infections (PJI). In this study, we evaluated the efficacy of antibiotic-loaded calcium sulfate beads (ALCSB) in inhibiting bacterial growth, encouraging biofilm formation and killing preformed biofilms of CRE and VRE. Three strains of Klebsiella pneumoniae (KP) and a strain of Enterococcus faecalis (EF) were used. ALCSB of 4.8-mm diameter were loaded with vancomycin (V) and gentamicin (G), V and rifampicin (R), V and tobramycin (T) or R and meropenem (M), and placed onto tryptic soy agar (TSA), spread with one of the test strains and incubated for 24 h at 37 °C. Beads were transferred daily onto fresh TSA spread plates and the zone of inhibition (ZOI) was recorded until no inhibition was observed. ALCSB containing R + M or R + V produced the most extensive ZOI up to 5 weeks. Biofilm prevention efficacy was investigated by challenging ALCSB daily with 5 × 105 CFU/mL bacterial cells and analyzing for biofilm formation at challenges 1, 2 and 3. In the biofilm killing experiments, ALCSB were added to pre-grown 3-day biofilms of KP and EF strains, which were then analyzed at days 1 and 3 post-exposure. The CFU counts and confocal images of the attached cells showed that ALCSB treatment reduced colonization and biofilm formation significantly (5–7 logs) with combinations of R + M or R + V, compared to unloaded beads. This study provides evidence that the local release of antibiotics from ALCSB may be useful in treating the biofilms of multidrug-resistant strains of CRE and VRE.
1. Introduction
In recent years, multidrug-resistant organisms, especially vancomycin-resistant enterococcus (VRE) and carbapenem-resistant enterobacteriaceae (CRE) strains have become more prevalent worldwide, and represent a serious public health threat since they are becoming increasingly resistant to current treatment modalities [1]. In the United States alone, antibiotic-resistant K. pneumoniae and Enterococcus spp. account for nearly 10% of all hospital-acquired infections [2]. Vancomycin resistance among enterococci has markedly increased since it was first described in the mid-1980s [3]. The increasing prevalence of carbapenem-resistant Enterobacteriaceae, primarily K. pneumoniae (KP), is rendering treatment of these infections challenging [4]. Broad-spectrum antibiotic exposure, immune suppression and intravascular devices increase the risk of colonization and infection with one or more antibiotic-resistant bacteria [5].
Periprosthetic joint infection (PJI) is a leading complication and cause of morbidity in joint replacement surgery [6,7]. An underlying problem with treating PJI is that many of the causative pathogens form bacterial biofilms [8]. Whilst Staphylococci are the most common PJI pathogens, VRE and carbapenem-resistant Klebsiella pneumoniae strains (a CRE strain) have also been reported, and are associated with poor outcomes [9,10]. Biofilms are microbial populations that adhere to surfaces forming a community inherently highly tolerant to antibiotics compared to their planktonic counterparts, even if isolates are shown to be sensitive by routine clinical microbiological methods, such as the minimum inhibitory concentration (MIC) assay [11]. Biofilms associated with orthopedic infections are typically difficult to diagnose and treat [12,13], and often the only effective intervention is extensive debridement or prostheses removal [14]. Treatment strategies for PJI in total hip and total knee arthroplasty patients include the use of bone cement [14,15], and absorbable calcium sulfate void fillers loaded with antibiotics [16,17], to increase the local concentration and exposure period at the surgical site, beyond those obtainable with systemic administration [18]. In vitro studies show how antibiotic-loaded calcium sulfate beads (ALCSB) can significantly reduce or even eradicate bacterial biofilms of various Gram-positive and -negative PJI pathogens [11,19,20]. ALCSBs are used clinically in total joint replacements. Studies have highlighted the application of ALCSBs for infection prophylaxis and treatment in total joint replacements [21,22,23]. Combinations of two or more antibiotics are commonly used, in local antibiotic delivery in calcium sulfate beads, for patients with hip and knee arthroplasty [17,24,25]. In another study, McPherson et al. (2013) have shown the use of ALCSBs in the treatment of PJI and revision arthroplasty [16]. However, there is little information concerning whether carbapenem-resistant Klebsiella pneumoniae and vancomycin-resistant E. faecalis strains form biofilms, or how they might be killed by ALCSB. Synergistic interactions between antibiotics have been shown in the treatment of biofilms [26,27]. In a recent study, dose-dependent synergistic interactions of colistin with rifampin, meropenem and tigecycline have been shown to be effective against K. pneumoniae biofilms [26]. Powdered rifampicin and vancomycin have shown efficacy against Staphylococcus aureus on orthopedic implants [28]. A combination of meropenem and rifampicin has been reported for the treatment of osteomyelitis [29]. We were interested to test the combination of antibiotics loaded in bone cement for use against the multidrug-resistant strains of CRE and VRE. The goals of the present study were as follows: (i) to assess biofilm formation in three CRE strains (including the metallo-beta-lactamase New Delhi strain) and one VRE strain, and (ii) to quantify the long-term bioactivities of various combinations of antibiotics released from ALCSBs, in order to determine the ability to prevent biofilm formation or kill pre-established biofilms of these strains in vitro.
2. Materials and Methods
2.1. Strains and Culture Conditions
The virulent and multidrug-resistant strains of carbapenem-resistant Enterobacteriaceae (CRE) [Klebsiella pneumoniae ATCC-BAA 1705 (KP-1705), K. pneumoniae ATCC-BAA 2524 (KP-2524), K. pneumoniae ATCC-BAA 2146 (KP-2146)] and the vancomycin-resistant Enterococci (VRE) strain of Enterococcus faecalis ATCC 51,299 (EF-51,299) were used in this study. The strains were obtained from the American Type Culture Collection (ATCC, Manassas, VA), USA and streaked onto tryptic soy agar (TSA) and incubated at 37 °C for 24 h. The colonies were grown on TSA plates and then inoculated into tryptic soya broth (TSB) and incubated at 37 °C for 24 h.
2.2. Determination of Minimum Inhibitory Concentration (MIC) of Antibiotics Against CRE and VRE
The MIC was determined using the sterile antibiotic loaded E-test strips (BioMerieux, Durham, NC, USA) following the standard procedure [30,31]. The E-test strips for gentamicin (G), rifampicin (R), tobramycin (T) and vancomycin (V) were used. For some of the strains, the values available in the literature for antibiotic MIC were used (Table 1).

Table 1.
Minimum inhibitory concentration (MIC) of antibiotics against CRE and VRE strains determined by E-test strip assay; where, KP is Klebsiella pneumoniae, EF is Enterococcus faecalis and r represents resistance.
