Biomechanical Loading Comparison between Titanium and Bioactive Resorbable Screw Systems for Fixation of Intracapsular Condylar Head Fractures

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Materials
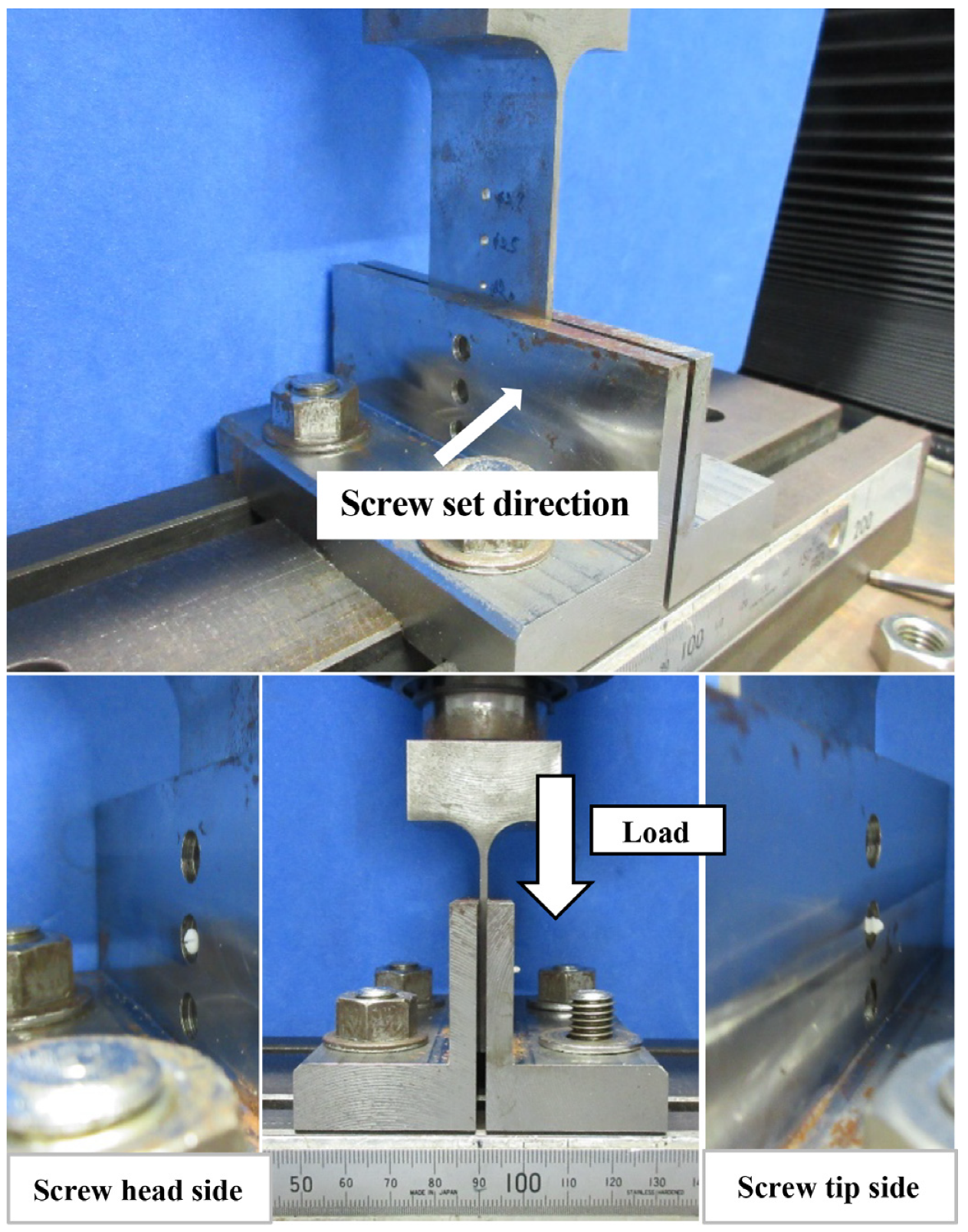
2.2. Evaluation of Shear Strength of Titanium and Bioresorbable Screw
Sample Preparation and Measurement
2.3. Biomechanical Loading Evaluation
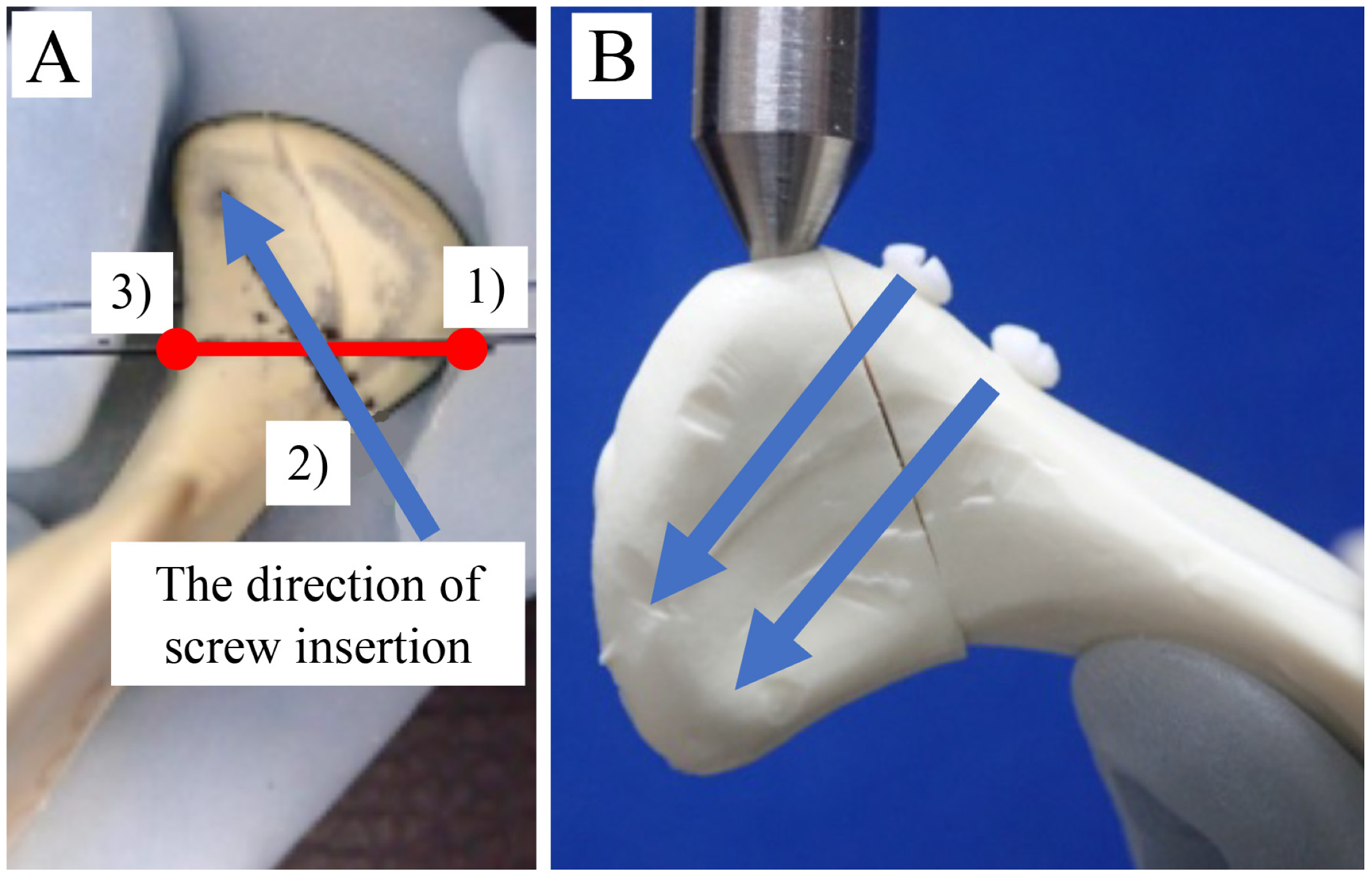
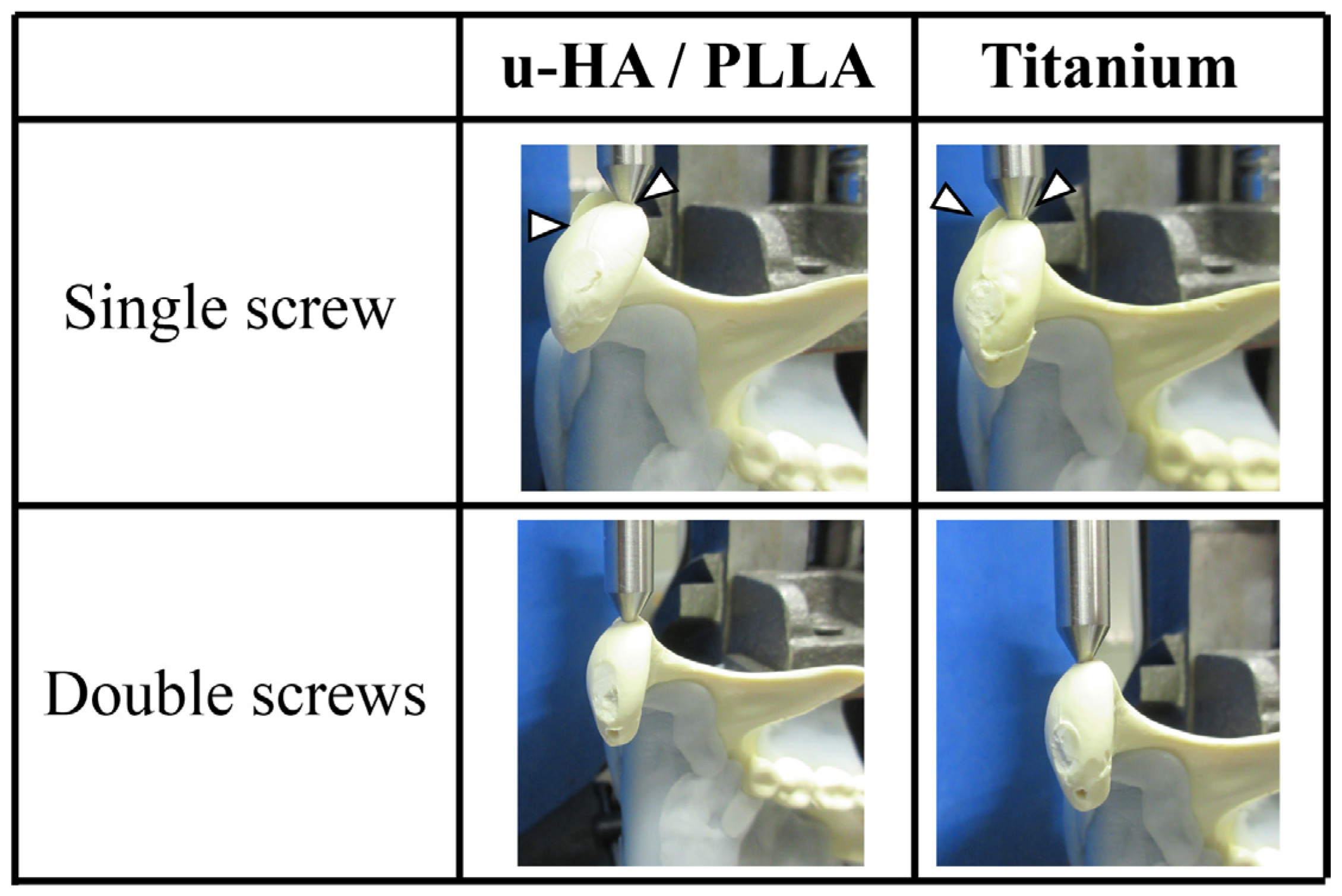
2.3.1. Sample Preparation
2.3.2. Fixation Method for Mandibular Condylar Fracture
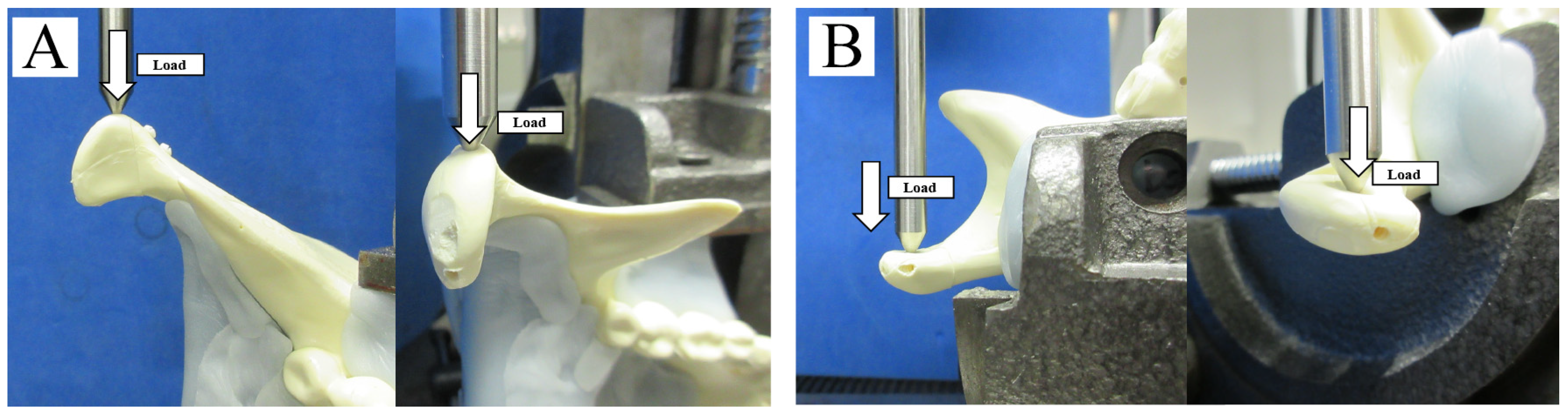
2.3.3. Biomechanical Loading Test
2.4. Statistical Analysis
3. Results
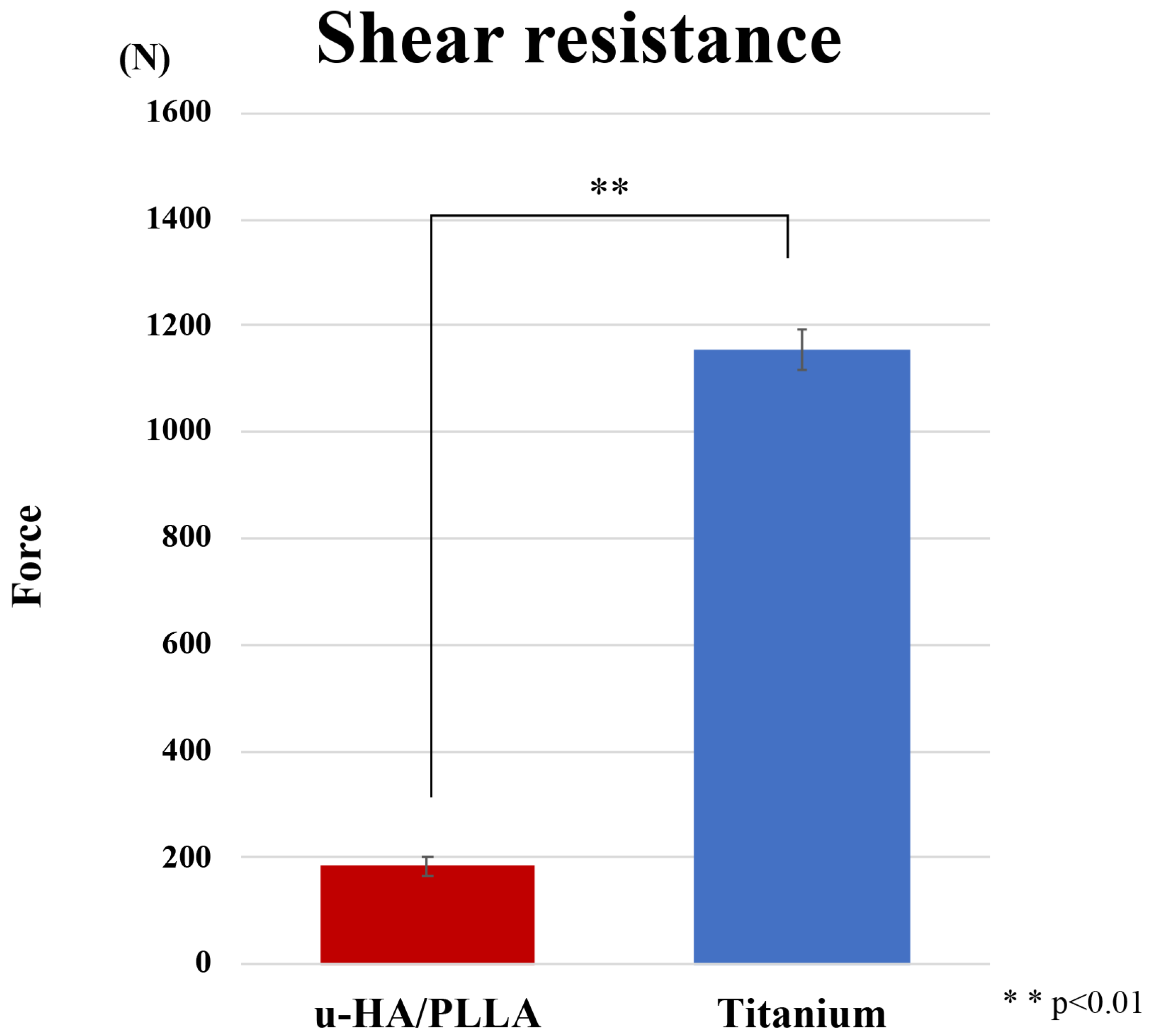
3.1. Strength Evaluation
3.2. Biomechanical Loading Evaluation
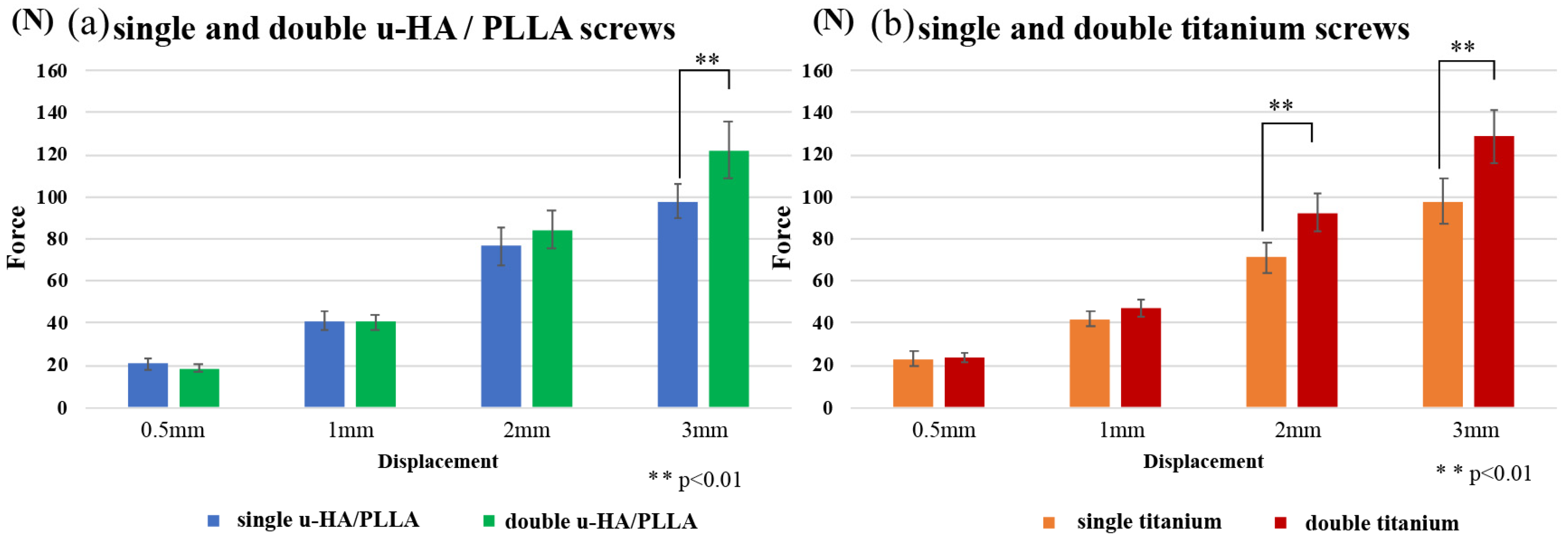
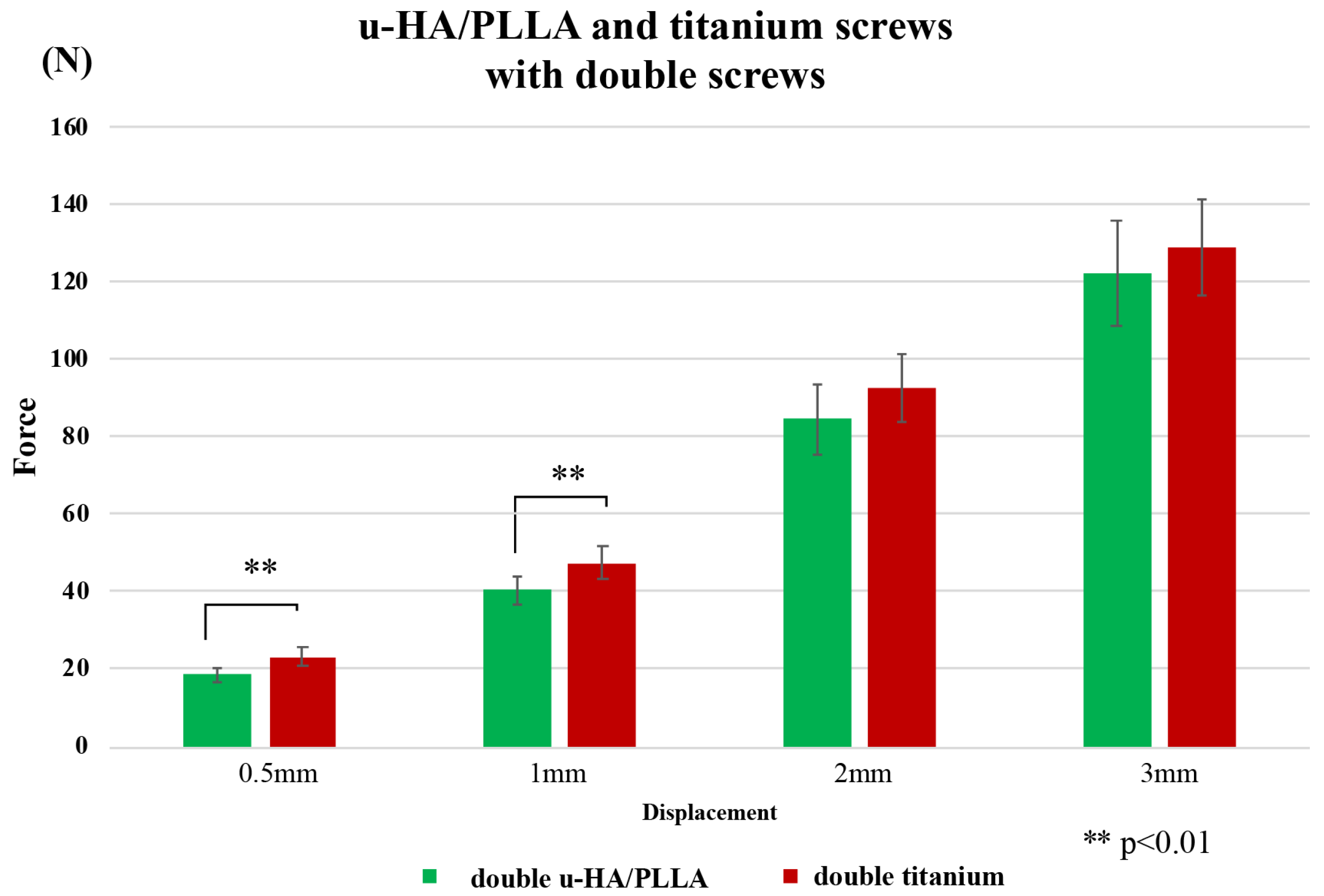
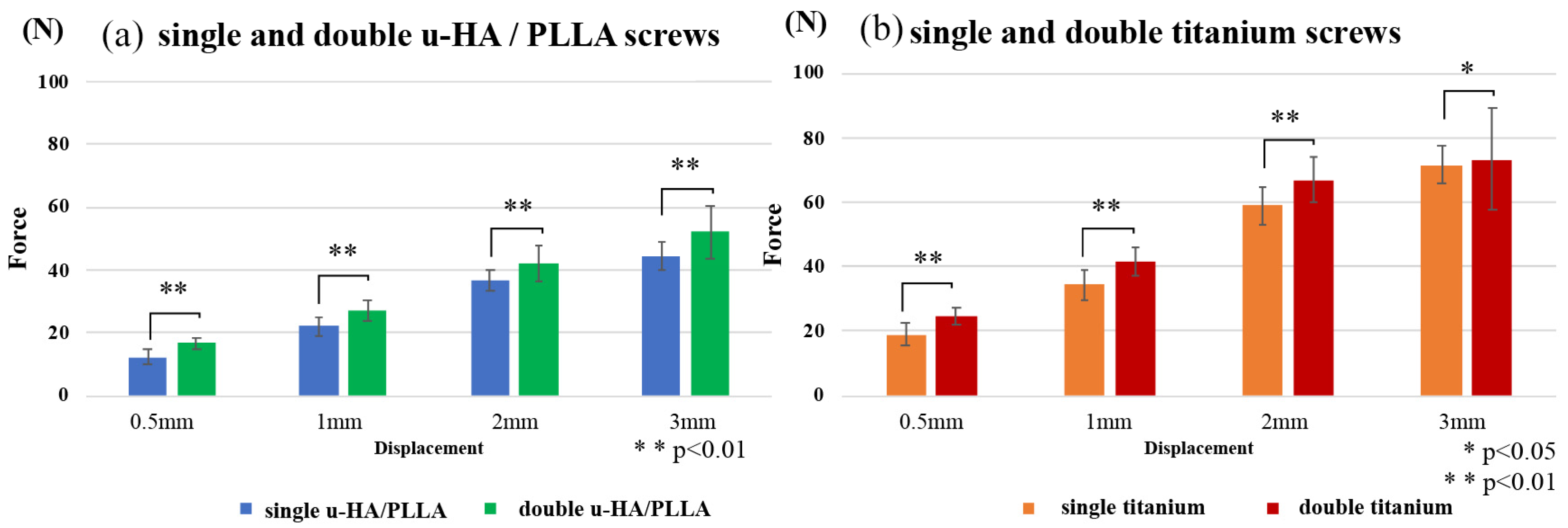
3.2.1. Horizontal Loading Test
3.2.2. Vertical Loading Test
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Sukegawa, S.; Saika, M.; Kanno, T.; Nakano, K.; Takabatake, K.; Kawai, H.; Nagatsuka, H.; Furuki, Y. Do the Presence of Mandibular Third Molar and the Occlusal Support Affect the Occurrence and the Mode of Mandibular Condylar Fractures? J. Hard Tissue Biol. 2019, 28, 377–382. [Google Scholar] [CrossRef]
