Background
Facial fractures are less common in children compared to adults.[
1] Children have an underdeveloped facial skeleton and large paranasal sinuses which lead to a disproportionaly larger cranium. This anatomical development protects the face from trauma.[
1] In the past, the National Trauma Data Bank indicated that the leading cause for facial fractures in the pediatric population was motor vehicle collisions (MVCs) with the mandible as the most common site.[
2] Since 2005, the Centers for Disease Control (CDC) noted an almost 15%
decrease in the number and rate of motor vehicle crash deaths. This decrease is likely secondary to changes in driver/passenger behaviors and vehicle safety technology.[
3]
Seat belt use among drivers and passengers increased from 71% in 2000 to 87% in 2013.[
3] Furthermore, newer safety technologies like dual front airbags have been mandated since 1998 in new car models by the National Highway Traffic Safety Administration (NHTSA).[
4] More recently, in 2006 the NHSTA introduced a wider array of performance tests to encourage the development of more sophisticated airbag triggering and deployment energy algorithms based on impacty severity, belt use, and occupant size.[
5] Nevertheless, a lag effect of these measures on the mortality of MVCs remains as older car models are replaced by newer car models over time. Previous studies have shown that the use of seatbelts and airbags significantly reduce the odds ratio of facial fractures from MVCs.[
6]
There is a paucity of longitudinal studies of the incidence of facial fractures in the pediatic population. We hypothesized that the overall incidence of pediatric facial fractures should decrease secondary to improvement in driver/passenger behaviors and vehicle safety technologies. The purpose of this study was to assess patterns of maxillofacial fractures in children at Children’s Healthcare of Atlanta (CHOA), the major pediatric trauma center in Atlanta, GA. A review of current trends is important to guide management and allocate resources for treatment of maxillofacial injuries in children.
Materials and Methods
This study was approved by the Children’s Healthcare of Atlanta IRB and all participants signed an informed consent agreement (Instutional Review Board #17-039). This was a retrospective chart of children 18 years or younger who presented to CHOA from October 2006 to September 2015. Patients were identified using International Classification of Diseases, Ninth Revision (ICD-9) diagnostic codes specific for maxillofacial trauma (i.e. codes 802.0 to 802.7, 905). September 2015 was chosen as the study period end date due to the implementation of ICD-10 codes in October 2015. Patients were included if they: (1) were aged 18 years old or younger at time of injurty, (2) presented to emergency department (ED) at CHOA from 2006 to 2015, (3) diagnosed with maxillofacial fractures [according to ICD-9 codes specific to maxillofacial trauma (e.g. 802.0-802.7, 905)], and (4) evaluated by Oral and Maxillofacial Surgery (OMS), Otolaryngology, or Plastic Surgery services. Exclusion criteria were patients with (1) incomplete medical records, (2) isolated soft tissue injuries, and/or (3) isolated dental/dentolaveolar injuries.
Medical records were reviewed to record: (1) demographics (age, gender), (2) mechanism of injury (MVC, fall, pedestrian struck, gunshot wound, sports injury, assault/abuse, other), (3) fracture location (nose, mandible, orbit, maxilla, dentoalveolar, zygoma, or complex [i.e. >2 facial bones]), and (4) yearly incidence of injury. Descriptive statistics were computed to summarize findings and overall trends.
