2. Materials and Methods
This study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline. We performed a single institution, retrospective chart review study at a level 1 trauma center. Inclusion criteria were (1) patient visits associated with International Classification of Diseases, Tenth Revision codes S02.2-S02.9 as a diagnosis of that visit; (2) patients aged 13 to 19 years at time of presentation, and (3) injury occurring between 1 October 2015, and 31 October 2017. Data analysis was conducted from 1 January 2018, to 1 March 2018, using a chi-square test of independence for independent samples with a p value of less than 0.05 was considered to indicate significance. Patients who did not meet these criteria were excluded from the study. Data fields included age, sport, fracture type, need for surgery, associated concussion, and time to return to play in days. Surgical intervention was determined due to radiographic or clinical evidence necessitating reduction of fractures. Concussion was defined via inclusion in the patient’s diagnosis as a part of the visit or explicit statement of at least 3 symptoms including headache, nausea, vomiting, amnesia, lethargy, photophobia, or hyperacusis. Regional middle school and high school sports participation data from the 2016 to 2017 and 2017 to 2018 New York State Public High School Athletic Association (NYSPHSAA) database were used to estimate the incidence of maxillofacial fractures in our study population. This study was approved by the State University of New York Upstate Medical University Institutional Review Board and was found to be exempt from review. Expedited review was obtained, allowing informed consent to be waived because no intervention was performed and no patient contact occurred while obtaining, reviewing, or analyzing the data. Data were organized in Microsoft Excel for Mac (Microsoft 2015). Analysis was performed using SPSS Statistics for Mac version 26.0 (IBM Corp).
3. Results
Initial record review revealed 1253 patients evaluated for facial fractures over the period of 1 October 2015, to 1 October 2017. Of these, 215 were between the ages of 13 and 19 years used as an initial screening criterion. Forty-two cases were identified as related to athletic competition or practice. The cases were further screened to identify injuries in middle or high school athletes. Thirty-three patients were identified and their medical records examined.
Thirty-three patients with middle or high school athletics associated maxillofacial fractures were treated at our institution during the 2-year study period (
Figure 1). Of these, 25 (76%) patients were males and 8 (24%) were females. Seventeen of the fractures were isolated nasal bone fractures (9 males, 8 females). Four mandible fractures were evaluated and treated as well as 12 midface fractures. All of the mandible and midface fractures occurred in male patients. The mandible fractures included 1 isolated ramus fracture and 3 parasymphyseal fractures in combination with either a body fracture (2) or a subcondylar fracture (1). The midface fractures included 7 zygomaticomaxillary complex (ZMC) fractures (5 isolated, 2 with orbital involvement), 3 isolated orbital fractures, 1 maxillary sinus fracture, and 1 frontal sinus fracture.
Operative intervention was required for 2 of 17 nasal bone fractures, 1 of 4 mandible fractures, and 7 of the 12 midface fractures (
Figure 2). The operative mandible fracture was placed in maxillomandibular fixation and 3 were treated conservatively with nonchewing diet. All 7 of the zygomaticomaxillary fractures underwent surgical correction. None of the isolated orbital fractures required operative intervention. There were no significant surgical complications such as surgical malunion or nonunion, wound dehiscence, or postoperative infection noted during the acute or early follow-up period.
Concussions were associated with 2 of 17 nasal bone fractures, 0 mandible fractures, and 0 midface fractures based on review of available medical records.