- Loukota, R.A.; Neff, A.; Rasse, M. Nomenclature/classification of fractures of the mandibular condylar head. Br. J. Oral Maxillofac. Surg. 2010, 48, 477–478. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R. Open versus closed reduction: Diacapitular fractures of the mandibular condyle. Oral Maxillofac. Surg. 2012, 16, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Kolk, A.; Neff, A. Long-term results of ORIF of condylar head fractures of the mandible: A prospective 5-year follow-up study of small-fragment positional-screw osteosynthesis (SFPSO). J. Craniomaxillofac. Surg. 2015, 43, 452–461. [Google Scholar] [CrossRef]
- Guo, S.; Zhou, W.; Wan, L.; Yuan, H.; Yuan, Y.; Du, Y.; Jiang, H. Computer-aided design-based preoperative planning of screw osteosynthesis for type B condylar head fractures: A preliminary study. J. Craniomaxillofac. Surg. 2016, 44, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Pilling, E.; Schneider, M.; Mai, R.; Loukota, R.A.; Eckelt, U. Minimally invasive fracture treatment with cannulated lag screws in intracapsular fractures of the condyle. J. Oral Maxillofac. Surg. 2006, 64, 868–872. [Google Scholar] [CrossRef]
- Xie, S.T.; Singhal, D.; Chen, C.T.; Chen, Y.R. Functional and radiologic outcome of open reduction and internal fixation of condylar head and neck fractures using miniplate or microplate system. Ann. Plast. Surg. 2013, 71, S61–S66. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Yang, C.; He, D.; Zhang, S.; Jiang, B. Soft tissue reduction during open treatment of intracapsular condylar fracture of the temporomandibular joint: Our institution’s experience. J. Oral Maxillofac. Surg. 2010, 68, 2189–2195. [Google Scholar] [CrossRef]
