Dog bite injuries are common and devastating with an annual incidence of 12.9 per 10,000 persons [
1]. Children are dispro- portionately affected compared with adults. It has been estimated that the likelihood of a child sustaining a dog bite in their lifetime is around 50% [
2] and approximately 80% of severe dog bites in children involve the head and neck [
3,
4]. Pediatric dog bites are increasingly recognized as a medi-cal and public health issue with obvious functional, aesthetic, and psychosocial consequences [
5]. Unfortunately, there is no standardized national reporting system for dog bites. This leads to inconsistent and often incomplete documentation of the details of each injury, particularly with regard to animal breed. The main objective of this study is to add to the existing medical literature regarding the epidemiologic characteris- tics of pediatric facial dog bites, with a particular emphasis on the breed of the offending dog.
Materials and Methods
A retrospective review of children with dog bites to the face was performed at the Children’s Hospital (Denver, CO), a large tertiary pediatric hospital, between 1 January 2003, and 31 December 2008. Approval from the Institutional, Review Board of the University of Colorado, Denver was obtained for this study. Patients with a diagnosis of dog bite were identi- fied by a search for medical records containing Code, E906.0 of the International, Classification of Diseases, Ninth, Revision, Clinical, Modification (ICD-9-CM). Each record was evaluated to identify children with bites to the face. Patients older than 18 years and who were bitten by animals other than dogs were excluded.
Data including patient demographics, animal breed and owner, circumstances surrounding the bites, and clinical course including need for hospital admission were recorded in an Excel spreadsheet. Families of those patients in whom the breed of dog was not documented were then contacted via telephone to obtain this information. A bite was classified as “provoked” if the child had been playing with, teasing, or feeding the dog at the time of the injury.
