“Phossy Jaw” and “Bis-Phossy Jaw” of the 19th and the 21st Centuries: The Diuturnity of John Walker and the Friction Match
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
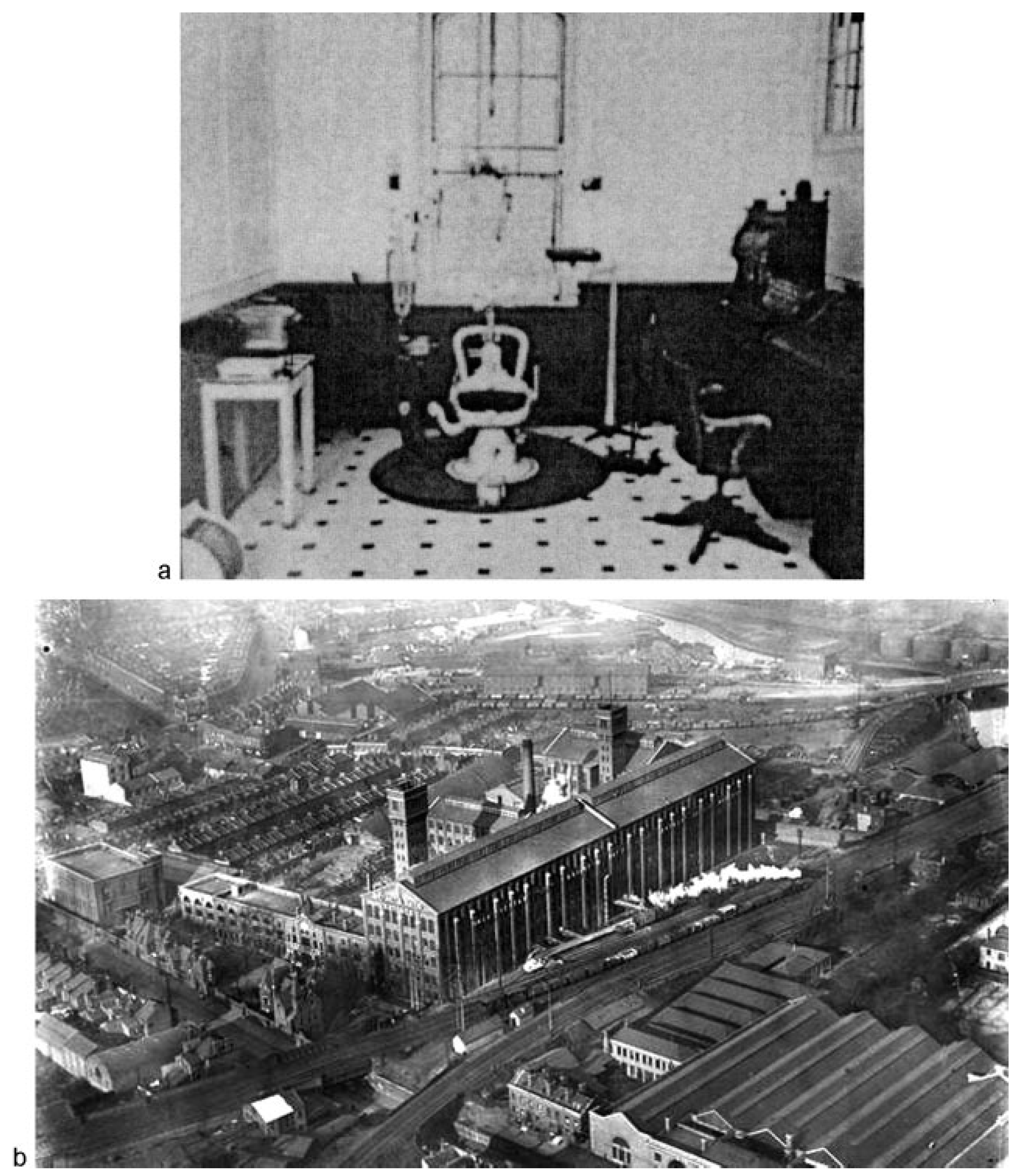
