Abstract
Management of fractures involving the frontal sinus seems to be more complex than merely obtaining an ideal reduction of the bony injuries. Multiple articles on the management of these fractures suggest that a great deal of controversy persists despite many years of surgical experience. The question posed in this article is whether or not the advent of endoscopic approaches has changed or should change the approaches/ algorithms used in the management of these challenging fractures. It is the conclusion of these authors that endoscopic techniques can indeed allow us to change the algorithm for management of frontal sinus trauma. New algorithms are proposed that should provide guidance to craniomaxillofacial surgeons treating these injuries in the endoscopic age.
In comparison to most other craniomaxillofacial fractures, management of fractures involving the frontal sinus seems to be more complex than merely obtaining an ideal reduction of the bony injuries. Multiple articles on the management of these fractures suggest that a great deal of controversy persists, despite many years of surgical experience [1,2,3,4,5,6,7]. The controversy persists because these injuries have a propensity to develop significant delayed complications, sometimes years after an excellent reduction with a good cosmetic repair has been accomplished [8]. Whether or not to explore rather than observe a nondisplaced or minimally displaced fracture, and what procedure to perform if exploration is considered remain controversial. Furthermore, how severe must displacement/disruption be to require exploration and/or repair, whether or not a transient cerebrospinal fluid (CSF) leak requires exploration and/or repair, and whether or not the sinus should be obliterated and/or cranialized also remain areas of great controversy in the literature and among experienced surgeons. The question posed in this article is whether or not the advent of endoscopic approaches has changed or should change the approaches/algorithms used in the management of these challenging fractures. It is the opinion of the authors that the answer is “yes,” and this article will discuss and illustrate some of the ways in which the endoscope offers new and hopefully better options for the management of these cases.
Why Is Management of the Frontal Sinus so Challenging?
First and foremost, it is believed that avoiding frontal sinus complications seems to hinge on proper functioning of the nasofrontal duct (NFD), which would then allow drainage of the mucus produced in the sinus into the nasal cavity. (Note that anatomical studies raise question as to whether or not the NFD is a “true duct” in the majority of humans. Therefore, it will be referred to as the “frontal sinus outflow tract” [FSOT].) Fractures that involve the floor of the frontal sinus create significant risk of FSOT injury/disruption. Numerous authors have attempted to determine which fractures are most likely to predict an NFD injury and the best known algorithm for this was developed by Robert Stanley over 20 years ago [2,3]. He found that involvement of the supraorbital rims and nasoethmoid complex (NOE, also known as nasoorbital ethmoid [NOE] fractures) had the highest association with FSOT injury, followed by fractures that involved the anterior and posterior frontal sinus walls. It should be noted that involvement of the frontal recess in the anterior ethmoid sinuses is probably the cause of frontal sinus outflow tract damage in the majority of patients in which it occurs.
What is generally agreed upon by most CMF surgeons is that damage to the sinus outflow tract(s) is a likely cause of later frontal sinus problems, including infection and mucocele formation. How to avoid these complications and how to manage them when they occur remain important clinical management questions.
Furthermore, as frontal sinus infection and mucocele can result in orbital and intracranial complications, including visual disturbance, meningitis, brain abscess, or even death, there remains a particularly powerful impetus for surgeons to avoid these problems. Many surgeons have advocated frontal sinus obliteration and cranialization after all severe fractures in hopes of avoiding these dreaded complications [9,10,11]. However, these procedures are not without their own challenges and failures as well [12]. Bell et al. noted in their series of 116 patients that 50 patients underwent surgical intervention, including sinus obliteration in 5 and cranialization in 16. With maximum follow-up of only 90 weeks, 13.6% of these 50 patients suffered complications, including meningitis, brain abscess, CSF leak, mucocele, and frontal osteomyelitis, despite these surgical interventions [1].
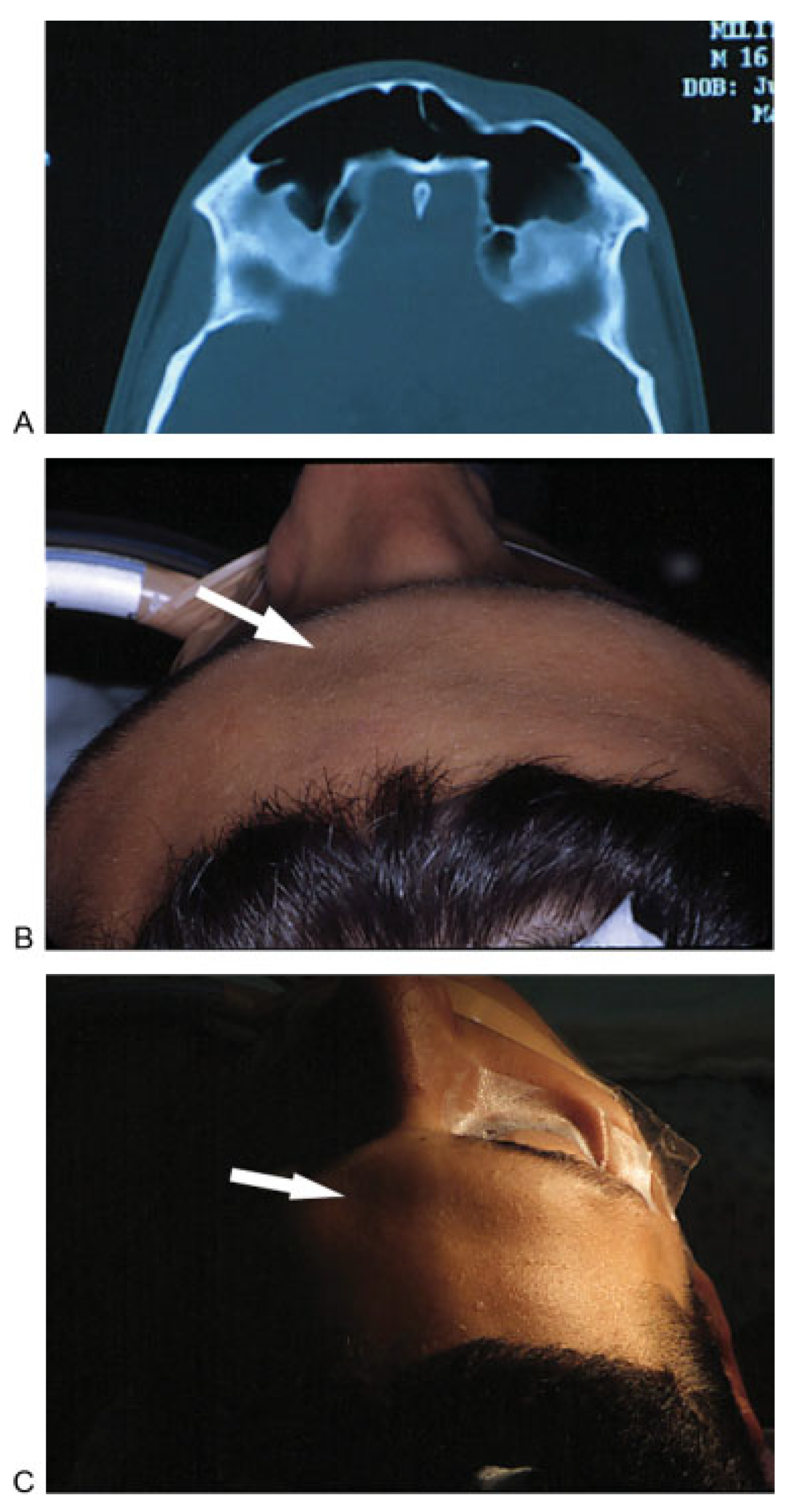
Numerous algorithms have been offered by surgeons to facilitate management of these difficult fractures [3,4,10,13]. In general, the anterior wall of the frontal sinus is repaired for cosmetic reasons, as it provides the forehead contour. A significant depression will generally leave the patient with a deformity such as a dent or irregularity (Figure 1A–C). Traditional approaches to such injuries include direct access through a laceration, brow and forehead crease (wrinkle line) incisions, and coronal incisions. Unfortunately, each of these options offers certain drawbacks and disadvantages. The direct approach through a laceration may require extending the skin wound for access, which will result in a more extensive scar. The brow incisions often result in unsightly scars and forehead and scalp numbness. Coronal incisions involve fairly extensive dissection with potential for numbness, hair loss, blood loss, and possibly unsightly scars in balding males.