2.3. Preparation of Antibiotic-Loaded Calcium Sulfate Beads (ALCSB)
ALCSBs were prepared using Stimulan Rapid Cure® (Biocomposites Ltd., Staffordshire, UK) as detailed previously [11]. ALCSBs were prepared as detailed in Table 2. All the antibiotics were obtained from GoldBio (St. Louis, MO, USA). Unloaded CSBs were used as negative controls. A 20-g pharmaceutical-grade calcium sulfate alpha-hemihydrate powder (Stimulan; Biocomposites Ltd., Keele, UK) was mixed with 6 mL of sterile water (unloaded beads). For antibiotic-loaded beads, tobramycin sulfate powder, vancomycin hydrochloride powder, gentamicin sulfate, rifampicin and meropenem, as shown in Table 2, were mixed with 6 mL sterile water. For preparing the beads, the components were mixed for 30 to 60 s to form a smooth paste, which was pressed into 4.8-mm-diameter hemispherical cavities in a flexible mold. The beads were left undisturbed for 30 to 60 min to set. When set, the beads were removed by flexing the mold.
Table 2.
Antibiotics and amounts used in the study. The amount of antibiotic loaded per pack of Stimulan (10 cc) to prepare beads is mentioned as mg/10 cc, and maximum concentration of antibiotic eluted within 24 h from beads per well during prevention and treatment is mentioned as mg/mL.
2.4. Modified Kirby–Bauer Assay for Assessing the Repeat Zone of Inhibition (ZOI)
A repeat zone of inhibition (ZOI) test, using a modified Kirby–Bauer assay, was performed to determine the release and potency of antibiotics from a 4.8-mm-diameter ALCSB over a period of 38 days. Briefly, bacteria were spread onto TSA plates using 50 µL of an overnight culture. A single bead was placed onto agar plates with sterile forceps after spreading the bacteria and the plates were incubated at 37 °C for 24 h. ZOI were assessed and photographed, and the beads were transferred onto a freshly spread bacteria on TSA plates. This process was repeated each day until the ZOI were lost. The ZOI were calculated using ImageJ (version 1.48, NIH, Kansas, MO, USA), as described previously [11]. Analyses were performed every day until potency was lost, as evidenced by growth right up to the edge of the bead or the beads having disintegrated. Assays were performed in triplicate, and the data was expressed as the mean of 3 data points with standard error bars.
2.5. ALCSBs for Preventing Biofilm Formation
Antibiotic-loaded and unloaded beads (10 beads per well) were placed into 6-well MatTek tissue culture plates (MatTek Corporation, Ashland, MA, USA). The numbers of beads were chosen to compromise between higher bead numbers, which may physically inhibit substratum colonization, and too few beads, which would limit clinical relevance [11]. The MatTek plates were inoculated with 4 mL of an overnight culture diluted with fresh TSB to achieve a concentration of approximately 106 cells/mL and incubated on a shaker incubator set at 37 °C with 5% CO2 and at 50 rpm. Every 24 h, the spent medium was replaced, and the beads subjected to a fresh bacterial challenge of 4 mL of 106 cells/mL. At challenges 1, 2 and 3 post-inoculation, CFU counts of the surface-attached bacterial populations in the 6-well plates were performed. Briefly, the wells were rinsed twice in PBS to remove the planktonic cells. The surfaces of the wells were scraped using sterile cell scrapers (VWR, Bridgeport, NJ, USA) to remove the attached biofilms into 1 mL PBS. Following vortexing for 20 s to homogenize the biofilm bacteria, serial dilutions were performed in PBS and plated onto TSA plates using the drop plate method [39,40]. Concurrently, at challenges 1 and 3, the fluorescent BacLight Live-Dead stains for microscopy (ThermoFisher Scientific, Waltham, MA, USA) containing SYTO9 and Propidium iodide (PI) were used to microscopically assess the surface-attached biomass in a second set of MatTek plates. Plates were rinsed with PBS and stained (with 2 µL of BacLight Live-Dead stain per mL of PBS) for 20 min. The plates were gently rinsed and analyzed using a confocal laser scanning microscope with 10 × objective (CLSM, Olympus Fluoview FV10i, Pittsburgh, PA, USA). Cells stained green were live and those in red were determined as dead based on the permeability of the dyes and as per manufacturer’s instructions.
2.6. ALCSBs Killing Efficacy of Preformed Biofilms
Each well of a 6-well MatTek plate was inoculated with 4 mL of culture (~106 cells/mL) as described above, but in this case, there were initially no beads in the wells. Biofilms were allowed to form for 3 days (37 °C, 5% CO2 and 50 rpm) with daily media exchanges of fresh media. On the 3rd day, 10 antibiotic-loaded or unloaded beads per well were added to each well along with fresh TSB. Every 24 h, the medium was replaced and CFUs were enumerated by sacrificing wells at days 1 and 3 as previously described [11]. Concurrently, at days 1 and 3 post-bead addition, the fluorescent BacLight Live-Dead stains containing SYTO9 and PI were used to microscopically assess the surface-attached biomass in a second set of MatTek plates as described above. The confocal images of prevention and killing experiments were analyzed for biofilm biomass and thickness using COMSTAT analysis (version 2.1, ImageJ plugin).
2.7. Statistics
Data were compared using a paired t-test assuming equal variance, and differences were considered significant when the p value was ≤ 0.05 (⁎), ≤ 0.01 (⁎⁎) and ≤ 0.001 (⁎⁎⁎), and non-significant when p ≥ 0.05 (ns). Multivariate ANOVA (MANOVA, SPSS version 25, IBM, New York, NY, USA) was performed using SPSS statistical data analysis software.
3. Results
3.1. Modified Kirby–Bauer Assay for Assessing the Repeat Zone of Inhibition (ZOI)
ALCSBs loaded with G + V, R + V, V + T and R + M elicited zones of inhibition (ZOI) against all bacterial strains tested, but with varying durations of potency, which was both antibiotic- and strain-dependent (Figure 1, Table 1). While all combinations exhibited potency against all strains for at least 5 days, generally the ALCSB loaded with R + V exhibited the greatest duration of potency, ranging from 23 to 38 days while the beads were still intact (Figure 1). The ALCSB loaded with R + M showed extended potency against KP-2524, KP-2146 and EF-51299, but not against the KP-1705 strain. For this strain, ALCSB loaded with G + V showed a potency duration of 20 days, similar to R + V, which was 22 days (Figure 1). The combinations of V + T were least effective against all the test strains, as compared to the R + V and R + M antibiotic combinations tested. This could be due to the lower MIC of antibiotics R and M, as compared to T and V, which showed either higher MIC or resistance against some of the CRE and VRE strains that were tested (Table 1).
