Persistent Upgaze Restriction After Orbital Floor Fracture Repair
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
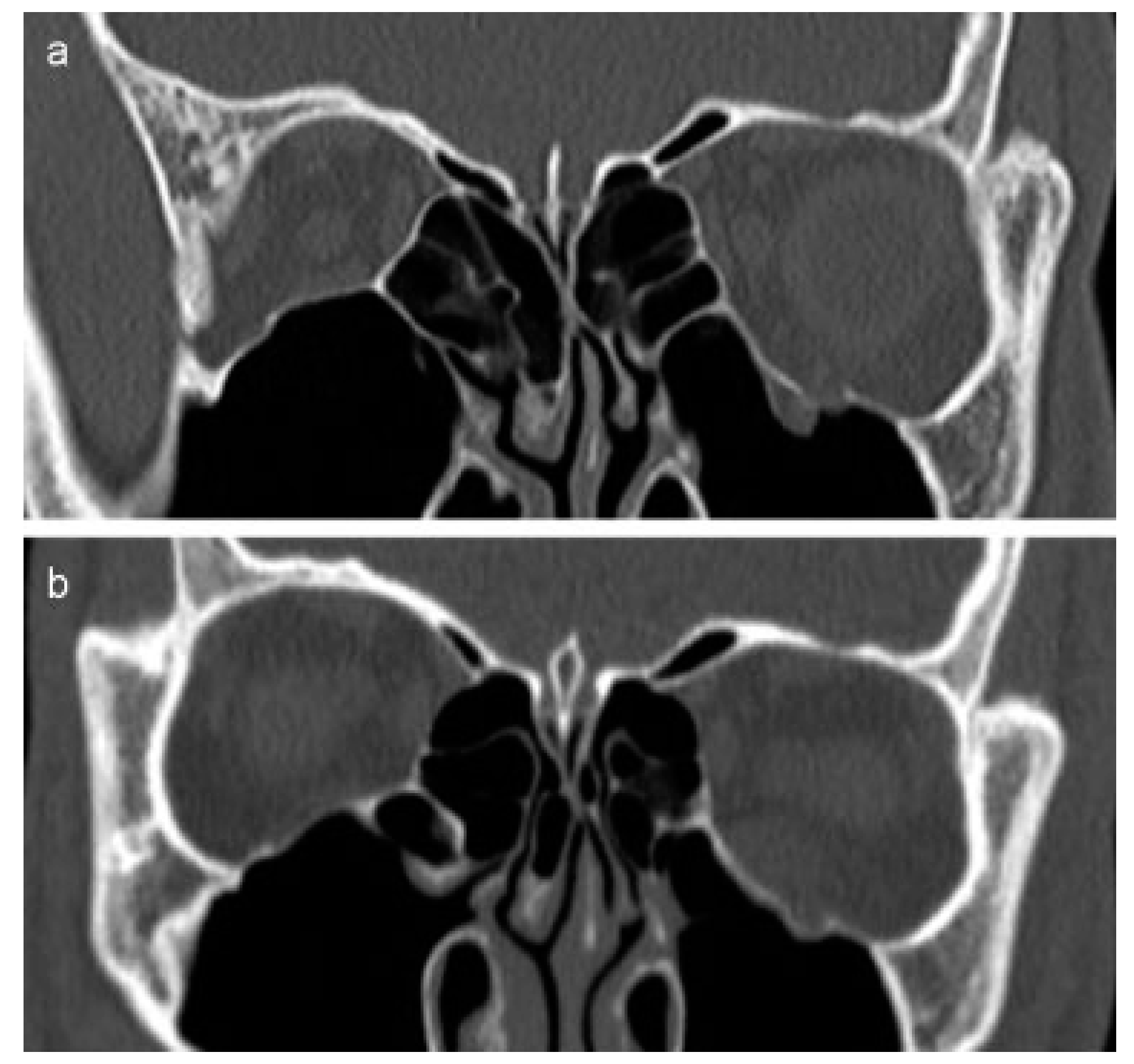
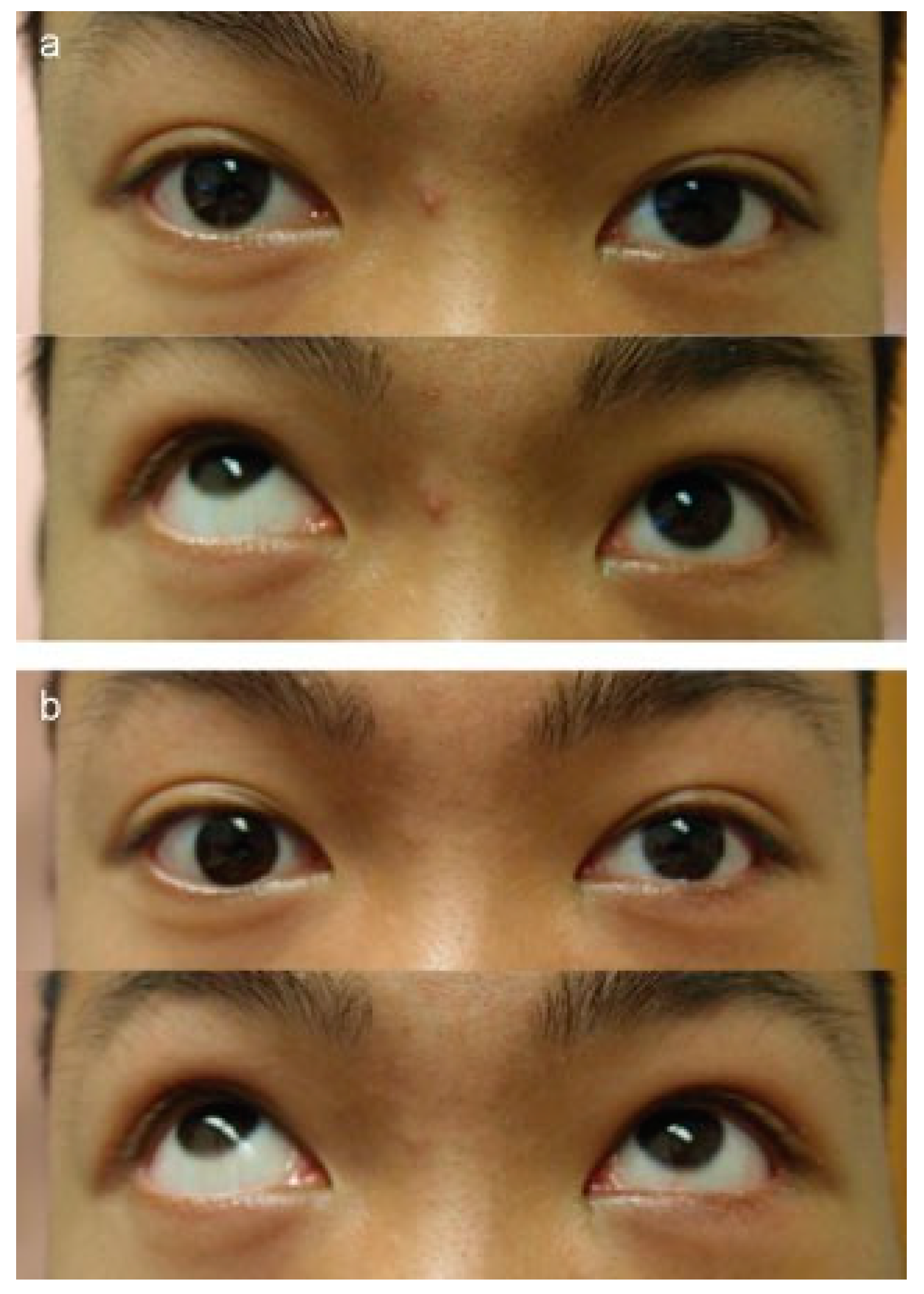
:Case 1
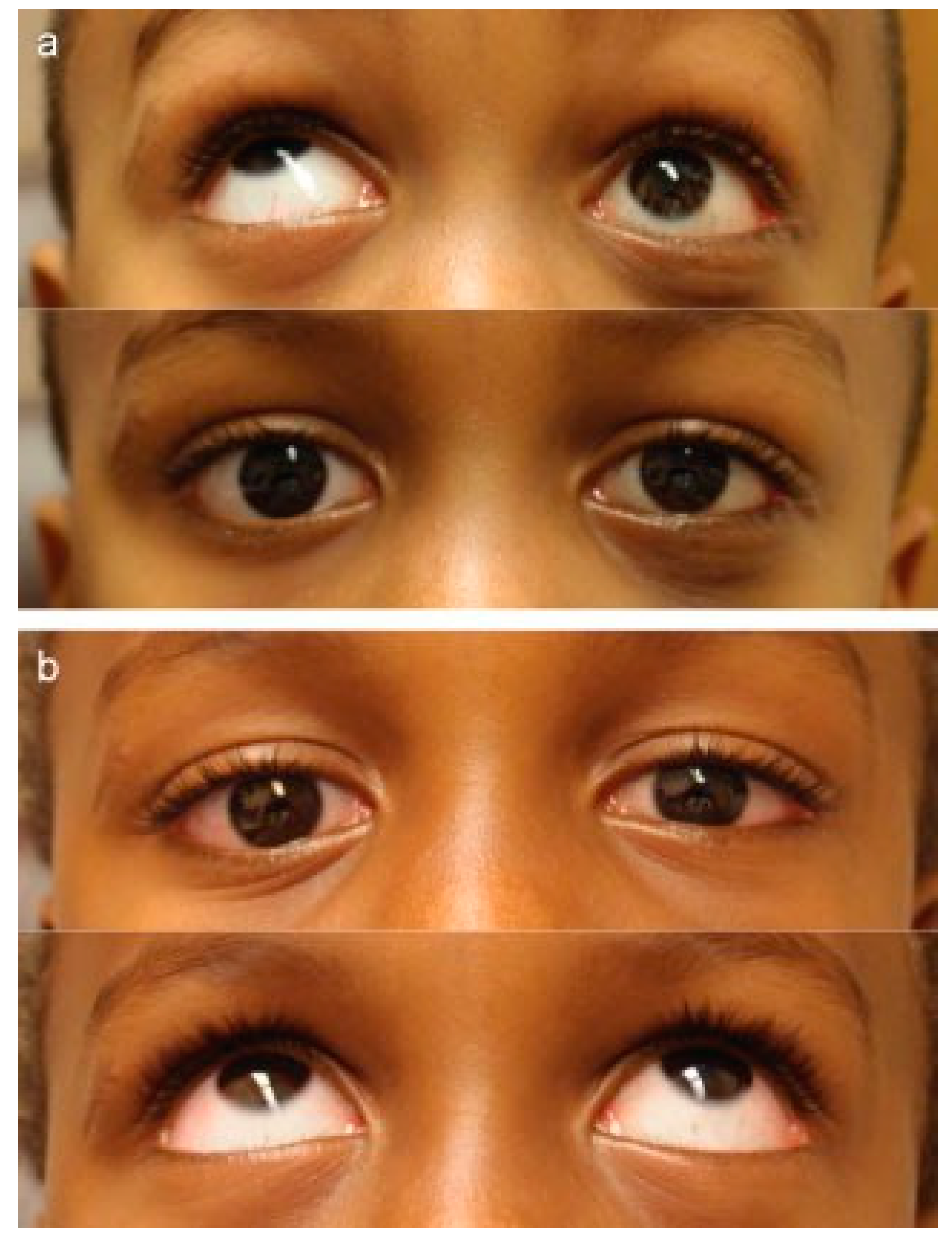
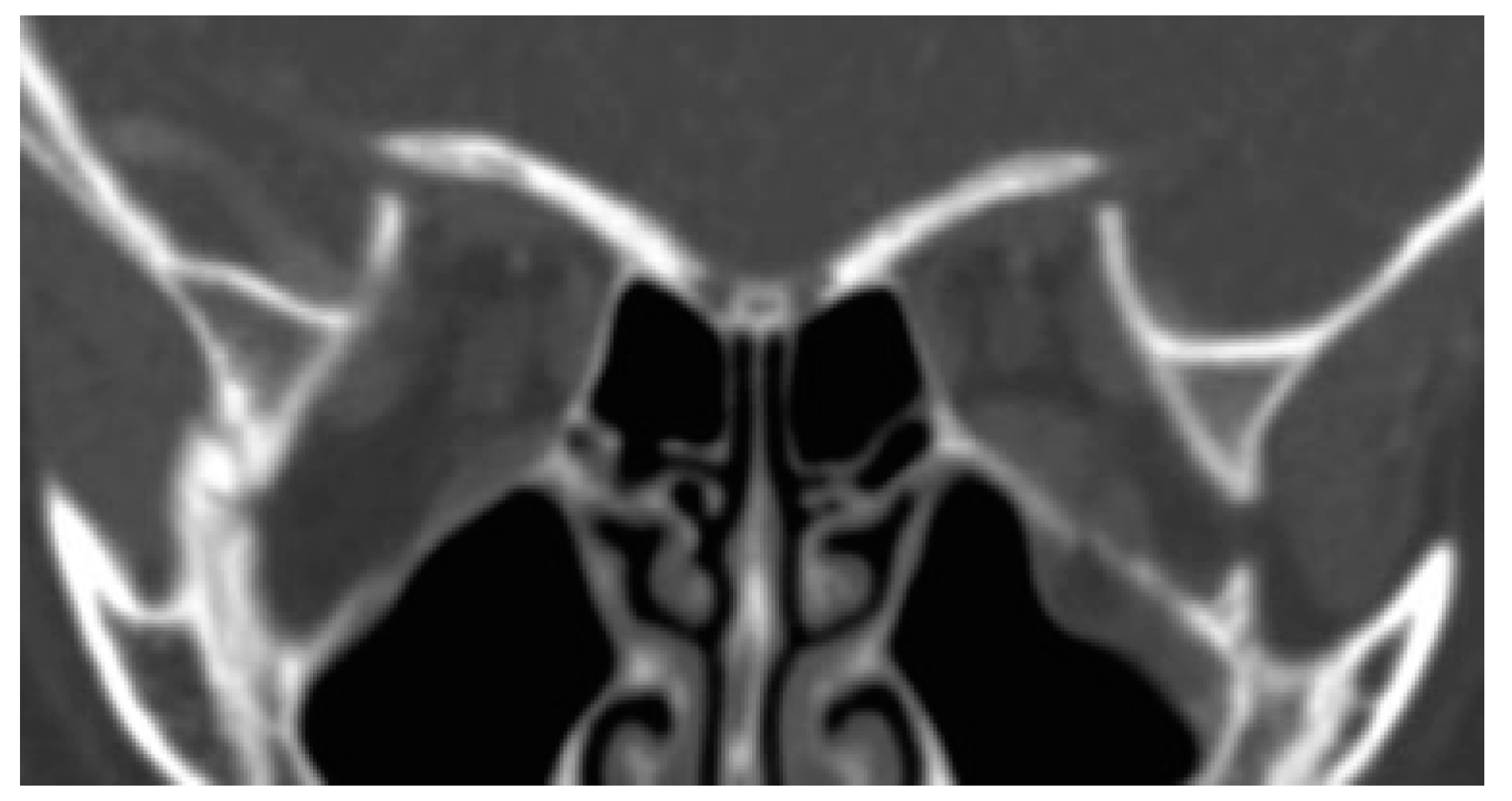
Case 2
Comment
References
- Biesman, B.S.; Hornblass, A.; Lisman, R.; Kazlas, M. Diplopia after surgical repair of orbital floor fractures. Ophthal Plast Reconstr Surg 1996, 12, 9–16; discussion 17. [Google Scholar] [CrossRef] [PubMed]