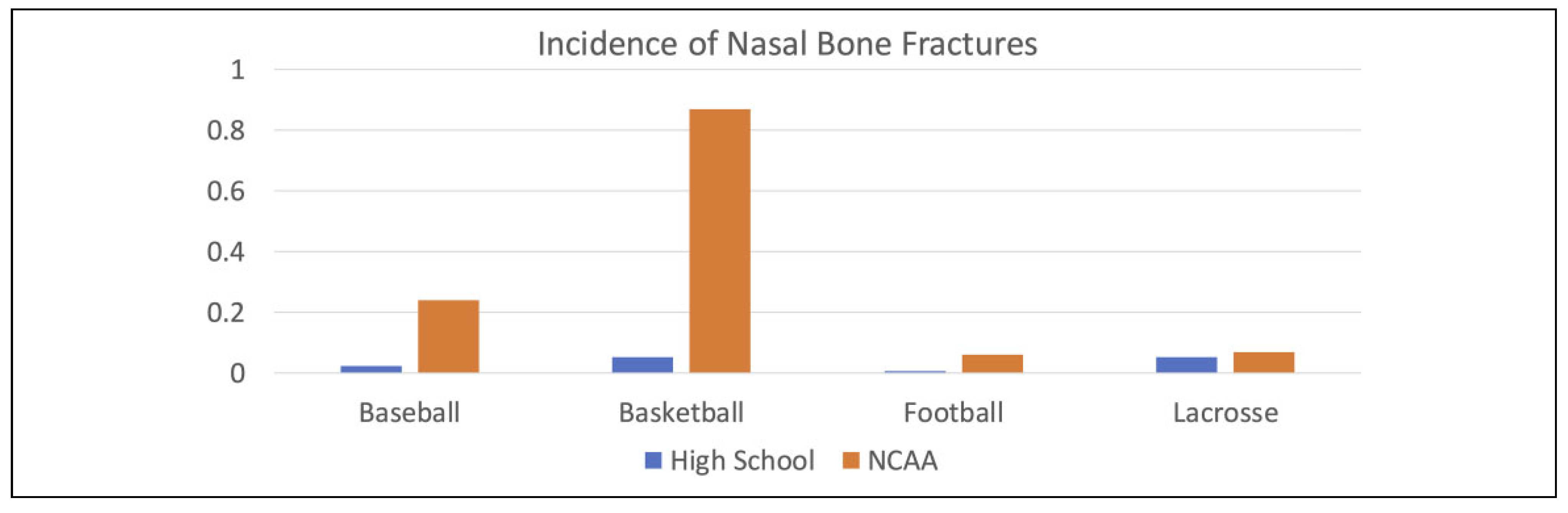
Nasal fractures occurred across a variety of sports both in males and females, most commonly playing basketball (5), soccer (3), or cheerleading (3);
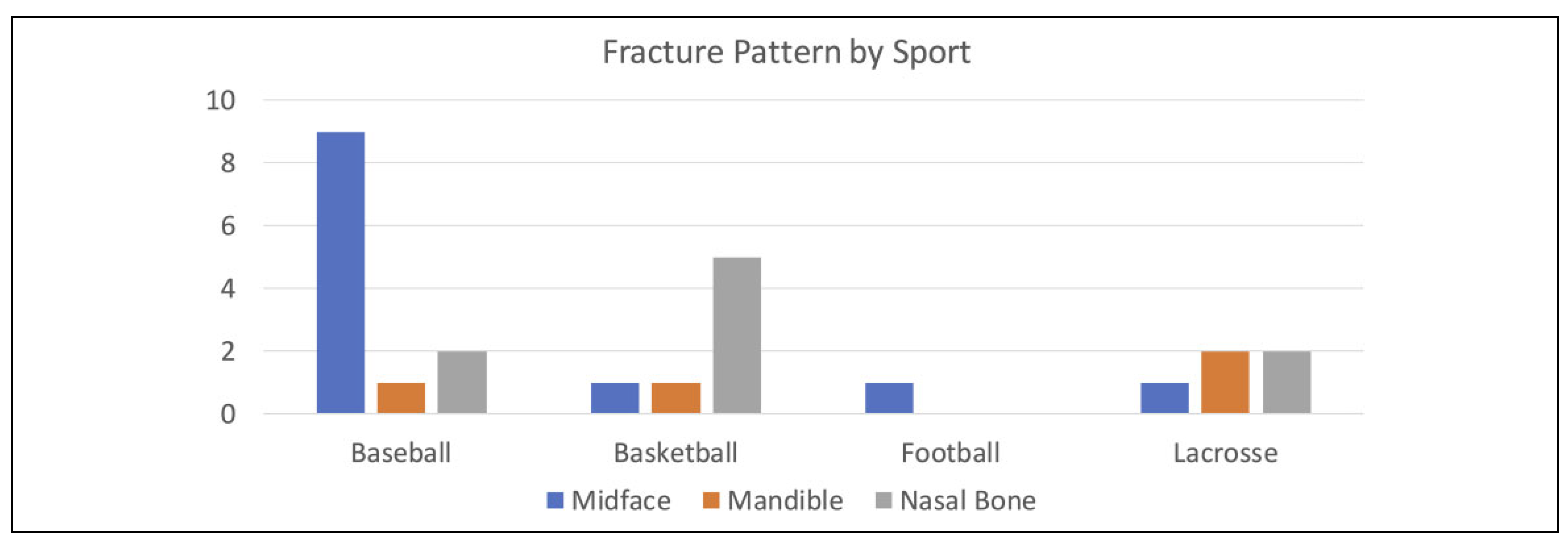
Figure 3. Mandible fractures occurred most frequently while playing lacrosse (2), followed by basketball (1), and baseball (1);
Figure 4. Midface fractures predominantly were sustained playing baseball (9), followed by basketball (1), lacrosse (1), and football (1);
Figure 5.