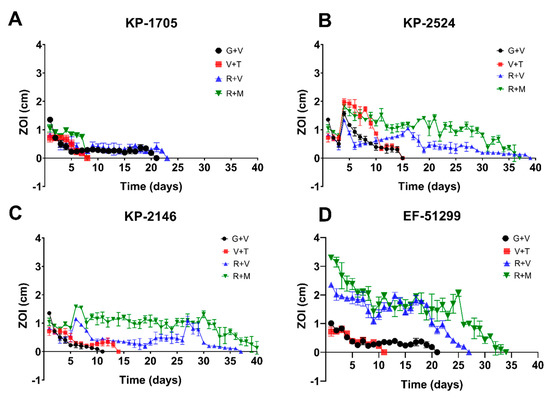
Figure 1.
Repeat modified Kirby–Bauer assays for assessing the zones of inhibition (ZOI) of K. pneumoniae (A) KP-1705, (B) KP-2524, (C) KP-2146 and (D) E. faecalis EF-51299 using combinations of antibiotics G + V, R + V, V + T and R + M over a period of 38 days. Data are expressed as means of 3 replicates with standard error bars.
3.2. ALCSBs for Preventing Biofilm Formation
All the antibiotic combinations demonstrated a significant (p < 0.05) retardation of biofilm formation after 24 h, showing a log reduction between 5–7 in CFU/cm2 compared to the unloaded control beads (Figure 2). KP-2524 was generally more susceptible to retardation of the formation of its biofilm, using all of the four antibiotic combinations after challenges 1, 2 and 3, as compared to other strains. Against KP-1705, significant log reduction (log 6.0–6.7) was achieved with the R + M combination after 1-, 2- and 3-day bacterial challenges, followed by R + V (with 4.6–6.3 log reduction) and V + T (5.7–5.9). G + V was relatively less effective, with 4.1–4.8 log reduction in bacterial count (Figure 2A). Similarly, in the case of KP-2524, R + M, V + T and R + V were equally effective, with a 6.1–7.6 log reduction, and G + V had the lowest (from 4–4.7 log), as compared to other combinations in reducing the biofilm (Figure 2B). All the antibiotic combinations were less effective in reducing the biofilms of KP-2146, with R + M (~2.5 log), R + V (2.8 log), V + T (1.9) and G + V causing only a 0.8 log reduction after the three daily bacterial challenges (Figure 2C). As expected with repeated challenges (which both removed the antibiotic eluted over the preceding 24 h, and added fresh media and a fresh bacterial challenge), the log reduction in biofilm growth diminished over time. However, there was still significant retardation of biofilm growth in the strains, as mentioned above, for KP-2524 and KP-1705. EF-51299 experienced a similar significant reduction in biofilm growth after the three bacterial challenges, showing >6 log reduction with R + M and V + T, a 5.5 log reduction with R + V and a 4.7 log reduction with G + V, compared to the control (Figure 2D).
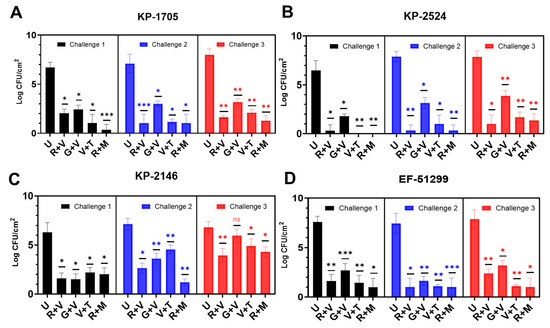
Figure 2.
Biofilm formation by (A) K. pneumoniae KP-1705, (B) KP-2524, (C) KP-2146 and (D) E. faecalis EF-51299 in the presence of 10 antibiotic loaded calcium sulfate beads (ALCSBs) as compared to unloaded bead controls (U) as determined by CFU. The differences were significant with p values ≤ 0.05 (⁎), ≤ 0.01 (⁎⁎) and ≤ 0.001 (⁎⁎⁎), and non-significant when p ≥ 0.05 (ns).
Confocal microscopy provided direct evidence that all these strains could form substantial biofilms (Figure 3 unloaded bead control). After 24 h the biofilms were similar in appearance and tended to be relatively flat (Figure 3A). However, after three daily bacterial challenges the biofilms had started to show the structures of aggregates of cells (Figure 3B). At this time, KP-1705 and EF-51,299 were more heterogeneous in structure, and KP-2146 and 2524 had filled in, creating a more uniform layer (Figure 3B). With respect to the effect of the ALCSB, there was general agreement with the CFU data. At days 1 and 3, all the antibiotic combinations were effective in reducing the biomass of biofilms as compared to the unloaded beads, with significant reductions in viability (more cells were red) (Figure 3A,B). Furthermore, it is evident that ALCSB loaded with R + M were more effective in inhibiting biofilm formation than other combinations assessed. Multivariate analysis (ANOVA) also showed significant differences between parameters in the prevention groups (Supplementary Materials, Table S1). Moreover, the biofilm biomass and biofilm thickness were significantly lower in R + M and R + V, compared to the other antibiotic combinations and the control without antibiotic treatment in prevention group (Table S2).
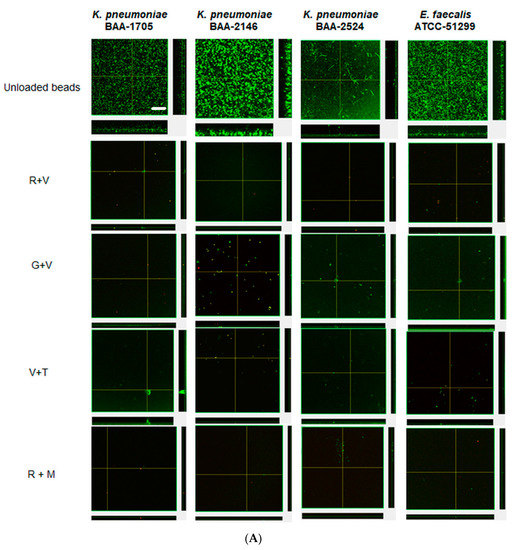
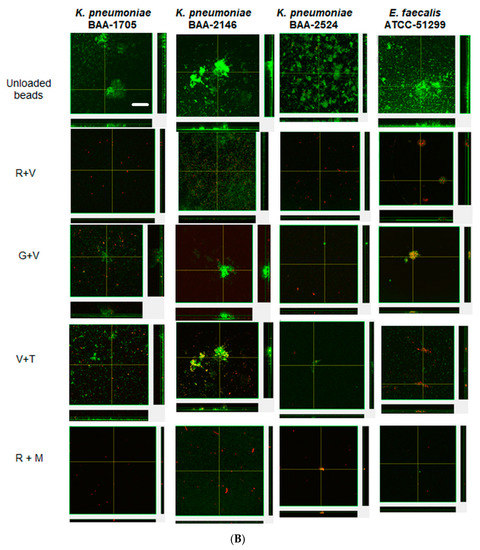
Figure 3.
