1. Introduction
Society depends on a whole range of infrastructure [
1]. Public infrastructure such as land, buildings, and facilities is defined into four areas. The first is transport infrastructure, such as roads, railways, waterways, airports and related facilities. The second, technical infrastructure, comprises lines, structures and operationally related specialised equipment (e.g., water mains, reservoirs), systems to reduce the risk of natural or other disasters, systems and disposal facilities with waste, transformer stations, power lines, communication lines in public communication networks, and others. The third area includes civic amenities, such as buildings, facilities and land used; for example, for education, social services and family care, and health services. The fourth area includes public spaces established or used in the public interest [
2]. Over time, some infrastructure elements and parts that are fundamentally essential to society have been called critical infrastructure [
3]. Critical infrastructure is defined as a vital infrastructure element or a system of essential infrastructure elements where the disruption of its function would severely impact state security, the basic living needs of the population, people’s health and the economy [
4].
Furthermore, sectoral and cross-sectional criteria are determined according to the laws of the Czech Republic. Cross-sectional criteria include measures concerning victims, economic impact and public impact according to the affected population.
Conversely, sectoral standards are technical or operational values for determining the critical infrastructure element in different sectors [
4]. The critical infrastructure sectors include [
4]:
Energy supply;
Water supply;
Food industry and agriculture;
Health services;
Public administration;
Emergency services;
Financial market and currency;
Information and communication systems;
Transport.
Rehak et al. state that the protection of critical infrastructure in the Czech Republic has been implemented in crisis management [
5]. As can be seen from the list of sectoral criteria for critical infrastructure, the areas of energy and healthcare are highlighted. The energy sector includes electricity, natural gas, crude oil and petroleum products and central heating. In contrast, the healthcare sector includes healthcare facilities (the total number of acute beds is at least 2500) and the manufacture of medicinal products. Various disasters can disrupt critical infrastructure. The concept of a disaster differs in different countries and is defined in different ways. The International Disaster Database (EM-DAT) defines a disaster as a situation or event that exceeds local capacity and requires external assistance at the national or international level. It further states that it is an unforeseen and frequently sudden event that causes significant damage and human suffering. Although disasters are frequently caused by nature, they can also be of human origin [
6]. The International Federation of Red Cross and Red Crescent Societies [
7] defines a disaster as a sudden, catastrophic event that seriously disrupts the functioning of society and causes human, material, economic and environmental losses beyond the capacity of the community or society to cope with this event using their own resources.
The term disaster was defined by the Ministry of the Environment of the Czech Republic in the journal
PLANETA with the publication “Natural Disasters and Risks”, in 2005. The term disaster can be used in a narrow or broad sense. By a strict definition, a disaster is a process that leaves human casualties and material damage. Experts could not agree on how many victims and what amount of damage this should be. According to the terminology used by significant world organisations such as the United Nations, the World Bank and the European Bank, the number of victims must be at least 25 or the damage at least USD 25 million. However, one item is sufficient for the number of victims or material damage [
8].
Czech legislation also refers to terms such as “crisis situation” and “emergency”. An emergency means the harmful effects of forces and phenomena caused by human activities, natural influences and accidents that endanger life, health, property and the environment and require rescue and liquidation work [
9]. According to the Integrated Rescue System Act, a crisis situation means an emergency, disruption of critical infrastructure, or other hazards that result in a state of emergency [
4]. Threats are highly unpredictable, with a wide range of consequences (for example, blackouts) [
10].
Further definitions of a disaster can be found in the Disaster Definitions document by Kelman (2019) [
11].
As the title suggests, the main aim of the paper is focused on power outages. This term can also be found in use throughout the world as “blackout”, “power outage”, “power cut” and “electricity outage”. All these terms have the same meaning. Disruption by a large-scale power outage (blackout) is a crisis that extensively impacts all state functions, including threats to the lives and health of those dependent on devices supporting essential life functions. There can be many causes: extreme climatic events, transmission system instability, operator error, failure, accident, terrorist attacks with an impact on transmission systems, etc. The probability of a power outage increases in the case of a combination of the above factors. This crisis can cause other domino effects in transport, communication networks, drinking water supply, food, heat and fuel [
12]. For this paper, the same term will always be used for the above-mentioned terms, namely, “power outage”, and the definition given here will be considered.