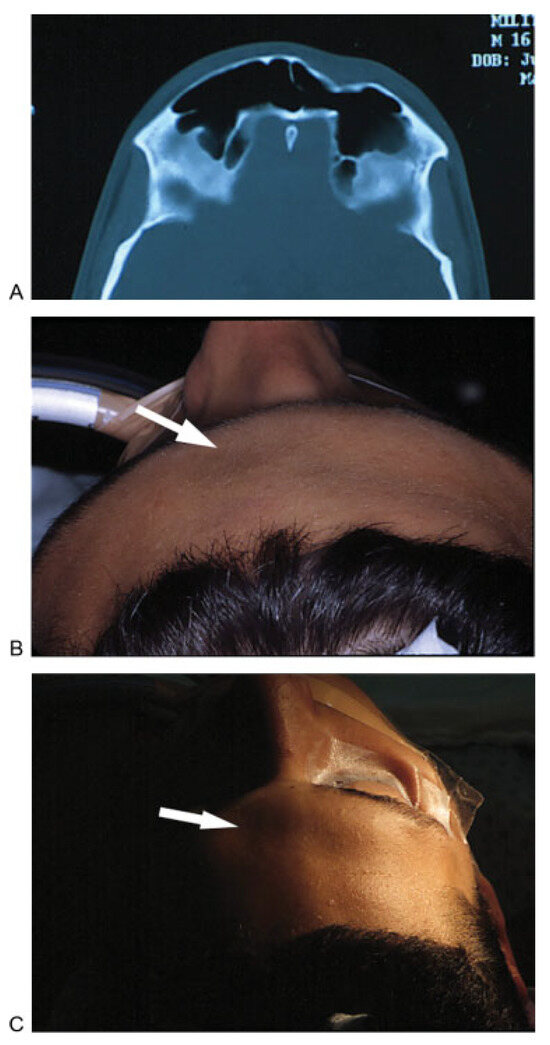
Figure 1.
(A) Axial computed tomographic image demonstrates a displaced fracture of the anterior table of the left frontal sinus. (B, C) Photographs showing depression along the left forehead as a result of the displaced fracture.
Posterior wall fractures present additional dilemmas, as it can be difficult to discern the presence of dural tears in the absence of obvious rhinorrhea. When a posterior wall fracture is nondisplaced, and the sinus is fully aerated, there is little concern for dural laceration and CSF leakage. However, if there is some degree of opacification overlying the fracture or if the sinus is completely opacified, the degree of pathology can be difficult to determine. The abnormality could be related to several findings, including CSF in the sinus, inflammation with polypoid change, blood and hematoma or even brain herniating into the sinus. It should be understood that in the pathophysiology of a posterior wall frontal sinus fracture, there had to be at least transient displacement during the impact to create the fracture, even though the bones return to their original position after the fracture occurs.
Most algorithms recommend sinus obliteration (or cranialization) if the floor (which of course contains the outflow tract) appears damaged on computed tomographic (CT) scan, and in the study by Rodriguez et al., complications were rare in the absence of this finding. Still, obliteration is a challenging and potentially risky procedure, and techniques and choice of obliteration material remain controversial as well [7]. In addition, as previously noted, it is not clear that obliteration is completely protective. Postoperative evaluation of the patient with headache who has had a fat obliteration of the frontal sinuses can be extremely challenging because CT and MRI may have difficulty discerning between living fat, scar, and various fluid densities.
Note that the most extensive review of frontal sinus fractures ever performed at a single institution (857 patients over a 26-year period) performed by Rodriguez et al. [7] indicated that 98.5% of complications occurred in patients with evidence of frontal sinus outflow tract injury by CT criteria. Overall, obliteration had a 10% complication rate in their series, and osteoneogenesis (drilling out the mucosa and leaving the sinus empty to fill in by itself) had a 56% complication rate. Furthermore, they noted that the best obliteration material was autologous bone, with autologous fat having a 22% complication rate (9 of 41).
What Might the Endoscope Offer?
The endoscope has thus far proven useful in three key areas:
- Diagnosis
- Primary treatment
- Delayed intervention
Use of the Endoscope in Diagnosis
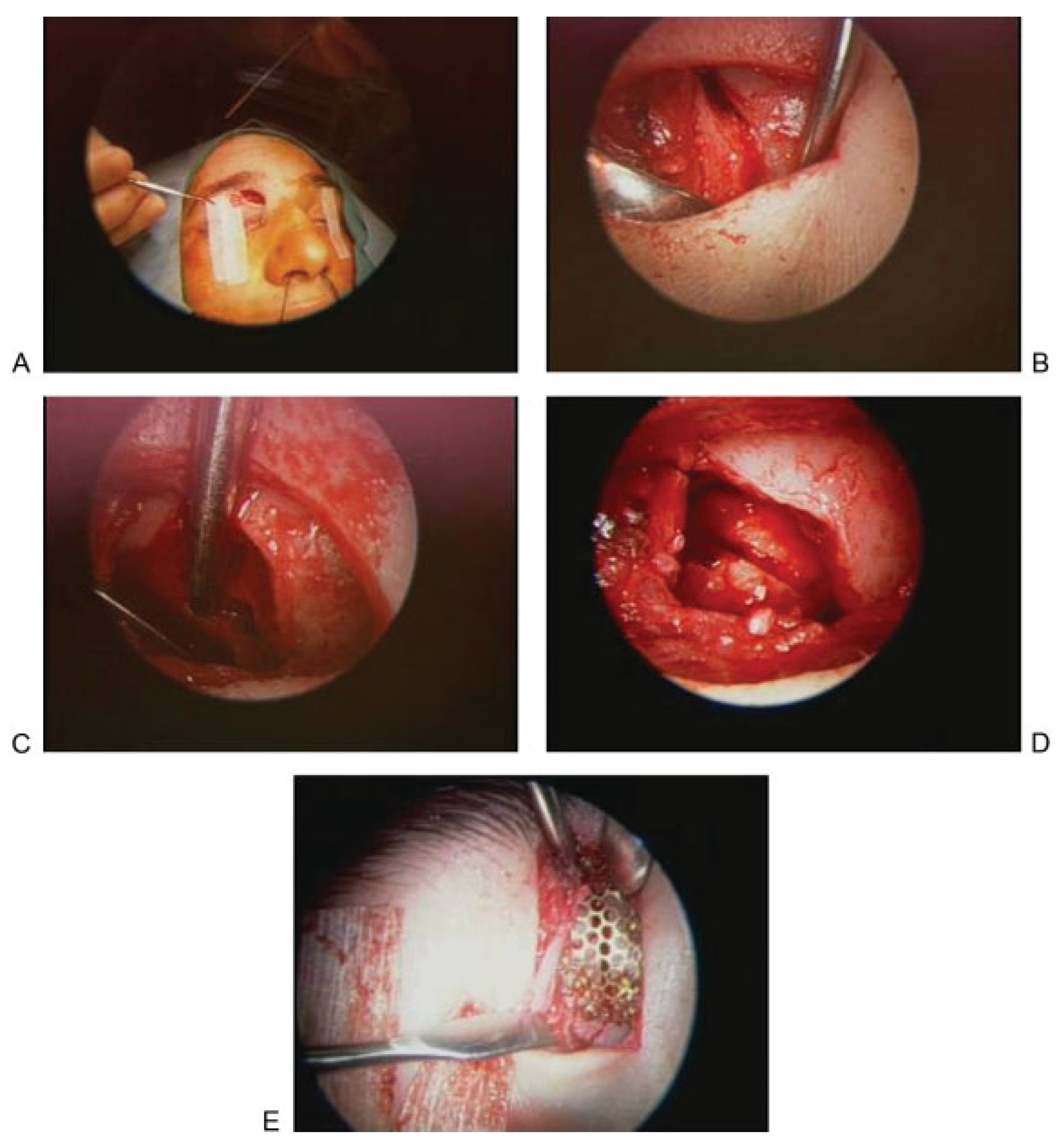
As noted above, there are two areas in which our radiologic assessments remain less than ideal. One is the evaluation of the frontal sinus outflow tract. The other is the posterior wall. The endoscope has proved helpful in both of these situations (Figure 2A–E). If there is a defect in the anterior wall inferiorly or of the supraorbital rim, a scope can be placed through a small incision (trephination approach) and the outflow tract can be visualized using angled lenses. If the bone is intact, a small medial incision below the brow will provide access to the medial inferior bone. A small trephination of the sinus can be accomplished with a burr, and a scope can then be placed into the sinus. Similarly, using the same trephination approach, a scope can be used to assess the posterior wall [14]. In the authors’ experience, on more than one occasion, brain has been encountered in the sinus, herniating through a nondisplaced fracture. When used in this manner in the acute trauma setting, trephination combined with endoscopic visualization can alter the treatment of frontal sinus injuries.