Confocal images of prevention of biofilms at challenge 1 (A), challenge 3 (B) by ALCSBs, and unloaded control beads. The biofilms were stained with Live-Dead stain where green represents live and red represents dead bacterial cells within biofilms. Bar represents 20 µm size.
3.3. ALCSBs Killing Efficacy of Preformed Biofilms
The killing efficacy of pre-established, 3-day biofilms showed a similar trend as was seen with the biofilm prevention assay (Figure 4). After 24 h exposure to the various ALCSB combinations, biofilms were reduced significantly (p < 0.05), by between 3 and 7 logs depending on the strain and antibiotic combination. Generally, ALCSB loaded with R + M exhibited the most efficacy, particularly at the longer exposure times, reducing the biofilm bacteria by ~5–6 logs in all strains. KP-1705 showed significant reduction in 3-day biofilms after treatment with R + M (6 log reduction), V + T (6.9 log reduction), G + V (6.7 log reduction) and R + V (5.7 log reduction) (Figure 4A). R + M and R + V were similar in reducing (~5.5 log) the biofilms of KP-2524, followed by G + V and V + T with 3.3 log reduction (p < 0.01, Figure 4B). Against KP-2146, R + M was more effective in reducing the biofilms up to 6 logs (p < 0.01), followed by R + V (4.7 log), G + V (4 log) and V + T (~3 log) (Figure 4C). R + M and R + V were effective against the VRE strain of EF-51299, with ~5 log reduction (p < 0.01), and V + T resulted in a 4.2 log reduction and G + V in a 3.8 log reduction. Multivariate analysis (ANOVA) showed significant differences between different parameters in the killing groups (Table S1). The reductions in biofilms of EF-51,299 were, however, non-significant (p > 0.05) at day 1 of the treatment (Figure 4D). The biofilm biomass and biofilm thickness in the killing group were significantly lower in the R + M and R + V treatment groups, as compared to the other antibiotic combinations and the control without antibiotic treatment (Table S3).
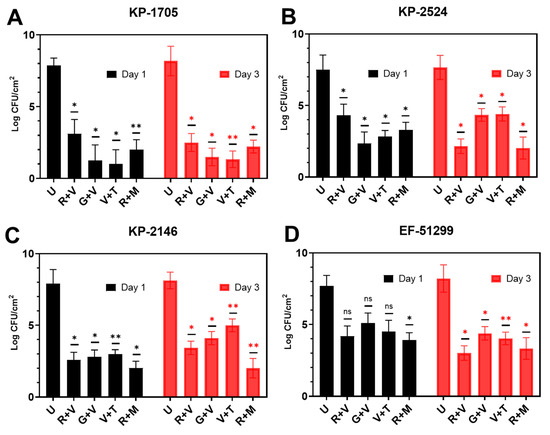
Figure 4.
Effect of ALCSB on pre-established biofilms of (A) K. pneumoniae KP-1705, (B) KP-2524, (C) KP-2146 and (D) E. faecalis EF-51299 over time as compared to unloaded bead controls as determined by CFU. The differences were significant with p value ≤ 0.05 (⁎), ≤ 0.01 (⁎⁎), and non-significant when p ≥ 0.05 (ns).
Confocal microscopy corroborated the CFU data, with unloaded preformed biofilms of KP-1705, 2146, 2524 and EF-51,299 showing thicker biofilms, and green staining with SYTO9 depicting viable cells. These biofilms, when treated with R + V and R + M, showed the killing of biofilms after 1 day of treatment. The residual biofilms were red in color, as compared to the unloaded biofilms and when compared with G + V and V + T (Figure 5A). V + T showed more red cells with KP-2146 and KP-2524 as compared to G + V. Similarly, after treatment with R + M and R + V, the significant killing of biofilms of all strains was evident (Figure 5B). V + T and G + V were less effective in reducing the preestablished biofilms, as evident from the confocal images showing large aggregates of biofilms still present and based on the CFU counts. Overall, ALCSB loaded with R + M showed the greatest reduction in biofilm after 1 and 3 days of treatment (Figure 5A,B).
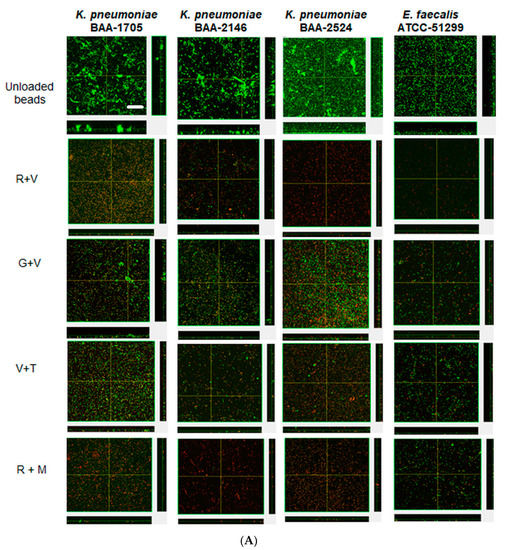
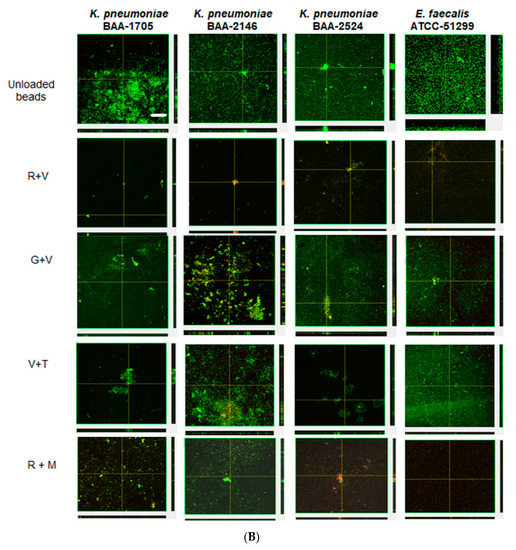
Figure 5.
Confocal images showing the effect of ALCSBs against 3-day pre-established biofilms at (A) day 1 and (B) day 3 post-bead addition. The biofilms were stained with Live-Dead stain, where green represents live and red represents dead bacterial cells within the biofilms. Bar represents 20 µm size.