Furthermore, various authors define large-scale power outages. Benes defines a blackout as a total power outage over a large area [
13]. This term indicates when a power outage occurred that disrupted the balance between electricity production and consumption and when the security of the supply was compromised [
14]. Brehovska states that a power outage affects people’s lives and the operation of the entire state, especially the economic development of the affected area. The peculiarity of a blackout is that the secondary consequences of the outage are several times greater than the consequences for the facilities that produce, transmit and distribute electricity. The cause of this is a domino effect, which arises from the interconnection of the entire critical infrastructure [
15]. In addition to the term power outage, the term blackout is sometimes used to mean a period when there is no electricity in a building or area [
16]. The word blackout implies a period of darkness (as in a city) caused by a power outage [
17]. Based on the Council Directive, electricity is a core sector of European critical infrastructure [
3]. Splichalova adds that its interdependence with and its effect on secondary sectors are very high [
18].
Hromada states that the energy sector and the services it provides belong among the fundamental pillars for the safe and reliable operation of all infrastructure while ensuring the needs of the population. The complexity and interconnection of the whole infrastructure are continually growing. However, within this interconnection, it is possible to identify a “building block”, without which all the infrastructure and the functionality provided by it would stop and subsequently collapse, and this building block is electricity. For this reason, the disruption of the electricity supply can rightly be considered one of the most critical threats to today’s society [
19]. Rehak et al. continue that the electricity sector is a unique critical infrastructure sector. Disruption or failure of its functions would have far-reaching effects on society and all dependent critical infrastructure sectors [
20]. Lervanos also confirms this citation in the publication “Uneven Resistance: Power Outage Time” [
21]. According to the authors’ references, it is clear that an electrical system represents significant infrastructure when its failure is a major threat to society. Therefore, it is logical that the following text analyses the fundamental aspects of how the electricity system works and what it consists of. The electricity system is a nationwide area system with a high degree of connections to the surrounding states’ electricity systems and is highly sensitive to the correct function and required interaction of its elements, which are closely related and interact with each other.
The most important elements of critical infrastructure in the energy sector can be ranked in terms of the transmission system [
4]:
- (a)
A transmission system with a voltage of at least 110 kV;
- (b)
A power station transmission system with a voltage of at least 110 kV;
- (c)
Technical dispatching control of the transmission system by an operator.
Very high voltage is then transformed into 35 kV or less and distributed through the distribution system to its final consumers. The most important critical electricity infrastructure sector elements can be also ranked in terms of distribution [
4]:
- (a)
110 kV (i.e., 110/110 kV, 110/22 kV and 110/35 kV 110/35 kV) lines and power lines for the 110 kV distribution system and 110 kV power lines are assessed according to their strategic importance in the distribution system;
- (b)
Technical dispatch of the distribution system operator.
Because electricity cannot be stored in significant quantities, the balance between production and consumption must be continuously maintained. The electricity system must continually ensure a balance over time with the changing magnitude of electricity consumption and production. This balance is provided by the electricity market and real-time transmission system operators [
22].
In the Czech Republic, the state aims to ensure a stable supply of electricity to customers. One of the documents approved in connection with the protection of critical infrastructure in energy is the State Energy Concept of the Czech Republic. In 2015, the Government of the Czech Republic approved this concept for the next 25 years. The main reason for supporting the State Energy Concept is to clearly articulate the state’s priorities and strategic intentions within the energy sector and thus provide investors, citizens and the state administration with stability in today’s turbulent and dynamic period [
23]. The State Energy Concept’s mission is to ensure uninterrupted energy supplies during a crisis to the extent required for the functioning of the most critical state components and the survival of the population.
Furthermore, this concept sets out the Czech energy sector’s strategic goals and protects critical infrastructure and critical energy systems in a broader context. As can be seen from the above text, electricity is an essential component of the state’s critical infrastructure. Power outages are a significant threat to any state. As a result of this event, total darkness occurs in the given location, and gradually, over time, there is a collapse of the entire society affected [
19]. Due to the sophisticated security system, the most probable reason for the occurrence of a large-scale power outage appears to be the concurrence of several significant causes simultaneously. The speed of the resumption of supplies also depends on the cause of the power failure. There should be marked physical damage to the infrastructure; the recovery time will be directly proportional to the extent of the damage in the order of days to weeks [
12].