- Smolka, W.; Cornelius, C.-P.; Lechler, C. Resorption behaviour of the articular surface dome and functional outcome after open reduction and internal fixation of mandibular condylar head fractures using small-fragment positional screws. J. Craniomaxillofac. Surg. 2018, 46, 1953–1959. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Masui, M.; Furuki, Y. Complications of a poly-l-lactic acid and polyglycolic acid osteosynthesis device for internal fixation in maxillofacial surgery. Odontology 2018, 106, 360–368. [Google Scholar] [CrossRef]
- Shikinami, Y.; Okuno, M. Bioresorbable devices made of forged composites of hydroxyapatite (HA) particles and poly-L-lactide (PLLA): Part I. Basic characteristics. Biomaterials 1999, 20, 859–877. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kawai, H.; Nakano, K.; Takabatake, K.; Kanno, T.; Nagatsuka, H.; Furuki, Y. Advantage of Alveolar Ridge augmentation with bioactive/bioresorbable screws made of composites of unsintered hydroxyapatite and poly-L-lactide. Materials 2019, 12, 3681. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kawai, H.; Nakano, K.; Kanno, T.; Takabatake, K.; Nagatsuka, H.; Furuki, Y. Feasible advantage of bioactive/bioresorbable devices made of forged composites of hydroxyapatite particles and poly-L-lactide in alveolar bone augmentation: A preliminary study. Int. J. Med. Sci. 2019, 16, 311–317. [Google Scholar] [CrossRef] [PubMed]
