Background
Facial fractures are a common reason for presentation to emergency departments (ED) across the globe, accounting for over 400,000 yearly ED visits in the United States alone. [
1] This category of injury consists of trauma to facial structures including the maxilla, mandible, zygoma, and orbit, and can result in patients experiencing significant pain and dysfunction. Facial fractures present as the result of a variety of etiologies, including falls, assaults, and other accidents, and this pathology frequently requires surgical treatment as standard of care. [
2,
3,
4,
5,
6]
Medical comorbidities such as diabetes, vascular disease, and substance use disorders predispose patients to poor post-surgical outcomes, a pattern which holds true for the treatment of facial fractures. [
7] For example, diabetes affects an increasingly large number of Americans, and creates a suboptimal wound healing environment as it impairs appropriate neovascularization and fracture union. [
8] Another significant contributor to morbidity in facial fractures is concomitant smoking, which has been shown to delay wound healing and impair the body’s ability to alleviate oxidative stress [
9,
10] Furthermore, across many surgical specialties, post-operative metrics have been shown to be worse in tobacco users, predisposing these patients to higher risk of infection, poorer local wound healing, and elevated readmission rates. [
11,
12,
13,
14,
15] Thus, comorbidities in the context of facial fractures represent an important avenue for investigation in regards to their influence on post-operative outcomes.
Despite the wealth of literature surrounding the topic of facial fractures and subsequent surgical repair, there exists a gap in the literature exploring general post-operative complications and their relationship to pre-operative comorbidities. It is critical that surgical outcomes of facial fractures are characterized in order to provide clinicians with accurate information and improve their ability to counsel patients. Thus, the purpose of our study is to leverage data from a United States national surgical database to describe general post-operative complications in this cohort. Further, we will examine this data to shed light on patient characteristics which may predispose them to experiencing increased rates of 30-day post-operative complications. We hypothesize that certain comorbidities, such as diabetes, will be associated with higher complication rates.
Materials and Methods
Study Design
We performed a retrospective cohort analysis of the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database between January 1, 2015 and December 31, 2019. This database captures surgical information from over 600 hospitals throughout the United States, collecting data from the pre-operative period to 30 days post-operatively. IRB approval was not required at our institution for this deidentified, population-based, retrospective descriptive study. All patients included in this study sample must have (a) been ≥ 18 years old and (b) underwent surgical repair of a facial fracture during the study period by a plastic surgeon or otolaryngologist. Facial fractures were identified via the following Current Procedural Terminology (CPT) codes for Mandibular fractures (21453, 21461, 21462, 21465, 21470), Zygomaticomaxil-lary Complex (ZMC) fractures (21355, 21356, 21360, 21365, 21366), Orbital fractures (21385, 21386, 21390, 21395, 21406, 21407, 21408), and Lefort fractures (21421, 21422, 21423, 21345, 21346, 21347, 21348, 21154, 21155, 21156, 21157, 21158, 21159, 21160). Patients were excluded from this study if they were (a) younger than 18 years old, (b) did not undergo surgical fixation of a facial fracture during the study period, and (c) did not have data on pre-operative comorbidities.
Study Sample
The NSQIP dataset is a risk-adjusted, non-administrative, surgical-outcomes database that collects 30-day postoperative patient outcomes data. [
16] The study population included patients captured by the NSQIP who underwent facial fracture repair. The predictor variables included gender, elective vs emergent surgery, diabetes status, and smoking status. The primary outcomes and response variables included overall incidence of 30-day post-surgical complications (superficial skin and soft tissue infection (SSI), deep SSI, organ space infection, wound disruption, and reoperation rate). Other variables of interest included subcategory analysis by complication type, type of surgery, and incidence of reoperation.
Surgical site infections were classified as either superficial, deep, or organ space infections occurring within 30 days of operation. Superficial SSIs included any wound involving only the skin and subcutaneous tissue that had at least one of the following: diagnosis of a superficial SSI, purulent drainage, isolated organisms from fluid, or superficial incision opened by the surgeon that had pain, swelling, redness, and heat. Deep SSIs included any wound involving tissue below the skin and subcutaneous fat that had one of the following: purulent drainage, abscess, or diagnosis by the surgeon. Lastly, organ space infection, in the context of facial fractures, relates to osteomyelitis of the bones of the face.
