Abstract
Oblique facial clefts are rare congenital anomalies that can present alone or in association with other craniofacial anomalies. A high degree of clefting in the embryo may lead to hyperdontia secondary to dichotomy of the dental lamina. Multiple facial clefts with hyperdontia are clinically challenging and demand comprehensive rehabilitation. This article reports a case of multiple oblique facial clefts of variable severity with multiple supernumerary teeth in a 12-year-old boy. The varied clinical presentation along with the rarity of the occurrence mandate documentation.
Oblique facial clefts are relatively rare conditions that exist in a multitude of patterns and varying severity. Often the soft tissue clefts do not correspond in their anatomy and severity with the hard tissue clefts. Moreover, soft tissue clefts medial to the infraorbital foramen are more destructive than their hard tissue counterparts whereas the hard tissue ones are more aggressive lateral to the foramen [1,2,3]. Dentoalveolar complex involvement occurs eventually in all the southbound Tessier facial clefts, disrupting the harmony of the dental occlusion and demanding a comprehensive rehabilitation. This article reports a rare case of multiple bilateral oblique facial clefts with 14 impacted and five erupted supernumerary teeth.
Case Report
A 12-year-old boy from consanguineous parents presented to us with a furrow and scar in the region of left commissure. Examination revealed an incomplete oblique facial cleft ex- tending across the face toward the left lateral canthus of the eye and an antimongoloid slant of the left palpebral fissure. This was associated with flattening of the left temporal fossa. Features of macrostomia suggested an incomplete soft tissue cleft, Tessier 7 on the right side and Tessier 6 on the left (Figure 1). Intraorally the patient presented with the following features: five clinically erupted and transpositioned super- numerary molars in the upper left quadrant (Figure 2); bony cleft in the right maxillary alveolus posterior to the first molar, with sequestered bone and impacted tooth germs (Figure 2 and Figure 3); and bone cleft in the left maxillary alveolus between the first and the second molar (Figure 4).
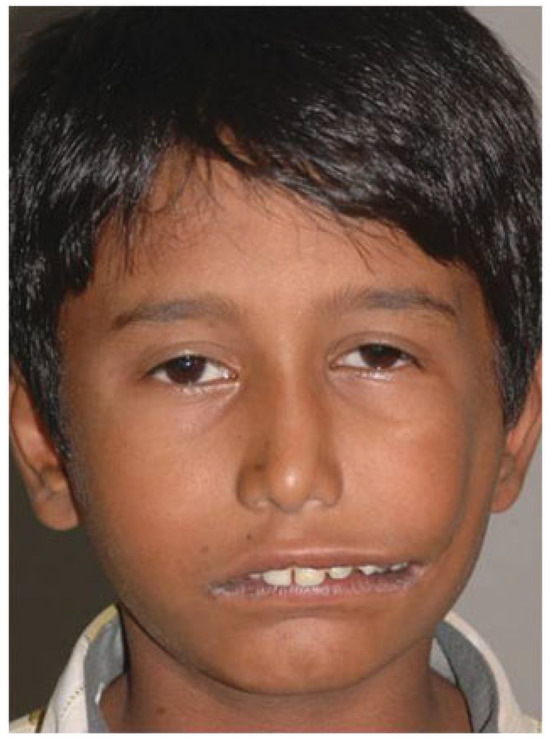
Figure 1.
Frontal profile showing the soft tissue Tessier 5 facial cleft on the left side and an incomplete soft tissue Tessier 7 facial cleft on the right side.

Figure 2.
Multiple supernumerary teeth in the second quadrant.

Figure 3.
(A) Tessier 7 bony cleft of the right maxilla (arrow). (B) Intraoperative exposure of the bony mass (arrow). (C) The excised sequestered bone mass with multiple tooth buds.

Figure 4.
Cleft alveolus in the left maxilla between the molars.
A clinical diagnosis of the following was made:
- Incomplete Tessier 7 soft tissue facial cleft and a complete skeletal Tessier 7 cleft on the right side
- Incomplete Tessier 5 skeletal and soft tissue Tessier 6 facial cleft on the left side
An orthopantomograph confirmed the position of the bone clefts (Figure 5) and also showed multiple impacted supernumerary teeth: four in the upper left quadrant apart from five clinically erupted molars and another 10 impacted tooth germs in the upper right quadrant (five in the cleft segment and five in the alveolus), for a total of 14 impacted tooth germs in the maxilla.

