Single Institute Audit of Maxillofacial Trauma Cases Before and During COVID-19 Pandemic

Abstract
:Introduction
Materials and Methods
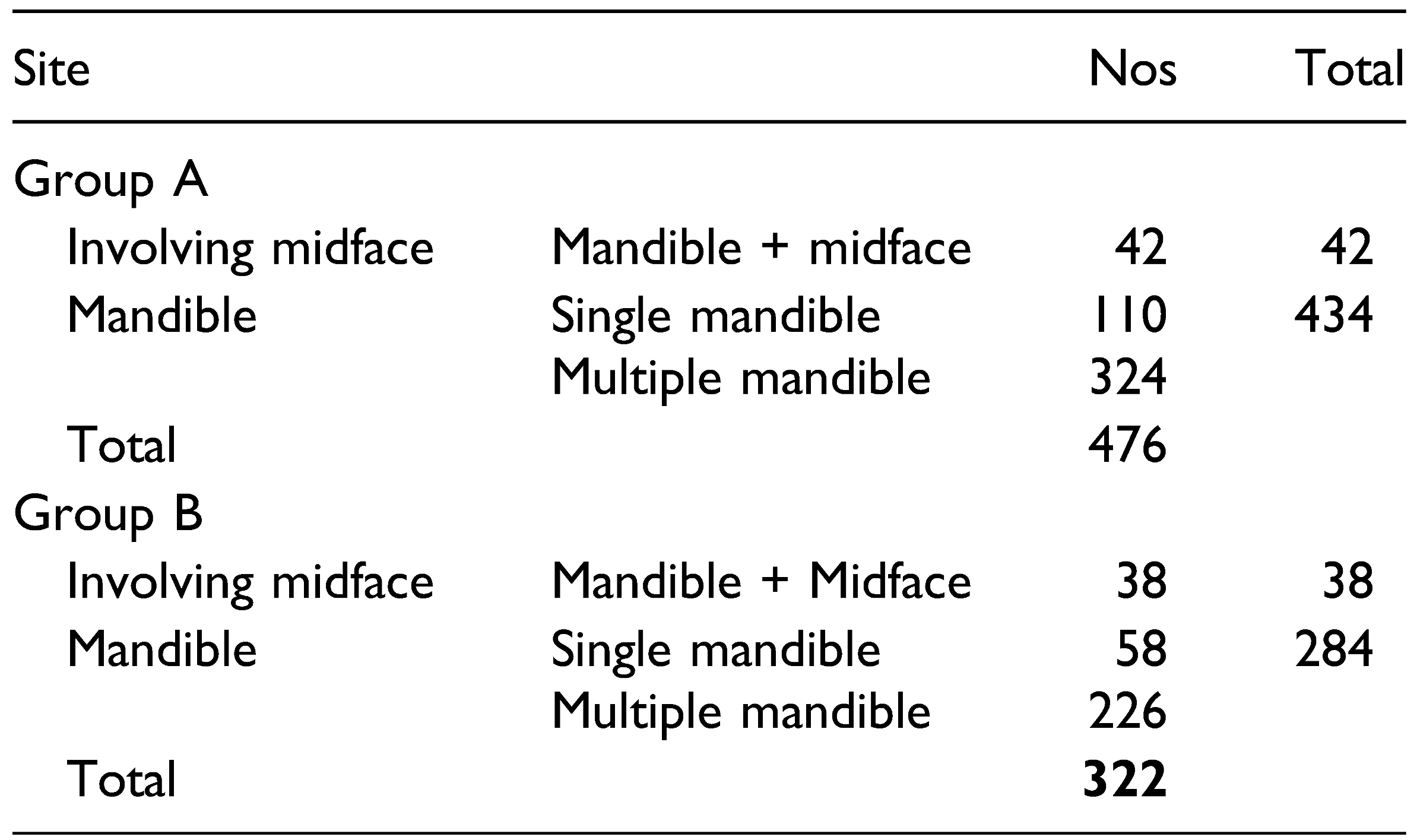
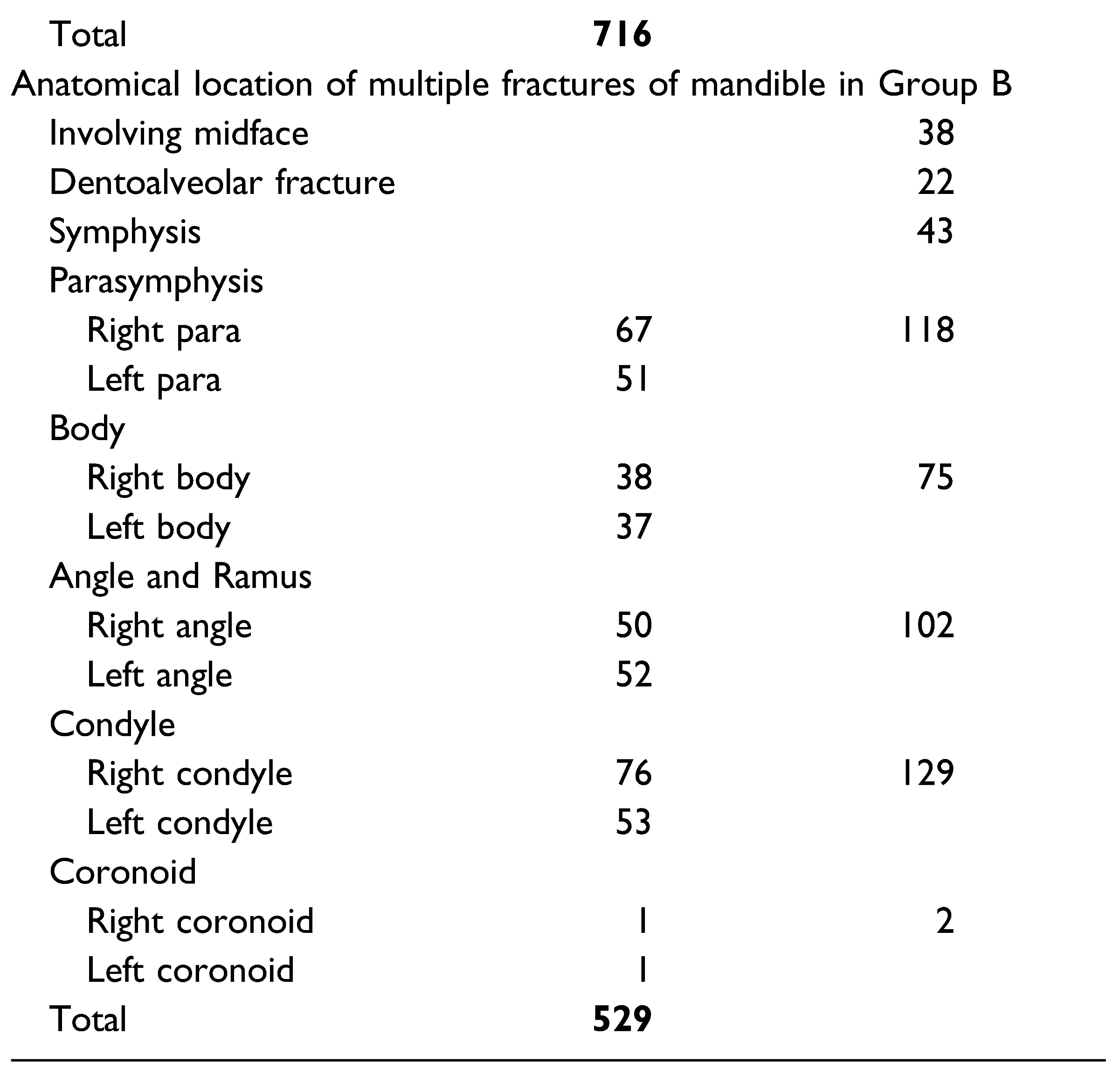
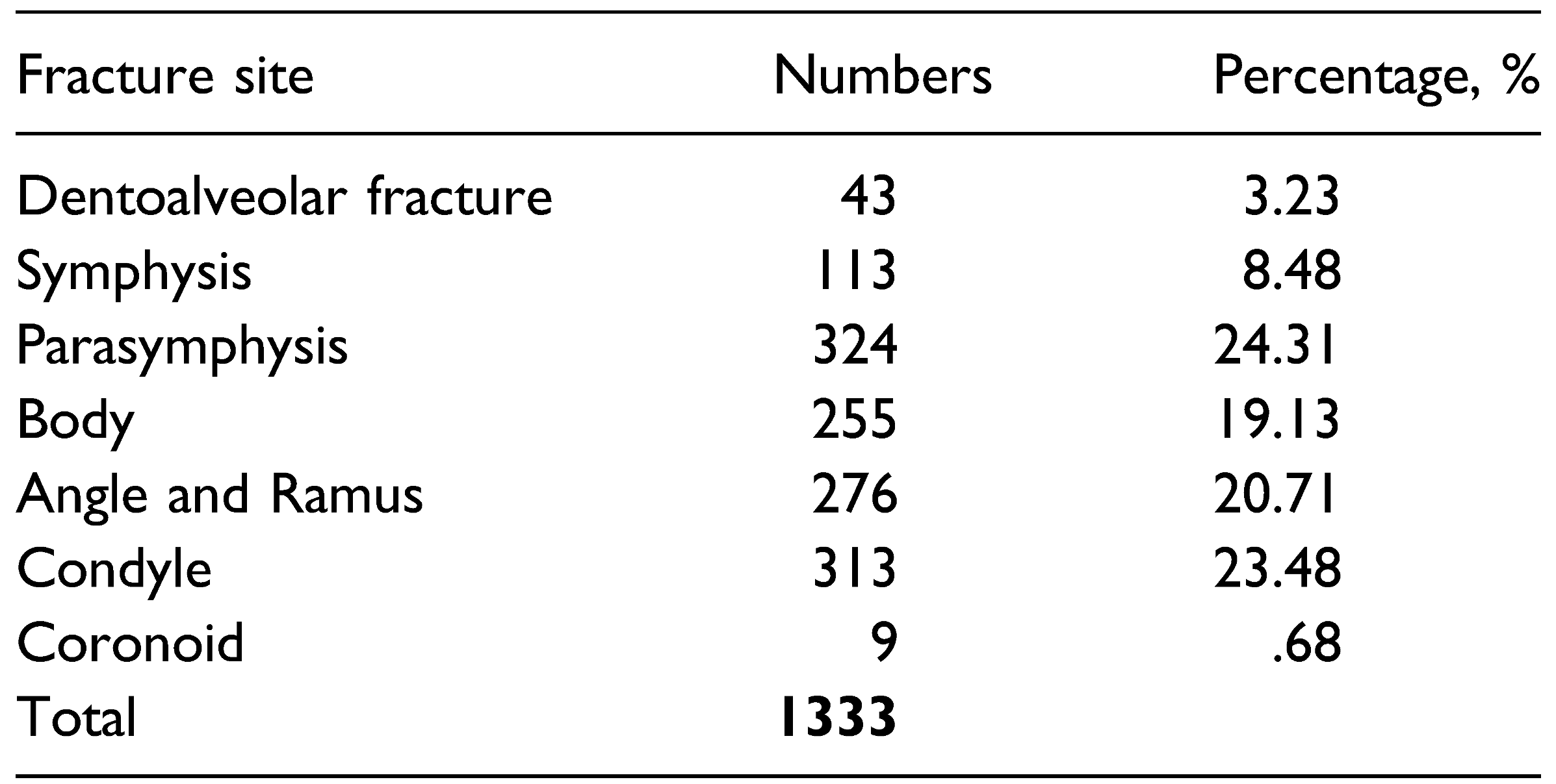
Results
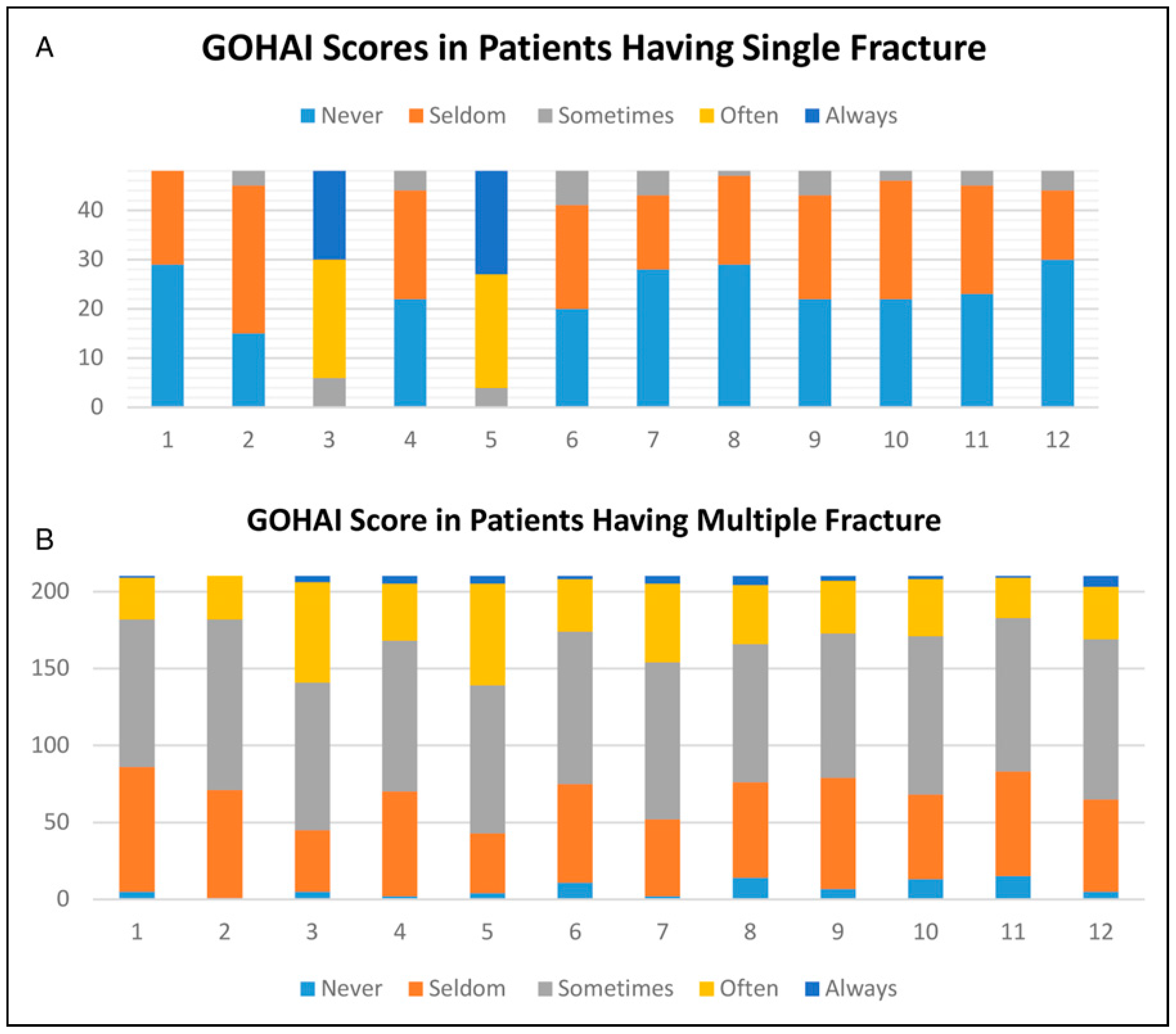
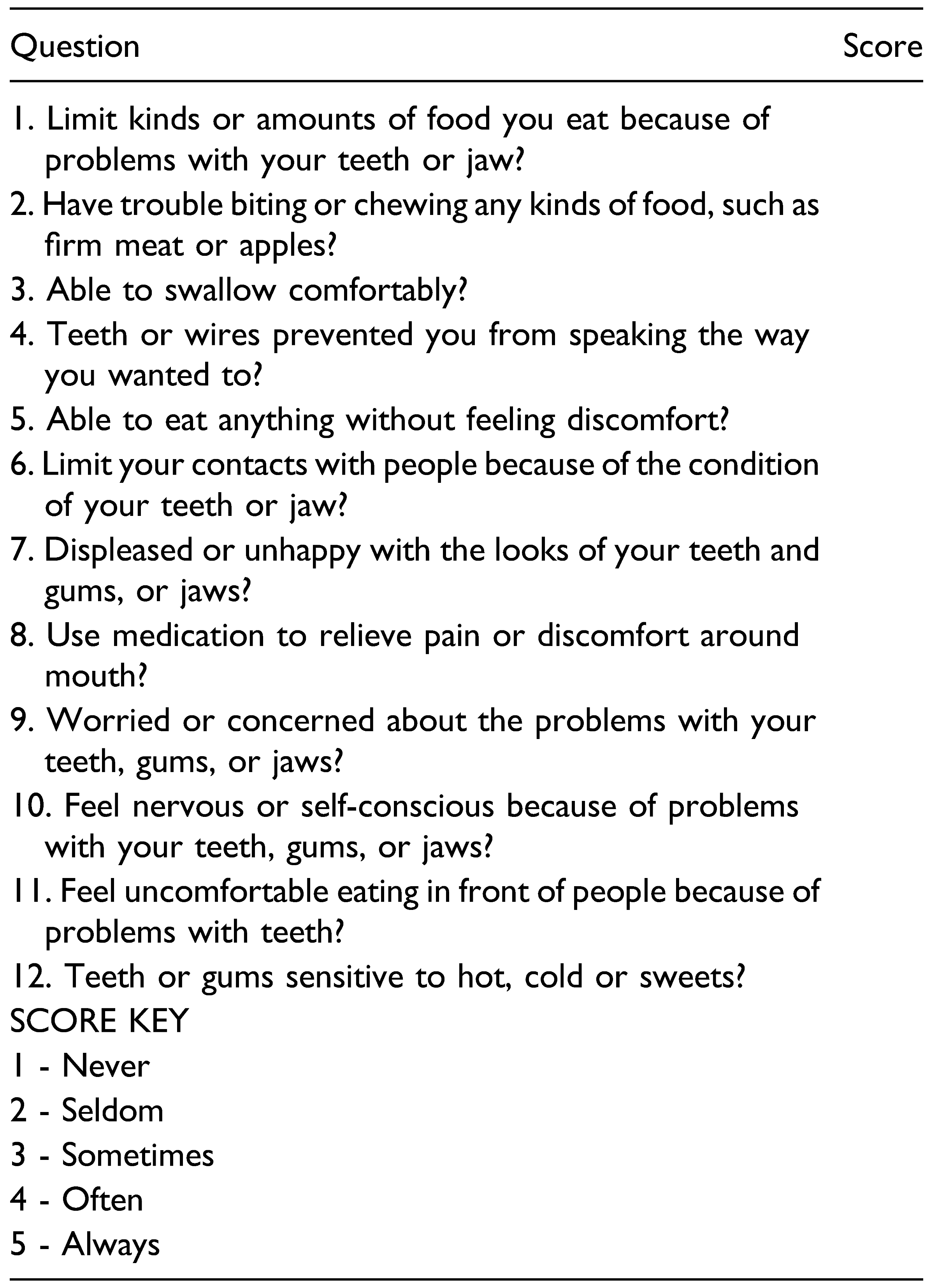
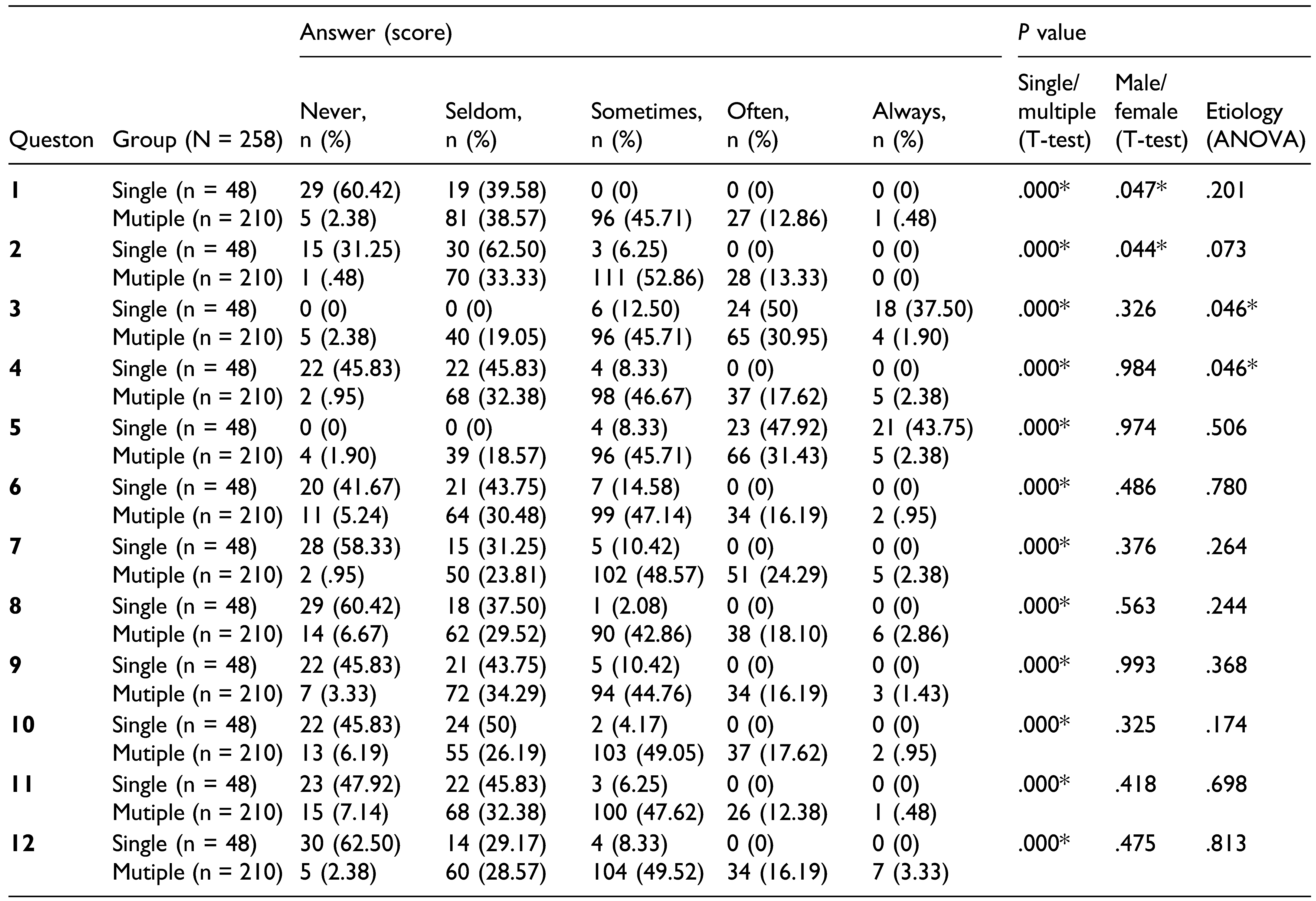
GOHAI QoL Results
Discussion
Supplementary Materials
Funding
Ethical Clearance
Declaration of Conflicting Interests
References
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef] [PubMed]
- Sawhney, C.; Singh, Y.; Jain, K.; Sawhney, R.; Trikha, A. Trauma care and COVID-19 pandemic. J. Anaesthesiol. Clin. Pharmacol. 2020, 36, S115–S120. [Google Scholar] [CrossRef] [PubMed]