The methodology of categorising and prioritising objects necessary for the renewal of large-scale electricity supplies after a blackout states how, with the time horizon, it is possible to restore the electricity supply. This methodology provides a type of scenario for when a blackout failure occurs and how to restore power to the area. As mentioned above, critical infrastructure has, according to Government Decree No. 432/2010 Coll. [
24] on the identification of a critical infrastructure element, nine defined elements. The disruption of the function of a critical infrastructure element or a system of critical infrastructure elements would have a serious impact on state security, the provision of the population’s basic living needs, the health of the inhabitants and the state economy. These elements of critical infrastructure are interconnected. In the event of a breach of energy in a given state, there is also an impact on other essential infrastructure elements. In this case, this may be the so-called cascade effect. One violation of a critical infrastructure component affects other elements, such as water management, healthcare, public administration, transport and others.
An example of a cascade effect is a violation of the energy element and its cascade effect on healthcare. The interconnection of the individual elements of critical infrastructure is within the framework of regional, national and transnational elements. In a globalised world, in which crisis incidents are becoming more frequent, more devastating and have a significant impact on the health and lives of societies. The quality of healthcare services, particularly including the operational capacity of hospitals, is crucial for the security of health [
25].
Further, attention will be focused on health services and the resulting healthcare facilities. A health service provider is a natural or legal person who is authorised to provide health services, whereas a healthcare facility is defined as premises intended to provide health services [
26]. The types of healthcare are preventive care, diagnostic care, dispensary care, medical care, medical rehabilitation care, nursing care, palliative care, pharmaceutical care and clinical–pharmaceutical care [
26].
As can be seen from the list of healthcare types, healthcare facilities do not only mean hospitals and medical facilities intended for treatment.
Healthcare facilities include:
Faculty hospitals;
Regional hospitals;
City hospitals;
Rehabilitation hospitals;
Hospitals with a polyclinic;
Psychiatric hospitals;
Healthcare facilities such as polyclinics;
Hospitals for long-term sickness;
Specialised centres providing health services;
Preventive care;
Rehabilitation care.
These healthcare facilities are defined based on Act No. 372/2011 Coll. [
26] on health services. In the event of a disaster, the affected population is dependent on health. Hospitals are expected to remain functioning during and in the immediate aftermath of disasters, as they are essential infrastructures in responding to such [
27]. Hospital buildings feature a high diversity of energy demands, e.g., thermal energy for heating buildings and domestic hot water, cooling for ventilation systems, electricity required to operate equipment, lighting, ventilation and air conditioning systems.
The aim of this article is to point out the significance of electricity supply to healthcare facilities. The first part of the paper is an introduction to the issue. The second part presents the methods and limits of the paper. The central part, the results, can be considered the introduction of an algorithm for assessing the healthcare facilities in times of a power outage. At the end of the paper, this algorithm is verified at healthcare facilities in the Czech Republic. We conclude that only 15% of the surveyed healthcare facilities are prepared for a power outage.
3. Results
This paper aims to present the algorithm for the evaluation of healthcare facilities. This method builds on the methodology for the categorisation and prioritisation of objects necessary for the resumption of the electricity supply after a blackout [
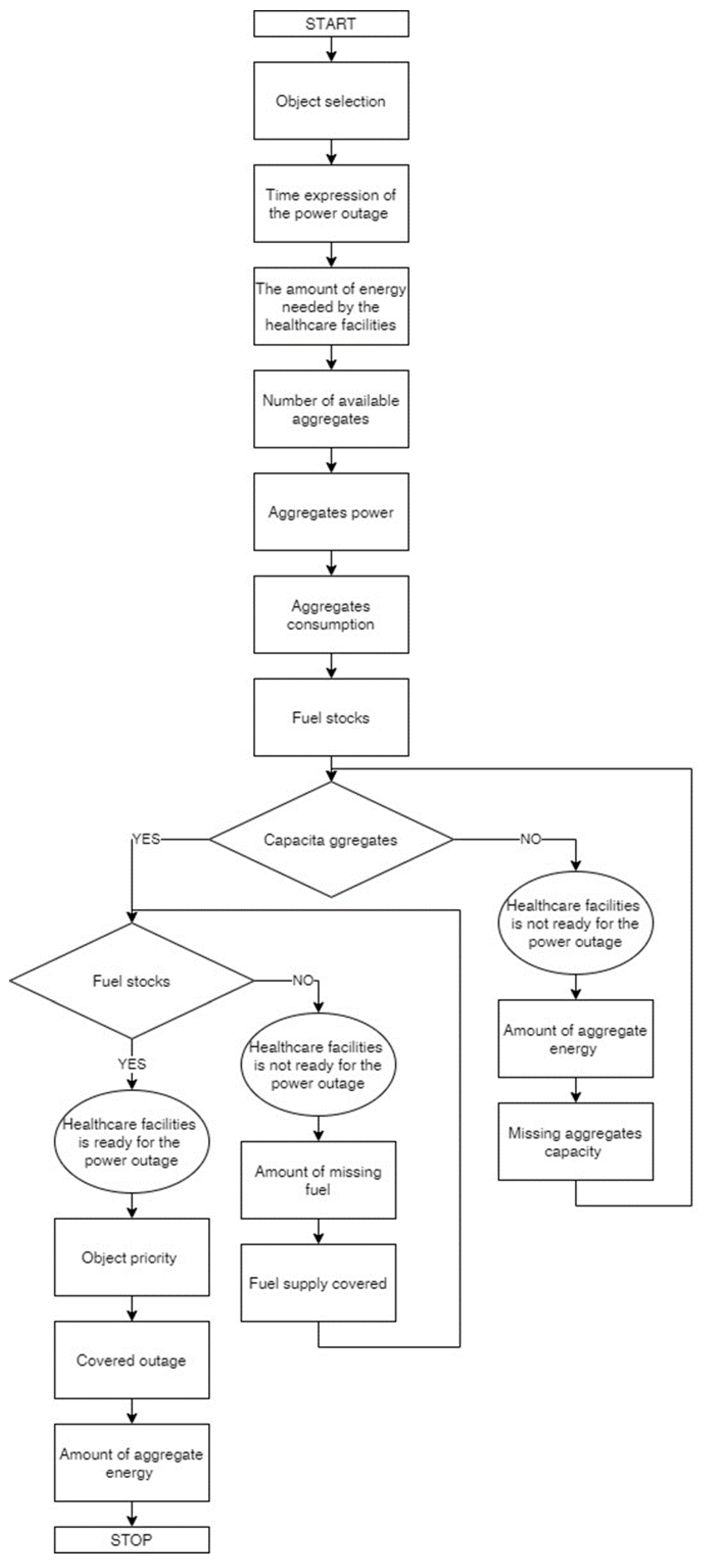
19]. The algorithm aims to determine the preparedness of the healthcare facilities to solve a power outage. It is an acute issue that can endanger thousands of lives that depend on electricity supplies in healthcare facilities.
First, the design of the algorithm for assessing the healthcare facilities to solve power outages is introduced (see
Figure 1). Second, the inputs and outputs are discussed in more detail.
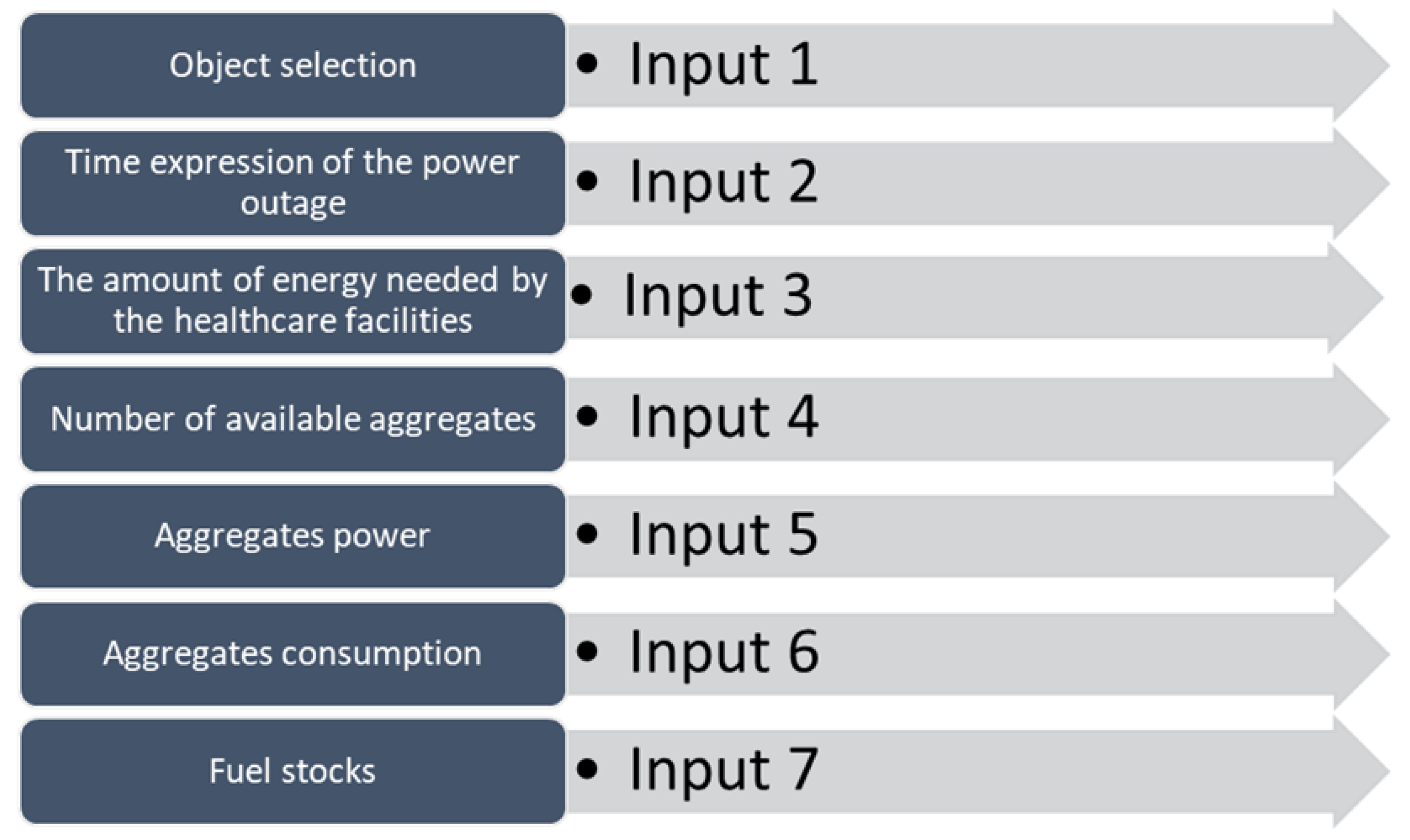
The primary aim of this paper is to design an algorithm to assess the healthcare facilities to solve power outages. These inputs are considered for the evaluation of medical facilities (see
Figure 2).