Figure 5.
Orthopantomograph showing the cleft alveolus on the right side (line arrow) and the posterior maxillary cleft Tessier 7 on the left side (dashed arrow).
The 3D CT revealed a distinct Tessier 7 skeletal cleft on the right side extending posterior to the first molar tooth across the maxillary tuberosity (Figure 6) like a sequestrated segment and a Tessier 5 bony cleft on the left side with a moderate degree of bony deficiency at the cleft site (Figure 7).
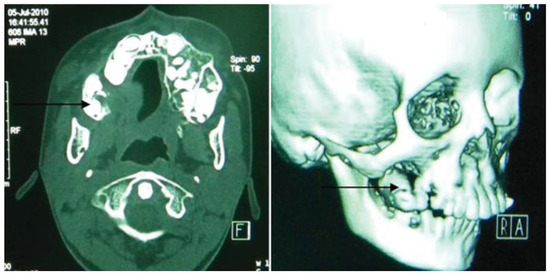
Figure 6.
Tessier 7 bone cleft as a sequestered mass in the right maxilla.
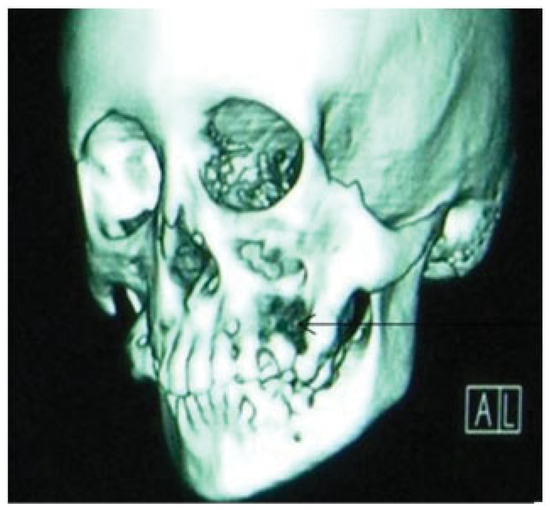
Figure 7.
Cleft in the left maxillary alveolus.
An orthodontic opinion was sought for possible extraction of unwanted erupted teeth and retention of necessary molars on the left side. The orthodontic team suggested the removal of the sequestrated bone segment on the right side to facilitate the eruption of the impacted molars along with the surgical removal of all other unwanted impacted teeth (Figure 8, Figure 9 and Figure 10). The surgical plan was bilateral commissuroplasty followed by second-stage secondary alveolar bone grafting (SABG) during orthodontic treatment, then wait for the patient to complete growth for further craniofacial management if necessary.

Figure 8.
Maxillary dental arch after sequestrectomy and prior to alveolar bone grafting.
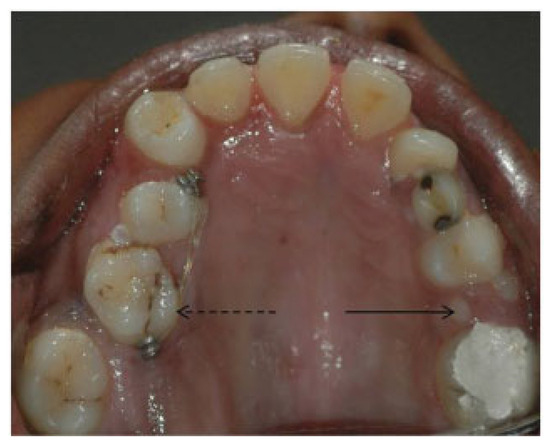
Figure 9.
Maxillary arch after alveolar bone grafting; second premolar can be seen erupting through the graft site in the second quadrant (line arrow); started with the first stage of orthodontic treatment (dashed arrow).