- Vishal, O.; Prakash, O.; Rohit, V.K.; Prajapati, V.K.; Shahi, A.K.; Khaitan, T. Incidence of maxillofacial trauma amid COVID-19: A comparative study. J. Maxillofac. Oral Surg. 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.C.; Nelson, J.L.; Burke, A.B.; Lang, M.S.; Dillon, J.K. What is the effect of COVID-19-related social distancing on oral and maxillofacial trauma? J Oral Maxillofac Surg. 2021, 79, 1091–1097. [Google Scholar] [CrossRef]
- Canzi, G.; De Ponti, E.; Corradi, F.; et al. Epidemiology of maxillofacial trauma during COVID-19 lockdown: Reports from the hub trauma center in Milan. Craniomaxillofacial Trauma Reconstr. 2020, 14, 277–283. [Google Scholar] [CrossRef]
- WHO. World Health Organization Considerations for the Provision of Essential Oral Health Services in the Context of COVID-19: Interim Guidance, Geneva PP—Geneva: World Health Organization. 3 August 2020. Available online: https://apps.who.int/iris/handle/10665/333625.
- Yeung, E.; Brandsma, D.S.; Karst, F.W.; Smith, C.; Fan, K.F. M. The influence of 2020 coronavirus lockdown on presentation of oral and maxillofacial trauma to a central London hospital. Br. J. Oral Maxillofac. Surg. 2021, 59, 102–105. [Google Scholar] [CrossRef]
- Afzal, A. Molecular diagnostic technologies for COVID-19: Limitations and challenges. J. Adv. Res. 2020, 26, 149–159. [Google Scholar] [CrossRef]
- Atchison, K.A.; Shetty, V.; Belin, T.R.; et al. Using patient self-report data to evaluate orofacial surgical outcomes. Community Dent. Oral Epidemiol. 2006, 34, 93–102. [Google Scholar] [CrossRef]
- Dingman, R.O.; Navig, P. Surgery of Facial Fractures; Saunders, 1964. [Google Scholar]