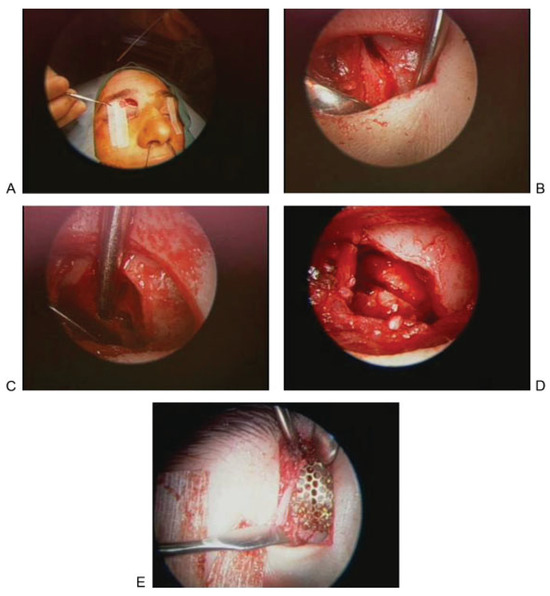
Figure 2.
Trephination approach for endoscopic assessment of the posterior wall. (A) Incision. (B) Exposure of fracture. (C) Exposure of sinus. (D) Exposure of posterior wall of frontal sinus. (E) Repair.
Endoscopic Management of Fractures
This approach is generally reserved for management of depressed anterior wall fractures (see Figure 1). Two approaches have been advocated: (1) endoscopic fracture reduction with percutaneous repair and (2) endoscopic camouflage.
For endoscopic fracture reduction, a brow lift approach is used, usually with two paramedian 1 to 2 cm incisions within the hairline. A long plate can be introduced and fixed percutaneously to the solid bone on either side of the fracture. Fragments can then be reduced and fixed to the plate with screws. This is a challenging technique, and few advocate its use, as severe fractures are best opened, and milder fractures are actually harder to reduce due to the large amount of force that has to be exerted to return the fragments to their preinjury position [15].
An alternative approach for endoscopic anterior table fracture reduction involves reduction through an endoscopic frontal sinusotomy or a frontal sinus trephination. In this technique, the surgeon gains access to the frontal sinus using endoscopic sinus surgical techniques or a frontal sinus trephination. Curettes and balloons can then be used to perform fracture reduction [16].
Endoscopic camouflage allows for restoration of the frontal contour in the absence of fracture reduction. Endoscopic camouflage is a useful technique that has been advocated by Kellman and Strong [15,17]. The camouflage approach offers two main advantages, in that it not only avoids large incisions and exposures (and therefore qualifies as a more minimally invasive technique), but it also allows for delayed intervention. This provides the particular advantage of waiting to see if the depression due to the fracture will be severe enough to justify intervention. This is in contrast to the reduction approach which requires repair before the bone healing in the malaligned position. Materials that have been advocated for the camouflage technique include porous polyethylene, titanium mesh, and hydroxyapatite cement [15,17]. Figure 3 shows CT and intraoperative images from a patient treated with the endoscopic camouflage technique for a depressed left frontal sinus fracture.
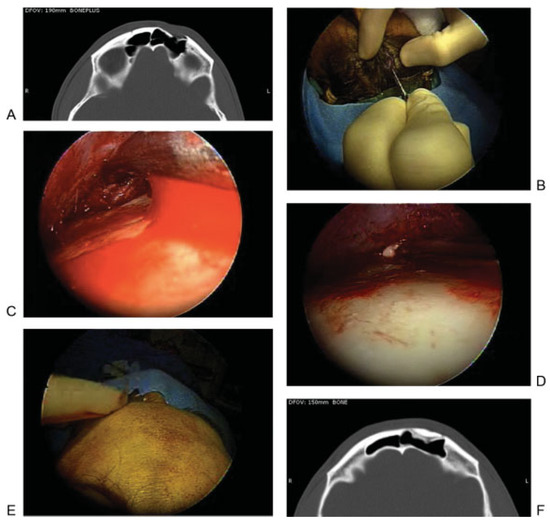
Figure 3.
(A)Axial computed tomographic image showing depression related to an anterior table fracture. (B–E) Intraoperative photographs showing repair of frontal depression related to an anterior table fracture. (B) After making an incision, (C) an endoscope is used to dissect in the subperiosteal plane and expose the depression. (D) Hydroxyapatite cement is then injected and gentle pressure is used to smooth the cement to restore the appropriate contour. (F) Axial postoperative image showing excellent restoration of the frontal contour after placement of bone cement.
Outflow Tract/Frontal Sinus Outflow Tract Injury
The endoscope adds another dimension to the management of these fractures, particularly if the posterior sinus wall is not significantly involved. Traditionally, FSOT injury has been an indication for frontal sinus obliteration. There is evidence from cat studies which indicates that FSOT obstruction leads to mucocele formation [18]. It is of course clear in humans that poor drainage of the sinuses will predispose the patient to infection and other complications [7]. Sinus obliteration is performed to create a “safe sinus,” to eliminate the sinus mucosa and thereby minimize the risk of development of sinusitis and/or mucocele. Part of the reason for this is that it is difficult to treat frontal sinusitis when the outflow tract is obstructed, and traditionally, chronic infections and mucoceles have been indications for osteoplastic obliteration as well.
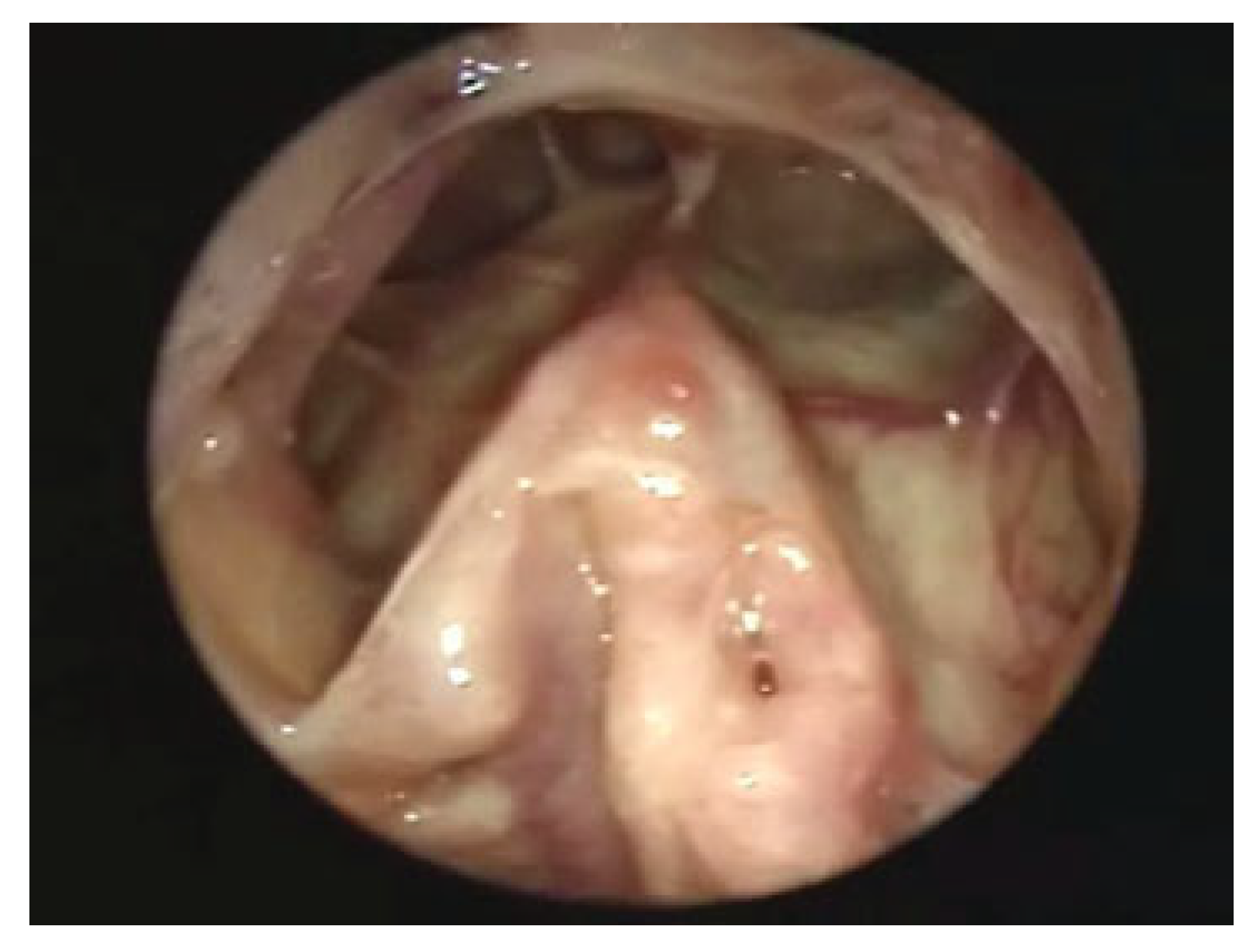
However, the endoscope offers other possible interventions. The Draf III procedure (also known as the endoscopic Lothrop) allows the surgeon to endoscopically, transnasally create a common outflow tract including the outflow tracts of both frontal sinuses and the frontal floor bilaterally between them, so that there can be wide drainage into the nose (Figure 4). This option allows the surgeon managing the fractures to consider a more conservative approach at the time of the injury. So long as the patient is available for follow-up, patients can be watched carefully and a CTscan in 3 to 6 months can be used to see if the frontal sinuses are aerated. Aerated sinuses suggest patent and functional frontal sinus outflow tracts, while persistent sinus opacification suggests sinus outflow tract obstruction. In cases of obstruction, the endoscopic Draf III will allow the surgeon to reestablish a pathway for frontal drainage [19]. A recent systematic review by Carter et al. [20] suggests that this is a reasonable alternative to obliteration. Endoscopic techniques for drainage of the frontal sinuses through the nose provide surgeons with an option that allows the sinuses to be effectively managed without obliteration after the fractures have healed. This allows time to determine if the sinuses might be able to develop successful drainage on their own, rather than committing to immediate intervention.