Data Collection
The NSQIP dataset is collected by certified surgical clinical reviewers (SCRs) who collect over 250 clinical variables, including pre-operative risk factors, intraoperative variables, 30-day post-operative mortality, and 30-day postoperative morbidity from participating sites. [
16] The quality of data abstraction is maintained by mandates for SCRs to complete standardized online training modules, followed by a yearly certification exam focused on various aspects and processes of the program including instructions on coding and perioperative procedural definitions. They are also given access to an online decision support system that shares specialized resources and enables individualized, case-based troubleshooting. Each surgical procedure is assigned a primary post-operative diagnosis using
International Classifi
cation of Diseases codes (ICD) and a primary surgical procedure code using
Current Procedural Terminology codes (CPT). NSQIP utilizes a systematic, risk-weighted sampling strategy to minimize bias and ensure data quality. It routinely audits participating hospitals and SCR’s to ensure inter-rater reliability which have demonstrated disagreement rates of less than 2.5% for all assessed program variables. [
16]
Data Analysis
Descriptive statistics were reported as a frequency and percentage for categorical variables. To associate patient characteristics with post-operative outcomes, we calculated significance using Fisher’s exact and chi-squared tests. Statistical significance was defined with a P-value < .05. All statistical analyses were performed using commercially available software (JMP 13, SAS, Inc.; Cary, NC, USA).
Results
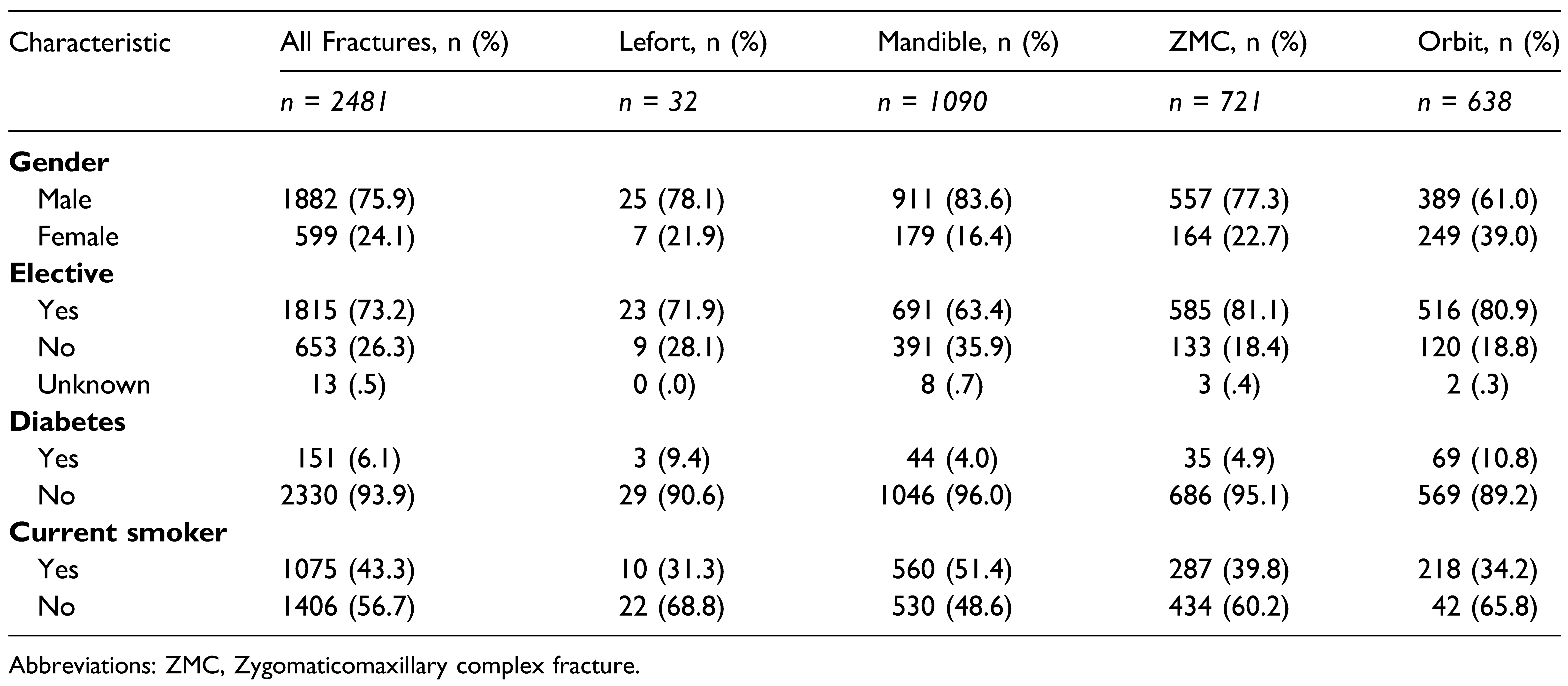
In total, 2481 patients met the primary outcome of facial fracture as specified above. This cohort was 75.9% male (1882/2481), and 73.2% (1815/2481) of corrective surgeries were performed as elective procedures following the initial trauma (
Table 1). Among the four different fracture types assessed, 1090 fractures (43.9%) were mandibular, 721 were zygomatic (29.1%), 638 were orbital (25.7%), and 32 (1.3%) were Lefort. Of the entire cohort, 1075 patients (43.3%) endorsed being current smokers, and (6.1%) had diabetes. These fractures were surgically managed in similar frequency by plastic surgery and otolaryngology providers.