4. Discussion
In this study, we evaluated the effect of Stimulan Rapid Cure antibiotic-loaded calcium sulfate beads on biofilms formed from Klebsiella pneumoniae (KP) and Enterococcus faecalis (EF) CRE and VRE clinical strains in-vitro. Few of these strains are resistant to gentamicin (G), tobramycin (T) and vancomycin (V) (Table 1). Therefore, combinations of antibiotics were used to determine the effect of ALCSB against these multidrug-resistant strains. Moreover, some of these antibiotic combinations were selected based on their clinical applications in the treatment of joint infections [17,24]. The beads were loaded with various combinations of antibiotics, which are commonly incorporated into bone cement and absorbable bone void fillers to treat PJI (Table 2).
Even though the CRE and VRE strains involved in PJI are relatively uncommon, they present a unique challenge in the era of antimicrobial resistance [10,41,42,43]. Until 2015, the antibiotic treatment regimens for these infections included combinations of agents, which was associated with high toxicity rates (aminoglycosides and colistin), suboptimal pharmacokinetics (aminoglycosides, colistin and tigecycline) and known microbiological resistance [41,43]. In addition to antibiotic resistance, biofilm formation in PJI and other infections associated with foreign bodies has an added virulence factor, since it provides both antibiotic tolerance and protection from host defenses. Biofilm formation by clinical CRE and VRE strains is not well characterized. Therefore, in this study we investigated the efficacy of combinations of potential antibiotic candidates, released from ALCSB, in controlling ATCC strains of K. pneumoniae CRE and E. faecalis VRE biofilms in-vitro.
In the first set of experiments, a Kirby–Bauer-type diffusion test showed that antibiotics loaded into ALCSB were potent against planktonic bacteria for multiple days, and zones of clearing were maintained for up to 38 days, indicating that eluted antibiotics remained at concentrations high enough to kill the planktonic cells throughout this time. The in vitro elution of antibiotics from high purity calcium sulfate beads has been shown previously in liquid medium [19,44,45,46,47]. Previous studies have shown the comparable time efficacies of ALCSB loaded with V + T against common Gram-negative and Gram-positive PJI species [11,48]. However, here we demonstrate that V + T was less effective in terms of potency duration against the CRE and VRE strains, with potency lost between 7 and 11 days. The in vitro release of R + V retained its potency against all the strains for between 24 and 36 days, and R + M was effective against three strains for 34–35 days. Rifampin (R) has been shown previously to have good anti-biofilm efficacy against Gram-positive bacteria, such as S. aureus [49], but should be used in combination with other antibiotics because of the fear of the rapid development of resistance [50,51,52].
Further, studies were performed to determine the effectiveness of the ALCSBs in preventing biofilm formation and killing pre-established biofilms of CRE and VRE strains. We found that in the absence of antibiotics all the strains could form robust biofilms within 3 days. Whether biofilm formation confers additional antibiotic tolerance remains to be seen and would require minimum biofilm eradication concentration (MBEC) and minimal biofilm inhibitory concentration (MBIC) assays, which are standard methods designed specifically for mature biofilms [53]. In a study of the efficacy of 10 different antibiotics (cefazolin, clindamycin, vancomycin, rifampin, linezolid, nafcillin, gentamicin, trimethoprim/sulfamethoxazole, doxycycline and daptomycin) in killing pre-established biofilms formed from 18 S. aureus clinical PJI isolates (10 methicillin-resistant and 8 methicillin-sensitive), only rifampin, doxycycline and daptomycin had measurable biofilm MIC values across all S. aureus isolates tested [18]. Therefore, the R + M and R + V combinations used in the present study may also demonstrate good efficacy against CRE and VRE strains in PJI. In a previous study, we demonstrated that R + V released from Stimulan ALCSB led to significant reductions in S. epidermidis ATCC 35,984 biofilms, a very robust biofilm-forming strain [19]. Along similar lines, we observed that the ALCSB antibiotic combinations significantly reduced biofilm formation, and killed preformed biofilms formed from these CRE and VRE strains, although the degree was dependent on both the strain and the antibiotic combination. Generally, the R + M and R + V combinations performed were the most efficacious in terms of log reductions, in agreement with the repeated ZOI data. Previous studies have found that the MBEC is reduced with time of exposure [54], which is consistent with the understanding that for some antibiotics, both concentration and exposure time are important [55]. In our experiments we saw a general loss of efficacy in retardation and killing over time; however, our assays were particularly challenging. For the prevention assay, the beads were challenged daily with approximately 4 × 106 CFU with fresh media, and any antibiotic that had eluted over the previous 24 h was completely removed, allowing time for the biofilm to grow until inhibitory levels were re-established. On the preformed biofilms, increasing the number of beads or the dose associated with the beads could result in a significant reduction in biofilm formation. This could be a part of the follow-on study to determine the influence of bead number and dose on biofilms. In the biofilm killing assay, although there was no daily challenge, nutrients were replenished, again removing previously eluted antibiotics. Nevertheless, we still saw significant log reductions in biofilm formation (up to 6 logs) after 3 days, the exception being KP-2146, which was more resistant to all antibiotic concentrations and exhibited between 1 and 3 log reductions, depending on the antibiotic combination after three challenges. Similarly, with the biofilm killing assays, there was a 3 to 6 log killing at 3 days with the R + M combination against all strains.
In this series of experiments, R + M and R + V generally performed the best in controlling biofilms of CRE and VRE strains in our in vitro assays. V + T in the US and V + G in Europe are more commonly used to provide coverage against Staphylococci spp. (the most common pathogens in PJI) and broad-spectrum coverage against Gram-negative bacteria, which might be present [56,57,58,59]. One of the issues with treating PJIs is that antibiotic selection is confounded by the difficulty in culturing biofilm bacteria, and often antibiotics administered systemically and locally in cement or in-absorbable mineral beads are often less effective [59,60]. Until more rapid and sensitive methods for isolating bacterial species and generating comprehensive antibiograms are developed, other antibiotic combinations may be considered if CRE or VRE are suspected.
In conclusion, we have shown that strains of CRE and VRE species formed robust biofilms after 3 days, and that Stimulan Rapid Cure antibiotic-loaded calcium sulfate beads retained their potency for up to 38 days. The degree of biofilm retardation and the killing of pre-established biofilms was dependent on the strain and the antibiotic combination, but generally all combinations resulted in significant log reductions for up to three challenges. The combinations of antibiotics rifampicin and vancomycin, and rifampicin and meropenem, were most effective in controlling these CRE and VRE biofilms. Whilst these combinations are effective in vitro, more tests in vivo and clinical investigations are needed.