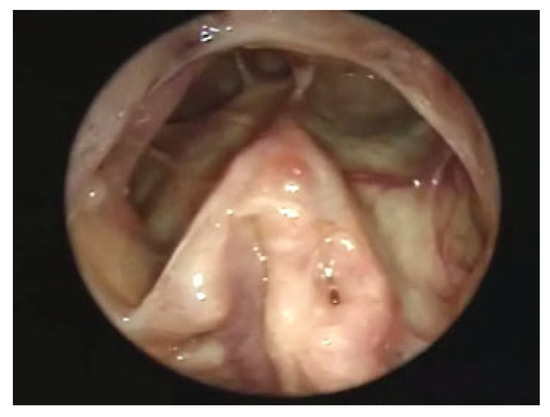
Figure 4.
Healed endoscopic view after an endoscopic modified Lothrop procedure.
The same concept can be applied to mucocele formation. Most mucoceles can now be managed endoscopically by marsupializing them into the nasal cavity [21,22]. This option makes them less threatening than before, and, so long as follow-up can be assured, intervention can be reserved for those who develop problems.
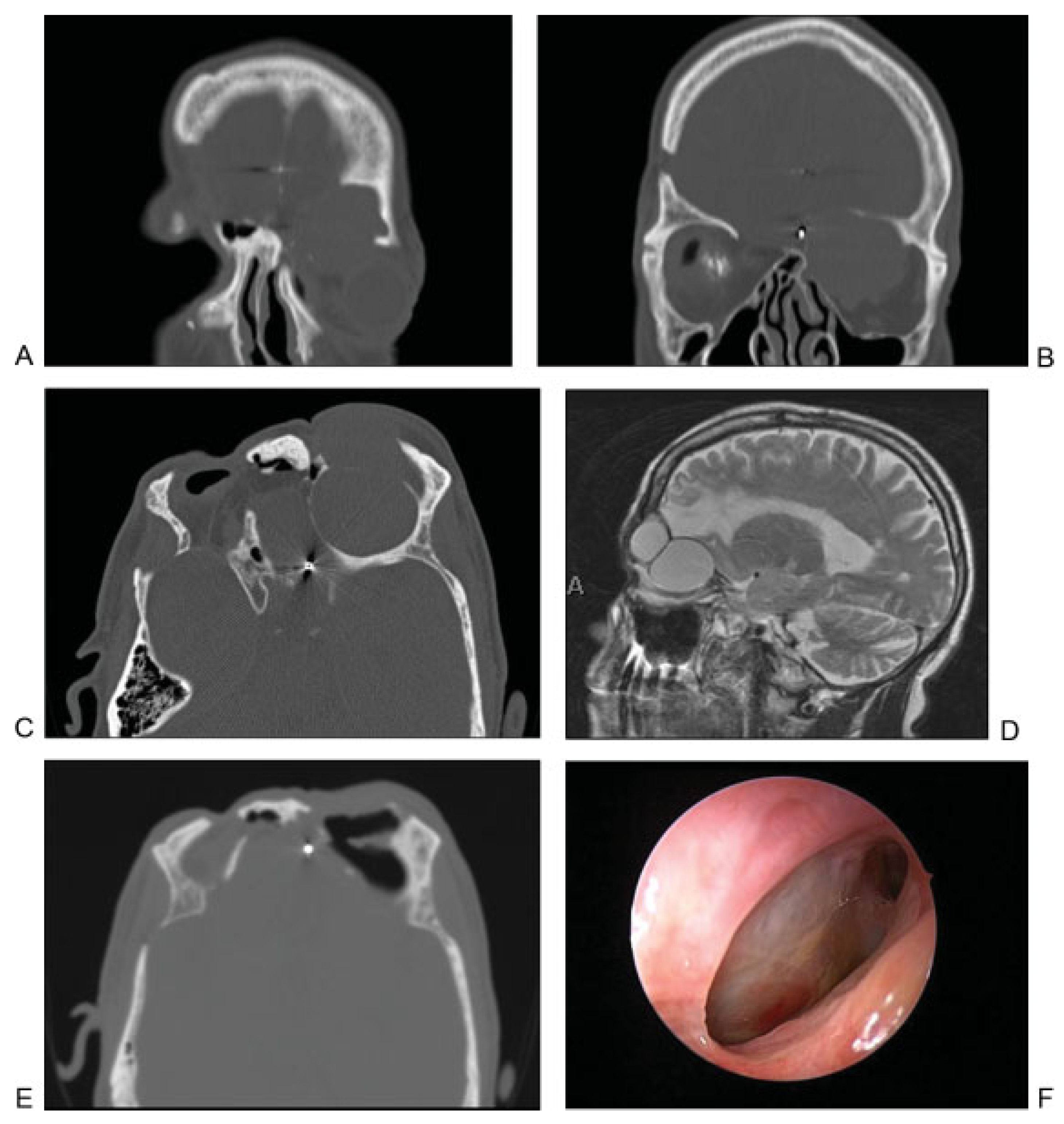
Mucoceles may also arise after obliterative procedures have been performed for trauma. Endoscopic marsupialization can also be used in these cases of delayed mucocele formation. Figure 5 shows images of a patient who developed two separate mucoceles after frontal sinus cranialization for extensive craniofacial trauma. The patient also had severe right orbital trauma at the time of his original injury and had undergone right enucleation. The patient presented with vision loss in his left eye approximately 12 years after his original injury and treatment. After being diagnosed with orbital and intracranial mucoceles, the patient underwent endoscopic marsupialization. The patient has subsequently been followed for 4 years, and continues be asymptomatic and has patent outflow tract to the mucocele cavities (Figure 5).
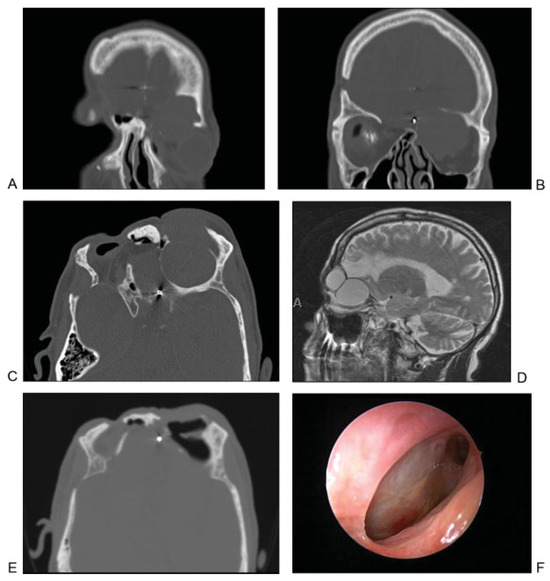
Figure 5.
(A) Coronal computed tomographic (CT) image showing mucocele that developed in a delayed fashion after extensive frontal sinus trauma and previous cranialization. Image shows mucocele with orbital and intracranial involvement. (B) Coronal CT image showing orbital mucocele. (C) Axial CT image demonstrating two separate mucoceles involving the left frontal and orbital regions. (D) Sagittal MRI demonstrating two distinct mucoceles. (E) Postoperative axial CT image demonstrating aeration of both mucocele cavities after endoscopic marsupialization. (F) Postoperative endoscopic view of the outflow tract of the two mucoceles after complete healing.
Posterior Wall Defects
Large posterior wall defects still require evaluation and management via an open approach. Obliteration via cranialization is preferred and likely represents the safest approach to these injuries.