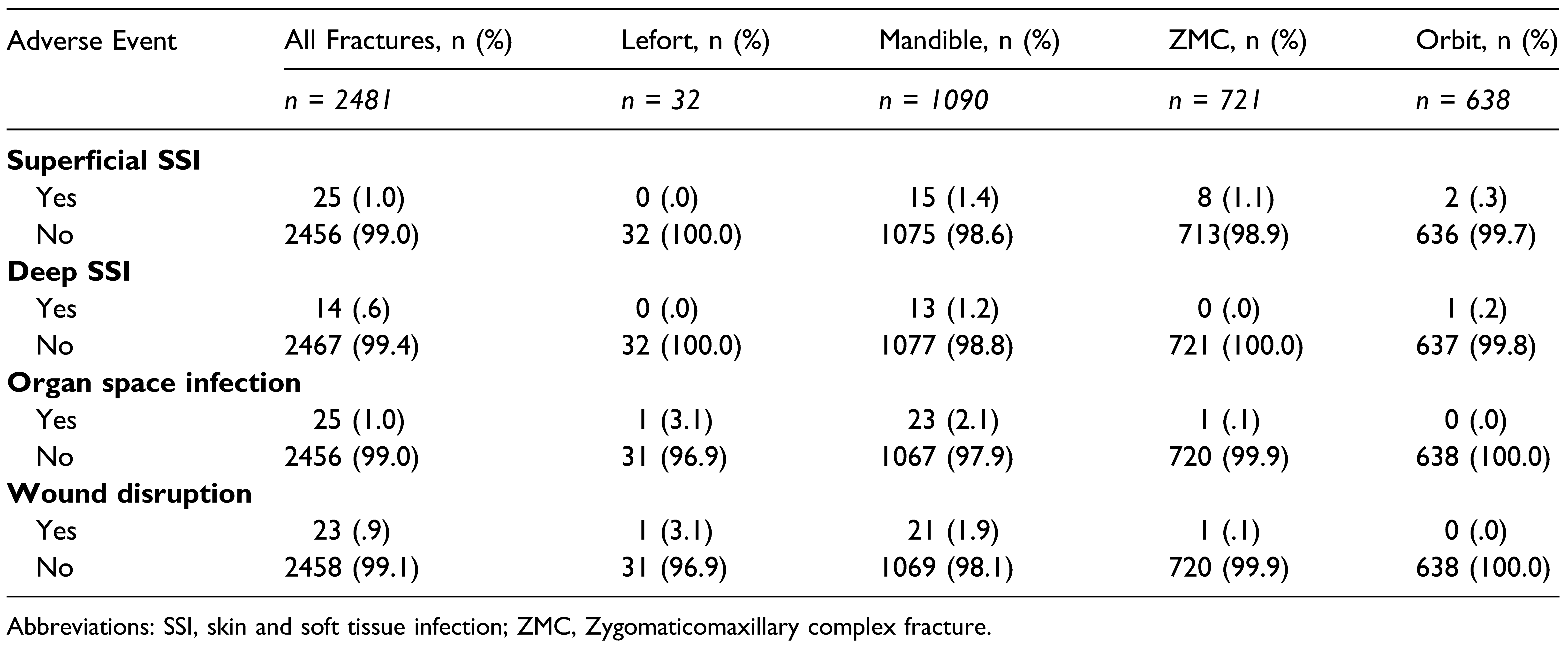
Adverse outcomes at 30 days post-surgery were characterized into four groups: superficial SSI, deep SSI, organ space infection, and wound disruption (
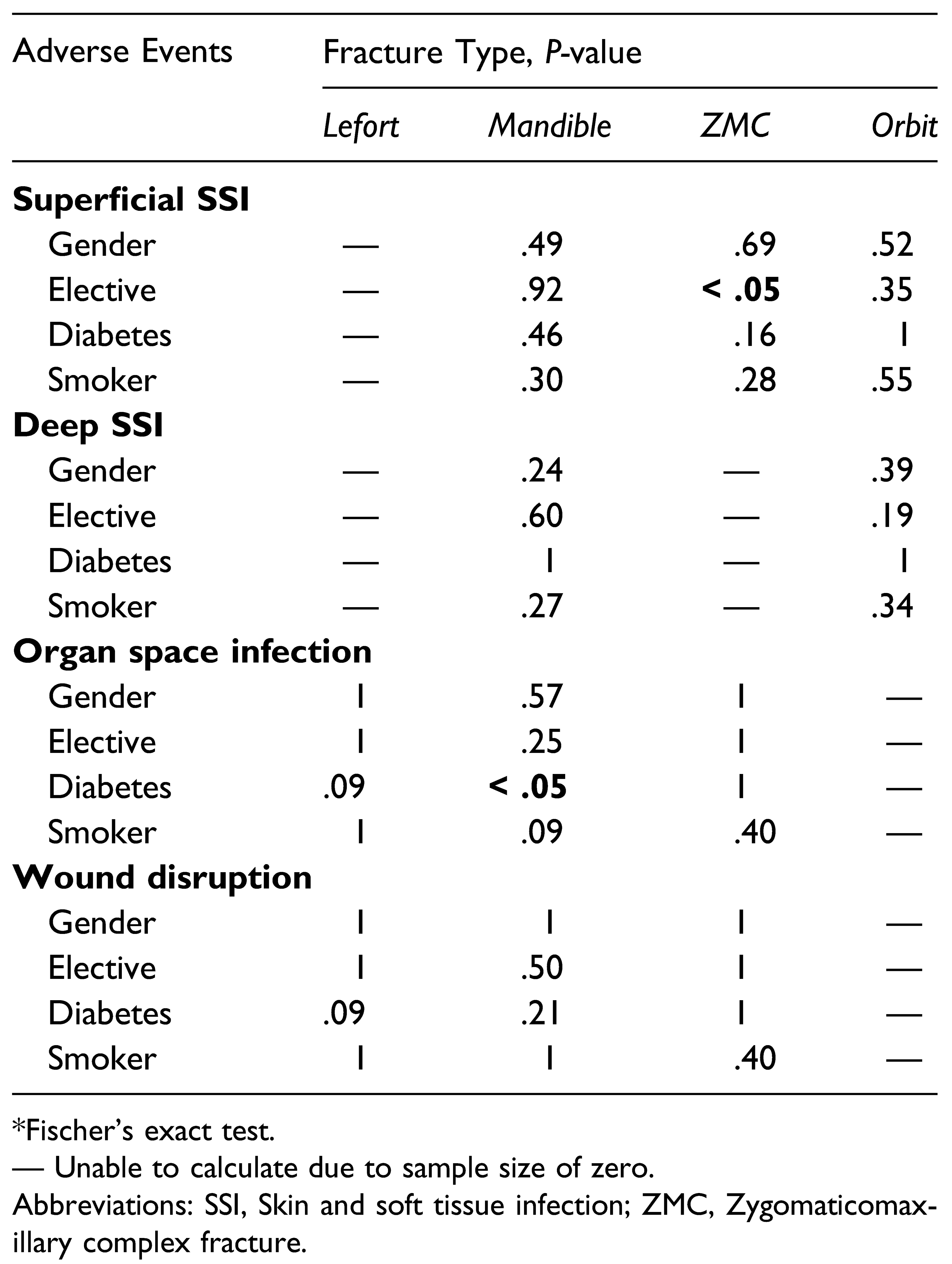
Table 2). In terms of overall complication rates, 25 patients (1.01%) experienced a superficial SSI, 14 patients (.56%) presented with a deep SSI, 25 fractures (1.01%) returned with an organ space infection, and 23 patients (.93%) experienced some type of wound disruption. Investigation between demographic categories and 30-day post-surgical outcomes for specific fracture categories showed that for mandibular fractures, patients with diabetes experienced a significantly higher proportion of organ space infections when compared to nondiabetic patients (
P < .05) (
Table 3). In patients with ZMC fractures, patients undergoing non-elective (immediate) procedures had a significantly higher rate of experiencing superficial SSIs in the initial post-operative period when compared to patients who underwent elective surgery (
P < .05).
