Should Degree of Third Molar Eruption Influence Operative Management of Mandibular Angle Fractures? A Systematic Review
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Sample
2.2. Eligibility
2.3. Variables
2.4. Data Collection
2.5. Quality Assessment
2.6. Data Analysis
3. Results
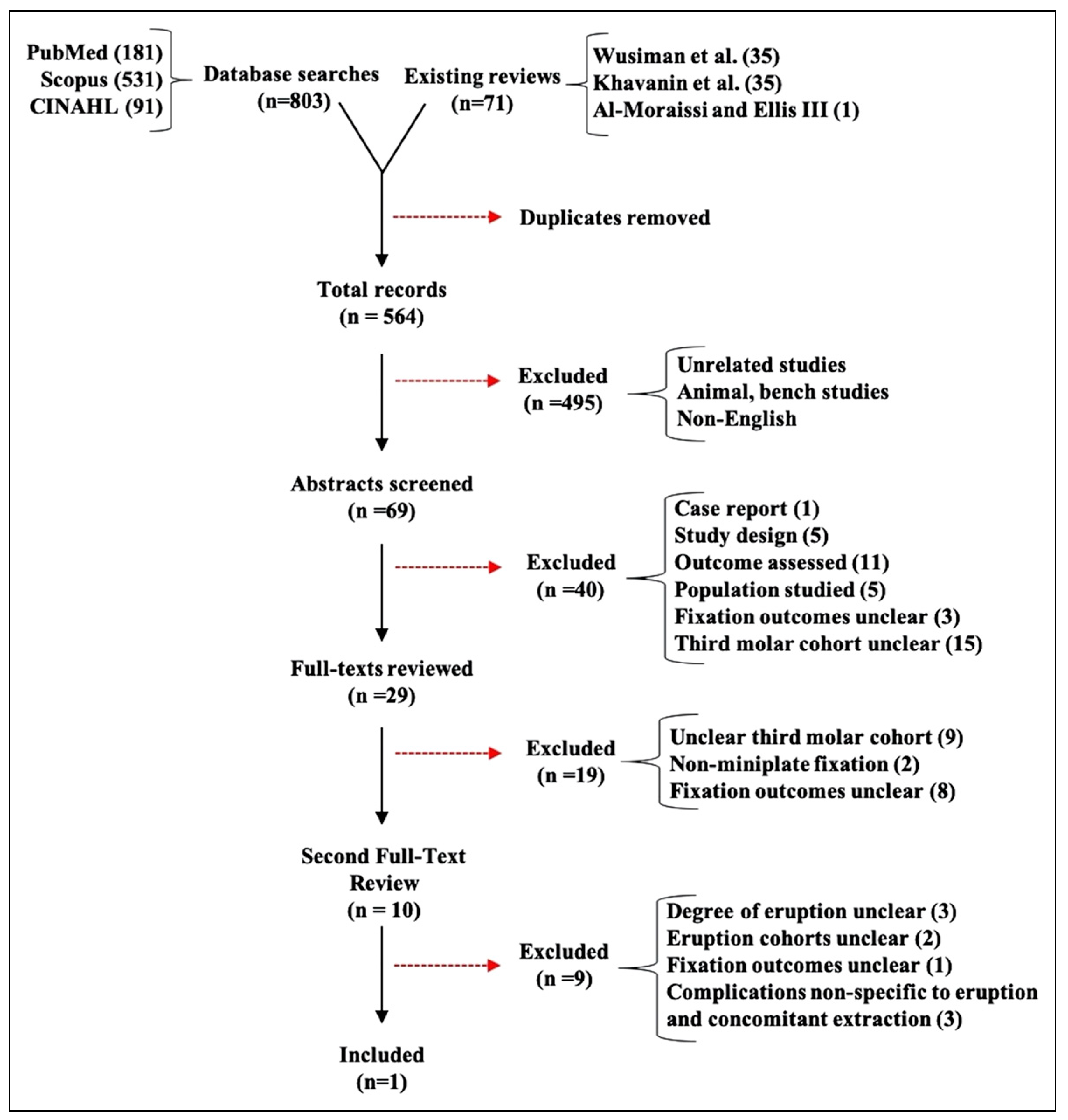
3.1. Study Selection
3.2. Characteristics of Included Studies
3.3. Influence of Molar Eruption and Extraction on Complications
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Ellis, E. Management of fractures through the angle of the mandible. Oral. Maxillofac. Surg. Clin. N. Am. 2009, 21, 163–174. [Google Scholar] [CrossRef]
- Ellis, E., 3rd. A prospective study of 3 treatment methods for isolated fractures of the mandibular angle. J. Oral. Maxillofac. Surg. 2010, 68, 2743–2754. [Google Scholar] [CrossRef] [PubMed]
- Al-Moraissi, E.A.; Ellis, E. What method for management of unilateral mandibular angle fractures has the lowest rate of postoperative complications? a systematic review and metaanalysis. J. Oral. Maxillofac. Surg. 2014, 72, 2197–2211. [Google Scholar] [CrossRef]
- Champy, M.; Lodde, J.P.; Schmitt, R.; Jaeger, J.H.; Muster, D. Mandibular osteosynthesis by miniature screwed plates via a buccal approach. J. Maxillofac. Surg. 1978, 6, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Gerbino, G.; Tarello, F.; Fasolis, M.; De Gioanni, P.P. Rigid fixation with teeth in the line of mandibular fractures. Int. J. Oral. Maxillofac. Surg. 1997, 26, 182–186. [Google Scholar] [CrossRef]
- Khavanin, N.; Jazayeri, H.; Xu, T.; Pedreira, R.; Lopez, J.; Reddy, S.; Shamliyan, T.; Peacock, Z.S.; Dorafshar, A.H. Management of teeth in the line of mandibular angle fractures treated with open reduction and internal fixation: A systematic review and metaanalysis. Plast. Reconstr. Surg. 2019, 144, 1393–1402. [Google Scholar] [CrossRef] [PubMed]
- Wusiman, P.; Abasi, K.; Maimaitishawuti, D.; Moming, A. Management of mandibular angle fractures using one miniplate or two miniplate fixation system: A systematic review and meta-analysis. J. Oral. Maxillofac. Surg. 2019, 77, 1673.e1–1673.e11. [Google Scholar] [CrossRef]
- McNamara, Z.; Findlay, G.; O’Rourke, P.; Batstone, M. Removal versus retention of asymptomatic third molars in mandibular angle fractures: A randomized controlled trial. Int. J. Oral. Maxillofac. Surg. 2016, 45, 571–574. [Google Scholar] [CrossRef]
- Schierle, H.P.; Schmelzeisen, R.; Rahn, B.; Pytlik, C. Oneor two-plate fixation of mandibular angle fractures? J. CranioMaxillo-Facial Surg. 1997, 25, 162–168. [Google Scholar] [CrossRef]
