Abstract
Coronoid process fractures are rarely encountered, commonly undiagnosed, usually asymptomatic, and most commonly treated conservatively, hence very little written about. We present two cases of coronoid process fractures with associated frontosphenoidal injuries.
Fracture of the coronoid process is rare and account for only 0.6 to 4.7% of all facial fractures [1]. They are usually simple and linear fractures with minimal displacement, since the fragment is splinted by the tendinous insertion of the temporalis muscle. But in cases of complex trauma, the bone might be displaced into the temporal fossa [2].
Natvig et al. [3] classified coronoid process fractures into two types:
- Intramuscular: where the fracture fragment is within the investing fascial attachment of the temporalis muscle.
- Submuscular: where the fracture is below the musculotendinous attachment. In these cases, there may be superior and medial displacement of the fragment.
The zygomatic complex shields the coronoid process; hence, an isolated coronoid fracture is rarely seen in the absence of an arch fracture [1].
Case Reports
Case 1
A 40-year-old male patient presented to our trauma center following a road traffic accident. Patient was referred to a neurosurgeon as he had frontosphenoidal trauma. He was managed conservatively by the neurosurgeon for the same.
As the patient also had facial injuries and difficulty in opening the mouth, he was referred to us. The computed tomography (CT) scan, apart from the fractures of the cranial bones, revealed a right zygomaticomaxillary complex (ZMC) fracture along with right coronoid, nasal bone, and an incomplete Le fort I fracture (Figure 1).
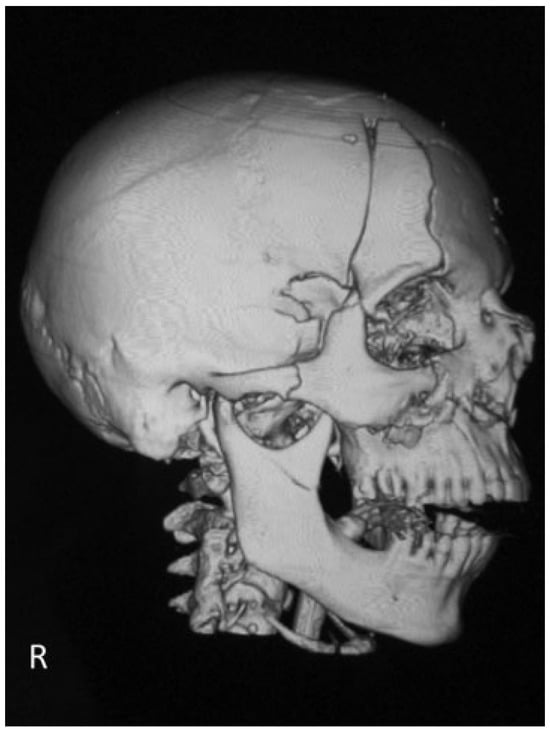
Figure 1.
The computed tomography (CT) scan, apart from the fractures of the cranial bones, revealed a right zygomaticomaxillary complex (ZMC) fracture along with right coronoid, nasal bone, and an incomplete Le fort I fracture.
All the facial bone fractures, apart from the right coronoid fracture, were managed with open reduction and internal fixation with mini plates.
Case 2
A 33-year-old male patient presented to our trauma center following a road traffic accident. Patient was referred to a neurosurgeon for the management of head injury. He was managed conservatively by the neurosurgeon.
The CT scan revealed frontosphenoidal fractures along with a left ZMC and left coronoid fracture (Figure 2).