Data are reported with standard descriptive statistics such as raw numbers with percentages, or means standard deviation (SD) as appropriate. Independent sample t-tests were used to test for differences between groups for continu- ous variables. Chi square test of independence was used to test for differences in distributions of categorical variables. When cell counts were < 5, the Fisher’s exact test was used. A p-value of < 0.05 was considered significant.
Results
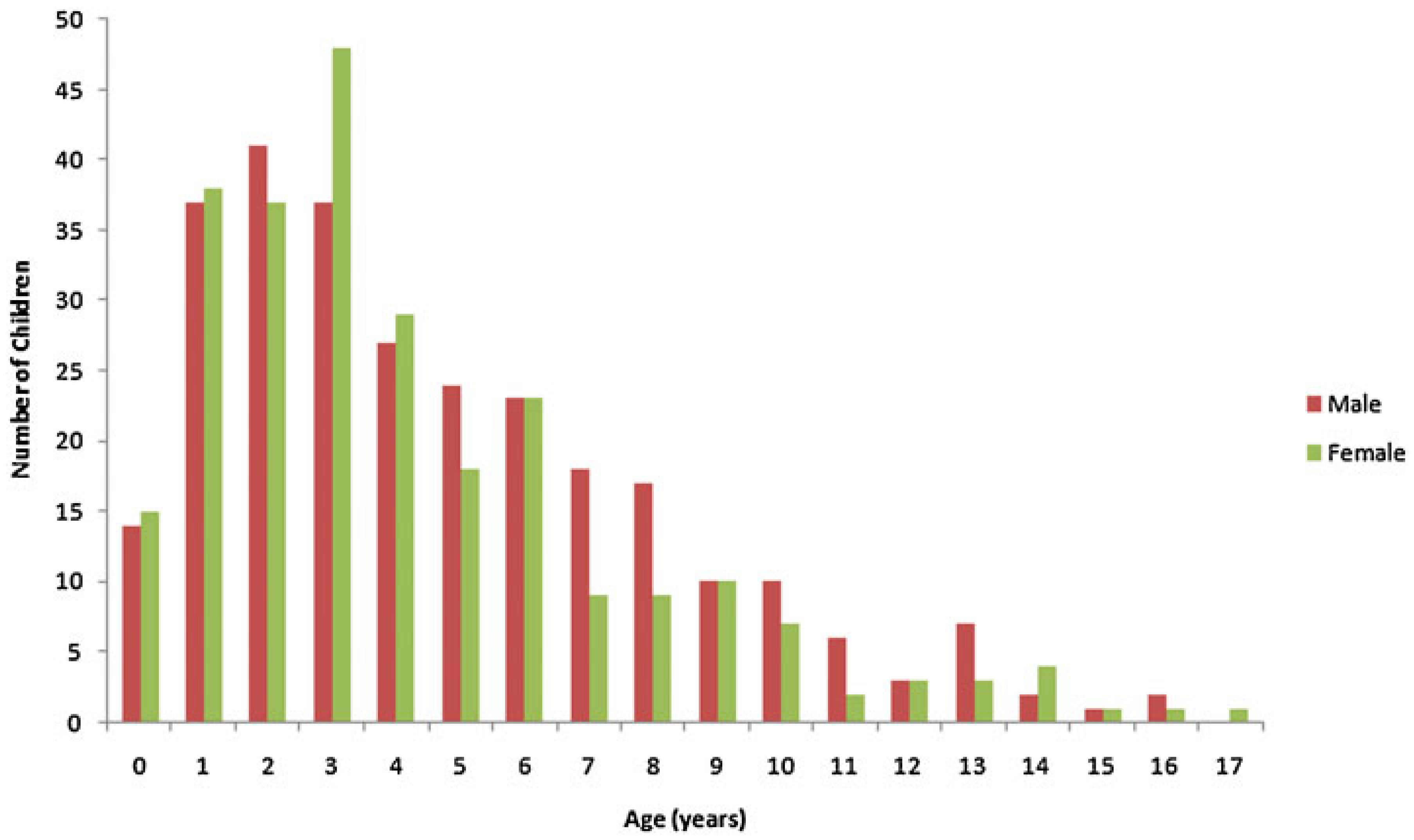
A total of 537 children were treated in the Children’s Hospital between January 1, 2003, and December 31, 2008, with dog bites to the face. This represents approximately 90 dog bite victims per year or one victim every 4 days. The mean age was 4.59 3.36 years (range, 0.5–17 years). There was a slight male preponderance (52.0%), but this was not statistically significant. The majority of dog bites occurred in children 5 years of age or younger (68.0%), with the highest incidence occurring in 3-year-olds (15.8%). Incidence decreased with increasing age (
Figure 1).
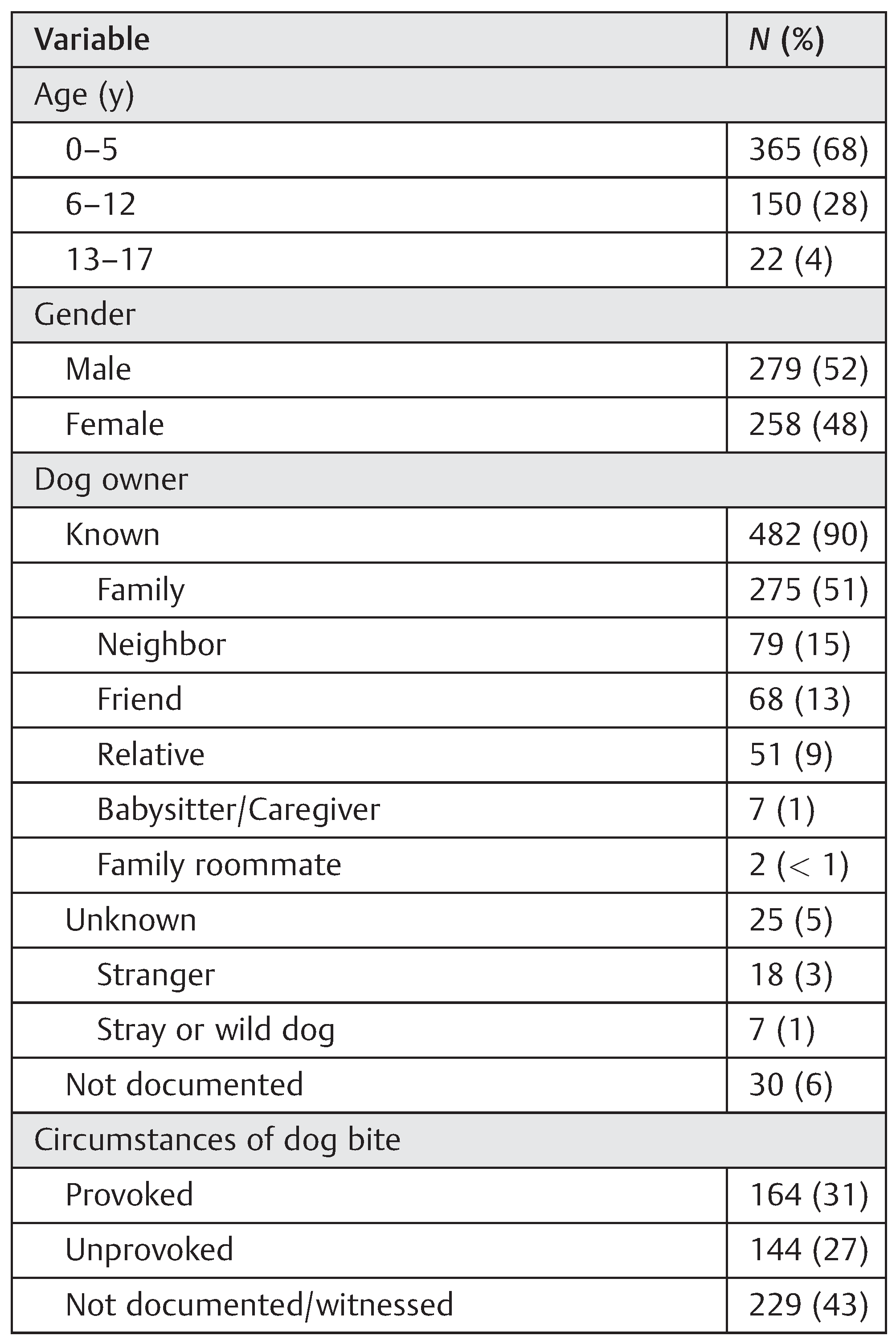
Almost all (89.8%) of the dogs were known to the children, either as the family pet (51.2%) or through a neighbor (14.7%), friend (12.7%), or relative (9.5%) (
Table 1). Among three age categories (0–5, 6–12, and 13–17 years), there was an associ-ation with age category and familiarity with the dog. Ado- lescents were more likely to be bitten by an unknown dog than younger children (
p = 0.0002), and younger children were more likely victims of known dogs (0–5 years,
p < 0.0001, 6–12 years,
p = 0.0018).
