The head and neck region is richly supplied by a network of multiple major and minor blood vessels. Thus, any penetrating injuries to the maxillofacial region demand early and prompt attention owing to the relatively high mortality rate associated with bleeding from these regional vessels. While bleeding from superficial penetrating wounds is relatively easy to treat, wounds which are deep to the investing layer of deep fascia are difficult to manage. Such bleeding from deep neck injuries represents a formidable challenge to the treating surgeon. Similarly, bleeding from the head and face is also practically impossible to control by external pressure tamponade. This is due to the presence of bony structures and the compromised condition of fragile anatomic structures like eyes, brain, and airway.
The most commonly involved vessels in penetrating head and neck injuries are the carotid artery, branches of external carotid arteries, jugular vein, and the prevertebral plexus. During emergencies, management of profuse bleeding from the deep anatomical location of neck requires great expertise. Often any attempt to explore such wounds without proper radiological investigations will be a futile and eventually increases the chances of further damage to blood vessels and cranial nerves. Furthermore, almost all the maxillofacial penetrating wounds invariably occur in regions which are not conducive to tourniquet use. In such cases, the application of a Foley catheter can effectively control bleeding from the vessels which are inaccessible clinically for ligation. [
1] However, literature regarding the use of this simple technique is scarce and is limited to only isolated case reports. [
2,
3] Hence, this study retrospectively evaluates the efficacy of Foley catheter tamponade in controlling hemorrhage in deep penetrating and perforating wounds of maxillofacial region in austere condition. It also evaluated the duration of application, safety, and complications associated with the balloon tamponade in emergency.
Materials and Methods
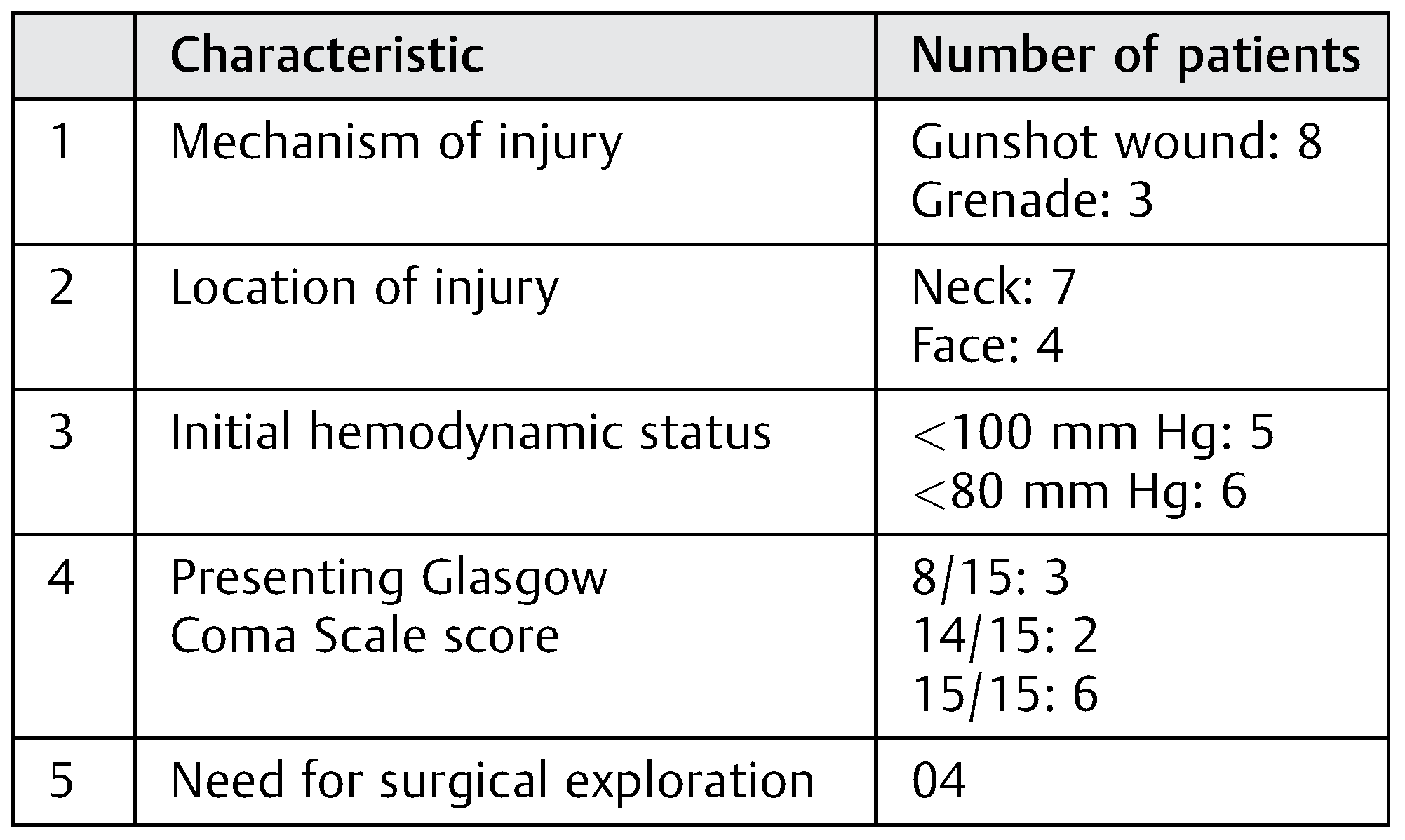
This retrospective case series evaluated a total of 26 penetrating maxillofacial injuries reported to a military trauma hospital during 2015–2017. All patients were males with age ranges between 24 and 39 years. Etiologies of these penetrating injuries were gunshots and grenade blasts sustained during the counterinsurgency operations. Data collection was done from the hospital records regarding the mode of injury, Glasgow Coma Scale and hemodynamic status at the time of admission, type and location of injury, method of hemorrhage control, and need for surgical exploration (