However, the endoscope does offer new options for smaller defects and posterior wall encephaloceles and CSF leaks. For medial posterior defects, the Draf III actually provides access through the nose [23]. If the area of encephalocele and/or CSF leak can be visualized and instrumented, it can generally be repaired. For more lateral defects, a trephination can be performed either through the anterior wall or through the floor. Encephaloceles that have protruded into the sinus in this area can generally be shrunken with bipolar cautery. Repair can be performed using various graft materials, including fascia, cartilage, bone, and mucosa. In recent years, the vascularized nasoseptal flap has gained popularity for endoscopic reconstruction of skull base defects, and this flap can be useful in the management of some posterior table defects [24]. The goal is to obtain a watertight repair of the defect at the time of surgery if a satisfactory postoperative outcome is to be dependably anticipated.
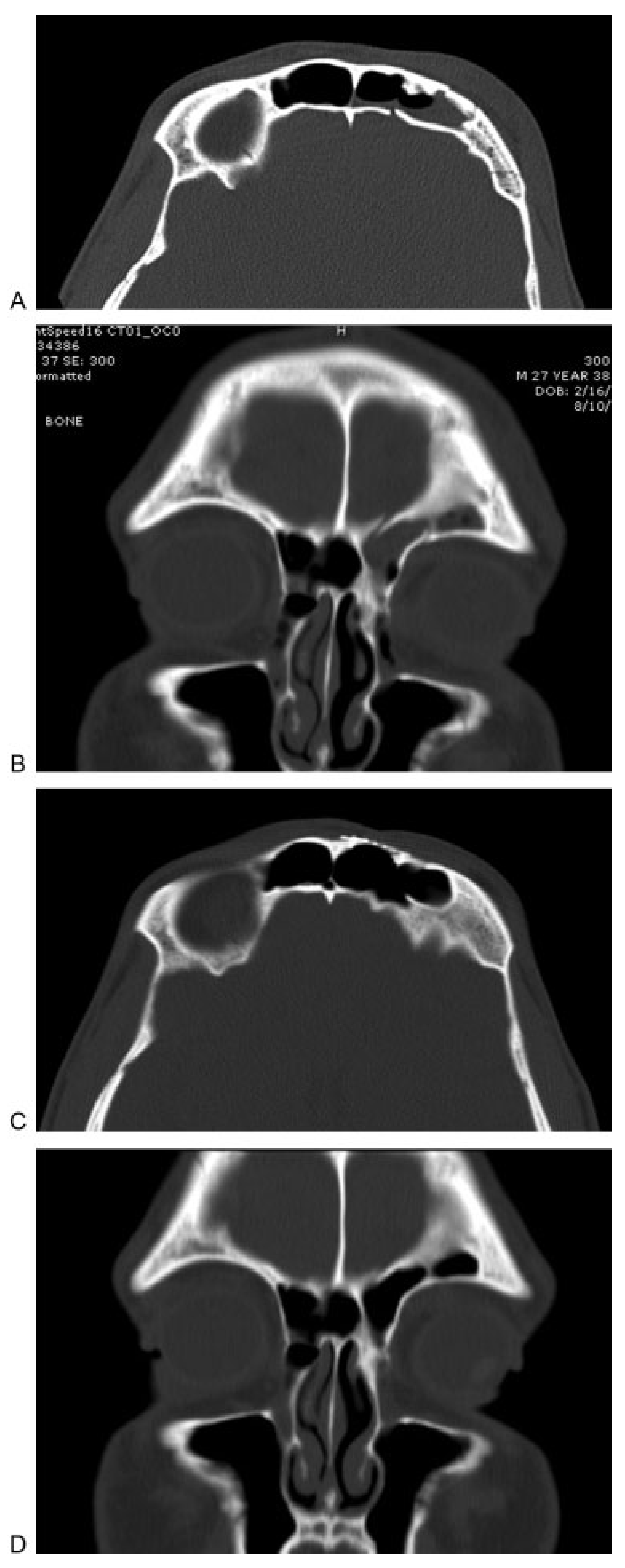
Figure 6 and Figure 7 illustrate cases in which trephination was used to repair posterior wall defects. Figure 6 demonstrates a situation in which the patient had active CSF rhinorrhea at the time of initial injury. Imaging studies demonstrated a fracture involving the posterior table of the frontal sinus, extending from the roof of the frontal sinus to the ethmoid skull base. The ethmoid portion of the defect was repaired using a graft by way of a transnasal endoscopic approach. However, the apex of the frontal sinus defect could not be reached in this way and was accessed through a frontal sinus trephination. Although there was not a large defect in the bone, there was an active CSF leak along the length of the fracture. The entirety of the defect was repaired with placement of a mucosal graft, and the trephination site was repaired using a small piece of titanium mesh. Postoperative imaging has shown a well aerated and healed frontal sinus, and endoscopic visualization has shown a patent frontal sinus outflow tract.
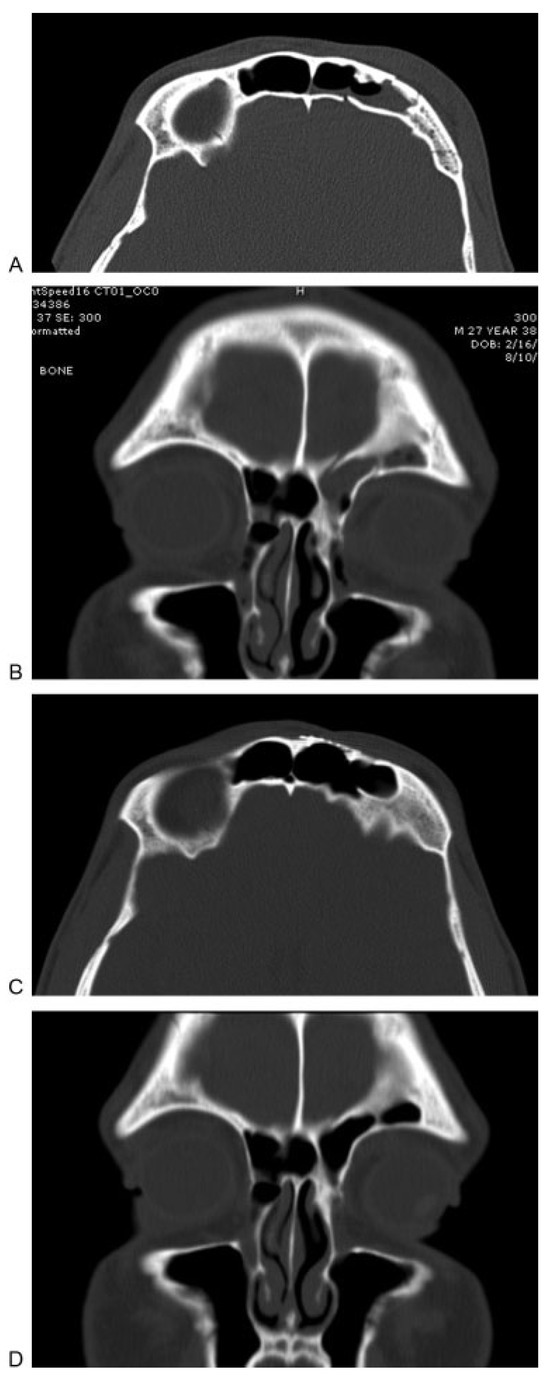
Figure 6.
(A, B) Axial and coronal computed tomographic (CT) images demonstrating a fracture involving the posterior table of the left frontal sinus. Fluid is also seen in the sinus. (C, D) Postoperative axial and coronal CT images demonstrating a well aerated and healed frontal sinus after use of a trephination for repair of the cerebrospinal fluid leak resulting from the defect. The axial image shows the titanium mesh used for reconstruction of the defect resulting from the entry into the frontal sinus.
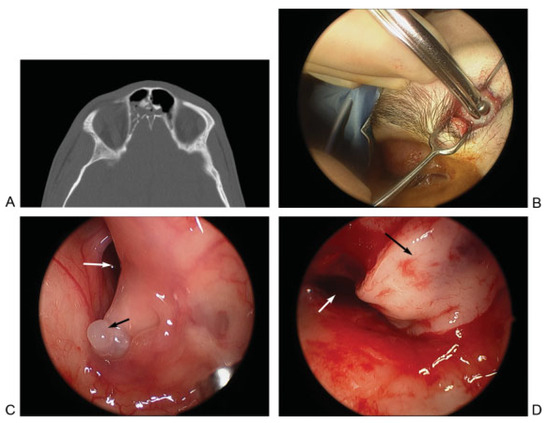
Figure 7.