Of the 308 cases where there was documentation of the circumstances of the injury, more than half (53.2%) were provoked. Common provocations included the child playing with or petting the dog too aggressively, startling the dog, and falling or stepping on the dog. There was no association between familiarity with the dog and whether the attack was provoked or unprovoked (p = 0.9023). There was no difference in mean age among those attacks that were provoked (4.77 ± 3.36 years), unprovoked (4.69 ± 3.60 years), or unknown (4.41 ± 3.20 years) (p = 0.1643).
A total of 58 offending breeds were found in 366 (68.2%) cases in which this information was obtainable, either through the medical record or from telephone contact with the family (
Table 2). The most common were mixed breed (23.0%), followed by Labrador retriever (13.7%), Rott-weiler (4.9%), and German shepherd (4.4%). Of the mixed breeds, the most common partial breeds included Labrador retriever (20.2%), Chow (17.9%), and German shepherd (11.9%).
Table 1 Demographics and characteristics of attacks
Table 1.
Demographics and characteristics of attacks.
Table 1.
Demographics and characteristics of attacks.
Table 2.
Breeds of dogs involved in attacks.
Table 2.
Breeds of dogs involved in attacks.
Inpatient treatment was required in 121 (22.5%) patients because of severity of the dog bite injury requiring operative management or because of a wound infection requiring intravenous antibiotics and/or incision and drainage for a total of 358 days of inpatient care. The average length of stay was 2.96 2.77 days (range, 1–28 days). Children 5 years or younger were more likely to be hospitalized than older children. There were no fatalities from facial dog bites.
Discussion
Dog bite injuries present a significant public health problem, yet they are largely preventable. It is estimated that 45 to 65 million households own dogs [
6,
7]. According to the Centers for disease Control and Prevention, approximately 4.5 million people are bitten by dogs each year and of these, 885,000 require medical attention [
8]. Conservative annual estimates of the total cost of these injuries range from
$235 to 250 million [
9]. Because of their size and immaturity, children are much more likely to be bitten than adults [
1,
7].
