
Trait Mindfulness and Physical Health among Chinese Middle-Older Adults: The Mediating Role of Mental Health

Abstract
:1. Introduction
1.1. Trait Mindfulness and Physical Health of Middle-Older Adults
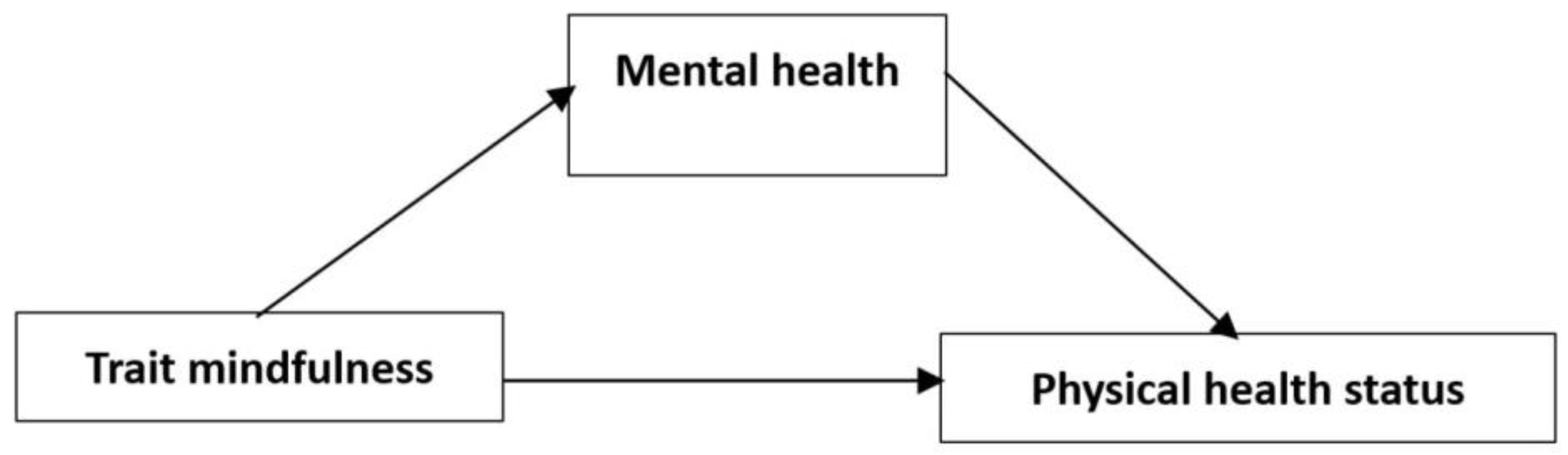
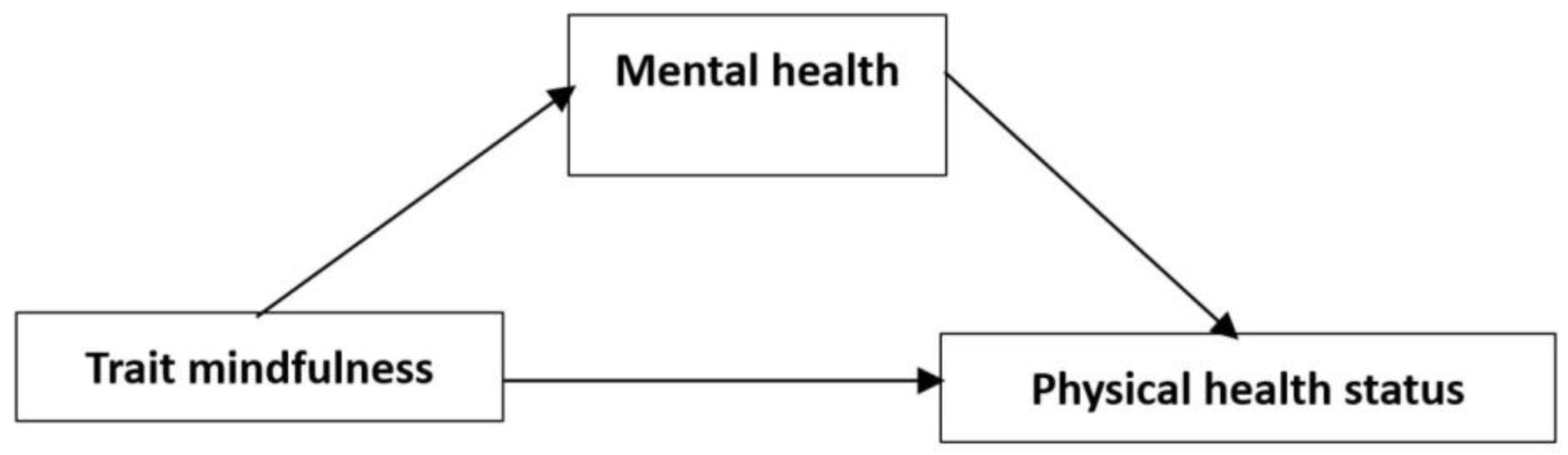
1.2. The Mediating Effects of Mental Health
1.3. The Present Study
2. Method
2.1. Participants and Setting
2.2. Measurements
2.2.1. Trait Mindfulness
2.2.2. Physical Health Status
Self-Rated Physical Health Status
Subjective Sleep Quality
2.2.3. Mental Health
2.3. Data Analysis
3. Results
3.1. Descriptive Statistics and Correlation
3.2. The Effects of Trait Mindfulness on the Physical Health of Middle-Older Adults
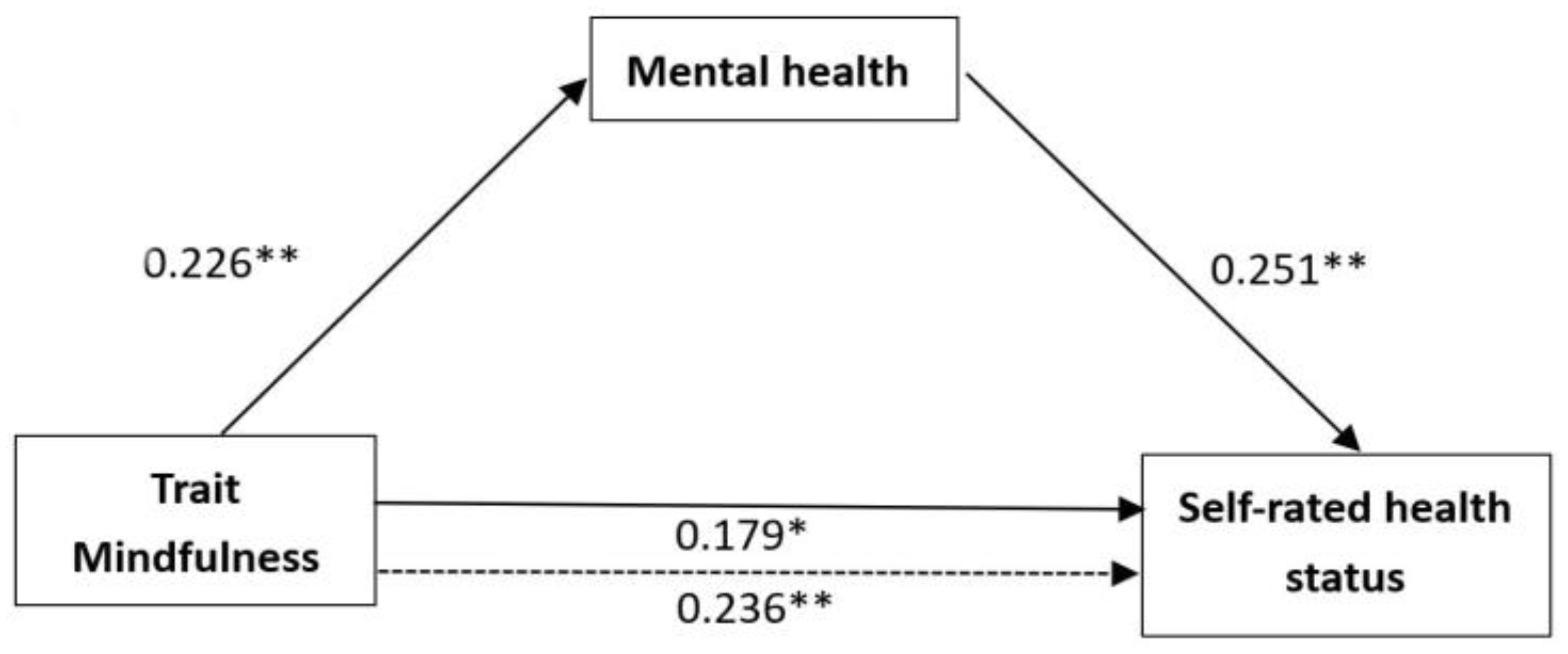
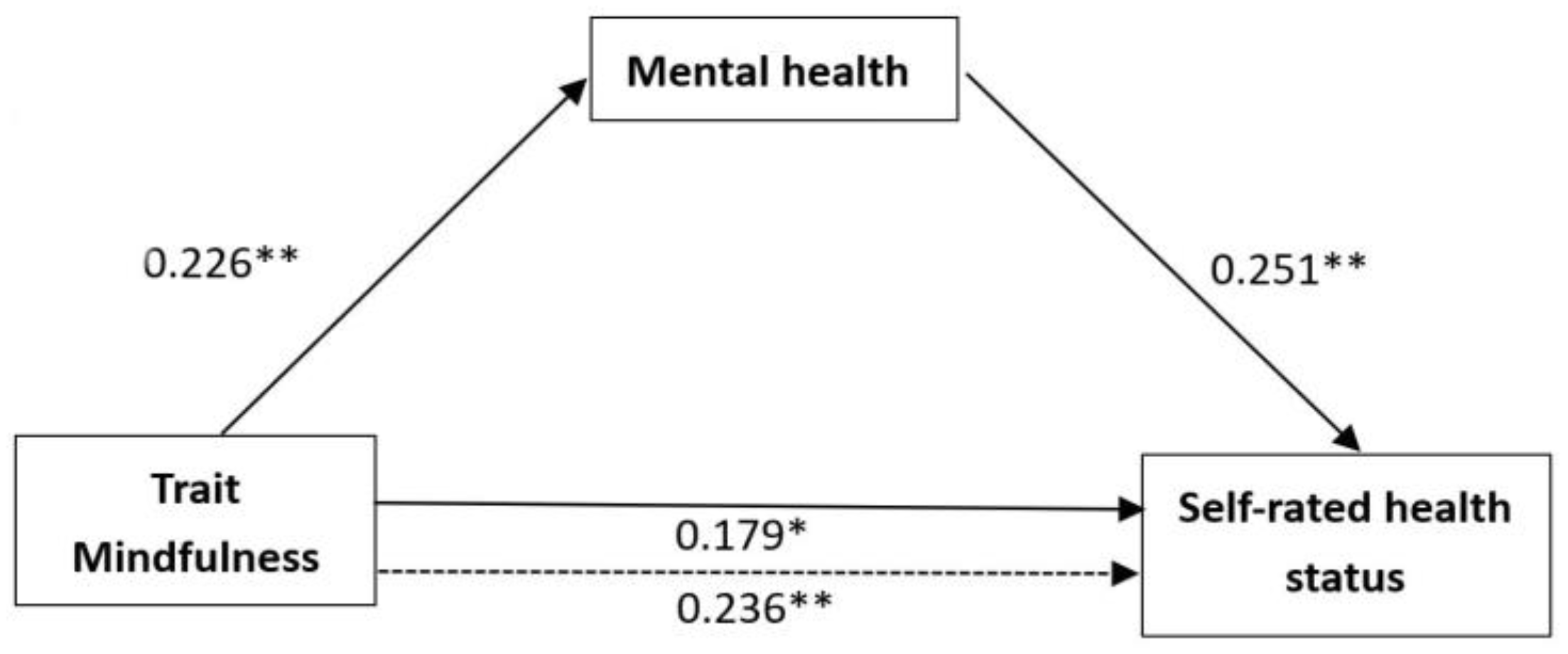
3.3. The Mediating Effects of Mental Health on Physical Health
3.3.1. The Mediating Effects of Mental Health on Self-Rated Health Status
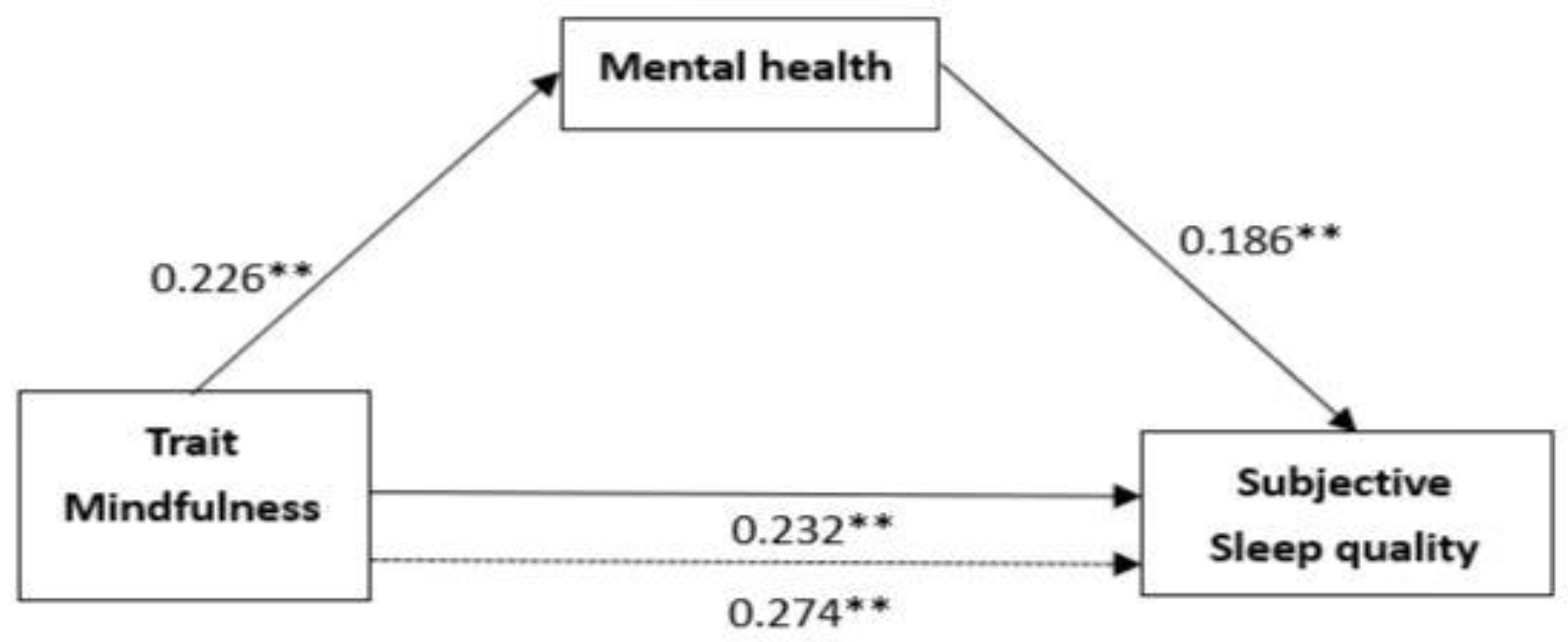
3.3.2. The Mediating Effects of Mental Health on Subjective Sleep Quality
4. Discussion
4.1. Trait Mindfulness Levels and Physical Health
4.2. Mediating Effects of Mental Health
4.3. Limitation and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations-Population Division. 2019 Revision. Available online: https://ourworldindata.org/grapher/historic-and-un-pop-projections-by-age?country=~CHN (accessed on 21 August 2022).
- Mahlo, L.; Windsor, T. Feasibility and Acceptability of App-Based Mindfulness-Meditation Training for Older Adults. Innov. Aging 2020, 4 (Suppl. S1), 411. [Google Scholar] [CrossRef]
- Liu, S.S.; Zhang, L.W.; Lu, Q.C.; Liu, H.L. Investigation on the status quo of multiple chronic diseases and health loss factors among middle-aged and elderly people in China: Based on CHARLS 2018 data. J. Pract. Med. 2021, 37, 518–524. [Google Scholar]
- Luo, L.; Luo, S.; Zhang, J.; Li, W.; Hu, S.J.; An, H.Q.; Dong, Y.; Liu, X.M. Research on the mental health status of different types of elderly in urban communities based on correspondence analysis. China Health Stat. 2018, 2, 209–211. [Google Scholar]
- Kabat-Zinn, J. Catalyzing movement towards a more contemplative/sacred-appreciating/non-dualistic society. In Proceedings of the Contemplative Mind in Society meeting of the Working Group, Pocantico, NY, USA, 29 September–2 October 1994. [Google Scholar]