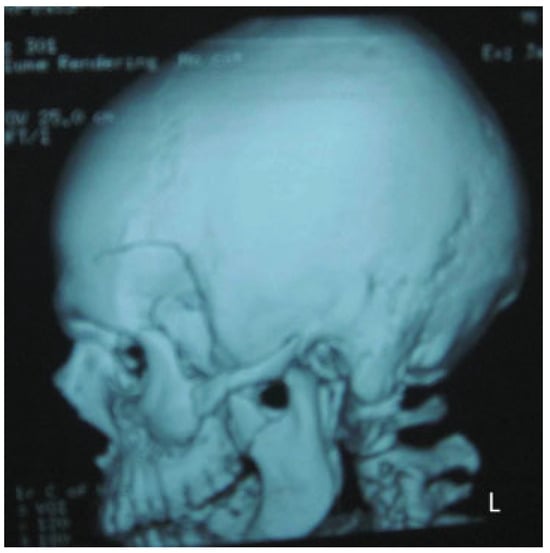
Figure 2.
The CT scan revealed frontosphenoidal fractures along with a left ZMC and left coronoid fracture.
Patient was managed with open reduction and internal fixation for the ZMC fracture and the coronoid process fracture was managed conservatively.
As both our patients had intramuscular coronoid fractures, they were managed conservatively for the same. They recovered uneventfully, and were asymptomatic postoperatively with no difficulty in mouth opening and lateral excursions of the mandible.
Discussion
Fractures of the coronoid process are often not evident clinically. Many such injuries go undiagnosed [4] because it is difficult to radiologically diagnose these fractures with conventional radiographs. But with the advent of CT, these are no longer difficult to accurately diagnose these fractures [5].
Isolated fractures of the coronoid process cause trismus and swelling in the region of the zygomatic arch. Swelling in the retromolar area and lateral cross bite are the other two clinical signs to look for when examining these patients [2].
In our case, we believe that the fracture of the coronoid process occurred due to the reflex contraction of the temporalis muscle as both the cases also had a cranial fracture at the site of origin of temporalis muscle.
Temporalis is a large, fan-shaped muscle arising from the temporal fossa (including the frontal and sphenoidal bone in the temporal fossa) of the skull and is inserted into the tip and medial aspect of the coronoid process [6]. It is a known fact that when a muscle is stretched, the myotactic reflex can lead to sudden excitation of the muscle spindles, and the reflex contraction of the large skeletal muscle fibers of the same muscle and closely allied synergistic muscles [7]. Therefore, a violent blow to the temporalis muscle can cause contraction of this muscle enough to cause a coronoid fracture (Figure 3 and Figure 4) [8].
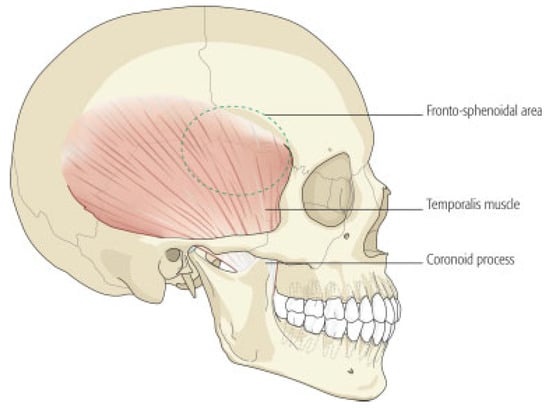
Figure 3.
Showing the attachment and insertion of the temporalis muscle.
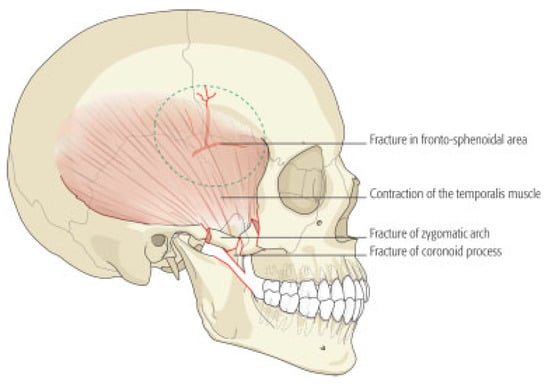
Figure 4.
Contraction of the temporalis muscle leading to coronoid process fracture.