Supplementary Materials
The following are available online at https://www.mdpi.com/1996-1944/13/15/3258/s1, Table S1: Multivariate analysis (ANOVA) of prevention and killing treatment groups. Table S2: Biomass and thickness of biofilms in prevention group analyzed by COMSTAT. Table S3: Biomass and thickness of biofilms in killing group analyzed by COMSTAT.
Author Contributions
P.S. and D.H.D. conceived and supervised the project. D.H.D, J.B. and C.W.P. performed the experiments. N.J. performed the COMSTAT analysis. P.S. and D.H.D. edited the figures. P.S., C.P.D., S.S.A., P.A.L., and D.H.D. interpreted the results. D.H.D. drafted the initial manuscript and P.S., C.P.D., S.S.A., P.A.L., and D.H.D. reviewed and revised the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Biocomposites Limited, Keele, U.K.
Acknowledgments
P.S. is funded by Biocomposites Ltd., P.S. and D.H.D. served as consultants for Biocomposites Ltd., S.S.A., C.P.D. and P.A.L. are employed by Biocomposites Ltd. The authors wish to acknowledge Tripti Gupta, who provided help with COMSTAT analysis.
Conflicts of Interest
P.S. receives funding and consulting fees from Biocomposites Ltd., Keele, UK. S.S.A., C.P.D. and P.A.L. are employed by Biocomposites Ltd. Biocomposites was involved in discussion on the experimental design. Other co-authors declare no conflict of interest.
References
- Gutiérrez-Gutiérrez, B.; Sojo-Dorado, J.; Bravo-Ferrer, J.; Cuperus, N.; De Kraker, M.; Kostyanev, T.; Raka, L.; Daikos, G.; Feifel, J.; Folgori, L. EUropean prospective cohort study on Enterobacteriaceae showing REsistance to CArbapenems (EURECA): A protocol of a European multicentre observational study. BMJ Open 2017, 7, e015365. [Google Scholar] [CrossRef]
- Magill, S.S.; Edwards, J.R.; Bamberg, W.; Beldavs, Z.G.; Dumyati, G.; Kainer, M.A.; Lynfield, R.; Maloney, M.; McAllister-Hollod, L.; Nadle, J. Multistate point-prevalence survey of health care—Associated infections. N. Engl. J. Med. 2014, 370, 1198–1208. [Google Scholar] [CrossRef] [PubMed]
- Arias, C.A.; Murray, B.E. Emergence and management of drug-resistant enterococcal infections. Expert Rev. Anti-Infect. Ther. 2008, 6, 637–655. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Limbago, B.M.; Patel, J.B.; Kallen, A.J. Carbapenem-resistant Enterobacteriaceae: Epidemiology and prevention. Clin. Infect. Dis. 2011, 53, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Safdar, N.; Maki, D.G. The commonality of risk factors for nosocomial colonization and infection with antimicrobial-resistant Staphylococcus aureus, enterococcus, gram-negative bacilli, Clostridium difficile, and Candida. Ann. Intern. Med. 2002, 136, 834–844. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, V.K.; Rasouli, M.R.; Parvizi, J. Periprosthetic joint infection: Current concept. Indian J. Orthop. 2013, 47, 10. [Google Scholar]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin. Microbiol. Rev. 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Tzeng, A.; Tzeng, T.H.; Vasdev, S.; Korth, K.; Healey, T.; Parvizi, J.; Saleh, K.J. Treating periprosthetic joint infections as biofilms: Key diagnosis and management strategies. Diagn. Microbiol. Infect. Dis. 2015, 81, 192–200. [Google Scholar] [CrossRef]
- Kheir, M.M.; Tan, T.L.; Higuera, C.; George, J.; Della Valle, C.J.; Shen, M.; Parvizi, J. Periprosthetic joint infections caused by enterococci have poor outcomes. J. Arthroplast. 2017, 32, 933–947. [Google Scholar] [CrossRef] [PubMed]
- De Sanctis, J.; Teixeira, L.; Van Duin, D.; Odio, C.; Hall, G.; Tomford, J.W.; Perez, F.; Rudin, S.D.; Bonomo, R.A.; Barsoum, W.K. Complex prosthetic joint infections due to carbapenemase-producing Klebsiella pneumoniae: A unique challenge in the era of untreatable infections. Int. J. Infect. Dis. 2014, 25, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Howlin, R.; Brayford, M.; Webb, J.; Cooper, J.; Aiken, S.; Stoodley, P. Antibiotic-loaded synthetic calcium sulfate beads for prevention of bacterial colonization and biofilm formation in periprosthetic infections. Antimicrob. Agents Chemother. 2015, 59, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.W. Biofilm theory can guide the treatment of device-related orthopaedic infections. Clin. Orthop. Relat. Res.® 2005, 437, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Gristina, A.G.; Costerton, J. Bacterial adherence to biomaterials and tissue. The significance of its role in clinical sepsis. JBJS 1985, 67, 264–273. [Google Scholar] [CrossRef]
- Jämsen, E.; Huhtala, H.; Puolakka, T.; Moilanen, T. Risk factors for infection after knee arthroplasty: A register-based analysis of 43,149 cases. JBJS 2009, 91, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Parvizi, J.; Saleh, K.J.; Ragland, P.S.; Pour, A.E.; Mont, M.A. Efficacy of antibiotic-impregnated cement in total hip replacement. Acta Orthop. 2008, 79, 335–341. [Google Scholar] [CrossRef]
- McPherson, E.; Dipane, M.; Sherif, S. Dissolvable antibiotic beads in treatment of periprosthetic joint infection and revision arthroplasty-the use of synthetic pure calcium sulfate (Stimulan®) impregnated with vancomycin & tobramycin. Reconstr. Rev. 2013, 3. [Google Scholar] [CrossRef]
- Lum, Z.C.; Pereira, G.C. Local bio-absorbable antibiotic delivery in calcium sulfate beads in hip and knee arthroplasty. J. Orthop. 2018, 15, 676–678. [Google Scholar] [CrossRef]