3.1. Input 1: Object Selection
According to Act No. 372/2011 Coll., the healthcare facilities are defined as when patients are provided with health care according to their condition in the Czech Republic. This paper builds on and expands the “Methodology of Categorisation and Prioritisation of Objects Necessary for the Resumption of the Electricity Supply after a Blackout.” Object categories were created, which were subsequently prioritised. To assess healthcare facilities in terms of their readiness to solve the power outage, they can be assessed according to
Table 2.
3.2. Input 2: Time Expression of the Power Outage
This input is the time expression of the length of the supply outage in hours. This input may vary depending on the expected size of the power outage. Therefore, it is an active part of assessing healthcare facilities to solve the power outage. This value was obtained from power engineers who can estimate the time without current due to the electrical system’s failure. Added to this value must be the time for restoration of the electricity supply. The determination of this value is linked to the methodology for categorisation and prioritisation of the objects necessary for the resumption of the electricity supply after a blackout (mentioned in
Table 1).
3.3. Input 3: The Amount of Energy Needed by Healthcare Facilities
The healthcare facilities determine the amount of healthcare device energy required for critical circuits. Each healthcare facility has a pre-designed critical circuit that will be powered in the event of a power outage. The healthcare facility will identify the buildings where this power supply is necessary and then colour-code the critical circuits’ sockets. The orange colour of the socket identifies essential circuits. These sockets are permanently powered by UPS means, which represent a continuous backup of voltage. The UPS power supply is connected to spare sources. The green colour of the socket identifies important circuits. These circuits are backed up by a spare source of electricity (unit). The socket’s yellow colour represents the isolated healthcare system, which is backed up by a spare source. The backup power outlets are used in operations where the patient’s life and health could be endangered, particularly in operating theatres, ICUs, neonatal wards, etc. The colour marking of drawers in healthcare is governed by Czech State Standard (33 2000-7-710) [
28].