- De Santis, R.; Sarracino, F.; Mollica, F.; Netti, P.A.; Ambrosio, L.; Nicolais, L. Continuous fibre reinforced polymers as connective tissue replacement. Compos. Sci. Technol. 2004, 64, 861–871. [Google Scholar] [CrossRef]
- Mühlberger, G.; Svejda, M.; Lottersberger, C.; Emshoff, R.; Putz, R.; Kuhn, V. Mineralization density and apparent density in mandibular condyle bone. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2009, 107, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Yamamoto, N.; Nakano, K.; Takabatake, K.; Kawai, H.; Nagatsuka, H.; Furuki, Y. Biomechanical loading comparison between titanium and unsintered hydroxyapatite/poly-L-lactide plate system for fixation of mandibular subcondylar fractures. Materials 2019, 12, 1557. [Google Scholar] [CrossRef]
- Neff, A.; Kolk, A.; Meschke, F.; Deppe, H.; Horch, H.H. Kleinfragmentschrauben vs. Plattenosteosynthese bei Gelenkwalzenfrakturen—Vergleich funktioneller Ergebnisse mit MRT und Achsiographie. Mund. Kiefer. Gesichtschir. 2005, 9, 80–88. [Google Scholar] [CrossRef]
- Vesnaver, A. Open reduction and internal fixation of intra-articular fractures of the mandibular condyle: Our first experiences. J. Oral Maxillofac. Surg. 2008, 66, 2123–2129. [Google Scholar] [CrossRef]