Results
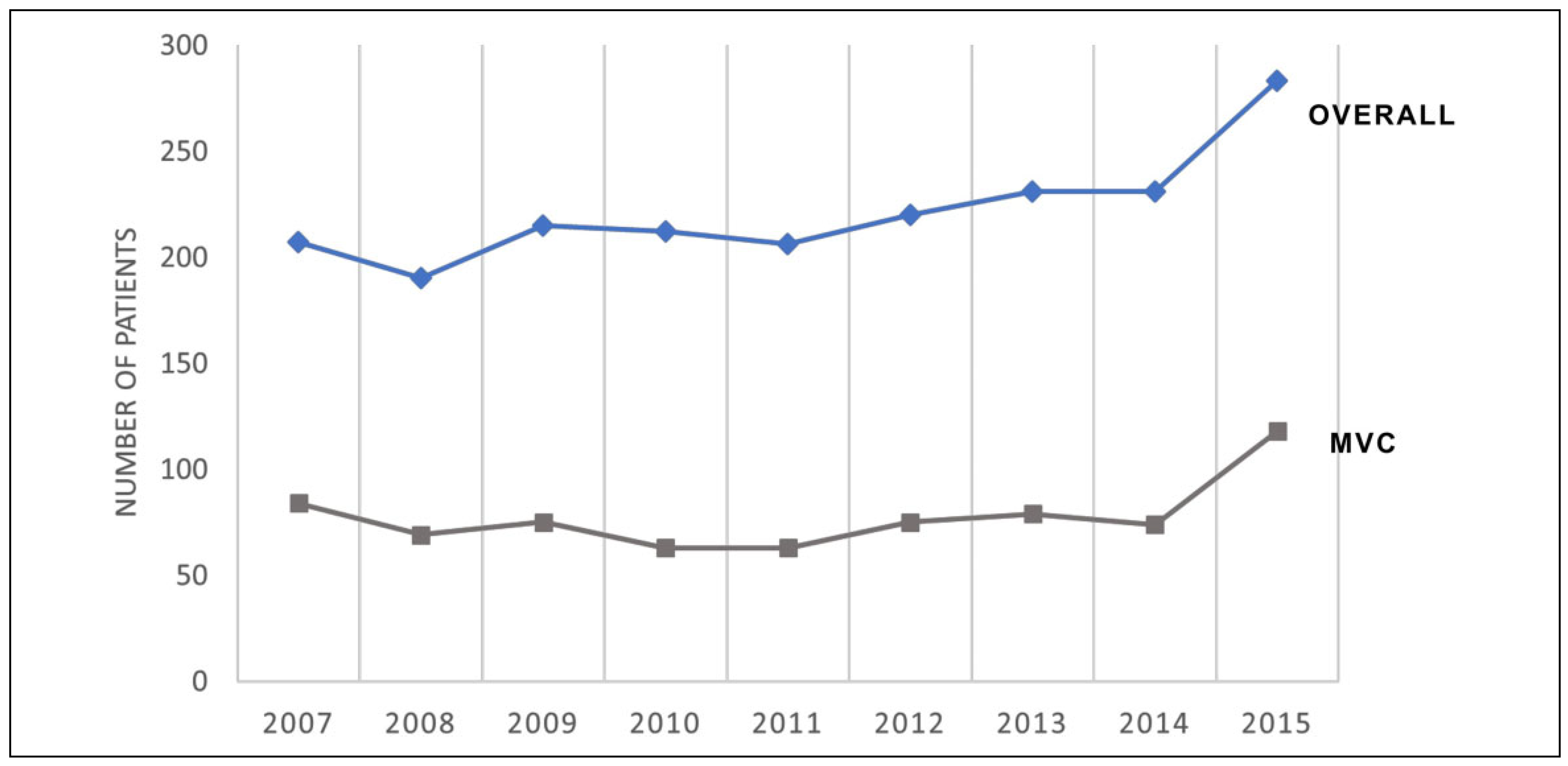
During the study period, 39,833 patients were identified. Of them, 1995 met the inclusion criteria. The majority were male (n = 1359, 68%) with an average age of 9.4 years old (range, 1 month to 18 years old). During the study period, there was an increase in the overall incidence of facial fractures as seen in
Figure 1 (207 cases in 2006-2007 to 283 cases in 2014-2015). Males had a higher incidence of assault than females (n = 185, 91% of assaults). The incidence of maxillofacial trauma increased with age with a peak incidence in 13 to 16-year-olds (n = 566, 28.3%). Younger age groups had a higher incidence of falls while older age groups had a higher incidence of MVCs, sports injury, or assault. During the years examined, there was an upward trend in MVCs as the etiology with peak incidence of facial fractures due to MVCs occurring in 2015 (84 cases in 2006-2007 to 118 cases in 2014-2015). All other mechanisms remained constant during this time period.
Mechanisms of injury were MVC (n = 597, 29.9%), fall (n = 565, 28.3%), sports injury (n = 317, 15.9%), pedestrian struck (n = 215, 10.8%), assault/abuse (n = 204, 10.2%), other (n = 81, 4.1%), and gunshot wound (n = 16, 0.8%) as seen in
Figure 2. Fracture sites were mandible (n = 519, 26%), complex or multiple sites (n = 479, 24%), nasal (n = 419, 21%), dentoalveolar (n = 279, 14%), orbit (n = 259, 13%), or maxilla (n = 40, 2%) as seen in
Figure 3.
Discussion
There are anatomical differences between pediatric and adult craniofacial skeleton: an increased ratio of cranium to the face in children which provides an anatomic protection to forces, relative strength of the facial bones in children due to lack of sinus pneumatization, and presence of unerupted tooth buds.[
1,
2] In theory, this provides protection to the craniofacial skeleton. Data from the National Trauma Bank identified 277,008 pediatric trauma patients from 2001-2005, of which, 12,739 patients or 4.6% sustained facial fractures. In this study, of the 39,833 pediatric patients that presented to the ED for maxillofacial trauma during the study period, 1995 or (5%) of patients were similarly diagnosed with a facial fracture.