On average, athletes returned to full athletic participation in 25 days for nasal fractures, 53 days for mandible fractures, and 52 days for midface fractures.
Given our status as a regional referral center for maxillofacial fractures in the counties surrounding Syracuse, New York, we treat the vast majority of maxillary and mandible fractures as patients are transferred for maxillofacial trauma assessment. Nasal fractures are suspected to be more common than indicated by our data, as they are less serious and therefore less likely to be transferred to a regional trauma center emergency room. Nasal fractures were excluded from incidence calculations for this reason.
The regional referral area for our institution roughly comprises the area of Section III of the NYSPHSAA for high school sports, consisting of approximately 100 schools in 7 counties. Participation data for Section III of the NYSPHSAA in 2016 to 2017 and 2017 to 2018 showed 70,756 male participants and 62,284 female participants across all sports for middle school and high school teams. Significant association of maxillofacial fractures occurred only with males while participating in 3 sports: baseball, lacrosse, and basketball. These injuries were in the area of midface fractures (p < 0.00001) for baseball, midface fractures for basketball (p ¼ 0.003748) for basketball, and mandible fractures (p ¼ 0.002458) specifically parasymphyseal fractures (p ¼ 0.000134) for lacrosse. In those 3 sports, NYSPHSAA data showed 7463 baseball players, 9650 basketball players, and 5450 male lacrosse players participated in the 2016 to 2017 and 2017 to 2018 seasons combined.
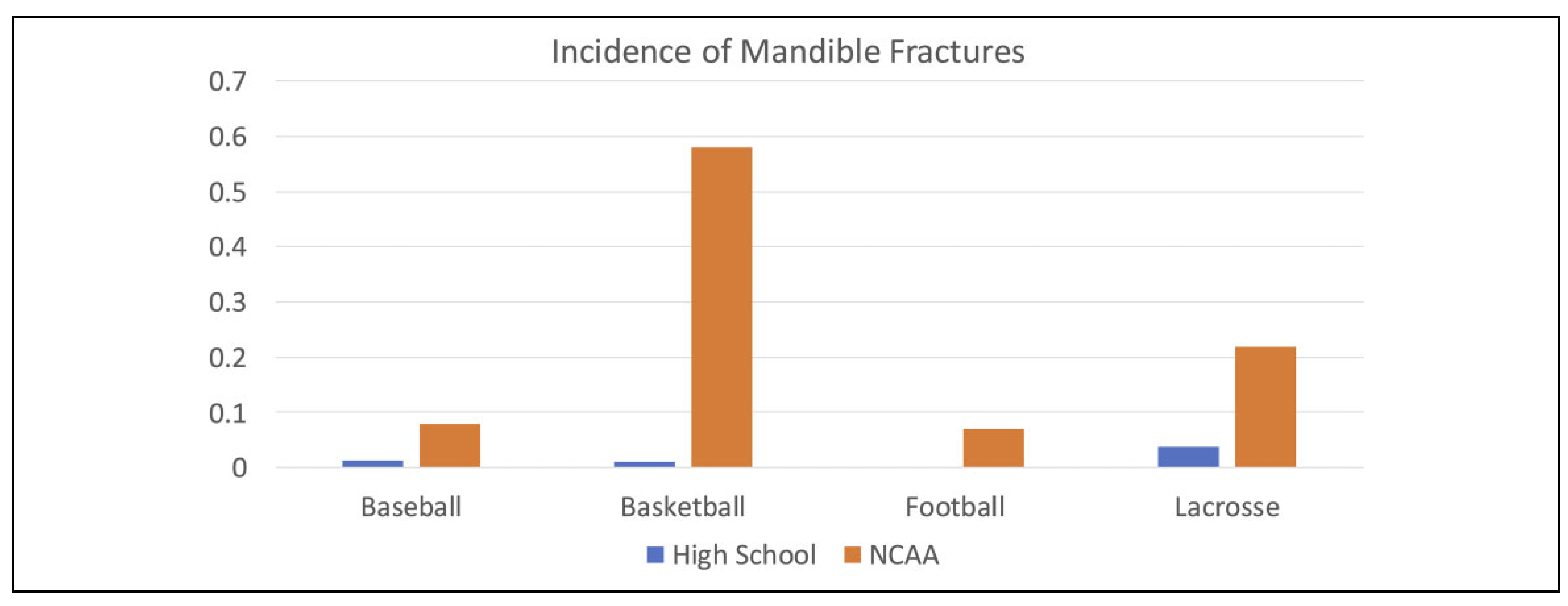
Over the 2-year study period, we treated 4 middle school or high school-aged mandible fractures that occurred playing lacrosse (2), basketball (1), and baseball (1). Annual mandible fracture risk is estimated to be 0.037% for lacrosse, 0.013% for baseball, and 0.01% for basketball participation.