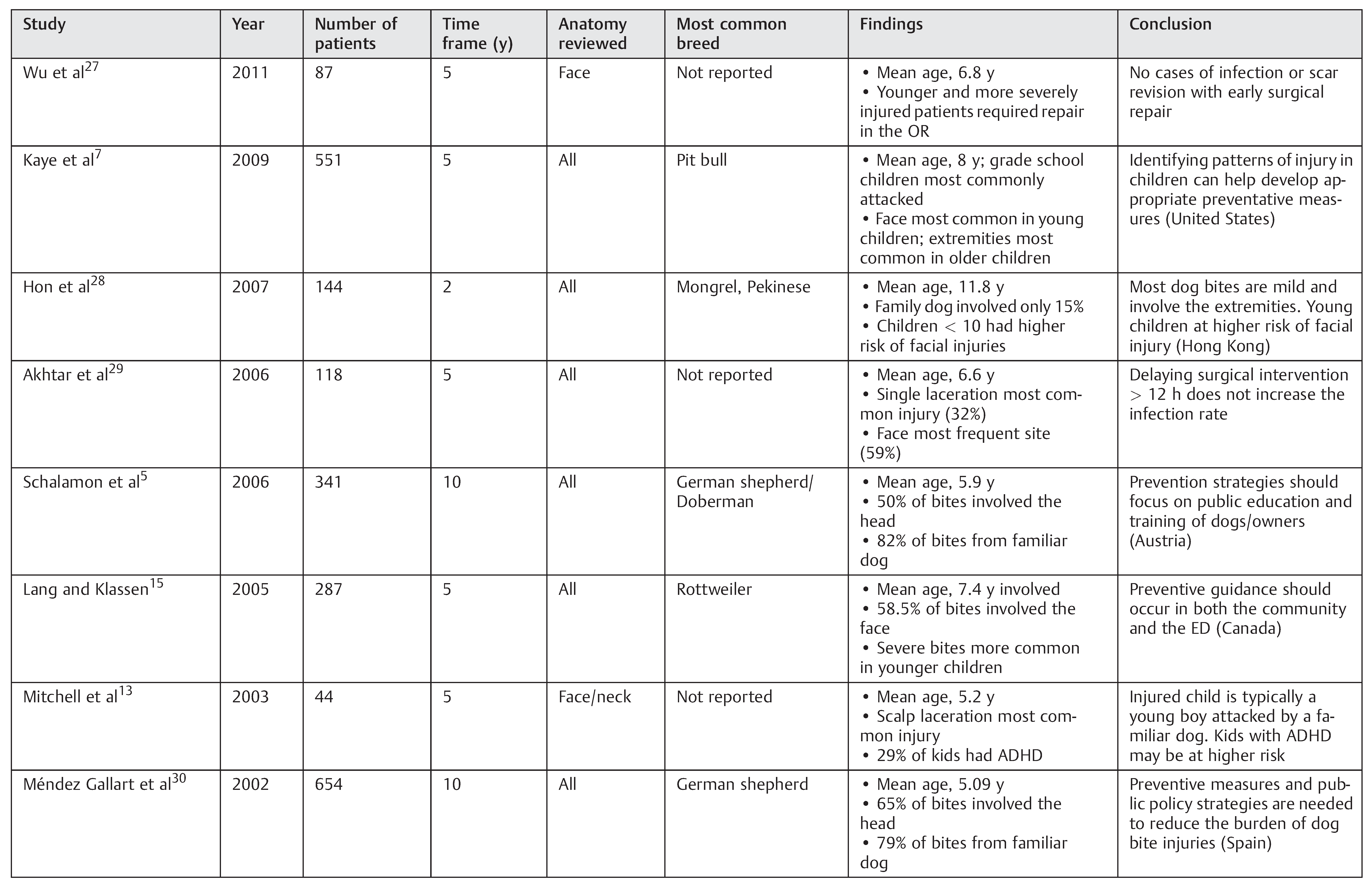
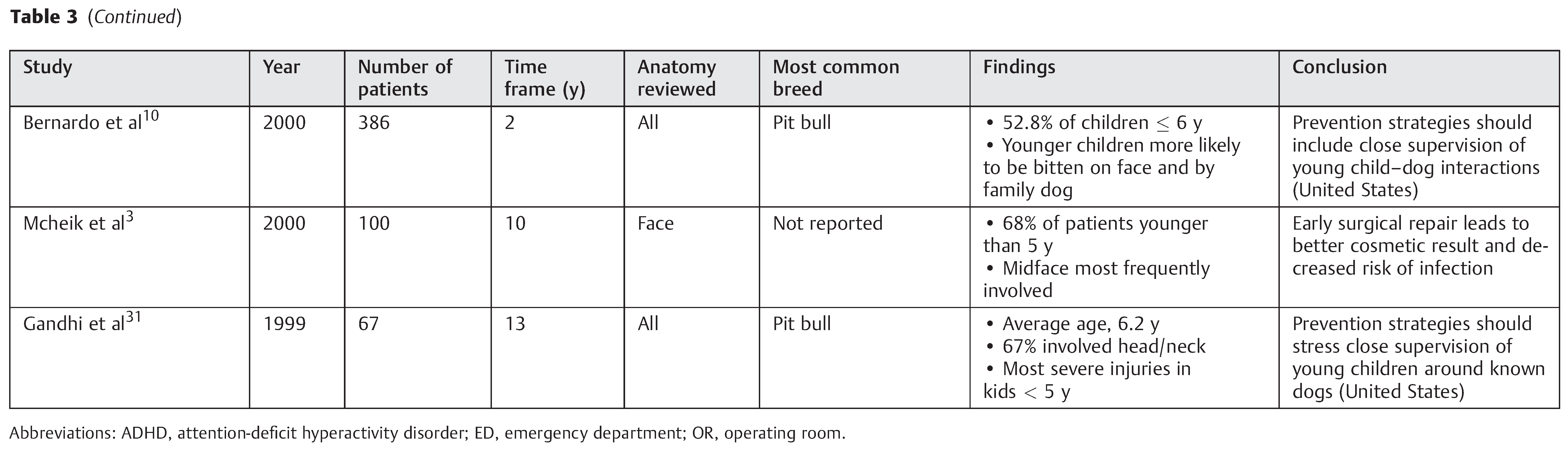
A search of the peer-reviewed medical literature reveals several retrospective studies analyzing pediatric dog bites.
Table 3 summarizes the pertinent studies in the past 15 years. There are several consistent findings among the studies. Children aged 5 through 9 years are at greatest risk of dog bites, and males are more commonly affected than females. The face and scalp are consistently reported as the most frequent location of injury, and younger children are more likely to have severe injuries. Pit bull terriers and German shepherds are the most common breeds involved in attacks, and the majority of bites documented in the literature occur from dogs familiar to the child. It is a universal conclusion that public education and preventive strategies are paramount to reducing pediatric dog bites.
We sought to examine our experience with pediatric facial dog bites in the hopes of further contributing to the existing knowledge surrounding these injuries. This study marks the largest and most extensive single-institution study to date regarding pediatric dog bites to the face.
The results of our study are mostly consistent with previ- ously reported data. The peak incidence of dog bite injuries is most commonly reported to occur between 5 and 9 years of age in studies that reviewed dog bites to the entire body [
1,
5,
6,
7,
10,
11]. We specifically looked at facial dog bites and found an overall younger population. The average age of patients in our study agrees with other published reports that focused on injuries of the head and neck [
3,
12,
13,