Imahara et al reported that pediatric facial fractures reported in the National Trauma Data Bank more often occurred in males at 68.6% with a mean age of 12.6 years old.[
2] Owusu et al reported a 4:1 male to female ratio with a mean age of 12.5 years old.[
1] Similarly, in our study, there was a predominance of 1359 male patients (68%) with a mean age of 9.4 years old. This difference is likely due to an increased incidence of assault in males (91%) compared to females.
Previous studies reported that the most commonly fractured sites involved the mandible (32.7%), nasal bone (30.2%) and the maxillary zygoma (28.6%) (Imahara et al). Shetawi et al reported that the mandible was the most commonly fractured site at 40.7% followed by multiple or complex fractures at 26.9%.[
7] Similarily, in our cohort, the mandible was the most common site of fracture (n = 519, 26%) followed by complex fractures involving multiple sites (n = 479, 24%) and nasal bone fractures (n = 419, 21%).
The present study also showed that the overall incidence of pediatric facial fractures has been increasing with a peak in incidence during 2015. This is contrast to the trend observed in the adult population (VandeGriend et al) who noted an overall decrease in the incidence of facial fractures since the 1990s.[
4] They attributed the decline largely due to a decrease in MVCs as a direct result from seat belt usage and safer technologies in newer car models.[
4] Other studies in the literature have shown similar results in the pediatric population. Shetawi et al reported that the most common mechanism of injury for their pediatric pediatic fractures were due to assault (48.1%) followed by pedestrian struck[
7] (20.5%). Out of the 156 total patients reviewed, only 13 (8.3%) of the cases were due to MVCs.[
7] Similarly, Owusu et al reported that the mechanism of injury varied with age and sex.[
1] For patients 12 years and younger, the most frequent cause was falls, accounting for 30.3% of fractures. In teenagers (13-18 years), the most frequent cause was assault, accounting for 39.9% of fractures.[
1] Only 12.9% of cases were due to MVCs.
In our study, MVCs remained the leading cause of pediatric facial fractures (29.9%). This was similar to data from the National Trauma Data Bank that showed MVCs being the most common etiology at 55.1%.[
2] Furthermore, when mechanisms of injury were stratified over time, the incidence of facial fractures secondary to MVCs also steadily increased with a peak in 2015. This trend reflects national patterns of MVCs and pedestrians struck in the United States. Although the rate of MVCs has decreased to 15-20% since 2006,[
3] the Governor’s Office of Highway Safety and the NHTSA noted a 21.2% increase in traffic fatalities and 20.1% increase in traffic injuries in 2015 compared to 2013. This was specificed as due to more “distractions” while driving[
8] (e.g. distracted driving). Gilklich et al surveyed more than 1200 US drivers and reported that nearly 60% of respondents reported a cell phone reading or writing activity within the prior 30 days, with reading texts (48%), writing texts (33%) and viewing maps (43%) most frequently reported.[
9] Furthermore, although the rate of selt belt use has improved in the US to 87%, it is still significantly lower compared to the average of other high income countries (94%).[
10] MVCs remained the leading cause of mortality and morbidity for children in 2015.[
8] These trends are signifcant to our specialty as MVCs are predictive of more severe facial fractures as well as concomitant injuries (eg. intracranial hemorrhage, long bone fractures, spinal injuries, etc).[
7,
8,
11]
There are some limitations to this study. The study period end date of September 2015 prevented further data to assess if this peak incidence of facial fractures in 2015 continued in subsequent years. September 2015 was chosen as the study period end date due to the implementation of ICD-10 codes in October 2015. When similar ICD-10 codes were used for facial fractures, there was a drastic decrease in pediatric facial fractures, possibly reflecting a change in coding practices in the ED since the transition to ICD-10 codes. Another limitation of this study was the inclusion criteria of patients younger than 18 years old. Although patients up to 18 years old can present to CHOA, they are skeletally mature with a biomechanical distribution similar to adults compared to patients younger than 13 years old or infants. Incomplete dentition provides additional strength to the maxilla and mandible due to increased stability and elasticity of the bone.[
12] An improvement to this study would be to group patients based on their dental age and then to assess for differences in facial fracture patterns. Lastly, Georgia has since enacted the “Hands-Free Law” on July 1, 2018 to deter distractions while driving and the effect of this new legislation on pediatric facial fractures should be explored.[
10] Further studies with national data collection systems are warranted to correlate this study’s findings in trends of pediatric facial fractures across the United States.

{kind=link}
{kind=link}
{kind=link}