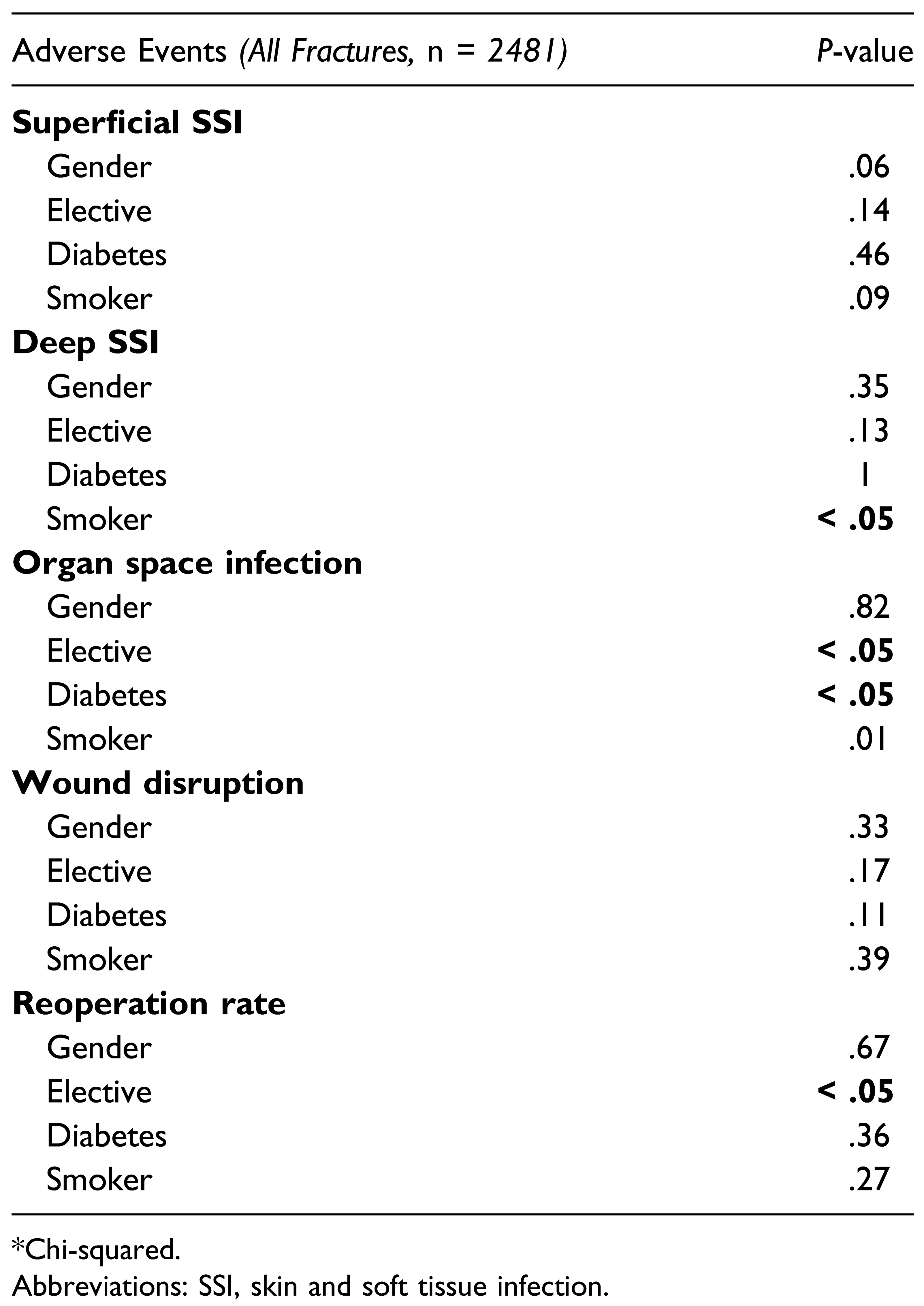
Complication rates among all fractures were analyzed (n = 2481) in relation to predictor variables (
Table 4). It was shown that smoking status was significantly associated with development of deep SSIs (
P < .05). Organ space SSIs were shown to be significantly increased in patients undergoing immediate operation (
P < .05), diabetes mellitus (
P < .05) and those who were smokers (
P < .05). Finally, the reoperation rate for patients undergoing emergent surgery was significantly higher than for patients undergoing delayed, elective procedures (
P < .05).