:“Phossy Jaw”: John Walker (1781–1859) and the Friction Match
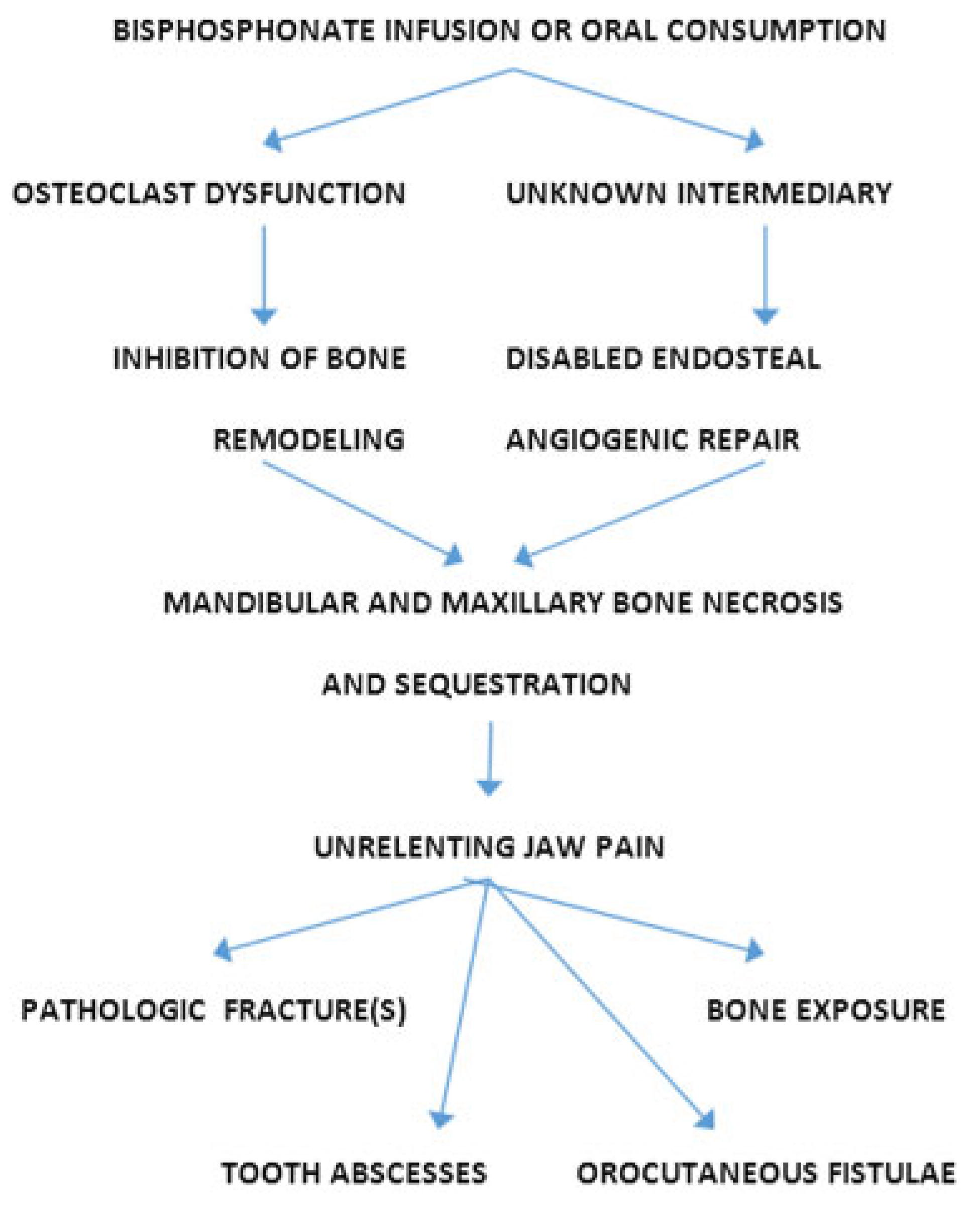
“Bis-Phossy Jaw” (Bisphosphonate-Induced Osteonecrosis): A Modern Equivalent
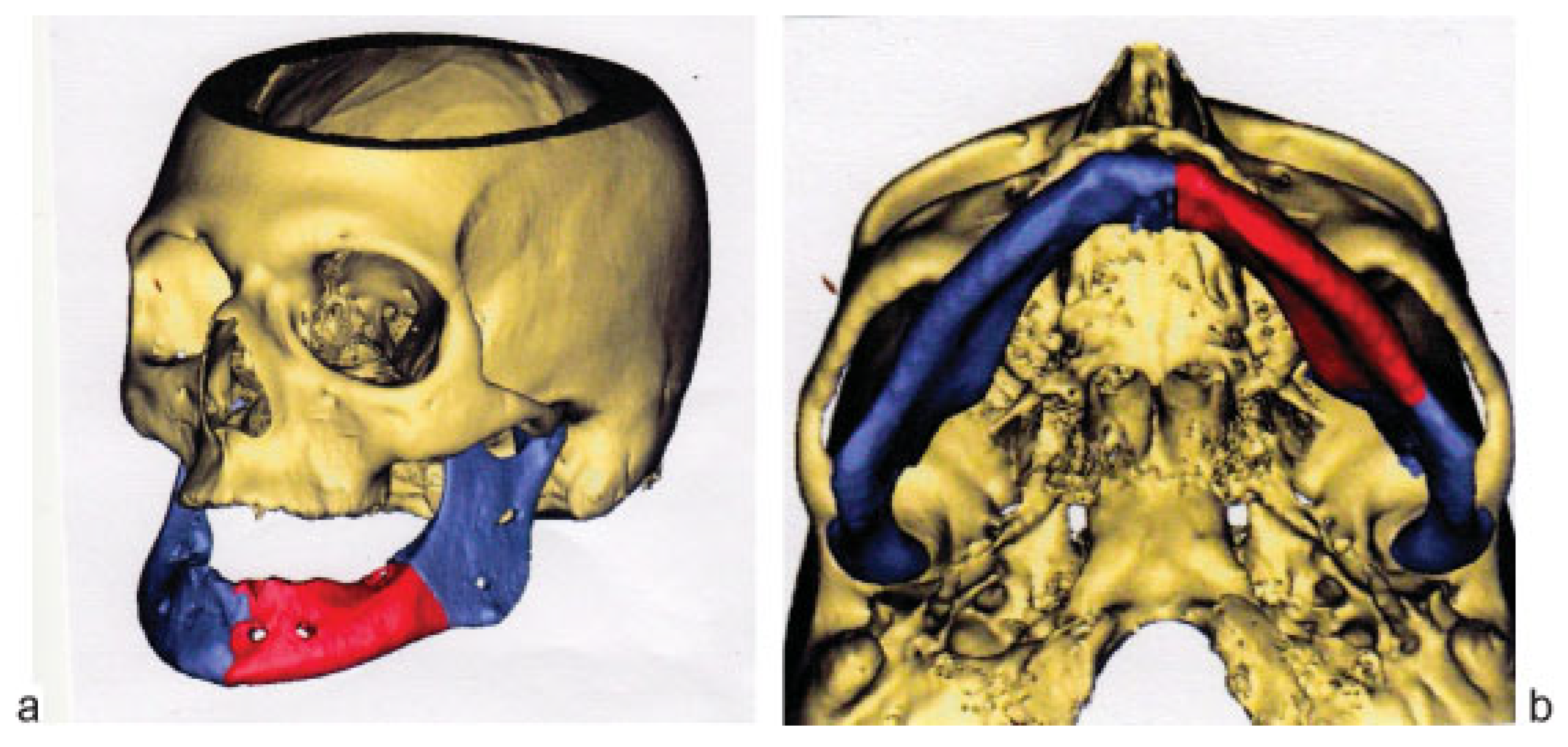
Case Report
Discussion
References
- John Walker. Available online: http://archives.rootsweb.ancestry.com/th/read/GENBRIT/2000-12/0977572827. Available online: http://www.historyofmatches.com/matches-inventors/john-walker/ (accessed on 1 August 2014).
