Unicoronal craniosynostosis can cause cranial deformity and several types of facial asymmetry. Unilateral coronal craniosynostosis is phenotypically characterized by a flattened supraorbital rim and frontal bone on the affected side. Dysmorphology in unilateral coronal synostosis has also been recognized clinically [
1]. Unilateral coronal synostosis can cause frontal plagiocephaly and occipital plagiocephaly. Simultaneous correction of frontal and occipital plagiocephaly has therefore been by total cranial vault surgery with barrel osteotomy, which tends to cause various dangerous complications [
2]. ‘‘Occipitofrontal switching’’ is a technique that replaces the affected hemifrontal triangular bone with a contralateral hemioccipital triangular bone for simultaneous correction of anterior and posterior plagiocephaly. To date, plagiocephaly has been corrected by fronto-orbital bar advancement or frontal bone advancement/rotation. For unicoronal synostosis, making a complete symmetrical curvature for the frontal bone is thought to be very difficult due to the flatness of the affected sides. Craniosynostosis may cause brain retardation and aesthetic problems (e.g., potential facial asymmetry), which is why surgery is indicated for unilateral coronal craniosynostosis. Without surgery, synostosis tends to cause severe types of facial deformity [
3,
4,
5]. Because our patient had posterior plagiocephaly, bones of optimal curvature were obtained from the bulging occipital area to relieve this area and then were used to reconstruct frontal flatness. We therefore tested if 3-D model-based preoperative surgery may make simultaneous correction of frontal and occipital plagiocephaly clinically effective and quicker.
Patients and Methods
Preoperative Planning
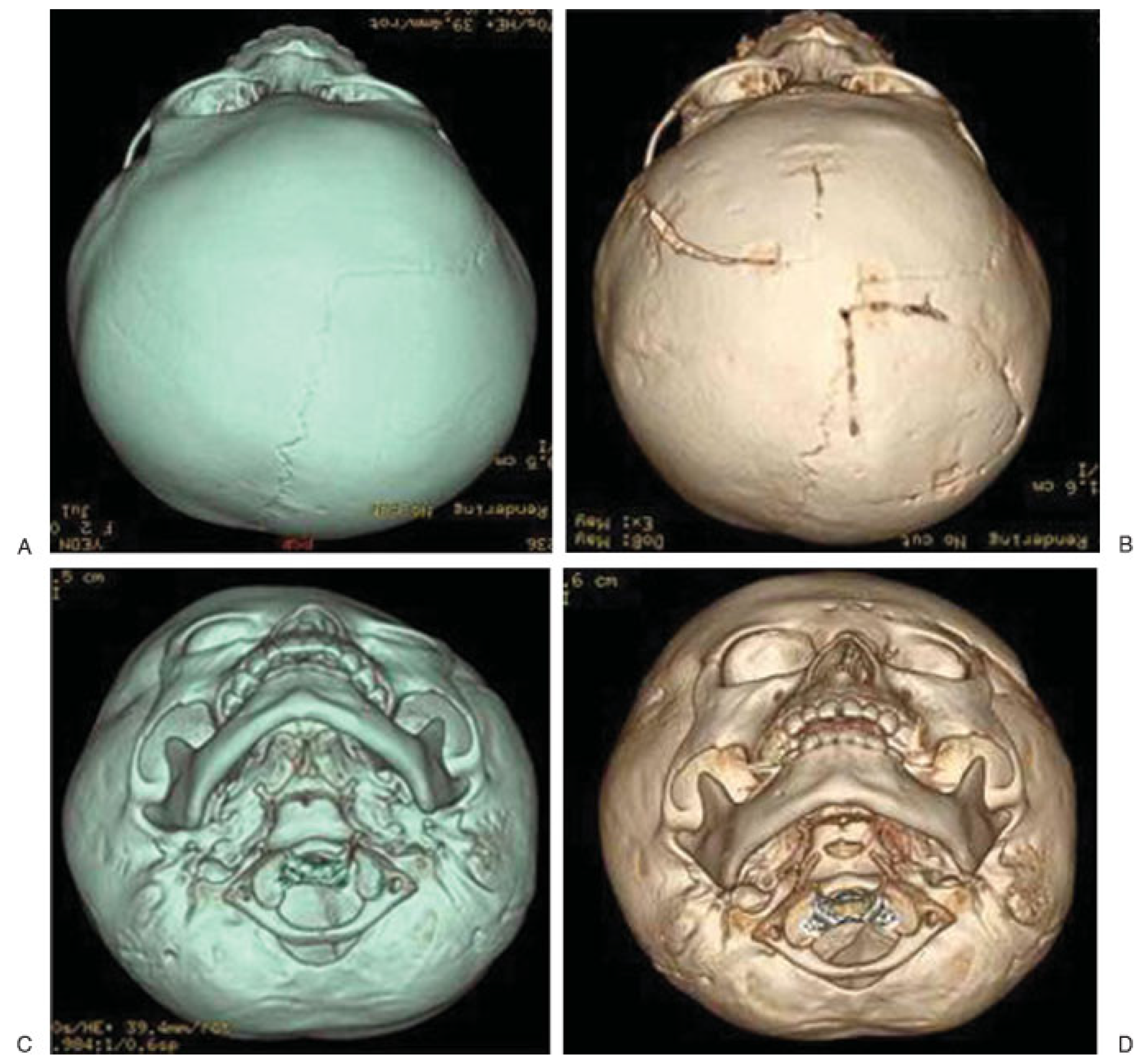
A 2-year-old girl suffering from unilateral forehead flattening visited our Dentofacial Clinic. She was diagnosed with left-sided unilateral coronal synostosis based upon physical examination (
Figure 1A) and 3-D computed tomography (CT) (
Figure 1B). Neither jaw deformity nor definite high intracranial pressure was noted on CT. She also displayed an abnormal bulge on the right occipital side (
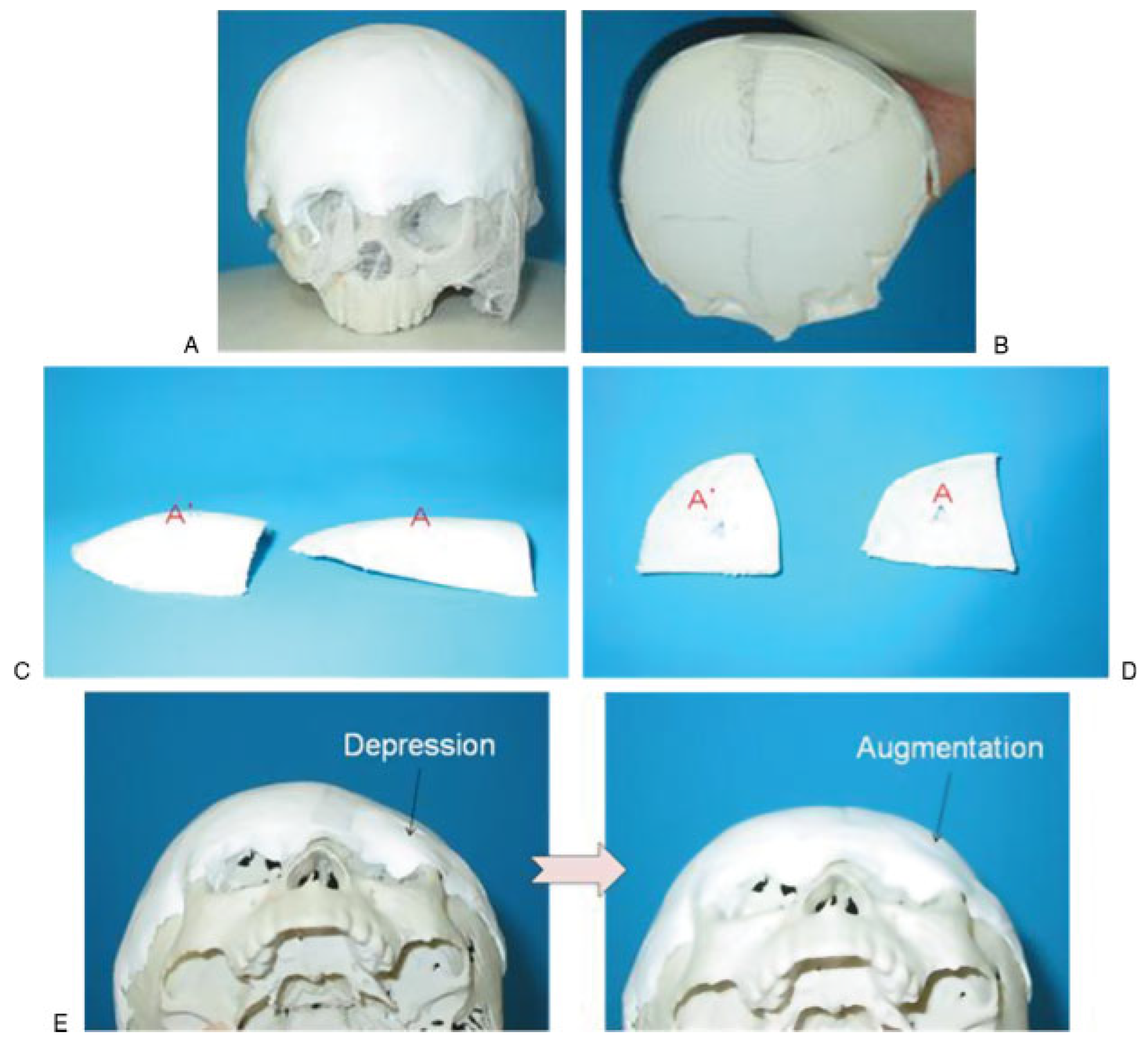
Figure 1C,D). A 3-D whole-skull plaster model was produced for preoperative planning and virtual simulation surgery. White-colored clay was applied to a rapid prototype (RP) model for multiple simulation surgery before delicate single surgery on the RP model. Malleable wire and frontal triangular white-colored clay were used to detect the optimal curvature from the opposite occipital bulging side. This was needed to obtain symmetrical frontal correction. Occipital triangular clay with curvature similar to that of the affected frontal bone was harvested and transferred to the flat site of the frontal bone using adhesive tapes (
Figure 2). The RP model was used for real virtual surgery because the preplanned surgery showed nearly symmetric correction (