- Virdi, M.K.; Durman, K.; Deacon, S. The debate: What are aerosol-generating procedures in dentistry? A rapid review. JDR Clin. Trans. Res. 2021, 6, 115–127. [Google Scholar] [CrossRef]
- Harding, H.; Broom, A.; Broom, J. Aerosol-generating procedures and infective risk to healthcare workers from SARSCoV-2: The limits of the evidence. J. Hosp. Infect. 2020, 105, 717–725. [Google Scholar] [CrossRef]
- Hamilton, G.S. Aerosol-generating procedures in the COVID era. Respirology. 2021, 26, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Ge, Z.-Y.; Yang, L.-M.; Xia, J.-J.; Fu, X.-H.; Zhang, Y.-Z. Possible aerosol transmission of COVID-19 and special precautions in dentistry. J. Zhejiang Univ. Sci. B 2020, 21, 361–368. [Google Scholar] [CrossRef]
- Mazza, M.; Marano, G.; Lai, C.; Janiri, L.; Sani, G. Danger in danger: Interpersonal violence during COVID-19 quarantine. Psychiatr. Res. 2020, 289, 113046. [Google Scholar] [CrossRef]
- Mittal, S.; Singh, T. Gender-based violence during COVID-19 pandemic: A mini-review. Front. Glob. Women’s Health. 2020, 1, 4. [Google Scholar] [CrossRef] [PubMed]
- Nadda, A.; Malik, J.S.; Rohilla, R.; Chahal, S.; Chayal, V.; Arora, V. Study of domestic violence among currently married females of Haryana, India. Indian J. Psychol. Med. 2018, 40, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Chaurasia, A.; Katheriya, G. Prevalence of mandibular fracture in patients visiting a tertiary dental care hospital in North India. Natl. J. Maxillofac. Surg. 2018, 9, 123–128. [Google Scholar] [CrossRef]
- Abhinav, R.; Selvarasu, K.; Maheswari, G.; Taltia, A. The patterns and etiology of maxillofacial trauma in South India. Ann. Maxillofac. Surg. 2019, 9, 114–117. [Google Scholar] [CrossRef]