Figure 10.
Postoperative 3D computed tomography scan.
Discussion
Oblique facial clefts are rare congenital defects with an incidence of 1.43 to 4.85 per 100,000 live births (Figure 11) [2]. These could occur as primary transformation defects (the true clefts) or as differentiation defects [4].
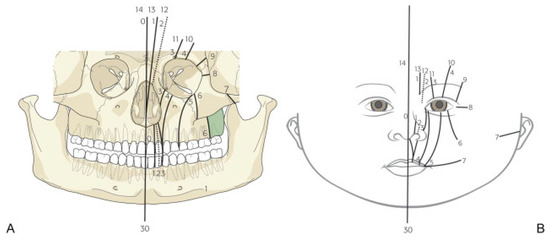
Figure 11.
(A,B) Tessier classification of craniofacial clefts.
Disruption of the stapedial artery blood supply with secondary hypoxia,2 disruption of amniotic membrane complex [5,6,7], and subtle genetic mutations have all been implicated as possible causes for severe facial clefting during embryogenesis.
The presence of a high degree of clefting in the embryo can lead to hyperdontia, which has a reported incidence of 14.6% [8,9]. This has been attributed to the dichotomy of the primary and the successional dental lamina or the tooth buds at the stage of histodifferentiation during the sixth week of the fetal life [8,9]. Hyperdontia can lead to discrepancy in the Bolton’s arch perimeter resulting in severe crowding and malpositioning, which warrants extraction of the supernumerary teeth followed by a rigorous orthodontic treatment. Soft tissue repair procedures include multiple Z-plasties and advancement cheek flaps [2,4,5]. Bauer’s and modified Bauer’s W-plasty [10] can be used for the correction of incomplete Tessier 7 cleft. Bone grafting the cleft alveolus followed by grafting of the facial cleft prior to the tooth movement becomes essential.
We believe in addressing the primary soft tissue defects prior to the bony component to avoid psychological trauma to the child and also to prevent damage to the vital structures (eye). Skeletal anomalies can be addressed at regular intervals as dictated by the facial growth kinetics.
Acknowledgments
Funding: Cleft Children International; Zurich Switzerland. Competing interests: None declared.
References
- Schlenker, J.D.; Ricketson, G.; Lynch, J.B. Classification of oblique facial clefts with Microopthalmia. Plast. Reconstr. Surg. 1979, 63, 680–688. [Google Scholar] [CrossRef] [PubMed]
- van der Meulen, J.C.H. Oblique facial clefts: Pathology, etiology, and reconstruction. Plast. Reconstr. Surg. 1985, 76, 212–224. [Google Scholar] [CrossRef] [PubMed]
- Tessier, P. Anatomical classification facial, cranio-facial and latero- facial clefts. J. Maxillofac. Surg. 1976, 4, 69–92. [Google Scholar] [CrossRef] [PubMed]
- van der Meulen, J.C.; Mazzola, R.; Vermey-Keers, C.; Stricker, M.; Raphael, B. A morphogenetic classification of craniofacial malformations. Plast. Reconstr. Surg. 1983, 71, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Rowsell, A.R. The amniotic band disruption complex. The pathogenesis of oblique facial clefts; an experimental study in the foetal rat. Br. J. Plast. Surg. 1989, 42, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Mayou, B.J.; Fenton, O.M. Oblique facial clefts caused by amniotic bands. Plast. Reconstr. Surg. 1981, 68, 675–681. [Google Scholar] [CrossRef] [PubMed]
- Coady, M.S.; Moore, M.H.; Wallis, K. Amniotic band syndrome: The association between rare facial clefts and limb ring constrictions. Plast. Reconstr. Surg. 1998, 101, 640–649. [Google Scholar] [CrossRef]
- Tereza, G.P.; Carrara, C.F.; Costa, B. Tooth abnormalities of number and position in the permanent dentition of patients with complete bilateral cleft lip and palate. Cleft Palate Craniofac J. 2010, 47, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Bernardes da Silva, P.R.; Costa, B.; de Carvalho Carrara, C.F. Dental anomalies of number and position in permanent dentition of patients with bilateral cleft lip: Radiographic study. Cleft Palate Craniofac J. 2008, 45, 473–476. [Google Scholar] [CrossRef] [PubMed]
- Parameswaran, A.; Ramanathan, M.; Thomas, T.K. Surgical management of lateral facial clefts —A modified W-plasty technique. Asia J. Oral. Maxillofac. Surg. 2007, 19, 150–154. [Google Scholar] [CrossRef]
© 2008 by the author. The Author(s) 2008.