Introduction
COVID-19 pandemic has posed wide-ranging ramifications to the people & community. Since the first reporting of SARS-CoV-2 virus in Wuhan, China at the end of Decem- ber 2019, countries have had to introduce & re-adjust extraordinary & radical reforms to control the spread. Needless to say, it also brought in restrictions on movement of people, work, schools & physical activities causing a tremendous impact on general as well as mental health. There was notable & worrying increase in domestic violence & self-harm during this period.[
1] Many people adopted lifestyle changes to cope with the imposed lock- down taking up new activities & hobbies to improve their physical & mental health.
Cycling is a beneficial physical activity with positive health outcomes. It has been proven to reduce risk of mul- tiple co-morbidities including mental health disorders & mortality apart from easing traffic congestion, protecting the environment & providing economic benefits.[
2,
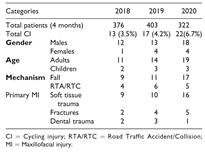
3] We noted an increase in cycling injuries presenting to our unit during the recent COVID-19 pandemic lockdown period compared to previous years (
Table 1). We investigated this sudden increase in cycling injuries presenting to our unit during this challenging period.
Methods
The data was derived from our robust maxillofacial trauma database & electronic patient record (Cerner®). The results were collected & analyzed by a single clinician. All bicycle-related injuries starting from 16th March 2020 (beginning of lockdown period in the UK) extending for a total period of 4 months (coincidental with easing of lockdown) were retrospectively interrogated in this study. Statistical analyses were conducted using Chi-square and Fisher’s Exact tests to ascertain relationships between dif- ferent variables (IBM SPSS® software).
Results
All 22 patients who suffered maxillofacial injuries cycling (CI) during the lockdown period were included in this study (
Table 2). The incidence was 6.7% (Total maxillofacial emergencies in this period: n ¼ 332). COVID-19 status testing was restricted to patients undergoing general anes- thetic procedures (18%) in our trust and were all reported as negative. All patients were assessed and treated using stan- dard personal protective equipment (PPE) provided as per
local trust protocol and in conjunction with the national guidelines.Majority of the patient cohort were Adult males (77%) with children constituting only 14% of cases comparable to data related to previous years (Average age: 35.41 years). This was mainly due to reduction in pediatric services in our trust leading to temporary restriction of pediatric emer- gencies needing admission from the end of March 2020 due to flurry of COVID-19 cases. Fall injuries related to loss of balance, hitting obstacles and intoxication made up 17/22 cases (77%) cases with the remaining cases related to Road traffic accidents/collision (RTA/RTC).
Seven patients suffered with minor head injury (HI) and 1 patient had traumatic brain injury (subarachnoid/subdural hemorrhage). Transient loss of consciousness, confusion/ disorientation, vomiting, retrograde amnesia, headaches were some of the symptoms noted in these patients with 3 patients presenting to Emergency Department(ED) with GCS of 14/15. Only 41% of these patients confessed to wearing a helmet during their journey. Three patients pre- sented with alcohol/recreational drug intoxication. Seven patients (32%) also presented with other bodily injuries (BI) including upper & lower limb abrasions, soft tissue swelling, shoulder dislocation, distal radius, and ulna sty- loid & scaphoid fractures.
Soft tissue facial trauma (73%), Facial fractures (23%) and Dental Trauma (5%) were the primary maxillofacial injuries (MI) suffered by this cohort. Majority of the lacera- tions were related to the lips (44%) followed by chin (25%) and forehead (19%) regions showing a predilection to mid face injuries.
Sixteen patients (73%) also had secondary injuries including Soft tissue trauma (62.5%), Dental trauma (25%) & other fractures (6.25%). Local anesthetic treatment was required in the majority (64%) and 4 patients needed general anesthetic procedures (18%). Two complications/ re-attendances (9%) were noted with 1 patient attending due to loose intermaxillary fixation screw & another complain- ing of residual foreign body in the upper lip.
No statistical significance was noted to establish any rela- tionship between alcoholwith falls (p ¼ 0.5584) & RTA/RTC (p ¼ 1); helmet use with head injury (p ¼ 0.8058); RTA/RTC with head injury (p ¼ 0.8475) & bodily injuries (p ¼ 0.5186) (
Table 3).
