
CS12192, a Novel JAK3/JAK1/TBK1 Inhibitor, Synergistically Enhances the Anti-Inflammation Effect of Methotrexate in a Rat Model of Rheumatoid Arthritis

 , , and
, , and
Abstract
1. Introduction
2. Results
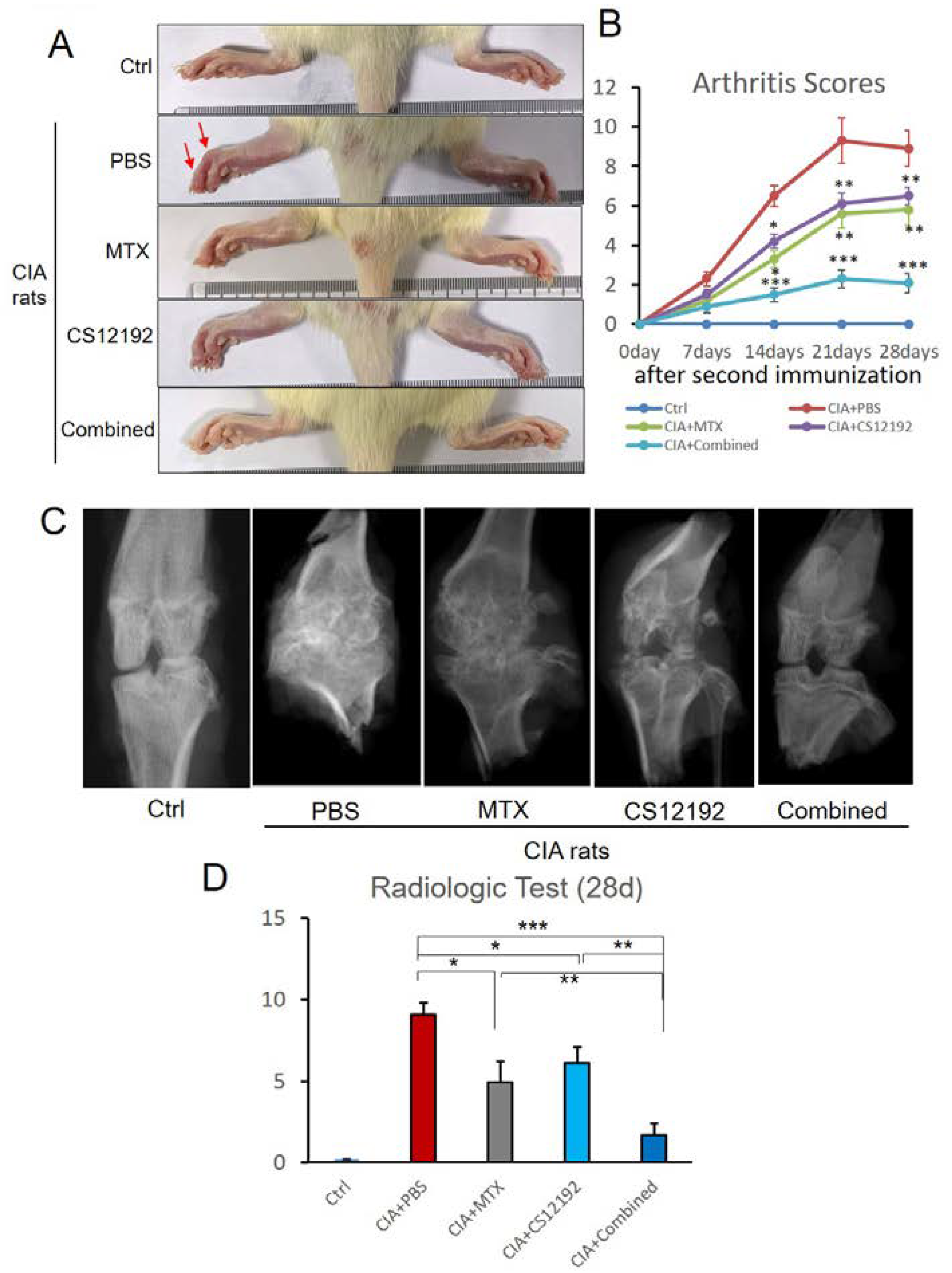
2.1. CS12192, Similar to MTX, Has a Therapeutic Effect on Arthritis Score, Joint Pathological Damage, and Serum Biomarkers in CIA Rats, Which Is Further Improved by the Combined Treatment with CS12192 and MTX
2.2. Combination Treatment with CS12192 and MTX produces a Better Inhibitory Effect on Joint Inflammation by Inducing Treg and M2 while Suppressing M1 Immune Responses in Synovial Tissues
2.3. Combination Treatment with CS12192 and MTX Produces a Better Inhibitory Effect on Joint Articular Cartilage Degradation
3. Discussion
4. Materials and Methods
4.1. Collagen-Induced Arthritis Model in Rats
4.2. Assessment of Joint Arthritis
4.3. X-ray Examination
4.4. Histopathological Examination
4.5. Immunofluorescent Staining
4.6. Measurement of Serum Rheumatoid Markers and Pro-Inflammatory Cytokines in Joint Fluids by ELISA
4.7. RNA Extraction and Real-Time PCR Analysis
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Firestein, G.S. Evolving concepts of rheumatoid arthritis. Nature 2003, 423, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Giannini, D.; Antonucci, M.; Petrelli, F.; Bilia, S.; Alunno, A.; Puxeddu, I. One year in review 2020: Pathogenesis of rheumatoid arthritis. Clin. Exp. Rheumatol. 2020, 38, 387–397. [Google Scholar] [PubMed]
- Jones, G.; Nash, P.; Hall, S. Advances in rheumatoid arthritis. Med. J. Aust. 2017, 206, 221–224. [Google Scholar] [CrossRef] [PubMed]
- Firestein, G.S.; McInnes, I.B. Immunopathogenesis of Rheumatoid Arthritis. Immunity 2017, 46, 183–196. [Google Scholar] [CrossRef]
- Emery, P.; Luqmani, R.; Gordon, C. Disease-modifying antirheumatic drugs in rheumatoid arthritis: Current concepts. Br. J. Clin. Pract. 1994, 48, 82–86. [Google Scholar]
- Haibel, H.; Specker, C. Disease-modifying anti-rheumatic drugs in rheumatoid arthritis and ankylosing spondylitis. Clin. Exp. Rheumatol. 2009, 27, S159–S163. [Google Scholar]