- Kabat-Zinn, J. Full Catastrophe Living, Revised Edition: How to Cope with Stress, Pain, and Illness Using Mindfulness Meditation; Piatkus: London, UK, 2013; ISBN 978-0749958411. [Google Scholar]
- Kabat-Zinn, J. Mindfulness-based interventions in context: Past, present, and future. Clin. Psychol. Sci. Pract. 2003, 10, 144–156. [Google Scholar] [CrossRef]
- Kiken, L.G.; Garland, E.L.; Bluth, K.; Palsson, O.S.; Gaylord, S.A. From a state to a trait: Trajectories of state mindfulness in meditation during intervention predict changes in trait mindfulness. Personal. Individ. Differ. 2015, 81, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Brown, K.W.; Cordon, S. Toward a phenomenology of mindfulness: Subjective experience and emotional correlates. In Clinical Handbook of Mindfulness; Springer: New York, NY, USA, 2009; pp. 59–81. [Google Scholar]
- Lyvers, M.; Makin, C.; Toms, E.; Thorberg, F.A.; Samios, C. Trait mindfulness in relation to emotional self-regulation and executive function. Mindfulness 2014, 5, 619–625. [Google Scholar] [CrossRef]
- Tomlinson, E.R.; Yousaf, O.; Vittersø, A.D.; Jones, L. Dispositional mindfulness and psychological health: A systematic review. Mindfulness 2018, 9, 23–43. [Google Scholar] [CrossRef] [Green Version]
- Keng, S.L.; Smoski, M.J.; Robins, C.J. Effects of mindfulness on psychological health: A review of empirical studies. Clin. Psychol. Rev. 2011, 31, 1041–1056. [Google Scholar] [CrossRef] [Green Version]
- Lenze, E.J.; Hickman, S.; Hershey, T.; Wendleton, L.; Ly, K.; Dixon, D.; Doré, P.; Wetherell, J.L. Mindfulness-based stress reduction for older adults with worry symptoms and cooccurring cognitive dysfunction. Int. J. Geriatr. Psychiatry 2014, 29, 991–1000. [Google Scholar] [CrossRef] [Green Version]
- Mahlo, L.; Windsor, T.D. Older and more mindful? Age differences in mindfulness components and well-being. Aging Ment. Health 2021, 25, 1320–1331. [Google Scholar] [CrossRef] [Green Version]
- Friese, M.; Hofmann, W. State mindfulness, self-regulation, and emotional experience in everyday life. Motiv. Sci. 2016, 2, 1. [Google Scholar] [CrossRef]