Table 1). The patients were managed in the emergency department according to the advance trauma and life support guidelines. Foley catheter was used to arrest hemorrhage in 11 patients with penetrating injury. The Foley (18–20 Fr) is slowly inserted into the penetrating wound and inflated with saline. The margin of the wound is then closed with sutures tightly for maintaining the Foley in place. The catheter is generally kept for 72 hours without any complication.
Results
The management of hemorrhage was effective with Foley catheter in 10 out of 11 patients (91%;
Figure 1,
Figure 2 and
Figure 3). One patient who failed to respond had a bullet lodged inside the neck (
Figure 4). In this case, the Foley was prematurely removed to prevent further damage to the great vessels. This was followed by management with surgical exploration and repair of internal jugular vein (IJV). Late surgical exploration was done in three cases after CT angiogram for major vessel injury within 24 hours. One case had external carotid injury above the level of facial artery, and the remaining two had IJV injuries. The carotid injury was managed by ligation and IJV injuries were managed by surgical repair by a vascular surgeon. Seven out of 10 cases did not require any intervention for bleeding and the catheter was carefully removed after 72 hours. There was no neurological deficit or complication associated with the use of Foley catheter.
Discussion
The rate of morbidity and mortality in penetrating injury is very high as compared with routine maxillofacial injuries. This is presumably due to the delayed diagnosis and damage to the deep seated major blood vessels of head and neck. Hemorrhage from maxillofacial penetrating injuries is a significant cause of mortality, second only to airway obstruction. [
3] Hence, the most critical aspect in the management of a penetrating injury is establishing an airway and control of hemorrhage. Traditionally, bleeding from the maxillofacial region is commonly controlled by gauze packing, external digital compression, and balloon tamponade. Most of the hemorrhages from the superficial neck wounds are easily assessable for direct pressure. However, gauze packing and external pressure are generally considered to be less reliable in deep head and neck wounds. In such emergency scenarios, Foley catheter balloon tamponade facilitates quick, easy, and predictable control of hemorrhage. It can be used in conjunction with hemostatic gauze which further increases the effectiveness of the procedure. Additionally, it prevents hematoma formation and tissue collapse until definitive management of the injury is undertaken.