- Pereira, M.D.; Marques, A.; Ishizuka, M.; Keira, S.M.; Brenda, E.; Wolosker, A.B. Surgical treatment of the fractured and dislocated condylar process of the mandible. J. Cranio-Maxillofac. Surg. 1995, 23, 369–376. [Google Scholar] [CrossRef]
- McLeod, N.M.H.; Saeed, N.R. Treatment of fractures of the mandibular condylar head with ultrasound-activated resorbable pins: Early clinical experience. Br. J. Oral Maxillofac. Surg. 2016, 54, 872–877. [Google Scholar] [CrossRef]
- Wang, W.H.; Deng, J.Y.; Zhu, J.; Li, M.; Xia, B.; Xu, B. Computer-assisted virtual technology in intracapsular condylar fracture with two resorbable long-screws. Br. J. Oral Maxillofac. Surg. 2013, 51, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Brignardello-Petersen, R. Resorbable plates and titanium plates might result in similar levels of postoperative pain after orthognathic surgery. J. Am. Dent. Assoc. 2018, 149, e54. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Nagano, D.; Shibata, A.; Sukegawa-Takahashi, Y.; Furuki, Y. The Clinical Feasibility of Newly Developed Thin Flat-Type Bioresorbable Osteosynthesis Devices for the Internal Fixation of Zygomatic Fractures: Is There a Difference in Healing Between Bioresorbable Materials and Titanium Osteosynthesis? J. Craniofac. Surg. 2016, 27, 2124–2129. [Google Scholar] [CrossRef] [PubMed]