- Stockton-on-Tees. (Photos 19th Century, Courtesy Thisisstockton.org). Available online: https://www.thisisstockton.gov.uk/…/historystocktonpicturesarchive (accessed on 1 August 2014).
- Phossy Jaw. Available online: http://en.wikipedia.org/wiki/Phossy_-jaw (accessed on 1 August 2014).
- Stephen, L.; Lee, S. Dictionary of National Biography; Smith, Elder & Co.: London, UK, 1885. [Google Scholar]
- Brady, A. Wildfire: A Verse Essay; Krupskaya Press: San Francisco, CA, USA, 2010; Available online: http://www.academia.edu/1904531/An-drea_Bradys_Wildfire_Generation_in_Destruction (accessed on 26 November 2014).
- Legge, T.M. Report of cases of phosphorus necrosis. J Industrial Hygiene 1920, 2, 50–52. [Google Scholar]
- Ward, E.F. Phosphorus necrosis in the manufacture of fireworks. J Ind Hyg Toxicol 1928, 10, 314–330. [Google Scholar]
- Heimann, H. Chronic phosphorus poisoning. J Ind Hyg Toxicol 1946, 28, 142–150. [Google Scholar] [PubMed]
- Hughes, J.P.W.; Baron, R.; Buckland, D.H.; et al. Phosphorus necrosis of the jaw: A present-day study. Br J Ind Med 1962, 19, 83–99. [Google Scholar]
- Miles, A.E. Phosphorus necrosis of the jaw: ‘phossy jaw’. Br Dent J 1972, 133, 203–206. [Google Scholar] [CrossRef]
- Toxicological Profile for White Phosphorus. Sciences International, Inc. for the United States Department of Health and Human Services, Agency for Toxic Substances and Disease Registry (ATSDR). 1997. [Google Scholar]
- Fleisch, H. Development of bisphosphonates. Breast Cancer Res 2002, 4, 30–34. [Google Scholar] [CrossRef]
- Bone, H.G.; Hosking, D.; Devogelaer, J.P.; et al. Alendronate Phase III Osteoporosis Treatment Study GroupTen years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med 2004, 350, 1189–1199. [Google Scholar] [CrossRef] [PubMed]
- Estilo, C.L.; Van Poznak, C.H.; Williams, T.; et al. Osteonecrosis of the maxilla and mandible in patients treated with bisphosphonates: A retrospective study. J Clin Oncol 2004, 22, 8088. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Mehrotra, B.; Rosenberg, T.J.; Engroff, S.L. Osteonecrosis of the jaws associated with the use of bisphosphonates: A review of 63 cases. J Oral Maxillofac Surg 2004, 62, 527–534. [Google Scholar] [CrossRef]
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonateinduced exposed bone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, recognition, prevention, and treatment. J Oral Maxillofac Surg 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- Delmas, P.D. The use of bisphosphonates in the treatment of osteoporosis. Curr Opin Rheumatol 2005, 17, 462–466. [Google Scholar] [CrossRef]
- Migliorati, C.A.; Schubert, M.M.; Peterson, D.E.; Seneda, L.M. Bisphosphonate-associated osteonecrosis of mandibular and maxillary bone: An emerging oral complication of supportive cancer therapy. Cancer 2005, 104, 83–93. [Google Scholar] [CrossRef]
- Migliorati, C.A.; Casiglia, J.; Epstein, J.; Jacobsen, P.L.; Siegel, M.A.; Woo, S.B. Managing the care of patients with bisphosphonate-associated osteonecrosis: An American Academy of Oral Medicine position paper. J Am Dent Assoc 2005, 136, 1658–1668. [Google Scholar] [CrossRef] [PubMed]
- Melo, M.D.; Obeid, G. Osteonecrosis of the jaws in patients with a history of receiving bisphosphonate therapy: Strategies for prevention and early recognition. J Am Dent Assoc 2005, 136, 1675–1681. [Google Scholar] [CrossRef] [PubMed]