- Creswell, J.D.; Irwin, M.R.; Burklund, L.J.; Lieberman, M.D.; Arevalo, J.M.; Ma, J.; Breen, E.C.; Cole, S.W. Mindfulness-based stress reduction training reduces loneliness and pro-inflammatory gene expression in older adults: A small randomized controlled trial. Brain Behav. Immun. 2012, 26, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, S.L.; Carlson, L.E.; Astin, J.A.; Freedman, B. Mechanisms of mindfulness. J. Clin. Psychol. 2006, 62, 373–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fiocco, A.J.; Mallya, S. The importance of cultivating mindfulness for cognitive and emotional well-being in late life. J. Evid.-Based Complement. Altern. Med. 2015, 20, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Boekel, W.; Hsieh, S. Cross-sectional white matter microstructure differences in age and trait mindfulness. PLoS ONE 2018, 13, e0205718. [Google Scholar] [CrossRef]
- Farb, N.A.; Anderson, A.K.; Irving, J.A.; Segal, Z.V. Mindfulness interventions and emotion regulation. In Handbook of Emotion Regulation; Gross, J.J., Ed.; The Guilford Press: New York, NY, USA, 2014; pp. 548–567. ISBN 978-1-4625-0350-6. [Google Scholar]
- Shaurya Prakash, R.; De Leon, A.A.; Klatt, M.; Malarkey, W.; Patterson, B. Mindfulness disposition and default-mode network connectivity in older adults. Soc. Cogn. Affect. Neurosci. 2013, 8, 112–117. [Google Scholar] [CrossRef]
- Nilsson, H.; Bülow, P.H.; Kazemi, A. Mindful sustainable aging: Advancing a comprehensive approach to the challenges and opportunities of old age. Eur. J. Psychol. 2015, 11, 494. [Google Scholar] [CrossRef]
- Fiocco, A.J.; Meisner, B.A. Mindful aging: The association between trait mindfulness and expectations regarding aging among middle-aged and older adults. Aging Ment. Health 2020, 24, 591–595. [Google Scholar] [CrossRef]
- Nilsson, H. The four-dimensional model of mindful sustainable aging: A holistic alternative. J. Relig. Spiritual. Aging 2022, 1–25. [Google Scholar] [CrossRef]
- Koipysheva, E.A.; Lebedinsky, V.Y.; Koipysheva, M.A. Physical health (definition, semantic content, study prospects). Eur. Proc. Soc. Behav. Sci. 2018, 601–605. [Google Scholar] [CrossRef]
- Orme-Johnson, D.W.; Farrow, J.T. Scientific Research on the Transcendental Meditation Program: Collected Papers; Maharishi European Research University Press: Bern, Switzerland, 1977; Volume I. [Google Scholar]