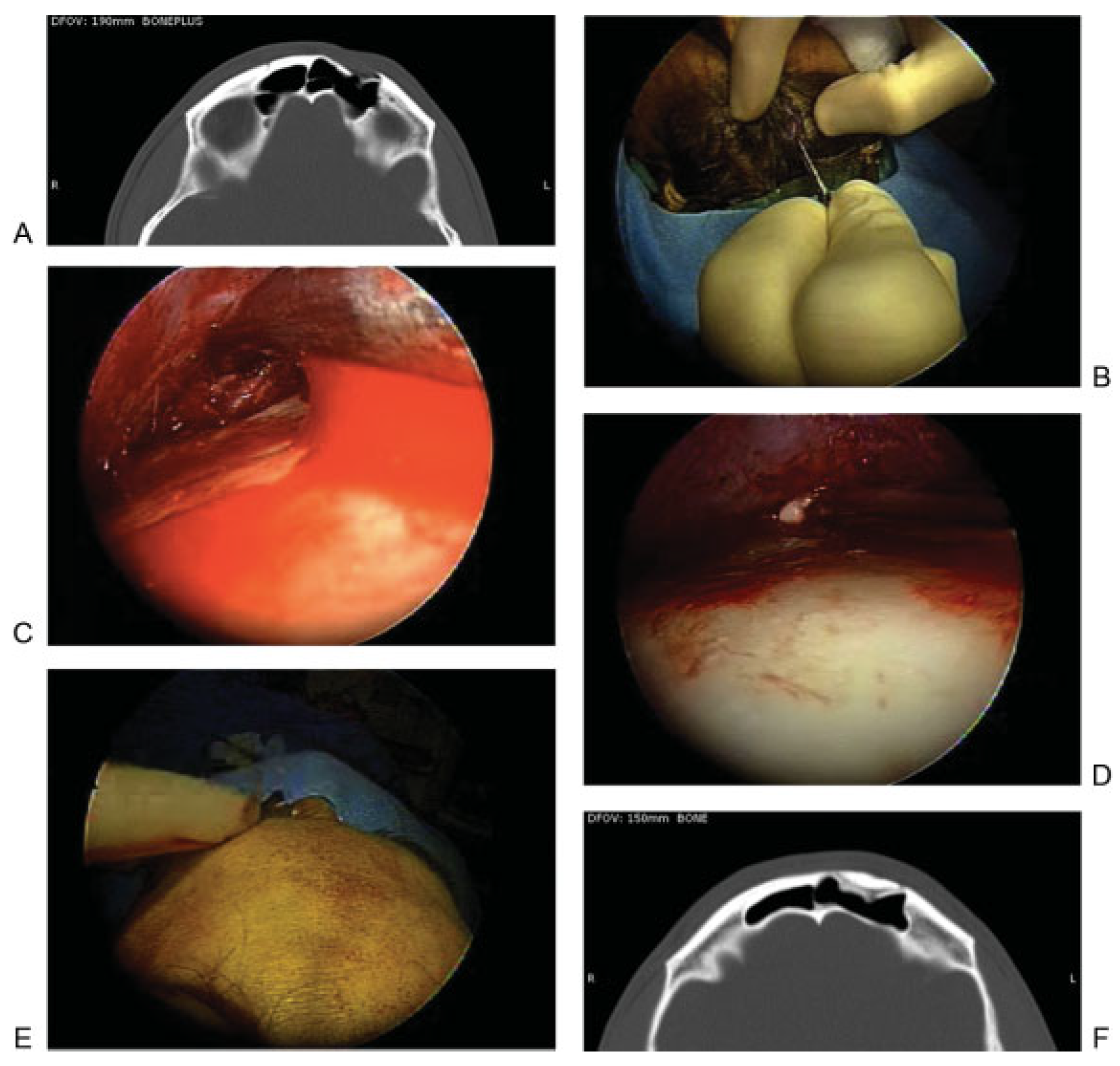
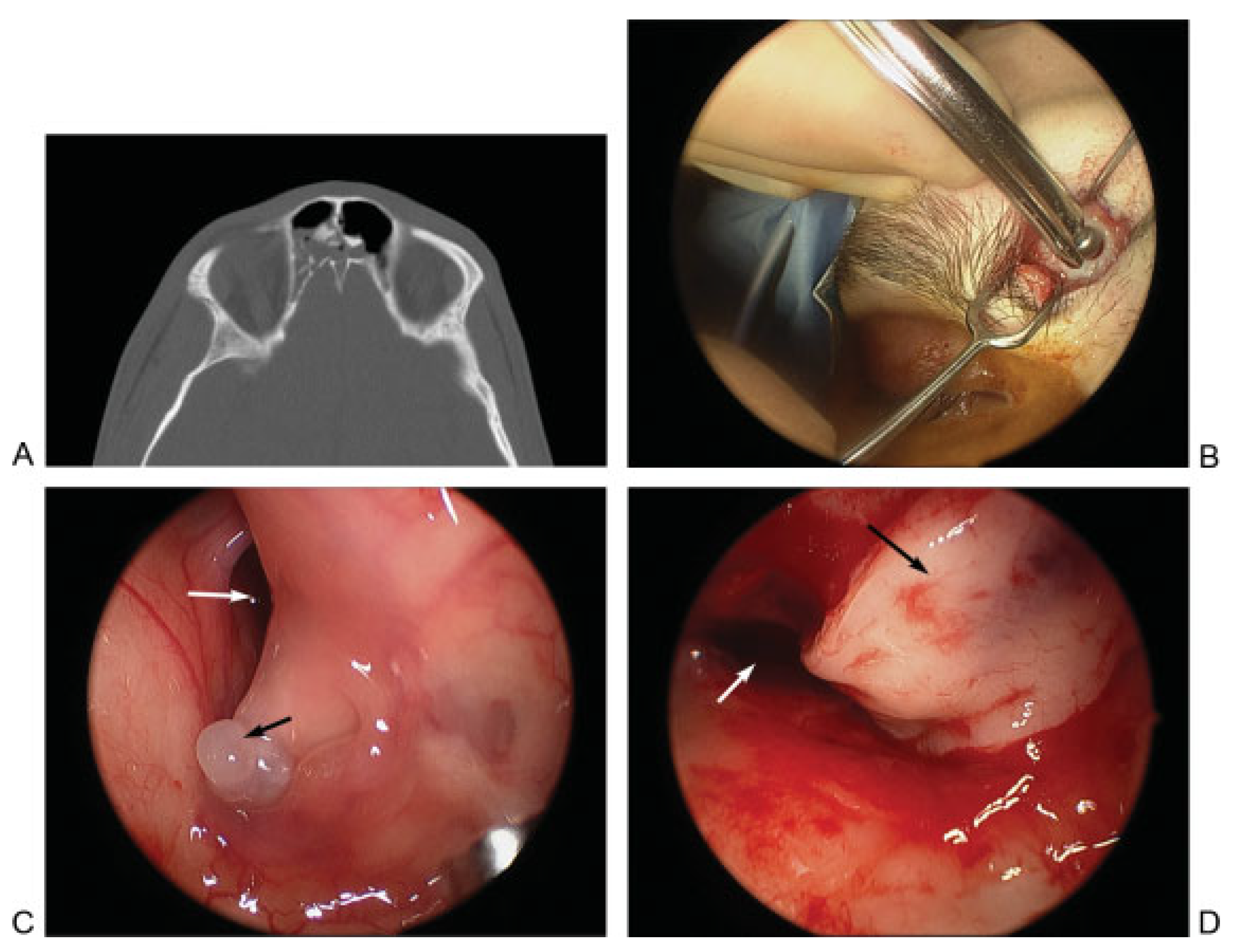
(A) Axial computed tomographic showing fractures of the posterior aspect of the right frontal sinus and the intersinus septum. A frontal sinus trephination approach was used to manage this defect. (B) Intraoperative picture showing a drill being used to perform the trephination and expose the frontal sinus lumen. (C) Endoscopic view of the frontal sinus lumen through the trephination shows a small area of brain herniation (black arrow) into the frontal sinus through the posterior table defect. Endoscopic visualization also shows a patent frontal sinus outflow tract (white arrow). (D) After encephalocele cauterization, repair was performed using a bone graft and mucosal graft. Image shows mucosal graft in place (black arrow) and that the frontal sinus outflow tract remains patent (white arrow).
The patient in Figure 7A did not have an active CSF leak at the time of initial injury. Imaging showed a fracture along the posterior frontal sinus wall. In the absence of a CSF leak, no acute exploration or repair was performed. The patient presented 2 years later with an episode of meningitis. Imaging revealed an encephalocele at the site of the previous posterior wall injury. The defect was repaired by way of a frontal sinus trephination approach, as shown in Figure 7B–D. In this case, the defect was repaired using bone and mucosal grafts while maintaining a patent frontal sinus outflow tract.
New Algorithm in the Endoscopic Age
It should be apparent from the above that the endoscope has indeed changed the algorithm for the management of frontal sinus trauma. Table 1 summarizes the relevant literature describing the use of endoscopic techniques in the evaluation and management of frontal sinus injuries. Although the number of articles is limited, the ideas introduced in the literature can have the potential to change management in many cases. Figure 8 represents a new algorithm to be considered for management of frontal sinus fractures in the “endoscopic age.”