- Kanno, T.; Sukegawa, S.; Karino, M.; Furuki, Y. Navigation-Assisted Orbital Trauma Reconstruction Using a Bioactive Osteoconductive/Bioresorbable u-HA/PLLA System. J. Maxillofac. Oral Surg. 2019, 18, 329–338. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Koyama, Y.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Masui, M.; Tanaka, S.; Furuki, Y. Precision of Post-Traumatic Orbital Reconstruction Using Unsintered Hydroxyapatite Particles/Poly-L-Lactide Composite Bioactive/Resorbable Mesh Plate with and without Navigation: A Retrospective Study. J. Hard Tissue Biol. 2017, 26, 274–280. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Shibata, A.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Sakaida, K.; Furuki, Y. Use of the bioactive resorbable plate system for zygoma and zygomatic arch replacement and fixation with modified Crockett’s method for maxillectomy: A technical note. Mol. Clin. Oncol. 2017, 7, 47–50. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Kawai, H.; Shibata, A.; Matsumoto, K.; Sukegawa-Takahashi, Y.; Sakaida, K.; Nagatsuka, H.; Furuki, Y. Surgical Treatment and Dental Implant Rehabilitation after the Resection of an Osseous Dysplasia. J. Hard Tissue Biol. 2016, 25, 437–441. [Google Scholar] [CrossRef]
- Shikinami, Y.; Okuno, M. Bioresorbable devices made of forged composites of hydroxyapatite (HA) particles and poly L-lactide (PLLA). Part II: Practical properties of miniscrews and miniplates. Biomaterials 2001, 22, 3197–3211. [Google Scholar] [CrossRef]