- Langer, E.J. Minding matters: The consequences of mindlessness–mindfulness. In Advances in Experimental Social Psychology; Academic Press: Cambridge, MA, USA, 1989; Volume 22, pp. 137–173. [Google Scholar]
- Jordan, C.H.; Wang, W.; Donatoni, L.; Meier, B.P. Mindful eating: Trait and state mindfulness predict healthier eating behavior. Personal. Individ. Differ. 2014, 68, 107–111. [Google Scholar] [CrossRef] [Green Version]
- Murphy, M.J.; Mermelstein, L.C.; Edwards, K.M.; Gidycz, C.A. The benefits of dispositional mindfulness in physical health: A longitudinal study of female college students. J. Am. Coll. Health 2012, 60, 341–348. [Google Scholar] [CrossRef] [PubMed]
- Idler, E.L.; Benyamini, Y. Self-rated health and mortality: A review of twenty-seven community studies. J. Health Soc. Behav. 1997, 38, 21–37. [Google Scholar] [CrossRef] [Green Version]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Bosworth, H.B.; Siegler, I.C.; Brummett, B.H.; Barefoot, J.C.; Williams, R.B.; Vitaliano, P.P.; Channing, N.C.; Lytle, B.L.; Mark, D.B. The relationship between self-rated health and health status among coronary artery patients. J. Aging Health 1999, 11, 565–584. [Google Scholar] [CrossRef]
- Wu, S.; Wang, R.; Zhao, Y.; Ma, X.; Wu, M.; Yan, X.; He, J. The relationship between self-rated health and objective health status: A population-based study. BMC Public Health 2013, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Greeson, J.M.; Chin, G.R. Mindfulness and physical disease: A concise review. Curr. Opin. Psychol. 2019, 28, 204–210. [Google Scholar] [CrossRef]
- Camilleri, G.M.; Méjean, C.; Bellisle, F.; Andreeva, V.A.; Sautron, V.; Hercberg, S.; Péneau, S. Cross-cultural validity of the Intuitive Eating Scale-2. Psychometric evaluation in a sample of the general French population. Appetite 2015, 84, 34–42. [Google Scholar] [CrossRef]
- Nebes, R.D.; Buysse, D.J.; Halligan, E.M.; Houck, P.R.; Monk, T.H. Self-reported sleep quality predicts poor cognitive performance in healthy older adults. J. Gerontol. Ser. B 2009, 64, 180–187. [Google Scholar] [CrossRef]
- Durmer, J.S.; Dinges, D.F. Neurocognitive consequences of sleep deprivation. In Seminars in Neurology; Thieme Medical Publishers: New York, NY, USA, 2005; Volume 25, pp. 117–129. [Google Scholar]