14]. Younger children are more prone to injuries to the face due to their smaller stature which is on the same level as dogs, their relatively large head size compared with their body, and their lack of understanding and fear of dogs leading them to bring their faces within an intimate and threatening distance from the dog [
3,
12]. Many authors have reported that males are more likely to suffer a dog bite [
10,
12] but like others [
8,
15] we found no gender difference.
The circumstances of the attack as well as the breed of the attacking dog are often incompletely documented in retro- spective studies. Through our telephone survey, we were able to obtain this information for more than 50% of our patients. Like previous reports, most victims in our study were bitten by a familiar dog [
5,
7,
10,
12,
13,
15]. Familiar dogs may be allowed more time with children and with less supervision, key circumstances that may precipitate attacks. Other reasons include modern media personification of dogs and the fact that increased comfort level with a dog may cause a child to get closer in its attempts to interact with the dog more like a person [
5,
7]. Of those bites where the circumstances were documented, more than half were provoked. This number may well be higher [
5], but unfortunately such details are often poorly documented in the medical record. Despite this, our data did not find an association between familiarity with the dog and whether the attack was provoked or not. Children appear to be bitten by familiar dogs simply because they are much more likely to be interacting with a familiar dog than an unfamiliar one. Unfortunately, familiarity with a dog does not protect against an attack. This suggests that behavioral strat- egies could prevent a large number of dog bites. In addition to the child’s interaction with the dog, other circumstances such as the breed and innate aggressiveness of the dog may play a role in whether a child is bitten.