Figure 3A). Measurement of donor sites and recipient sites was recorded for delicate occipitofrontal switching, after which the patient underwent surgery (
Figure 3B).
Surgical Technique
A coronal incision was made to expose frontal diseased and occipital donor parts of the plagiocephalic skull. To make the fronto-orbital bar correction, the frontal scalp flap was dissected up to the top of the nasal bone while preserving the supraorbital and supratrochlear nerves. Before harvesting triangular bones and the fronto-orbital bar, all measured numbers and distances obtained from preplanned surgery were transferred to her real skull (
Figure 4A). The left-sided frontal diseased area was then obtained for reconstructing the fronto-orbital bar. After harvesting both triangular bones, two curvatures were noticed (
Figure 4B). Fronto-orbital reconstruction was initially performed using malleable wire by mirror image techniques (
Figure 4C). The malleable plate template was also used to get optimal curvature from the healthy frontal side, turned over to the affected orbital rim, and then fixed with a frontal orbital bar that was reconstructed with three pieces. Occipitofrontal switching was also performed using resorbable plates and screws. The affected frontal bone was placed on the donor area of the occipital side, resulting in overall symmetry in flatness in frontal and occipital sides (
Figure 4D). Extreme care was used when drilling for screw placement to avoid injury to brain parenchyma.