- Urponen, H.; Partinen, M.; Vuori, I.; Hasan, J. Sleep quality and health: Description of the sleep quality index. In Sleep and Health Risk; Springer: Berlin/Heidelberg, Germany, 1991; pp. 555–558. [Google Scholar]
- Allen, T.D.; Kiburz, K.M. Trait mindfulness and work–family balance among working parents: The mediating effects of vitality and sleep quality. J. Vocat. Behav. 2012, 80, 372–379. [Google Scholar] [CrossRef]
- Brown, K.W.; Ryan, R.M. The benefits of being present: Mindfulness and its role in psychological well-being. J. Personal. Soc. Psychol. 2003, 84, 822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, E.S.; Tkatch, R.; Martin, D.; MacLeod, S.; Sandy, L.; Yeh, C. Resilient aging: Psychological well-being and social well-being as targets for the promotion of healthy aging. Gerontol. Geriatr. Med. 2021, 7, 23337214211002951. [Google Scholar] [CrossRef] [PubMed]
- Diener, E.; Suh, E.M.; Lucas, R.E.; Smith, H.L. Subjective well-being: Three decades of progress. Psychol. Bull. 1999, 125, 276–302. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Barnes, L.L.; Bennett, D.A. Effect of a purpose in life on risk of incident Alzheimer disease and mild cognitive impairment in community-dwelling older persons. Arch. Gen. Psychiatry 2010, 67, 304–310. [Google Scholar] [CrossRef] [Green Version]
- Gawronski, K.A.; Kim, E.S.; Langa, K.M.; Kubzansky, L.D. Dispositional optimism and incidence of cognitive impairment in older adults. Psychosom. Med. 2016, 78, 819. [Google Scholar] [CrossRef] [Green Version]
- Oh, J.; Chopik, W.J.; Kim, E.S. The association between actor/partner optimism and cognitive functioning among older couples. J. Personal. 2020, 88, 822–832. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Schaeffer, J.A.; Kraemer, S.; Wicker, E.; Yeh, C.S. The additive impact of multiple psychosocial protective factors on selected health outcomes among older adults. Geriatr. Nurs. 2021, 42, 502–508. [Google Scholar] [CrossRef]
- Anicha, C.L.; Ode, S.; Moeller, S.K.; Robinson, M.D. Toward a cognitive view of trait mindfulness: Distinct cognitive skills predict its observing and nonreactivity facets. J. Personal. 2012, 80, 255–285. [Google Scholar] [CrossRef]
- Yıldız Akyol, E.; Demir, A. Burnout as a predictor of senior students’ mindfulness. J. Hum. Behav. Soc. Environ. 2019, 29, 256–265. [Google Scholar] [CrossRef]