- Cope, M.R.; Moos, K.F.; Speculand, B. Does diplopia persist after blow- out fractures of the orbital floor in children? Br J Oral Maxillofac Surg 1999, 37, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Gerbino, G.; Roccia, F.; Bianchi, F.A.; Zavattero, E. Surgical management of orbital trapdoor fracture in a pediatric population. J Oral Maxillofac Surg 2010, 68, 1310–1316. [Google Scholar] [CrossRef] [PubMed]
- Gunarajah, D.R.; Samman, N. Biomaterials for repair of orbital floor blowout fractures: A systematic review. J Oral Maxillofac Surg 2013, 71, 550–570. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.A.; Durairaj, V.D. Pediatric orbital floor fractures. J AAPOS 2011, 15, 173–180. [Google Scholar] [PubMed]
- Seiff, S.R.; Good, W.V. Hypertropia and the posterior blowout fracture: Mechanism and management. Ophthalmology 1996, 103, 152–156. [Google Scholar] [CrossRef] [PubMed]
© 2016 by the author. The Author(s) 2016.
Share and Cite
DeParis, S.W.; Grumbine, F.L.; Vagefi, M.R.; Kersten, R.C. Persistent Upgaze Restriction After Orbital Floor Fracture Repair. Craniomaxillofac. Trauma Reconstr. 2016, 9, 268-270. https://doi.org/10.1055/s-0035-1570076
DeParis SW, Grumbine FL, Vagefi MR, Kersten RC. Persistent Upgaze Restriction After Orbital Floor Fracture Repair. Craniomaxillofacial Trauma & Reconstruction. 2016; 9(3):268-270. https://doi.org/10.1055/s-0035-1570076
Chicago/Turabian StyleDeParis, Sarah Willcox, F. Lawson Grumbine, M. Reza Vagefi, and Robert C. Kersten. 2016. "Persistent Upgaze Restriction After Orbital Floor Fracture Repair" Craniomaxillofacial Trauma & Reconstruction 9, no. 3: 268-270. https://doi.org/10.1055/s-0035-1570076
APA StyleDeParis, S. W., Grumbine, F. L., Vagefi, M. R., & Kersten, R. C. (2016). Persistent Upgaze Restriction After Orbital Floor Fracture Repair. Craniomaxillofacial Trauma & Reconstruction, 9(3), 268-270. https://doi.org/10.1055/s-0035-1570076