In the present series, the use of Foley catheter resulted in complete elimination of bleeding in 10 patients thereby aiding in hemodynamic stabilization. It also rendered a grace period to carry out CT angiography to rule out major vessel injury within minimum time duration without deteriorating the vitals of the patient. The most important advantage of balloon tamponade is that it requires minimal or no training for its use in emergency scenarios. The average time required for placement of Foley catheter is less than 1 minute. In the present study, we have achieved hemostasis in all our patients but one (n = 10). Nonetheless, the one patient who did not respond had a bullet lodged inside the neck; therefore, the authors had to remove the catheter prematurely to prevent inadvertent damage to the vital structure by the sharp bullet. Furthermore, the case has been managed by open surgical exploration and repair of IJV.
Once the catheter is applied, the wound around the catheter is closed tightly to prevent slippage of the catheter and to achieve adequate pressure for hemostasis. Afterward, the distal end of Foley is tied with a thread to prevent back flow of the blood to the exterior. A radiographic investigation, preferably a CT angiogram, is requested to rule out the cause of bleeding. [
4] Considering the magnitude and severity of the injury and asper radiological finding, the patient is further managed by surgical exploration or close monitoring for 72 hours. If the patient is stable and no evidence of bleeding is seen, the catheter is slowly removed after a period of 72 hours. [
5] Treatment strategies that may include a wait-and-watch policy or a more radical open exploration approach is usually the preference of the individual surgeon. However, when in doubt, it is advised to do a surgical exploration, provided adequate resources are available once the patient is stabilized.
Most penetrating injuries in within the neck are easily amenable to Foley catheter tamponade. However, through and through perforating injuries are quite unpredictable and may call for the use of two catheters from both the ends. If one catheter is found to be inadequate, two catheters can be used to achieve adequate hemostasis. In cases of grave injuries where bleeding cannot be managed by balloon tamponade, open exploration or angiography and selective embolization of the involved vessel should be implemented. Nevertheless, the use of transarterial embolization often results in complications such as facial nerve palsy, necrosis of tongue, blindness, and migration of emboli, as well as stroke in nearly 50% of patients. [
6] Although surgical exploration and ligation of the carotid is possible, it is almost always unproductive in an emergency situation due to multiple collaterals in the head and neck region. Unlike other methods of hemorrhage control, the use of Foley catheter results in both proximal and distal control of hemorrhage. Generally, a volume of 10 mL is sufficient to arrest bleeding in penetrating injuries. This will create adequate pressure on the adjacent tissues without affecting the microcirculation. However, depending on the magnitude of bleeding, we can inflate the balloon up to 30 mL without failure of balloon.
Weppner [
7] in his study noted one case of cerebral ischemia secondary to Foley catheter application in a case of life-threatening hemorrhage from the internal carotid artery. The authors sated that factors like preoperative neurological status, hemorrhagic shock, and profuse bleeding from the carotid system may be associated with neurological deficits in such patients. The reason for stroke in one patient in his series was due to carotid artery dissection. Shuker [
3] stated that Foley catheter tamponade also prevents complications like air embolism resulting from IJV injuries.
There are no particular contraindications for the application of balloon tamponade in penetrating injuries. The complication rate associated with the use of balloon tamponade is relatively low. However, this technique should be executed with caution in penetrating injuries with comminution of nasoorbitoethmoid region. In an attempt to control hemorrhage, overzealous balloon dilatation may push the fractured fragments of bone into the orbit or intracranially, increasing morbidity. Likewise when the catheter is used in injuries near the vicinity of airway, it should be inflated with air rather than saline. This will prevent accidental spillage of saline into the airway if puncture of balloon occurs.
Conclusion
Penetrating head and neck injuries are relatively common. This subset of maxillofacial trauma results in life-threatening vascular and neural injuries. The outcome of the present study and existing literature supports the use of this technique in the management of hemorrhage. Even though the number of studies and sample size are less, the results are quite encouraging. Our experience suggests that this is a very reliable technique and can be used in emergency without causing any collateral damage.





{kind=link}
{kind=link}
{kind=link}
{kind=link}