- Glomb, T.M.; Duffy, M.K.; Bono, J.E.; Yang, T. Mindfulness at work. In Research in Personnel and Human Resources Management; Emerald Group Publishing Limited: Bingley, UK, 2011; pp. 115–157. [Google Scholar]
- Carpenter, J.K.; Conroy, K.; Gomez, A.F.; Curren, L.C.; Hofmann, S.G. The relationship between trait mindfulness and affective symptoms: A meta-analysis of the Five Facet Mindfulness Questionnaire (FFMQ). Clin. Psychol. Rev. 2019, 74, 101785. [Google Scholar] [CrossRef] [PubMed]
- Miners, R. Collected and Connected: Mindfulness and the Early Adolescent. Ph.D. Thesis, Concordia University, Montreal, QC, Canada, 2007. [Google Scholar]
- Barnes, J.W.; Radebaugh, J.; Brown, R.H.; Wall, S.; Soderblom, L.; Lunine, J.; Burr, D.; Sotin, C.; Le Mouélic, S.; Rodriguez, S.; et al. Near-infrared spectral mapping of Titan’s mountains and channels. J. Geophys. Res. Planets 2007, 112, E11. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.F.; Chi, X.L.; Zhang, J.T.; Duan, W.J.; Wen, Z.K. Reliability and validity of the Children and Adolescent Mindfulness Scale (CAMM) in Chinese adolescents. New Psychol. 2019, 3, 250–256. [Google Scholar]
- Vingilis, E.; Wade, T.J.; Adlaf, E. What factors predict student self-rated physical health? J. Adolesc. 1998, 21, 83–97. [Google Scholar] [CrossRef]
- Hicks, R.A.; Lucero-Gorman, K.; Bautista, J.; Hicks, G.J. Ethnicity, sleep duration, and sleep satisfaction. Percept. Mot. Ski. 1999, 88, 234–235. [Google Scholar] [CrossRef]
- The China Health and Retirement Longitudinal Study Wave 4 (2018) Questionnaire. Available online: https://charls.charlsdata.com/pages/Data/2018-charls-wave4/zh-cn.html (accessed on 21 August 2022).
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to mediation, moderation, and conditional process analysis: A regression–based approach. J. Educ. Meas. 2013, 51, 335–337. [Google Scholar]
- Chen, L.; Yan, Z.; Tang, W.; Yang, F.; Xie, X.; He, J. Mobile phone addiction levels and negative emotions among Chinese young adults: The mediating role of interpersonal problems. Comput. Hum. Behav. 2016, 55, 856–866. [Google Scholar] [CrossRef]
- Bogusch, L.M.; Fekete, E.M.; Skinta, M.D. Anxiety and depressive symptoms as mediators of trait mindfulness and sleep quality in emerging adults. Mindfulness 2016, 7, 962–970. [Google Scholar] [CrossRef]