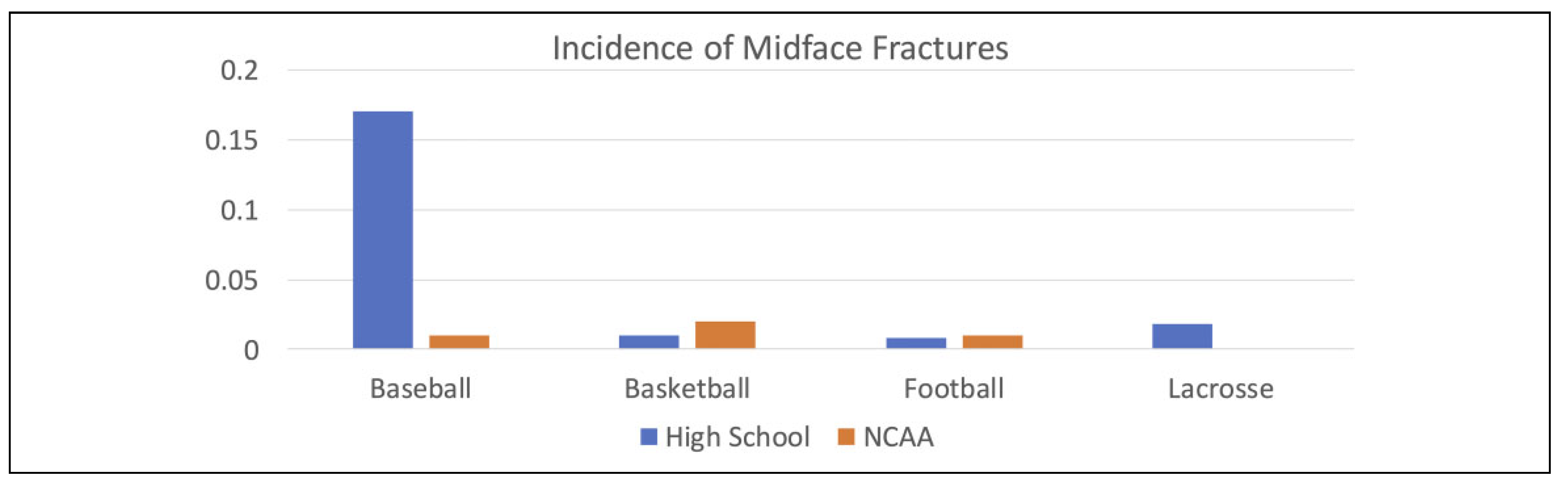
Over the same 2-year study period, we treated 12 middle and high school-aged midface (ZMC, orbit) fractures that occurred during sports participation in baseball (9), lacrosse (1), basketball (1), and football (1). Annual midface fracture risk is estimated to be 0.17% (baseball), 0.018% (lacrosse), 0.01% (basketball), and 0.008% (football).
4. Discussion
Athletics are a very popular activity among the middle and high school age-group of 13 to 19 years old. This can be seen with the NYSPHSAA survey referenced in this study, which shows over 65,000 participants annually in just 1 administrative section of New York state public high school athletics. Participation in team sports does present increased risk for injury. Previous studies have attempted to analyze the causes of facial trauma among young people and several have shown participation in sporting events as accounting for a large percentage of facial trauma, along with interpersonal violence and motor vehicle collisions [
1,
2]. While maxillofacial fractures are uncommon injuries among middle school and high school athletes, they tend to have important consequences including time lost for the athlete and potential surgical management of the fracture in young patients who may still be developing their facial skeleton leading to cosmetic or functional consequences in the future [
3,
4,
5]. Previously, studies to analyze the trends of maxillofacial injury have been focused on college-aged athletes or professional athletes due to the more thorough injury tracking of both the NCAA and professional sports leagues [
1,
3,
6,
7]. The High School Sports-Related Injury Surveillance Study (University of Colorado School of Public Health, Program for Injury Prevention, Education & Research) has been an annual survey of athletic trainers across the nation since 2005 that has attempted to analyze the types of injuries among high school athletes. This study showed an average annual incidence rate of head/face injuries to be roughly 20% of all injuries among high school athletes. However, the study does not breakdown this category of injury to site of injury and also isolated concussion is included in this injury category, likely inflating the true incidence of facial injuries reported in this study. Given the popularity of middle and high school athletics, we feel it is important to better understand the maxillofacial trauma risk related to participation in these activities in order to ensure the proper evolution of sporting equipment and rules to ensure a decreased rate of maxillofacial injury among athletes. Our original hypothesis stated that due to the decreased incidences of direct contact in the sporting event, “noncontact” or modified contact sports such as baseball would have lower rates of injury than “contact” sports such as football or lacrosse. However, our results surprisingly showed a higher rate of midface maxillofacial trauma in the modified contact or noncontact sports than contact sports.