- Durie, B.G.; Katz, M.; Crowley, J. Osteonecrosis of the jaw and bisphosphonates. N Engl J Med 2005, 353, 99–102, discussion 99–102. [Google Scholar]
- Jimenez-Soriano, Y.; Bagan, J.V. Bisphosphonates, as a new cause of drug-induced jaw osteonecrosis: An update. Med Oral Patol Oral Cir Bucal 2005, 10 (Suppl. 2), E88–E91. [Google Scholar]
- Hellstein, J.W.; Marek, C.L. Bisphosphonate osteochemonecrosis (bisphossy jaw): Is this phossy jaw of the 21st century? J Oral Maxillofac Surg 2005, 63, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.B.; Hellstein, J.W.; Kalmar, J.R. Narrative [corrected] review: Bisphosphonates and osteonecrosis of the jaws. Ann Intern Med 2006, 144, 753–761. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Fantasia, J.; Carlson, E. Bisphosphonate-related osteonecrosis of the jaw: Background and guidelines for diagnosis, staging and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006, 102, 433–441. [Google Scholar] [CrossRef]
- Ruggiero, S.; Gralow, J.; Marx, R.E.; et al. Practical guidelines for the prevention, diagnosis, and treatment of osteonecrosis of the jaw in patients with cancer. J Oncol Pract 2006, 2, 7–14. [Google Scholar] [CrossRef]
- Kademani, D.; Koka, S.; Lacy, M.Q.; Rajkumar, S.V. Primary surgical therapy for osteonecrosis of the jaw secondary to bisphosphonate therapy. Mayo Clin Proc 2006, 81, 1100–1103. [Google Scholar] [CrossRef]
- Lam, D.K.; Sándor, G.K.B.; Holmes, H.I.; Evans, A.W.; Clokie, C.M.L. A review of bisphosphonate-associated osteonecrosis of the jaws and its management. J Can Dent Assoc 2007, 73, 417–422. [Google Scholar] [PubMed]
- Mavrokokki, T.; Cheng, A.; Stein, B.; Goss, A. Nature and frequency of bisphosphonate-associated osteonecrosis of the jaws in Australia. J Oral Maxillofac Surg 2007, 65, 415–423. [Google Scholar] [CrossRef]
- Marx, R.E. Uncovering the cause of “phossy jaw” Circa 1858 to 1906: Oral and maxillofacial surgery closed case files-case closed. J Oral Maxillofac Surg 2008, 66, 2356–2363. [Google Scholar] [CrossRef]
- Khosla, S.; Burr, D.; Cauley, J.; et al. Editorial: Bisphosphonate-associated osteonecrosis of the jaw (ONJ): Report of a task force of the American Society for Bone and Mineral Research. JBMR 2007, 22, 1479–1488. [Google Scholar] [CrossRef] [PubMed]
- Ault, A. Jaw necrosis affects 1 in 1700 on oral bisphosphonates. Internal Medicine News 2008, 41, 23. [Google Scholar] [CrossRef]
- Abu-Id, M.H.; Warnke, P.H.; Gottschalk, J.; et al. “Bis-phossy jaws” high and low risk factors for bisphosphonate-induced osteonecrosis of the jaw. J Craniomaxillofac Surg 2008, 36, 95–103. [Google Scholar] [CrossRef]
- Hoff, A.O.; Toth, B.B.; Altundag, K.; et al. Frequency and risk factors associated with osteonecrosis of the jaw in cancer patients treated with intravenous bisphosphonates. J Bone Miner Res 2008, 23, 826–836. [Google Scholar] [CrossRef]
- Cartsos, V.M.; Zhu, S.; Zavras, A.I. Bisphosphonate use and the risk of adverse jaw outcomes: A medical claims study of 714,217 people. J Am Dent Assoc 2008, 139, 23–30. [Google Scholar] [CrossRef]
- Carlson, E.R.; Basile, J.D. The role of surgical resection in the management of bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg 2009, 67 (Suppl. 5), 85–95. [Google Scholar] [CrossRef]
- AAOMS (American Association of Oral and Maxillofacial Surgeons) Position Paper on Bisphosphonate-Related Osteonecrosis Update. 2009.