Traditionally, the reason for zygomatic arch postfracture trismus was cited as impingement of translating coronoid process of the mandible. According to Fonseca and Betts, trismus after zygomatic arch fractures is also due to temporal muscle spasm secondary to impingement of the displaced fractures on the muscle, as the distance between the arch and the coronoid is very large to cause even actual mechanical interference. Hence, direct trauma to cause coronoid process fracture is unlikely [9].
Most of the authors have justified conservative management of the intramuscular coronoid fracture with soft, nonchewy diet. Intermaxillary fixation for approximately 3 weeks has been recommended in cases where the fracture is symptomatic as it will relieve the discomfort and aid in prompt healing [5].
In cases of submuscular fractures that might be large enough to interfere with mandibular functions, some authors have recommended an intraoral open reduction and fixation with wire osteosynthesis [10].
In coronoid process fractures, where the mandibular movements are limited due to fibrosis of temporalis muscle, the recommended treatment plan is the removal of the fractured coronoid segment.
Yaremchuck recommended rigid internal fixation for displaced coronoid fractures [12]. Therefore, there are a wide range of treatment options available for the management of coronoid fractures and the operating surgeon should customize the surgical plan based on the type of fracture and the symptoms presented by the patient.
References
- Philip, M.; Sivarajasingam, V.; Shepherd, J. Bilateral reflex fracture of the coronoid process of the mandible. A case report. Int J Oral Maxillofac Surg 1999, 28, 195–196. [Google Scholar] [CrossRef] [PubMed]
- Rapidis, A.D.; Papavassiliou, D.; Papadimitriou, J.; Koundouris, J.; Zachariadis, N. Fractures of the coronoid process of the mandible. An analysis of 52 cases. Int J Oral Surg 1985, 14, 126–130. [Google Scholar] [PubMed]
- Natvig, P.; Sicher, H.; Fodor, P.B. The rare isolated fracture of the coronoid process of the mandible. Plast Reconstr Surg 1970, 46, 168–172. [Google Scholar] [PubMed]
- Scrimshaw, G.C. Malar/orbital/zygomatic fracture causing fracture of underlying coronoid process. J Trauma 1978, 18, 367–368. [Google Scholar] [CrossRef] [PubMed]
- Takenoshita, Y.; Enomoto, T.; Oka, M. Healing of fractures of the coronoid process: Report of cases. J Oral Maxillofac Surg 1993, 51, 200–204. [Google Scholar] [PubMed]
- Bannister, L.H.; Berry, M.M.; Collins, P.; Dyson, M.; Dussek, J.E.; Ferguson, M.W.J. Gray’s Anatomy. In The Anatomical Basis of Medicine and Surgery, 38th ed.; Churchill Livingstone: London, UK, 1999. [Google Scholar]
- Guyton, A.C.; Hall, J.E. Text Book of Human Physiology; W.B. Saunders: London, UK, 1996; pp. 82–83. [Google Scholar]
- Rowe, N.L.; William, J.L. Maxillofacial Injuries; Churchill Livingstone: London, UK, 1985; Volume 1. [Google Scholar]
- Fonseca, W.; Betts, B. Powers. In Oral and Maxillofacial Trauma, 3rd ed.; Elsevier Saunders: St. Louis, MO, USA, 2005; Volume 1. [Google Scholar]
- de Oliveira, D.M.; Vasconcellos, R.J.; Laureano Filho, J.R.; Cypriano, R.V. Fracture of the coronoid and pterygoid processes by firearms: Case report. Braz Dent J 2007, 18, 168–170. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Johnson, R.L. Unusual (coronoid) fractures of mandible: Report of case. J Oral Surg 1958, 16, 73–77. [Google Scholar] [PubMed]
- Yaremchuk, M.J. Rigid internal fixation of a displaced mandibular coronoid fracture. J Craniofac Surg 1992, 3, 226–229. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the author. The Author(s) 2014.