In our study, nasal bone fractures were the most common maxillofacial injuries, followed by midface and mandibular fractures (
Figure 1). These findings are in concordance with previous studies of NCAA and professional athletes [
6,
7,
8,
9,
10,
11,
12,
13]. The specific NCAA study cited as inspiration for this study, measured the incidence rate of maxillofacial injuries by site, sport, and gender along with need for surgical intervention were measured over a 10-year period [
6]. Our data suggest that participation in some of the traditionally noncontact sports, specifically baseball, carries a higher risk of midface maxillofacial trauma (
p < 0.00001) similar to previous NCAA and professional sports population studies (
Figure 4) [
6,
7,
9,
10,
11,
12,
13]. While these sports generally limit physical contact compared to football or hockey, they also provide less protective equipment. Mechanism of injury in baseball in our data set was related to being hit in the face with a batted or thrown baseball. Batters’ helmets have been modified in recent years to better protect the lower face, though many baseball-related maxillofacial injuries occur in fielders.
In regard to mandible fractures, though low in absolute number, there was an increased rate among male lacrosse players compared to other sports (
p ¼ 0.002458), again in similar accordance with other studies highlighting NCAA and professional sports data (
Figure 3) [
1,
6,
7,
9,
10,
11,
12,
13]. Record review in these cases suggests the mechanism of injury is likely due to the lack of adequate helmet coverage over the inferior aspect of the mandible. A rising shot or a shot off the ground may inadvertently strike the exposed portion of the mandible. Helmet manufacturers are encouraged to consider this potential injury mechanism in the future research and development of protective equipment.
Moreover, another area of concern that is often associated with sports is concussions. There are several articles as well as studies that link head injuries to sporting events [
8,
14,
15,
16]. This is particularly noted with repetitive head injuries incurred during contact sports such as football. However, there are very few studies that specifically measured the incidence of concussion in patients with facial trauma as a result of athletic participation [
17,
18,
19]. Our study only revealed 2 facial fracture cases with a diagnosis of concussion based on patient medical records and symptomatology at that encounter. As a retrospective study, it is unclear if this low incidence of concussion associated with facial fractures is accurate or reflective of failure to test, diagnose, or document. Further research into the incidence rate of concussions among facial trauma patients would help identify at risk patients and potentially guide improvement of protective equipment [
5,
6,
8,
14,
20].
Finally, while this is the first study to attempt to analyze maxillofacial injuries among high school-aged athletes, there are several notable limitations to our study. First, over the 2-year study period, our sample size was limited to 33 patients who presented to our single institution for evaluation for maxillofacial trauma related to sporting events making this study similar to a case series review. While this number is low, it appears to be in line with previous studies of NCAA and professional athletes where the annual incidence rate of maxillofacial injury across the NCAA was found to be 3.4% nationwide across a group of 489,000 participants [
1,
6,
10,
11,
12,
13,
21]. Our total population size for our catchment area is roughly one-fifth the size of the NCAA population studied, so subsequently our incidence rate appears to be proportional due to size along with amount of athletic events per year. The NCAA athletics generally have longer seasons along with number and length of time per athletic event leading to increased opportunities for injury in comparison to high school and middle school athletics. However, further analysis over a longer period of time along with possible multi-institutional review could provide a larger sample size to gather additional information on maxillofacial patterns among high school and middle school athletes. Also, upon review, New York state does not keep a database of injuries that occur during athletic events that is similar to the NCAA. The only database appears to be the one cited from the University of Colorado that relies on survey results from each high school’s athletic trainer and also was noted to include concussion as a part of the category of “head/facial injuries” [
22]. Thus, this database may overestimate the incidence of maxillofacial trauma due to the inclusion of these other conditions such as concussions and skull fractures in the same category without further delineating each injury within the category as well.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}