- Vineeth, K.; Lalitha, R.M.; Prasad, K.; Ranganath, K.; Shwetha, V.; Singh, J. A comparative evaluation between single noncompression titanium miniplate and three dimensional titanium miniplate in treatment of mandibular angle fracture–A randomized prospective study. J. Craniomaxillofac. Surg. 2013, 41, 103–109. [Google Scholar] [CrossRef]
- Xue, A.S.; Koshy, J.C.; Wolfswinkel, E.M.; Weathers, W.M.; Marsack, K.P.; Hollier, L.H. A prospective study of strut versus miniplate for fractures of mandibular angle. Craniomaxillofac. Trauma. Reconstr. 2013, 6, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Barry, C.P.; Kearns, G.J. Superior border plating technique in the management of isolated mandibular angle fractures: A retrospective study of 50 consecutive patients. J. Oral. Maxillofac. Surg. 2007, 65, 1544–1549. [Google Scholar] [CrossRef]
- Bhatt, K.; Arya, S.; Bhutia, O.; Pandey, S.; Roychoudhury, A. Retrospective study of mandibular angle fractures treated with three different fixation systems. Natl. J. Maxillofac. Surg. 2015, 6, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Boffano, P.; Roccia, F. Bilateral mandibular angle fractures: Clinical considerations. J. Craniofac Surg. 2010, 21, 328–331. [Google Scholar] [CrossRef]
- Ferrari, R.; Lanzer, M.; Wiedemeier, D.; Rucker, M.; Bredell, M. Complication rate in mandibular angle fractures-one vs. two plates: A 12-year retrospective analysis. Oral. Maxillofac. Surg. 2018, 22, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Ulbrich, N.; Ettl, T.; Waiss, W.; Gosau, M.; Moralis, A.; Reichert, T.E.; Mueller, S. The influence of third molars in the line of mandibular angle fractures on wound and bone healing. Clin. Oral. Investig. 2016, 20, 1297–1302. [Google Scholar] [CrossRef]
- Wan, K.; Williamson, R.A.; Gebauer, D.; Hird, K. Open reduction and internal fixation of mandibular angle fractures: Does the transbuccal technique produce fewer complications after treatment than the transoral technique? J. Oral. Maxillofac. Surg. 2012, 70, 2620–2628. [Google Scholar] [CrossRef]
- Bobrowski, A.N.; Sonego, C.L.; Chagas, O.L. Postoperative infection associated with mandibular angle fracture treatment in the presence of teeth on the fracture line: A systematic review and meta-analysis. Int. J. Oral. Maxillofac. Surg. 2013, 42, 1041–1048. [Google Scholar] [CrossRef]
- Shetty, V.; Freymiller, E. Teeth in the line of fracture: A review. J. Oral. Maxillofac. Surg. 1989, 47, 1303–1306. [Google Scholar] [CrossRef]
- Neal, D.C.; Wagner, W.F.; Alpert, B. Morbidity associated with teeth in the line of mandibular fractures. J. Oral. Surg. 1978, 36, 859–862. [Google Scholar]