Discussion
About 3% of the population in England & Wales are depen- dent on bicycles for commuting.[
3] They are included in the “vulnerable road users” along with pedestrians & motorcy- clists. A recent large population survey of cycling commu- ters from 22 sites in UK noted significantly increased risk of traffic related incidents & hospital admissions in this cohort adding to UK Government statistics showing increase in number of fatalities/serious injuries among cyclists (by 29% compared to 2008).[
4,
5] A recent retrospec- tive review of orthopedic injuries in pediatric population related to cycling during the COVID-19 period noted
>100% increase in bicycle-related injuries.[
6]
The City of London in particular is known to have increased bicycle traffic & considered widely as “bike friendly.”[
7] It has developed effective sustainable transport facilities including provision of “Cycleways” (previously London Cycle Superhighway’) to assist commuters to reach different areas of the city.[
8] The London cycle hire scheme (LCHS) was started in 2010 providing easy access to shared bicycles round the year connecting different parts of the city. Woodcock et al noted improved overall health benefits in a large health outcome study for cyclists using the bike hire scheme in London.[
9] A number of “cycling friendly” initiatives including ultra-low emission zones, segregated cycle paths & congestion charges have been implemented to curtail motor vehicle traffic in many parts of the city. Unfortunately, the cyclists also constituted 8% of all road traffic fatalities in London in 2017 which increased to 11% in 2018.[
10]
Our cohort consisted of patients between the ages of 4 to 67 years (Mean 35.41 years (with 82% (n ¼ 18) being males & majority of these patients did not wear protective
ing helmets.[
13,
15]
A retrospective cohort study of about 7000 patients in Germany showed no reduction in facial injuries in helmet wearers and this is attributed to the design of the helmets which did not afford facial protection. 16 Recently,
lightweight full face helmets have entered the market pro-mising protection from facial trauma along with head injury (Figure 1). There is no law in the UK making helmet use mandatory, although the Highway Code specifies wear- ing a correct sized & securely fastened helmet for all cyclists.[
17]
Additionally, the LCHS does not provide a pro- tective helmet & current evidence suggests that cyclists using this scheme are also less likely to use helmets.[
18]
There is market availability of a range of protective portable/ foldable helmets that can be stored and carried easily, albeit they are on the expensive side [100€–400€] (
Figure 2). At least, 29 countries have some form of legislation toward use of helmets for cyclists [
19]
(Table 4). A political discussion has ensued regarding mandatory helmet requirement in spite of concrete evidence that they reduce head/facial injuries in cyclists. Many argue that legislations discourage people from taking up sustainable transport. A number of studies especially in countries like Sweden & Australia have noted reduction of cycling injuries & associated fatalities due to
compulsory helmet use.[
20,
21]
A Cochrane study in children noted similar findings suggesting that helmet use decreased head injuries.[
22]
Recent meta-analyses of 21 studies observed significant reductions of minor & major head injuries as well as debunking the generalized notion that helmet use dissuades people from cycling.[
23]
Majority of cyclists who attended the emergency depart- ment were due to “single cycling accidents” i.e. without involvement/collision with other vehicles (77%). This is also one of the reasons for underreporting of cycling inju- ries as the injuries are less likely to be “serious” in nature compared to road traffic collisions. Due to the retrospective nature of study, specific data with regards to type of bicycles (conventional or electric or modified) was not available. Early studies of electric bicycle injuries have been noted to be more serious in nature & comparable to motorcycle related injuries.[
24] Cyclists are also at a higher risk of spinal injuries and increased incidences of these life-changing injuries during recent times are concerning.[
25]
In our study, only 3 patients confessed to have been cycling under the influence of alcohol. However, there is growing evidence to associate cycling injuries with alcohol intake. In the UK, there are no laws to measure the legal limit of alcohol for a cyclist as observed in some European countries.[
26]
Limitations of This Study
Our study was limited by a small cohort and retrospective nature of the study and the sample may not be representa- tive of all bicycle injuries of North London as it is depen- dent on patients reporting these injuries as well presence of other ED in the vicinity which are not part of our trust. Small facial injuries seen by ED may still be discharged without any maxillofacial review. No information was gathered regarding type of bicycle, speed, experience of the rider & location of the injury. Major inferences are there- fore not possible from this humble review. A prospective multi-center investigation may provide a realistic sample & data for accurate analysis.
Conclusion
In general, providing cyclists a safe environment (cycle paths/bicycle lanes; decreasing speed limit in built up areas to 20 mph) is essential & the “safety in numbers” (more cyclists on the road decreases risk of cycling injuries) concept seems to get a boost from current research.[
27,
28] We recommend sweeping changes to the current laws to improve road safety, legislation of personal safety mea- sures & active policing of drug intoxication among cyclists just as other road users. The pandemic of COVID-19 will lead to long term changes to the lifestyle & health of our population especially in major cities of the world. Prospec- tive studies are needed to derive robust data related to cycling injuries & its associations to prevent debilitating injuries.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Acknowledgment
We express our gratitude to Ms Sue Adams at UCL Library ser- vices, London for assisting us in obtaining relevant literature for this publication.
Conflicts of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
- Olding J, Zisman S, Olding C, Fan K. Penetrating trauma during a global pandemic: Changing patterns in interpersonal violence, self-harm and domestic violence in the Covid-19 outbreak. [published online ahead of print, 2020 Jul 30]. Surgeon, 1479.
- Dinu M, Pagliai G, Macchi C, Sofi F. Active commuting and multiple health outcomes: a systematic review and meta- analysis. Sports Med.