- Roberts, K.C.; Danoff-Burg, S. Mindfulness and health behaviors: Is paying attention good for you? J. Am. Coll. Health 2010, 59, 165–173. [Google Scholar] [CrossRef]
- Chen, S.; Liu, J.; Chen, Y. Analysis of the behavioral characteristics and living conditions of the elderly in Shenzhen’s public rental housing under the background of intergenerational support. Chin. J. Archit. 2022, 25 (Suppl. S1), 51–57. [Google Scholar]
- Fischer, D.G.; Fick, C. Measuring social desirability: Short forms of the Marlowe-Crowne social desirability scale. Educ. Psychol. Meas. 1993, 53, 417–424. [Google Scholar] [CrossRef]
- Gallegos, A.M.; Hoerger, M.; Talbot, N.L.; Krasner, M.S.; Knight, J.M.; Moynihan, J.A.; Duberstein, P.R. Toward identifying the effects of the specific components of mindfulness-based stress reduction on biologic and emotional outcomes among older adults. J. Altern. Complement. Med. 2013, 19, 787–792. [Google Scholar] [CrossRef] [PubMed]
- Salmon, P.G.; Santorelli, S.F.; Sephton, S.E.; Kabat-Zinn, J. Intervention elements promoting adherence to mindfulness-based stress reduction (MDSR) programs in a clinical behavioral medicine setting. In The Handbook of Health Behavior Change; Shumaker, S.A., Ockene, J.K., Riekert, K.A., Eds.; Springer Publishing Company: New York, NY, USA, 2009; pp. 271–286. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Variable | M | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Trait mindfulness | 3.631 | 0.598 | - | ||||||
| 2. Mental health | 3.881 | 0.645 | 0.226 ** | - | |||||
| 3. Self-rated physical health | 3.707 | 0.973 | 0.236 ** | 0.292 *** | - | ||||
| 4. Subjective sleep quality | 3.333 | 0.946 | 0.274 *** | 0.239 ** | 0.341 *** | - | |||
| 5. Gender | 1.710 | 0.456 | −0.022 | 0.193 ** | 0.252 ** | −0.058 | - | ||
| 6. Age | 62.610 | 6.280 | 0.027 | −0.078 | −0.165 * | 0.017 | −0.281 ** | - | |
| 7. Education | 4.300 | 1.755 | 0.080 | 0.058 | 0.043 | 0.030 | −0.129 | −0.033 | - |
| Self-Rated Physical Health | β a | R2 | Adjust R2 | F | ΔR2 | ΔF | |
|---|---|---|---|---|---|---|---|
| B (SE) | |||||||
| Analysis One: Trait mindfulness to Self-rated physical health (path c) | 0.384 (0.116) | 0.236 ** | 0.056 | 0.05 | 10.943 ** | 0.056 | 10.943 ** |