Pit bulls, German shepherds, Rottweilers, and Dobermans have been implicated in the majority of dog bites [
5,
6,
7,
10,
11,
12,
13,
16]. However, the breed of dog is often not documented in a large percentage of cases of published studies leading to skewing of the data. We attempted to mitigate this by calling the families in which this information was not documented in the medical record. We were able to obtain breed information in almost 70% of our patients. Our data found that mixed breeds accounted for the most bites.
Of the pure breeds, Labrador retriever, Rottweiler, and German shepherd were the most common. In addition, Labrador retriever, Chow, and German shepherd were the most common breeds represented in the mixed breeds. While the accuracy of breed information is subject to recall bias in a retrospective study, almost 90% of the offending dogs were known to the patient. Thus, the accuracy of breed identifica- tion is expected to be high. What is clear from our data is that virtually any breed of dog can bite. The tendency of a dog to bite is related to heredity, early experience, later socialization and training, health (medical and behavioral), and victim behavior [
17].
In 1991, Gershman et al performed a case–control study in Denver and found that male, unneutered dogs that were of Chow, Chow or German shepherd breed were more likely to bite [
11]. No pit bull terriers were identified as a biting dog in this study, consistent with a ban of pit bulls in Denver, County that was passed in 1989. Since that time, this breed-specific legislation has been challenged and upheld by the Colorado, State Supreme, Court [
18]. Pit bulls were banned in Denver because of several gruesome maulings and fatalities that occurred between 1984 and 1989. Our study found 11 victims of pit bull bites from 2003 to 2008, including the patient who suffered the most extensive injuries and the longest hospital- ization of our entire population, indicating that despite legislation, pit bull bites continue to be a public health concern.
The burden of facial dog bite injuries is massive, from financial costs to emotional and psychological tolls. Conser- vative annual estimates of the total cost of dog bite injuries range from
$235 to 250 million [
9]. Of this, an estimated
$62.5 million is spent on hospital admissions. Much harder to calculate is the emotional distress victims and families must deal with afterward. The number of unreported cases of emotional distress likely is much higher than reported and the need for early psychological support in victims is underestimated [
5,
19].
Like many authors before us, we fully support prevention strategies to minimize the incidence of pediatric dog bites [
5,
10,
12,
15,
20,
21,
22,
23,
24]. Tantamount to this is providing education to parents, children, and the community. In addition, dogs need appropriate behavioral training. It is clear that children will most likely be the victims of a bite from a dog familiar to them, often their own dog. The impetus is on parents to recognize aggressive breeds as well as behaviors and never allow their young children to be left unsupervised around any dog.
Weaknesses of our study relate to its retrospective nature and the fact that tracking and complete reporting of dog bites remains extremely problematic. There is no standardized national reporting system for dog bites. As such, data on offending dog age, sex, weight, and immunization and neuter status were not routinely documented in the medical records of our patients. Neither was the time from time of injury to presentation to the emergency department. Dog breed, own- er, and the circumstances surrounding the incident were more frequently documented, but this information was still incomplete. Despite contacting families directly, we were still not able to obtain breed information for a third of our patients. The data collected through telephone interviews are self-reported and unvalidated and are subject to recall bias.
While we were able to obtain a large population dataset, it is hard to generalize our findings to the entire population. The local distribution of dogs varies from city to city, and dog registries are uncommon. It is possible that Labrador re- trievers, not commonly viewed as aggressive in previous studies, were highly implicated in our study because they are the most popular dogs in the United, States and Denver [
25]. Further, less than 50% of dog bites are reported to physi- cians [
26], and bites that result in no injury or only minor injuries may have been missed because they never sought medical attention. This would have underestimated the total number of victims and skewed the data toward more serious injuries.
Table 3.
Summary of pediatric dog bite studies in the peer-reviewed literature, past 15 years.
Table 3.
Summary of pediatric dog bite studies in the peer-reviewed literature, past 15 years.

{kind=link}