- Patterson R, Panter J, Vamos EP, Cummins S, Millett C, Laverty AA. Associations between commute mode and car- diovascular disease, cancer, and all-cause mortality, and can- cer incidence, using linked Census data over 25 years in England and Wales: a cohort study. Lancet Planet Health.
- Welsh C, Celis-Morales CA, Ho F, et al. Association of injury related hospital admissions with commuting by bicycle in the UK: prospective population based study. BMJ.
- Department for Transport. Reported road casualties in Great Britain 2018. Publised 2019. Updated , 2020. Accessed November 11, 2020. https://assets.publishing.ser vice.gov.uk/government/uploads/system/uploads/attach ment_data/file/820562/Reported_road_casualties_-_Main_ Results_2018. 12 February.
- Bram JT, Johnson MA, Magee LC, et al. Where have all the fractures gone? The epidemiology of pediatric fractures dur- ing the COVID-19 pandemic. J Pediatr Orthop.
- Klemmer K, Brandt T, Jarvis S. Isolating the effect of cycling on local business environments in London. PLoS One, e: 13(12), 0209.
- Ding H, Sze NN, Li H, Guo Y. Roles of infrastructure and land use in bicycle crash exposure and frequency: a case study using greater London bike sharing data. Accid Anal Prev, 1056.
- Woodcock J, Tainio M, Cheshire J, O’Brien O, Goodman A. Health effects of the London bicycle sharing system: health impact modelling study. BMJ.
- Transport for London, TfL. Travel in London, report 12. Published 2019. Accessed , 2020. http://con tent.tfl.gov.uk/travel-in-london-report-12. 11 November.
- Strotmeyer SJ, Behr C, Fabio A, Gaines BA. Bike helmets prevent pediatric head injury in serious bicycle crashes with motor vehicles. Inj Epidemiol, 2: 1).
- Scott LR, Bazargan-Hejazi S, Shirazi A, et al. Helmet use and bicycle-related trauma injury outcomes. Brain Inj, 1: 33(13-14), 1597.
- Olivier J, Creighton P. Bicycle injuries and helmet use: a systematic review and meta-analysis. Int J Epidemiol, 2: 46(1).
- Boffano P, Roccia F, Gallesio C, Karagozoglu KH, Forouzanfar T. Bicycle-related maxillofacial injuries: a double-center study. Oral Surg Oral Med Oral Pathol Oral Radiol.
- Fitzpatrick DG, Goh M, Howlett DC, Williams M. Bicycle helmets are protective against facial injuries, including facial fractures: a meta-analysis. Int J Oral Maxillofac Surg, 1: 47(9), 1121.
- Stier R, Jehn P, Johannsen H, Mu¨ ller CW, Gellrich NC, Spalthoff S. Reality or wishful thinking: Do bicycle helmets prevent facial injuries? Int J Oral Maxillofac Surg, 1: 48(9), 1235.
- Highway Code. Rules for cyclists. Published 2015. Updated , 2019. Accessed November 18, 2020. https://www. gov. 20 August.
- Goodman A, Green J, Woodcock J. The role of bicycle sharing systems in normalising the image of cycling: an observational study of London cyclists. J Transport Health.
- Esmaeilikia M, Grzebieta R, Olivier J. A systematic review of bicycle helmet laws enacted worldwide. J Australas Coll Road Saf.
- Bonander C, Nilson F, Andersson R. The effect of the Swedish bicycle helmet law for children: an interrupted time series study. J Safety Res.
- Olivier J, Boufous S, Grzebieta R. The impact of bicycle helmet legislation on cycling fatalities in Australia. Int J Epidemiol, 1197.
- Macpherson A, Spinks A. Bicycle helmet legislation for the uptake of helmet use and prevention of head injuries. Cochrane Database Syst Rev, 2008.
- Hoye, A. Recommend or mandate? A systematic review and meta-analysis of the effects of mandatory bicycle helmet leg- islation. Accid Anal Prev.
- Gross I, Weiss DJ, Eliasi E, Bala M, Hashavya S. E-bike- related trauma in children and adults. J Emerg Med, 7: 54(6).
- Broe MP, Kelly JC, Groarke PJ, Synnott K, Morris S. Cycling and spinal trauma: a worrying trend in referrals to a national spine centre. Surgeon.
- Airaksinen NK, Nurmi-Lu¨thje IS, Kataja JM, Kro¨ger HPJ, Lu¨ thje PMJ. Cycling injuries and alcohol. Injury, 9: 49(5).
- Embree TE, Romanow NT, Djerboua MS, Morgunov NJ, Bourdeaux JJ, Hagel BE. Risk factors for bicycling injuries in children and adolescents: a systematic review. Pediatrics, 2016.
- Cook R, Davidson P, Martin R; NIHR Dissemination Centre. Twenty miles per hour speed zones reduce the danger to pedestrians and cyclists. BMJ.
© 2021 by the author. The Author(s) 2021.




{kind=link}
{kind=link}