- Barde, D.; Madan, R.; Mudhol, A. Prevalence and pattern of mandibular fracture in Central India. Natl. J. Maxillofac. Surg. 2014, 5, 153–156. [Google Scholar] [CrossRef]
- Edwards, S.P.; Kasten, S.; Nelson, C.; Elner, V.; McKean, E. Maxillofacial trauma management during COVID-19: Multidisciplinary recommendations. Facial Plast. Surg. Assihelj Med. 2020, 22, 157–159. [Google Scholar] [CrossRef]
- Puglia, F.A.; Hills, A.; Dawoud, B.; et al. Management of oral and maxillofacial trauma during the first wave of the COVID-19 pandemic in the United Kingdom. Br. J. Oral Maxillofac. Surg. 2021, 59, 867–874. [Google Scholar] [CrossRef]
- Blitz, M.; Notarnicola, K. Closed reduction of the mandibular fracture. Atlas Oral Maxillofac. Surg. Clin. 2009, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Omeje, K.U.; Rana, M.; Adebola, A.R.; et al. Quality of life in treatment of mandibular fractures using closed reduction and maxillomandibular fixation in comparison with open reduction and internal fixation—A randomized prospective study. J. Craniomaxillofac. Surg. 2014, 42, 1821–1826. [Google Scholar] [CrossRef] [PubMed]
- Osunde, O.; Omeje, K.; Efunkoya, A.; Adebola, A. Oral health-related quality of life in non-surgical treatment of mandibular fractures: A pilot study. Niger. J. Exp. Clin. Biosci. 2015, 3, 8–13. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
 |
  |
 |
 |
 |
© 2022 by the author. Multimed Inc.
Share and Cite
Kadanthode, M.; Chaudhary, Z.; Sharma, P.; Mohanty, S.; Sharma, C. Single Institute Audit of Maxillofacial Trauma Cases Before and During COVID-19 Pandemic. Craniomaxillofac. Trauma Reconstr. 2023, 16, 102-111. https://doi.org/10.1177/19433875211064514
Kadanthode M, Chaudhary Z, Sharma P, Mohanty S, Sharma C. Single Institute Audit of Maxillofacial Trauma Cases Before and During COVID-19 Pandemic. Craniomaxillofacial Trauma & Reconstruction. 2023; 16(2):102-111. https://doi.org/10.1177/19433875211064514
Chicago/Turabian StyleKadanthode, Mithilesh, Zainab Chaudhary, Pankaj Sharma, Sujata Mohanty, and Chayanika Sharma. 2023. "Single Institute Audit of Maxillofacial Trauma Cases Before and During COVID-19 Pandemic" Craniomaxillofacial Trauma & Reconstruction 16, no. 2: 102-111. https://doi.org/10.1177/19433875211064514
APA StyleKadanthode, M., Chaudhary, Z., Sharma, P., Mohanty, S., & Sharma, C. (2023). Single Institute Audit of Maxillofacial Trauma Cases Before and During COVID-19 Pandemic. Craniomaxillofacial Trauma & Reconstruction, 16(2), 102-111. https://doi.org/10.1177/19433875211064514