The coronal incision was sutured back with polydioxanone suture (PDS) 4–0 and 2-octylcyanoacrylate (Dermabond, ® Ethicon, West Somerville, NJ) for skin approximation. The patient was brought to the intensive care unit to monitor for epidural hematoma or high intracranial pressure.
Results
Optimal curvature for the affected area was predicted by virtual surgery using an RP model and clay works, which served to minimize error. Each of the three sides of the triangular bone was fixed with resorbable plates and screws. The patient’s parents were satisfied with the cosmetic appearance. Postoperative CT findings at 6 months showed no displacement of the two triangle bones and almost completely healed bones (
Figure 5B). Postoperative imaging also showed corrected forehead depression, symmetrical forehead shape, and symmetrical eyebrow position (
Figure 5D), as compared with preoperative imaging (
Figure 5C).
Discussion
The occipital triangle bone was initially harvested. The frontal bone was then harvested to reduce the difference in the gap between frontal and occipital harvests. The only factor we did not consider was the location of the occipital sinus. To lessen occipital sinus injury, we should have moved our predicted design 4 cm laterally so that the final curvature was relatively flatter than expected. Nevertheless, the outcome was acceptable.
There is a report that cranial vault asymmetry improves in surgical cases as compared with nonsurgical cases [
6]. If synostotic anterior and posterior plagiocephaly were treated simultaneously, the risk of complications resulting from remodeling the entire cranial vault would have increased. Anterior and posterior diseased sites should be corrected with minimal donor morbidity. This was why we treated the two affected areas simultaneously and ‘‘switched’’ them with each other. The main purpose was to obtain maximal effect from minimal surgery. Various techniques of plagiocephaly correction have been described, such as unilateral/bilateral frontal bone monoblock advancement, supraorbital rim advancement, or distraction osteogenesis using the same procedures [
7,
8]. Making an optimal and symmetrical curvature with the healthy sides is difficult. If patients with unilateral coronal synostosis reach adulthood, upper facial asymmetry may cause midand lower-facial asymmetry and problems with the temporomandibular joint [
3,
5,
9,
10]. These deformities tend to improve with correction of unilateral craniosynostosis [
1].
In the real surgery, we prepared a sterilized polyvinyl bag for the 3-D model of the skull to confirm the design and bone measurement. We observed some discrepancy in occipital and frontal thickness between the RP model and real human skull. The thickness of clay is thinner than that of real cranial bone. Clay has less curvature due to its application on the skull, which may cause an error in thickness measurement for simulation surgery. When the occipital triangle was harvested from the RP model, a measurement error attributable to incongruous curvature between occipital and frontal curvatures may have resulted. Facial asymmetry is one of the main concerns of patients with unilateral coronal synostosis. Upper-facial asymmetry may affect midand lower-facial symmetry [
4].
This is the first report describing an occipitofrontal switching technique for correction of unilateral coronal craniosynostosis. Most articles describe frontal bar advancement, frontal bone advancement/rotation, or distraction osteogenesis, which requires several types of minor touches to create symmetrical forehead shape [
5]. We consider these techniques to be related to advancement of the flat frontal bone instead of achieving symmetrical curvature with the curvature of the other side. Simultaneous correction of frontal and occipital plagiocephaly is achieved by total cranial vault surgery with barrel strip craniectomy. Our switching technique of triangle cranial bones was effective for simultaneously correcting frontal and occipital plagiocephaly. Even with this short-term success in correction, long-term evaluation is needed to observe skull growth and bone graft reabsorption because this is a ‘‘free’’ bone graft instead of a ‘‘vascularized’’ bone graft.
Conclusion
Our technique for simultaneous correction cannot be applied to all types of plagiocephaly, but we can draw some conclusions from this study: (1) the RP model and clay replica method can make real surgery predictable and less time-consuming; (2) the occipitofrontal switching technique enables the surgeon to simultaneously correct frontal and occipital plagiocephaly; and (3) an exact preoperative evaluation and a simulation surgery permit predictable and safe surgery, which likely leads to fewer chances of error for the ultimate goals of plagiocephaly correction.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}