- Mandell, J.B.; Orr, S.; Koch, J.; Nourie, B.; Ma, D.; Bonar, D.D.; Shah, N.; Urish, K.L. Large variations in clinical antibiotic activity against Staphylococcus aureus biofilms of periprosthetic joint infection isolates. J. Orthop. Res.® 2019, 37, 1604–1609. [Google Scholar] [CrossRef]
- Laycock, P.A.; Cooper, J.J.; Howlin, R.P.; Delury, C.; Aiken, S.; Stoodley, P. In vitro efficacy of antibiotics released from calcium sulfate bone void filler beads. Materials 2018, 11, 2265. [Google Scholar] [CrossRef]
- Dusane, D.H.; Brooks, J.R.; Sindeldecker, D.; Peters, C.W.; Li, A.; Farrar, N.R.; Diamond, S.M.; Knecht, C.S.; Plaut, R.D.; Delury, C. Complete Killing of Agar Lawn Biofilms by Systematic Spacing of Antibiotic-Loaded Calcium Sulfate Beads. Materials 2019, 12, 4052. [Google Scholar] [CrossRef]
- Jiranek, W.A.; Hanssen, A.D.; Greenwald, A.S. Antibiotic-loaded bone cement for infection prophylaxis in total joint replacement. J. Bone Jt. Surg. 2006, 88, 2487–2500. [Google Scholar] [CrossRef] [PubMed]
- Kenna, D.M.; Irojah, B.B.; Mudge, K.; Eveler, K. Absorbable Antibiotic Beads Prophylaxis in Immediate Breast Reconstruction. Plast. Reconstr. Surg. 2018, 141, 486e–492e. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, J.M.; Logue, M.E.; Kunkel, R.; Demas, C.P. Off-label Usage of Absorbable Beads Containing Antibiotics for Prevention of Surgical Site Infections. Wounds 2017, 29, E84–E87. [Google Scholar] [CrossRef] [PubMed]
- Kallala, R.; Harris, W.E.; Ibrahim, M.; Dipane, M.; McPherson, E. Use of Stimulan absorbable calcium sulphate beads in revision lower limb arthroplasty: Safety profile and complication rates. Bone Jt. Res. 2018, 7, 570–579. [Google Scholar] [CrossRef] [PubMed]
- Maale, G.E.; Eager, J.J.; Mohammadi, D.K.; Calderon, F.A. Elution Profiles of Synthetic CaSO. Eur. J. Drug Metab. Pharmacokinet. 2020, 1–9. [Google Scholar] [CrossRef]
- Geladari, A.; Simitsopoulou, M.; Antachopoulos, C.; Roilides, E. Dose-Dependent Synergistic Interactions of Colistin with Rifampin, Meropenem, and Tigecycline against Carbapenem-Resistant Klebsiella pneumoniae Biofilms. Antimicrob. Agents Chemother. 2019, 63. [Google Scholar] [CrossRef]
- Houlihan, H.H.; Mercier, R.C.; Rybak, M.J. Pharmacodynamics of vancomycin alone and in combination with gentamicin at various dosing intervals against methicillin-resistant Staphylococcus aureus-infected fibrin-platelet clots in an in vitro infection model. Antimicrob. Agents Chemother. 1997, 41, 2497–2501. [Google Scholar] [CrossRef]
- Douthit, C.; Gudenkauf, B.; Hamood, A.; Mudaliar, N.; Caroom, C.; Jenkins, M. Effects of powdered rifampin and vancomycin solutions on biofilm production of staphylococcus aureus on orthopedic implants. J. Clin. Orthop. Trauma 2020, 11, S113–S117. [Google Scholar] [CrossRef]
- Pavoni, G.L.; Giannella, M.; Falcone, M.; Scorzolini, L.; Liberatore, M.; Carlesimo, B.; Serra, P.; Venditti, M. Conservative medical therapy of prosthetic joint infections: Retrospective analysis of an 8-year experience. Clin. Microbiol. Infect. 2004, 10, 831–837. [Google Scholar] [CrossRef]
- Kresken, M.; Körber-Irrgang, B. Performance of the Etest for susceptibility testing of Enterobacterales (Enterobacteriaceae) and Pseudomonas aeruginosa towards ceftazidime-avibactam. J. Clin. Microbiol. 2018, 56, e00528-18. [Google Scholar] [CrossRef]
- Kahlmeter, G.; Brown, D. Chapter 9. Laboratory control of antimicrobial therapy. In Antibiotic and Chemotherapy: Anti-infective Agents and Their Use in Therapy, 8th eds.; Finch, R.G., Greenwood, D., Norrby, S.R., Whitley, R.J., Eds.; Churchill Livingstone: London, UK, 2003; pp. 115–122. [Google Scholar]
- Li, J.; Liu, F.; Wang, Q.; Ge, P.; Woo, P.C.; Yan, J.; Zhao, Y.; Gao, G.F.; Liu, C.H.; Liu, C. Genomic and transcriptomic analysis of NDM-1 Klebsiella pneumoniae in spaceflight reveal mechanisms underlying environmental adaptability. Sci. Rep. 2014, 4, 6216. [Google Scholar] [CrossRef] [PubMed]
- Warn, P.; Thommes, P.; Vaddi, S.; Corbett, D.; Coles, D.; Vaccaro, L.; Lister, T.; Parr Jr, T. In Vivo Efficacy of Combinations of Novel Antimicrobial Peptide Spr741 and Rifampicin in Short-Duration Murine Thigh Infection Models of Gram-Negative Bacterial Infection. Poster Monday-561. In Proceedings of the ASM Microbe 2016—American Society for Microbiology Conference, Boston, CA, USA, 16–20 June 2016. [Google Scholar]
- Chen, X.; Liu, Y.; Wang, C.; Hu, X.; Wu, Y.; Zhang, Y.; Bian, C.; You, X.; Hu, L. Synthesis and in vitro activity of asymmetric indole-based bisamidine compounds against Gram-positive and Gram-negative pathogens. Bioorg. Med. Chem. Lett. 2020, 30, 126887. [Google Scholar] [CrossRef]
- Munson, E.; Huband, M.D.; Castanheira, M.; Fedler, K.A.; Flamm, R.K. Determination of MIC and disk diffusion quality control guidelines for meropenem–vaborbactam, a novel carbapenem/boronic acid β-lactamase inhibitor combination. Diagn. Microbiol. Infect. Dis. 2018, 90, 324–328. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, M.; Payasi, A. Antimicrobial susceptibility patterns and molecular characterization of Klebsiella pneumoniae clinical isolates from north Indian patients. Int. J. Med. Med. Sci. 2013, 46, 1218–1224. [Google Scholar]
- Ng, S.M.S.; Sioson, J.S.P.; Yap, J.M.; Ng, F.M.; Ching, H.S.V.; Teo, J.W.P.; Jureen, R.; Hill, J.; Chia, C.S.B. Repurposing Zidovudine in combination with Tigecycline for treating carbapenem-resistant Enterobacteriaceae infections. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, A.; Thänert, R.; Burnham, C.-A.D.; Dantas, G. In vitro activity of meropenem/piperacillin/tazobactam triple combination therapy against clinical isolates of Staphylococcus aureus, Staphylococcus epidermidis, Staphylococcus pseudintermedius and vancomycin-resistant Enterococcus spp. Int. J. Antimicrob. Agents 2020, 55, 105864. [Google Scholar] [CrossRef]