| Analysis Two: Trait mindfulness to Mental health (path a) | 0.244 (0.077) | 0.226 ** | 0.051 | 0.046 | 9.975 ** | 0.051 | 9.975 ** |
| Analysis Three: Step 1: Mental health to Self-rated physical health (path b) | 0.379 (0.107) | 0.251 *** | 0.085 | 0.08 | 17.304 *** | 0.085 | 17.304 *** |
| Step 2: Trait mindfulness to Self-rated physical health (path c) | 0.291 (0.115) | 0.179 * | 0.116 | 0.106 | 12.082 *** | 0.060 | 12.592 ** |
| Subjective Sleep Quality | β a | R2 | Adjust R2 | F | ΔR2 | ΔF | |
|---|---|---|---|---|---|---|---|
| B (SE) | |||||||
| Analysis One: Trait mindfulness to Subjective sleep quality (path c) | 0.434 (0.112) | 0.274 *** | 0.075 | 0.07 | 15.125 *** | 0.075 | 15.125 *** |
| Analysis Two: Trait mindfulness to Mental health (path a) | 0.244 (0.077) | 0.226 ** | 0.051 | 0.046 | 9.975 ** | 0.051 | 9.975 ** |
| Analysis Three: Step 1: Mental health to Subjective sleep quality (path b) | 0.273 (0.104) | 0.186 ** | 0.057 | 0.052 | 11.251 ** | 0.057 | 11.251 ** |
| Step2: Trait mindfulness to Subjective sleep quality (path c) | 0.367 (0.113) | 0.232 ** | 0.108 | 0.099 | 11.222 *** | 0.033 | 6.844 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lei, Y.; Liu, J.; Wang, X.; Deng, Z.; Gao, Q. Trait Mindfulness and Physical Health among Chinese Middle-Older Adults: The Mediating Role of Mental Health. Int. J. Environ. Res. Public Health 2022, 19, 16088. https://doi.org/10.3390/ijerph192316088
Lei Y, Liu J, Wang X, Deng Z, Gao Q. Trait Mindfulness and Physical Health among Chinese Middle-Older Adults: The Mediating Role of Mental Health. International Journal of Environmental Research and Public Health. 2022; 19(23):16088. https://doi.org/10.3390/ijerph192316088
Chicago/Turabian StyleLei, Yuruo, Jiawei Liu, Xinyu Wang, Zhiqi Deng, and Qiufeng Gao. 2022. "Trait Mindfulness and Physical Health among Chinese Middle-Older Adults: The Mediating Role of Mental Health" International Journal of Environmental Research and Public Health 19, no. 23: 16088. https://doi.org/10.3390/ijerph192316088
APA StyleLei, Y., Liu, J., Wang, X., Deng, Z., & Gao, Q. (2022). Trait Mindfulness and Physical Health among Chinese Middle-Older Adults: The Mediating Role of Mental Health. International Journal of Environmental Research and Public Health, 19(23), 16088. https://doi.org/10.3390/ijerph192316088