- de Amaratunga, N.A. The effect of teeth in the line of mandibular fractures on healing. J. Oral. Maxillofac. Surg. 1987, 45, 312–314. [Google Scholar] [CrossRef] [PubMed]
- Galvão, E.L.; da Silveira, E.M.; de Oliveira, E.S.; da Cruz, T.M.M.; Flecha, O.D.; Falci, S.G.M.; Gonçalves, P.F. Association between mandibular third molar position and the occurrence of pericoronitis: A systematic review and meta-analysis. Arch. Oral. Biol. 2019, 107, 104486. [Google Scholar] [CrossRef]
- Levy, F.E.; Smith, R.W.; Odland, R.M.; Marentette, L.J. Monocortical miniplate fixation of mandibular angle fractures. Arch. Otolaryngol. Neck Surg. 1991, 117, 149–154. [Google Scholar] [CrossRef]
- Choi, B.H.; Kim, K.N.; Kang, H.S. Clinical and in vitro evaluation of mandibular angle fracture fixation with the two-miniplate system. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 1995, 79, 692–695. [Google Scholar] [CrossRef] [PubMed]
- Curran, J.B. An assessment of the use of prophylactic antibiotics in third molar surgery. Int. J. Oral. Surg. 1974, 3, 1–6. [Google Scholar] [CrossRef]
- Pasupathy, S.; Alexander, M. Antibiotic prophylaxis in third molar surgery. J. Craniofac Surg. 2011, 22, 551–553. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
 |
 |
 |
© 2021 by the authors. Published by MDPI on behalf of the AO Foundation. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kotha, V.S.; de Ruiter, B.J.; Knudsen, M.G.; Nicoleau, M.; Davidson, E.H. Should Degree of Third Molar Eruption Influence Operative Management of Mandibular Angle Fractures? A Systematic Review. Craniomaxillofac. Trauma Reconstr. 2022, 15, 379-386. https://doi.org/10.1177/19433875211059330
Kotha VS, de Ruiter BJ, Knudsen MG, Nicoleau M, Davidson EH. Should Degree of Third Molar Eruption Influence Operative Management of Mandibular Angle Fractures? A Systematic Review. Craniomaxillofacial Trauma & Reconstruction. 2022; 15(4):379-386. https://doi.org/10.1177/19433875211059330
Chicago/Turabian StyleKotha, Vikas S., Brandon J. de Ruiter, M. Grace Knudsen, Marvin Nicoleau, and Edward H. Davidson. 2022. "Should Degree of Third Molar Eruption Influence Operative Management of Mandibular Angle Fractures? A Systematic Review" Craniomaxillofacial Trauma & Reconstruction 15, no. 4: 379-386. https://doi.org/10.1177/19433875211059330
APA StyleKotha, V. S., de Ruiter, B. J., Knudsen, M. G., Nicoleau, M., & Davidson, E. H. (2022). Should Degree of Third Molar Eruption Influence Operative Management of Mandibular Angle Fractures? A Systematic Review. Craniomaxillofacial Trauma & Reconstruction, 15(4), 379-386. https://doi.org/10.1177/19433875211059330