- Naghili, H.; Tajik, H.; Mardani, K.; Rouhani, S.M.R.; Ehsani, A.; Zare, P. Validation of drop plate technique for bacterial enumeration by parametric and nonparametric tests. Vet Res Forum. 2013, 4, 179–183. [Google Scholar]
- Ben-David, A.; Davidson, C.E. Estimation method for serial dilution experiments. J. Microbiol. Methods 2014, 107, 214–221. [Google Scholar] [CrossRef]
- Desai, H.; Wong, R.; Pasha, A.K. A novel way of treating multidrug-resistant enterococci. N. Am. J. Med. Sci. 2016, 8, 229. [Google Scholar] [CrossRef]
- Tseng, S.-W.; Chi, C.-Y.; Chou, C.-H.; Wang, Y.-J.; Liao, C.-H.; Ho, C.-M.; Lin, P.-C.; Ho, M.-W.; Wang, J.-H. Eight years experience in treatment of prosthetic joint infections at a teaching hospital in Central Taiwan. J. Microbiol. Immunol. Infect. 2012, 45, 363–369. [Google Scholar] [CrossRef]
- Martinez-Pastor, J.; Vilchez, F.; Pitart, C.; Sierra, J.; Soriano, A. Antibiotic resistance in orthopaedic surgery: Acute knee prosthetic joint infections due to extended-spectrum beta-lactamase (ESBL)-producing Enterobacteriaceae. Eur. J. Clin. Microbiol. Infect. Dis. 2010, 29, 1039–1041. [Google Scholar] [CrossRef]
- Cooper, J.J.; Florance, H.; McKinnon, J.L.; Laycock, P.A.; Aiken, S.S. Elution profiles of tobramycin and vancomycin from high-purity calcium sulphate beads incubated in a range of simulated body fluids. J. Biomater. Appl. 2016, 31, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Aiken, S.S.; Cooper, J.J.; Florance, H.; Robinson, M.T.; Michell, S. Local release of antibiotics for surgical site infection management using high-purity calcium sulfate: An in vitro elution study. Surg. Infect. 2015, 16, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Kanellakopoulou, K.; Panagopoulos, P.; Giannitsioti, E.; Tsaganos, T.; Carrer, D.P.; Efstathopoulos, N.; Giamarellos-Bourboulis, E.J. In vitro elution of daptomycin by a synthetic crystallic semihydrate form of calcium sulfate, stimulan. Antimicrob. Agents Chemother. 2009, 53, 3106–3107. [Google Scholar] [CrossRef] [PubMed]
- Panagopoulos, P.; Tsaganos, T.; Plachouras, D.; Carrer, D.P.; Papadopoulos, A.; Giamarellou, H.; Kanellakopoulou, K. In vitro elution of moxifloxacin and fusidic acid by a synthetic crystallic semihydrate form of calcium sulphate (StimulanTM). Int. J. Antimicrob. Agents 2008, 32, 485–487. [Google Scholar] [CrossRef] [PubMed]
- McConoughey, S.J.; Howlin, R.; Granger, J.F.; Manring, M.M.; Calhoun, J.H.; Shirtliff, M.; Kathju, S.; Stoodley, P. Biofilms in periprosthetic orthopedic infections. Future Microbiol. 2014, 9, 987–1007. [Google Scholar] [CrossRef]
- Zimmerli, W.; Sendi, P. Role of rifampin against staphylococcal biofilm infections in vitro, in animal models, and in orthopedic-device-related infections. Antimicrob. Agents Chemother. 2019, 63, e01746-18. [Google Scholar] [CrossRef] [PubMed]
- Tyers, M.; Wright, G.D. Drug combinations: A strategy to extend the life of antibiotics in the 21st century. Nat. Rev. Microbiol. 2019, 17, 141–155. [Google Scholar] [CrossRef]
- Karam, G.; Chastre, J.; Wilcox, M.H.; Vincent, J.-L. Antibiotic strategies in the era of multidrug resistance. Crit. Care 2016, 20, 136. [Google Scholar] [CrossRef]
- Zavascki, A.P.; Bulitta, J.B.; Landersdorfer, C.B. Combination therapy for carbapenem-resistant Gram-negative bacteria. Expert Rev. Anti-Infect. Ther. 2013, 11, 1333–1353. [Google Scholar] [CrossRef]
- Thieme, L.; Hartung, A.; Tramm, K.; Klinger-Strobel, M.; Jandt, K.D.; Makarewicz, O.; Pletz, M.W. MBEC Versus MBIC: The Lack of Differentiation between Biofilm Reducing and Inhibitory Effects as a Current Problem in Biofilm Methodology. Biol. Proced. Online 2019, 21, 18. [Google Scholar] [CrossRef]
- Castaneda, P.; McLaren, A.; Tavaziva, G.; Overstreet, D. Biofilm antimicrobial susceptibility increases with antimicrobial exposure time. Clin. Orthop. Relat. Res.® 2016, 474, 1659–1664. [Google Scholar] [CrossRef]
- Nicolau, D.P. Optimizing outcomes with antimicrobial therapy through pharmacodynamic profiling. J. Infect. Chemother. 2003, 9, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.M.; Rotschafer, J.C.; Behrens, F. Use of vancomycin and tobramycin polymethylmethacrylate impregnated beads in the management of chronic osteomyelitis. Drug Intell. Clin. Pharm. 1988, 22, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Henry, S.L.; Galloway, K.P. Local antibacterial therapy for the management of orthopaedic infections. Clin. Pharmacokinet. 1995, 29, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Bistolfi, A.; Massazza, G.; Verné, E.; Massè, A.; Deledda, D.; Ferraris, S.; Miola, M.; Galetto, F.; Crova, M. Antibiotic-loaded cement in orthopedic surgery: A review. ISRN Orthop. 2011, 2011. [Google Scholar] [CrossRef]
- Van de Belt, H.; Neut, D.; Schenk, W.; Van Horn, J.R.; Van de Mei, H.C.; Busscher, H.J. Infection of orthopedic implants and the use of antibiotic-loaded bone cements: A review. Acta Orthop. Scand. 2001, 72, 557–571. [Google Scholar] [CrossRef]
- Gogia, J.S.; Meehan, J.P.; Di Cesare, P.E.; Jamali, A.A. Local antibiotic therapy in osteomyelitis. Semin. Plast. Surg. 2009, 23, 100–107. [Google Scholar] [CrossRef]







© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).