Table 1.
Summary of the literature describing use of endoscopic techniques for the management of frontal sinus trauma.
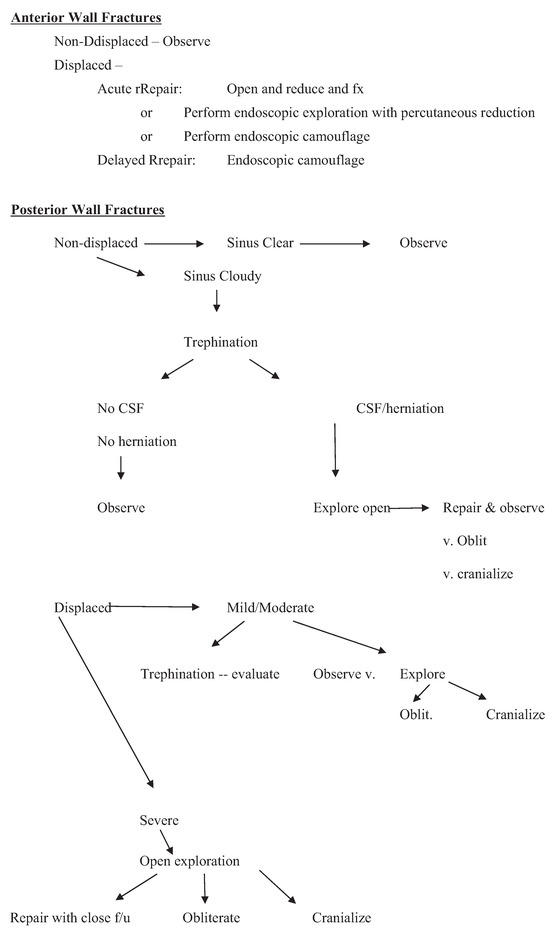
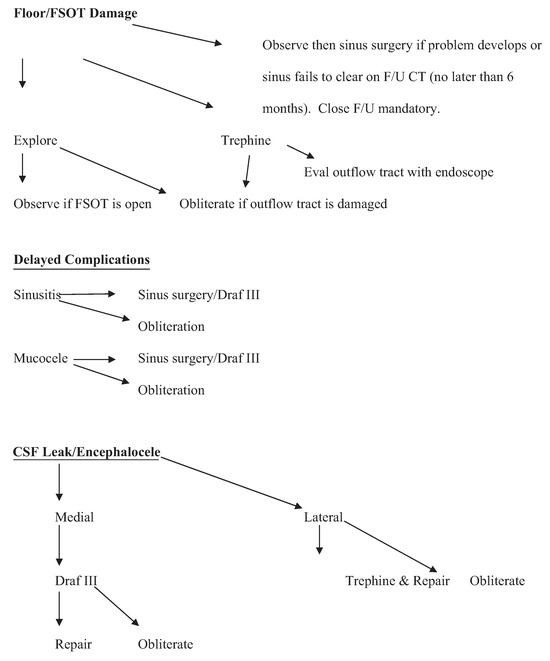
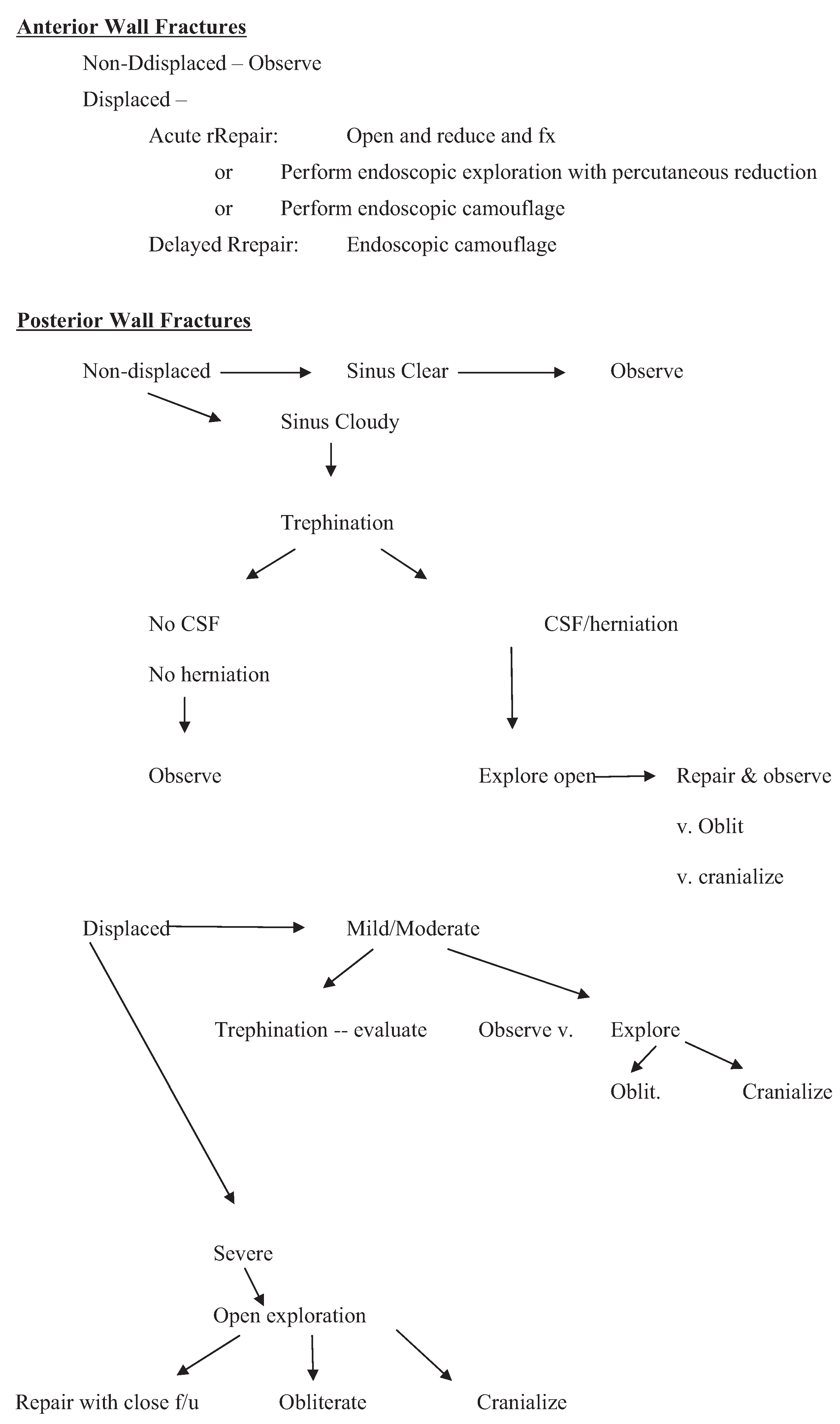
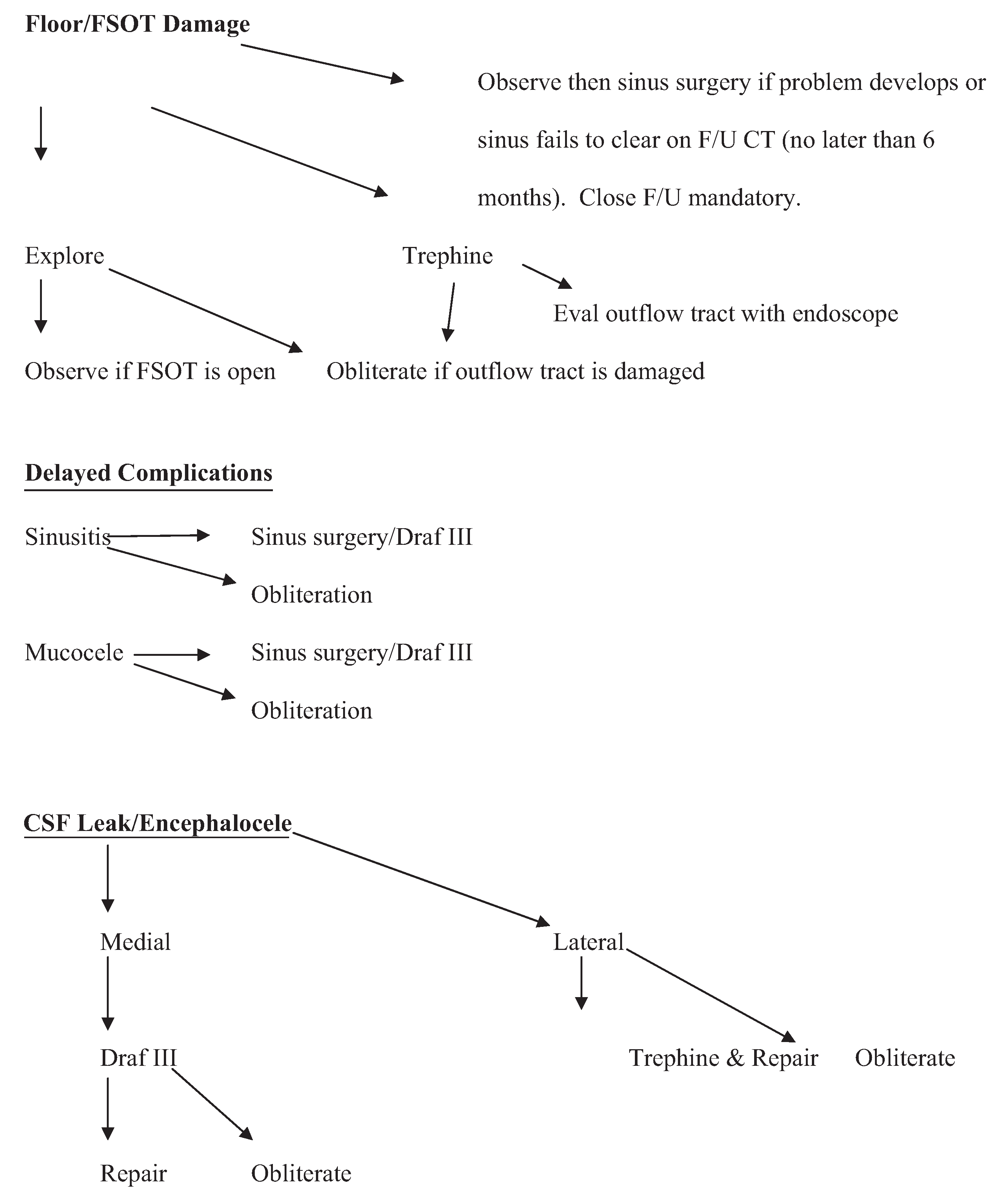
Figure 8.