3.4. Inputs 4–6: Information about Aggregates
The following three inputs are necessary to determine the baseline information to assess a healthcare facility’s readiness. To assess readiness in the event of a power failure, it is essential to consider that the healthcare facility has one or more units that supply critical circuits. Determining the correct number and power of the units is necessary for the proper functioning of the power supply in the event of a power failure.
An alternative source of electricity, aggregates or the unit, can burn diesel or petrol. The analysis of the evaluated healthcare facilities showed that all assessed healthcare facilities have units that burn diesel. Each unit has a label displaying basic information. The medical facility technicians will use this label to ascertain the unit’s maximum power and consumption at full power. The maximum power and maximum load consumption of the unit must always be considered. The label usually indicates the power in units of kVA and kW, where the unit of kW is calculated in the proposed evaluation system. Consumption with a 100% load is given in litres per hour.
As mentioned for Input 3, the selected critical circuits are powered to the UPS (uninterruptible power supply). In the event of a power failure, essential circuits are powered by a UPS. The recovery occurs in the order of milliseconds and is usually used for a short time to bridge the time until the start of the operation of the units. The UPS operating time is generally in the order of minutes.
3.5. Input 7: Fuel Stocks
The last input necessary to determine a healthcare facility’s readiness for a power outage is fuel stocks. Each unit has a tank, where the amount of fuel is chosen. It is also necessary to consider that the medical facility may have fuel stocks outside the unit. It is essential to consider that the medical facility must meet the conditions for the storage of flammable liquids.
Based on the inputs, the following outputs can be used (
Figure 3).
3.6. Output 1: Object Priority
Based on the selected type of healthcare facility, the building will be assigned priority according to the methodology for categorisation and prioritisation of the buildings necessary for the renewal of electricity supplies after a blackout (see
Table 3).
3.7. Output 2: Preparedness of a Healthcare Facility
The calculation of the readiness of a healthcare facility to solve a large-scale power outage can be determined on the basis of the following relationship:
where:
Pr—preparedness of healthcare facility;
Rt—real time for backup power supply (h);
Pt—required time for backup power supply (h);
Di—determinant of Pr;
The healthcare facility is prepared for a power outage if
where:
Pr—preparedness of the healthcare facility.
The healthcare facility is not prepared for a power outage if
where:
Pr—preparedness of the healthcare facility.
The overall calculation of the readiness of the healthcare facility is based on the time that the healthcare facility can cover in the event of a power failure. For this calculation, it is necessary to calculate the capacities of the aggregates (total rated power) and fuel stocks.
where:
Rt—real time (h);
Di—determinant of Rt;
CA—aggregate capacity (kW);
FS—fuel stocks (l);
FS is expressed by the sum of the capacities of all fuel tanks and the total number of aggregates.
where:
FS—fuel stocks (l).
where:
Rt—real time (h);
Di—determinant of Rt;
CA—aggregate capacity (kW);
FS—fuel stocks (l).
where:
Rt—real time (h);
CA—aggregate capacity (kW);
FS—fuel stocks (l).
3.8. Output 3: Missing Aggregates Capacity
As mentioned in Output 1, to determine the readiness of healthcare facilities, it is necessary to determine whether the aggregates’ capacity is sufficient. If the capacity of the aggregates is not sufficient, it is essential to determine the missing capacities. The missing capacity of the aggregates can be determined based on the following relationship:
where:
MCA—missing aggregate capacity (kW);
RC—real aggregate capacity (kW);
PC—required aggregate capacity (kW);
CHKi—determinant of M
CA.
where:
RC—real aggregate capacity (kW);
PC—required aggregate capacity (kW).
3.9. Output 4: Missing Fuel Stocks
If the healthcare facility has sufficient aggregates’ capacity, it is necessary to determine whether it also has enough fuel stocks. If fuel stocks are insufficient, missing stocks must be identified. Missing fuel stocks can be determined based on the following formula:
where:
MF—missing fuel stocks (l);
Rf—real fuel stocks (l);
Pf—required fuel stocks (l);
MFi—determinant of MF.
where:
Rf—real fuel stocks (l);
Pf—required fuel stocks (l).
All units used in this assessment are not reported in basic units but in the units that are realistic for the assessment. (Therefore, the time is not given in seconds, but hours.)







{kind=link}
{kind=link}
{kind=link}
{kind=link}