- Watters, A.L.; Hansen, H.J.; Williams, T.; et al. Intravenous bisphosphonate-related osteonecrosis of the jaw: Long-term follow-up of 109 patients. Oral Surg Oral Med Oral Pathol Oral Radiol 2013, 115, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Morris, J.H. Biphase connector, external skeletal splint for reduction and fixation of mandibular fractures. Oral Surg Oral Med Oral Pathol 1949, 2, 1382–1398. [Google Scholar] [CrossRef] [PubMed]
- Pollock, R.A.; Schubert, W. The mandible (Part 1, Surgical Anatomy and General Considerations, Chapter 5). In Craniomaxillofacial Buttresses: Anatomy and Operative Repair; Pollock, R.A., Ed.; Thieme Medical Publishers: New York, NY, USA, 2012. [Google Scholar]
- Cryer, M.H. The Internal Anatomy of the Face; Lea & Febiger: Philadelphia, PA, USA, 1916. [Google Scholar]
- Knapp, D.E.; Avery, J.K.; Costich, E.R. A technique for the study of the internal structure of calcified tissues. J Dent Res 1958, 37, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Dempster, W.T.; Enlow, D.H. Osteone organization and the demonstration of vascular canals in the compacta of the human mandible. Anat Rec 1959, 133, 268. [Google Scholar]
- Dempster, W.T.; Enlow, D.H. Patterns of vascular channels in the cortex of the human mandible. Anat Rec 1959, 135, 189–205. [Google Scholar] [CrossRef]
- Cohen, L. Methods of investigating the vascular architecture of the mandible. J Dent Res 1959, 38, 920–931. [Google Scholar] [CrossRef]




© 2015 by the author. The Author(s) 2015.
Share and Cite
Pollock, R.A.; Brown, T.W., Jr.; Rubin, D.M. “Phossy Jaw” and “Bis-Phossy Jaw” of the 19th and the 21st Centuries: The Diuturnity of John Walker and the Friction Match. Craniomaxillofac. Trauma Reconstr. 2015, 8, 262-270. https://doi.org/10.1055/s-0035-1558452
Pollock RA, Brown TW Jr., Rubin DM. “Phossy Jaw” and “Bis-Phossy Jaw” of the 19th and the 21st Centuries: The Diuturnity of John Walker and the Friction Match. Craniomaxillofacial Trauma & Reconstruction. 2015; 8(3):262-270. https://doi.org/10.1055/s-0035-1558452
Chicago/Turabian StylePollock, Richard A., Ted W. Brown, Jr., and David M. Rubin. 2015. "“Phossy Jaw” and “Bis-Phossy Jaw” of the 19th and the 21st Centuries: The Diuturnity of John Walker and the Friction Match" Craniomaxillofacial Trauma & Reconstruction 8, no. 3: 262-270. https://doi.org/10.1055/s-0035-1558452
APA StylePollock, R. A., Brown, T. W., Jr., & Rubin, D. M. (2015). “Phossy Jaw” and “Bis-Phossy Jaw” of the 19th and the 21st Centuries: The Diuturnity of John Walker and the Friction Match. Craniomaxillofacial Trauma & Reconstruction, 8(3), 262-270. https://doi.org/10.1055/s-0035-1558452