New algorithm to be considered for management of frontal sinus fractures in the “endoscopic age.” CSF, cerebrospinal fluid; CT, computed tomography; FSOT, frontal sinus outflow tract.
Conclusion
The advent of endoscopic techniques can indeed allow us to change the algorithm for management of frontal sinus trauma. New algorithms are proposed that should provide guidance to craniomaxillofacial surgeons treating these injuries in the endoscopic age.
Notes
Presented in part at the AOCMF Symposium, Davos, Switzerland, December 2011.
References
- Bell, R.B.; Dierks, E.J.; Brar, P.; Potter, J.K.; Potter, B.E. A protocol for the management of frontal sinus fractures emphasizing sinus preservation. J Oral Maxillofac Surg 2007, 65, 825–839. [Google Scholar] [CrossRef]
- Stanley, R.B., Jr.; Becker, T.S. Injuries of the nasofrontal orifices in frontal sinus fractures. Laryngoscope 1987, 97, 728–731. [Google Scholar] [CrossRef] [PubMed]
- Gonty, A.A.; Marciani, R.D.; Adornato, D.C. Management of frontal sinus fractures: a review of 33 cases. J Oral Maxillofac Surg 1999, 57, 372–379, discussion 380–381. [Google Scholar] [CrossRef] [PubMed]
- Gonty, A.A.; Marciani, R.D.; Adornato, D.C. Management of frontal sinus fractures: a review of 33 cases. J Oral Maxillofac Surg 1999, 57, 372–379, discussion 380–381. [Google Scholar] [CrossRef]
- Raveh, J.; Vuillemin, T.; Sutter, F. Subcranial management of 395 combined frontobasal-midface fractures. Arch Otolaryngol Head Neck Surg 1988, 114, 1114–1122. [Google Scholar] [CrossRef]
- Schultz, R.C. Frontal sinus and supraorbital fractures from vehicle accidents. Clin Plast Surg 1975, 2, 93–106. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, E.D.; Stanwix, M.G.; Nam, A.J.; et al. Twenty-six-year experience treating frontal sinus fractures: a novel algorithm based on anatomical fracture pattern and failure of conventional techniques. Plast Reconstr Surg 2008, 122, 1850–1866. [Google Scholar] [CrossRef]
- Metzinger, S.E.; Metzinger, R.C. Complications of frontal sinus fractures. Craniomaxillofac Trauma Reconstr 2009, 2, 27–34. [Google Scholar] [CrossRef]
- Swinson, B.D.; Jerjes, W.; Thompson, G. Current practice in the management of frontal sinus fractures. J Laryngol Otol 2004, 118, 927–932. [Google Scholar] [CrossRef]
- Rohrich, R.J.; Hollier, L.H. Management of frontal sinus fractures. Changing concepts. Clin Plast Surg 1992, 19, 219–232. [Google Scholar] [CrossRef]
- Rohrich, R.J.; Hollier, L. The role of the nasofrontal duct in frontal sinus fracture management. J Craniomaxillofac Trauma 1996, 2, 31–40. [Google Scholar] [PubMed]
- Weber, R.; Draf, W.; Keerl, R.; et al. Osteoplastic frontal sinus surgery with fat obliteration: technique and long-term results using magnetic resonance imaging in 82 operations. Laryngoscope 2000, 110, 1037–1044. [Google Scholar] [CrossRef] [PubMed]
- Chen, K.T.; Chen, C.T.; Mardini, S.; Tsay, P.K.; Chen, Y.R. Frontal sinus fractures: a treatment algorithm and assessment of outcomes based on 78 clinical cases. Plast Reconstr Surg 2006, 118, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Crozier, D.L.; Hwang, P.H.; Goyal, P. The endoscopic-assisted trephination approach for repair of frontal sinus cerebrospinal fluid leaks. Laryngoscope 2013, 123, 321–325. [Google Scholar] [CrossRef]
- Strong, E.B. Endoscopic repair of anterior table frontal sinus fractures. Facial Plast Surg 2009, 25, 43–48. [Google Scholar] [CrossRef]
- Steiger, J.D.; Chiu, A.G.; Francis, D.O.; Palmer, J.N. Endoscopic-assisted reduction of anterior table frontal sinus fractures. Laryngoscope 2006, 116, 1978–1981. [Google Scholar] [CrossRef]
- Kellman, R.M. Endoscopy in craniomaxillofacial surgery. Facial Plast Surg 2009, 25, 1. [Google Scholar] [CrossRef]
- Hybels, R.L.; Newman, M.H. Posterior table fractures of the frontal sinus: I. An experimental study. Laryngoscope 1977, 87, 171–179. [Google Scholar] [CrossRef]
- Smith, T.L.; Han, J.K.; Loehrl, T.A.; Rhee, J.S. Endoscopic management of the frontal recess in frontal sinus fractures: a shift in the paradigm? Laryngoscope 2002, 112, 784–790. [Google Scholar] [CrossRef]
- Carter, K.B., Jr.; Poetker, D.M.; Rhee, J.S. Sinus preservation management for frontal sinus fractures in the endoscopic sinus surgery era: a systematic review. Craniomaxillofac Trauma Reconstr 2010, 3, 141–149. [Google Scholar] [CrossRef]
- Har-El, G. Endoscopic management of 108 sinus mucoceles. Laryngoscope 2001, 111, 2131–2134. [Google Scholar] [CrossRef] [PubMed]
- Sautter, N.B.; Citardi, M.J.; Perry, J.; Batra, P.S. Paranasal sinus mucoceles with skull-base and/or orbital erosion: is the endoscopic approach sufficient? Otolaryngol Head Neck Surg 2008, 139, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Woodworth, B.A.; Schlosser, R.J.; Palmer, J.N. Endoscopic repair of frontal sinus cerebrospinal fluid leaks. J Laryngol Otol 2005, 119, 709–713. [Google Scholar] [CrossRef] [PubMed]
- Jones, V.; Virgin, F.; Riley, K.; Woodworth, B. Changing paradigms in frontal sinus cerebrospinal fluid leak repair. Int Forum Allergy Rhinol 2012, 2, 227–232. [Google Scholar] [CrossRef]
- Chen, D.J.; Chen, C.T.; Chen, Y.R.; Feng, G.M. Endoscopically assisted repair of frontal sinus fracture. J Trauma 2003, 55, 378–382. [Google Scholar] [CrossRef]
- Hueman, K.; Eller, R. Reduction of anterior frontal sinus fracture involving the frontal outflow tract using balloon sinuplasty. Otolaryngol Head Neck Surg 2008, 139, 170–171. [Google Scholar] [CrossRef]
- Chaaban, M.R.; Conger, B.; Riley, K.O.; Woodworth, B.A. Transnasal endoscopic repair of posterior table fractures. Otolaryngol Head Neck Surg 2012, 147, 1142–1147. [Google Scholar] [CrossRef]
© 2014 by the author. The Author(s) 2014.