- Lin, Y.J.; Anzaghe, M.; Schulke, S. Update on the Pathomechanism, Diagnosis, and Treatment Options for Rheumatoid Arthritis. Cells 2020, 9, 880. [Google Scholar] [CrossRef]
- Lopez-Olivo, M.A.; Siddhanamatha, H.R.; Shea, B.; Tugwell, P.; Wells, G.A.; Suarez-Almazor, M.E. Methotrexate for treating rheumatoid arthritis. Cochrane Database Syst. Rev. 2014, 6, CD000957. [Google Scholar] [CrossRef]
- Borchers, A.T.; Keen, C.L.; Cheema, G.S.; Gershwin, M.E. The use of methotrexate in rheumatoid arthritis. Semin. Arthritis Rheum. 2004, 34, 465–483. [Google Scholar] [CrossRef]
- Alarcon, G.S. Methotrexate use in rheumatoid arthritis. A Clinician’s perspective. Immunopharmacology 2000, 47, 259–271. [Google Scholar] [CrossRef]
- Wessels, J.A.; Huizinga, T.W.; Guchelaar, H.J. Recent insights in the pharmacological actions of methotrexate in the treatment of rheumatoid arthritis. Rheumatology 2008, 47, 249–255. [Google Scholar] [CrossRef] [PubMed]
- Mazouyes, A.; Clay, M.; Bernard, A.C.; Gaudin, P.; Baillet, A. Efficacy of triple association methotrexate, sulfasalazine and hydroxychloroquine in early treatment of rheumatoid arthritis with insufficient response to methotrexate: Meta-analysis of randomized controlled trials. Jt. Bone Spine 2017, 84, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Furst, D.E. The combination of methotrexate, sulfasalazine and hydroxychloroquine is highly effective in rheumatoid arthritis. Clin. Exp. Rheumatol. 1999, 17, 39–40. [Google Scholar]
- Sarzi-Puttini, P.; D’Ingianna, E.; Fumagalli, M.; Scarpellini, M.; Fiorini, T.; Cherie-Ligniere, E.L.; Panni, B.; Fiorentini, F.; Corbelli, V.; Beyene, N.B.; et al. An open, randomized comparison study of cyclosporine A, cyclosporine A + methotrexate and cyclosporine A + hydroxychloroquine in the treatment of early severe rheumatoid arthritis. Rheumatol. Int. 2005, 25, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Shan, S.; Zhou, Y.; Yu, J.; Yang, Q.; Pan, D.; Wang, Y.; Li, L.; Zhu, J.; Zhang, Y.; Huang, S.; et al. Therapeutic treatment of a novel selective JAK3/JAK1/TBK1 inhibitor, CS12192, in rat and mouse models of rheumatoid arthritis. Int. Immunopharmacol. 2019, 77, 105914. [Google Scholar] [CrossRef] [PubMed]