- Neff, A.; Kolk, A.; Deppe, H.; Horch, H.H. New aspects for indications of surgical management of intra-articular and high temporomandibular dislocation fractures. Mund. Kiefer. Gesichtschir. 1999, 3, 24–29. [Google Scholar] [CrossRef]
- De Souza, G.M.; Rodrigues, D.C.; Celegatti Filho, T.S.; Moreira, R.W.F.; Falci, S.G.M. In-vitro comparison of mechanical resistance between two straight plates and a Y-plate for fixation of mandibular condyle fractures. J. Cranio-Maxillofac. Surg. 2018, 46, 168–172. [Google Scholar] [CrossRef]
- Matsusue, Y.; Nakamura, T.; Iida, H.; Shimizu, K. A long-term clinical study on drawn poly-L-lactide implants in orthopaedic surgery. J. Long Term Eff. Med. Implants 1997, 7, 119–137. [Google Scholar]
- Bergsma, J.E.; De Bruijn, W.C.; Rozema, F.R.; Bos, R.R.M.; Boering, G. Late degradation tissue response to poly(l-lactide) bone plates and screws. Biomaterials 1995, 16, 25–31. [Google Scholar] [CrossRef]
- Sukegawa, S.; Kanno, T.; Katase, N.; Shibata, A.; Takahashi, Y.; Furuki, Y. Clinical evaluation of an unsintered hydroxyapatite/poly-l-lactide osteoconductive composite device for the internal fixation of maxillofacial fractures. J. Craniofac. Surg. 2016, 27, 1391–1397. [Google Scholar] [CrossRef] [PubMed]
- Sukegawa, S.; Kanno, T.; Kawai, H.; Shibata, A.; Takahashi, Y.; Nagatsuka, H.; Furuki, Y. Long-Term Bioresorption of Bone Fixation Devices Made from Composites of Unsintered Hydroxyapatite Particles and Poly-L-Lactide. J. Hard Tissue Biol. 2015, 24, 219–224. [Google Scholar] [CrossRef]









© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sukegawa, S.; Yamamoto, N.; Nakano, K.; Takabatake, K.; Kawai, H.; Kanno, T.; Nagatsuka, H.; Furuki, Y. Biomechanical Loading Comparison between Titanium and Bioactive Resorbable Screw Systems for Fixation of Intracapsular Condylar Head Fractures. Materials 2020, 13, 3153. https://doi.org/10.3390/ma13143153
Sukegawa S, Yamamoto N, Nakano K, Takabatake K, Kawai H, Kanno T, Nagatsuka H, Furuki Y. Biomechanical Loading Comparison between Titanium and Bioactive Resorbable Screw Systems for Fixation of Intracapsular Condylar Head Fractures. Materials. 2020; 13(14):3153. https://doi.org/10.3390/ma13143153
Chicago/Turabian StyleSukegawa, Shintaro, Norio Yamamoto, Keisuke Nakano, Kiyofumi Takabatake, Hotaka Kawai, Takahiro Kanno, Hitoshi Nagatsuka, and Yoshihiko Furuki. 2020. "Biomechanical Loading Comparison between Titanium and Bioactive Resorbable Screw Systems for Fixation of Intracapsular Condylar Head Fractures" Materials 13, no. 14: 3153. https://doi.org/10.3390/ma13143153
APA StyleSukegawa, S., Yamamoto, N., Nakano, K., Takabatake, K., Kawai, H., Kanno, T., Nagatsuka, H., & Furuki, Y. (2020). Biomechanical Loading Comparison between Titanium and Bioactive Resorbable Screw Systems for Fixation of Intracapsular Condylar Head Fractures. Materials, 13(14), 3153. https://doi.org/10.3390/ma13143153