Discussion
Facial fractures are a common reason for presentation to EDs across the globe, and these injuries can damage delicate structures within the head and neck region. Fractures of the face often require surgical intervention to promote adequate bone union and healing, and these procedures may be performed on an emergent or elective basis depending on the presentation of the injury. It is crucial that the postoperative outcomes of surgical fracture repairs are welldocumented in order for clinicians to provide patients with accurate information regarding procedure risks. Furthermore, it is critical that surgeons can identify risk factors which may place patients at an elevated risk for postoperative complications following facial fracture repair. To our knowledge this is the first study to categorize 30-day facial fracture repair characteristics and complications using a large national database. The data presented in our study show that complication rates are generally low in the postoperative period for facial fracture repairs, and that certain patient characteristics, such as smoking and diabetes, are associated with higher complication rates in the context of facial fractures.
Firstly, our data show that four of the most common types of post-operative complications in facial fracture repair (superficial SSI, deep SSI, organ space infection, and wound disruption) are relatively uncommon, with each of these pathologies being identified in approximately 1% of patients undergoing repair. This is promising data and suggests that most facial fracture repairs are likely performed without significant complications in the immediate post-operative period (30 days), regardless of patient demographics/comorbidities. Our data also highlight that the vast majority of facial fracture patients are male (75.9%), and many of them are everyday smokers (43.3%). Though complication rates were generally low, given the large volume of patients treated for facial fractures each year this represents a sizeable number of patients, and complication rates increase costs for both patients and the healthcare system.
Upon further analysis, we observed multiple predictor variables which were significantly associated with 30-day post-operative complications on univariate analysis. Notably, when assessing complication rates among all types of fractures, smokers had significantly higher rates of deep SSI (P < .05) and organ space infection (P <.05) and had a higher rate (but non-significant association) with superficial SSIs (P = .09). Thus, smoking status represents a consistently important predictor of post-operative morbidity in facial fracture patients. Patients should be counseled for smoking cessation both at the time of fracture workup/ treatment, as well as at routine appointments by primary care providers.
In terms of other predictive variables, we observed that among all fracture types, patients with diabetes mellitus were more likely to experience organ space complications than those without diabetes (P < .05). This trend also held true for patients with mandibular fractures (P < .05), suggesting that diabetes likely impairs the body’s ability to clear infection at the level of facial bones. Furthermore, this represents an opportunity for the care team to reinforce the importance of optimal diabetes management in the pre- and post-operative setting. Finally, reoperation rates were higher in patients who underwent emergent surgery compared to those who were treated electively, suggesting that higher acuity injuries are more likely to require reoperation in the first 30 days after facial fracture.
One disadvantage of utilizing the NSQIP database is its lack of data on procedures performed by oral maxillofacial surgeons (OMFS). These surgeons, who typically attend dental school and subsequently complete an OMFS residency, are trained in treating a variety of craniofacial disorders including facial fractures. Furthermore, there are an estimated 5300 OMFS practitioners in the United States, [
17] and many are fellows of the American College of Surgeons, the facilitator of the NSQIP dataset. Given that many facial fractures across the United States are likely repaired by surgeons of OMFS background, we are uncertain whether the NSQIP database includes this data, as there is no way to stratify procedures performed by OMFS surgeons. Therefore, the authors recommend that future work is pursued to solicit this information and provide comprehensive insight on this topic.
Our study presents other limitations which must be addressed. The NSQIP database is designed to track many types of operations and patient variables, however, not all pertinent variables may be captured by the database. This study describes the presence of multiple post-operative complications in the setting of facial fracture repair, including infections, but pre-operative antibiotic administration is not collected by the NSQIP database. Thus, we are lacking a potentially important variable in the postoperative course of this patient cohort. Last, the database is maintained by humans and may be missing data and/or have inaccuracies. However, prior studies have been conducted to assess the data abstraction process for NSQIP and have found it to be generally accurate with only a few limiting factors when capturing data on complications. [
18,
19]