- Yu, T.; Yi, Y.S.; Yang, Y.; Oh, J.; Jeong, D.; Cho, J.Y. The pivotal role of TBK1 in inflammatory responses mediated by macrophages. Mediat. Inflamm. 2012, 2012, 979105. [Google Scholar] [CrossRef] [PubMed]
- Hasan, M.; Yan, N. Therapeutic potential of targeting TBK1 in autoimmune diseases and interferonopathies. Pharmacol. Res. 2016, 111, 336–342. [Google Scholar] [CrossRef]
- Ciobanu, D.A.; Poenariu, I.S.; Cringus, L.I.; Vreju, F.A.; Turcu-Stiolica, A.; Tica, A.A.; Padureanu, V.; Dumitrascu, R.M.; Banicioiu-Covei, S.; Dinescu, S.C.; et al. JAK/STAT pathway in pathology of rheumatoid arthritis (Review). Exp. Ther. Med. 2020, 20, 3498–3503. [Google Scholar] [CrossRef]
- Malemud, C.J. The role of the JAK/STAT signal pathway in rheumatoid arthritis. Ther. Adv. Musculoskelet. Dis. 2018, 10, 117–127. [Google Scholar] [CrossRef]
- Malemud, C.J. Negative Regulators of JAK/STAT Signaling in Rheumatoid Arthritis and Osteoarthritis. Int. J. Mol. Sci. 2017, 18, 484. [Google Scholar] [CrossRef]
- Norman, P. Selective JAK inhibitors in development for rheumatoid arthritis. Expert Opin. Investig. Drugs 2014, 23, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Boissier, M.C.; Assier, E.; Biton, J.; Denys, A.; Falgarone, G.; Bessis, N. Regulatory T cells (Treg) in rheumatoid arthritis. Jt. Bone Spine 2009, 76, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Fox, D.A. Targeting IL-17 and Th17 cells in rheumatoid arthritis. Rheum. Dis. Clin. N. Am. 2010, 36, 345–366. [Google Scholar] [CrossRef] [PubMed]
- Lin, X.L.; Lv, J.J.; Lv, J.; Di, C.X.; Zhang, Y.J.; Zhou, T.; Liu, J.L.; Xia, Z.W. Heme oxygenase-1 directly binds STAT3 to control the generation of pathogenic Th17 cells during neutrophilic airway inflammation. Allergy 2017, 72, 1972–1987. [Google Scholar] [CrossRef]
- Tardito, S.; Martinelli, G.; Soldano, S.; Paolino, S.; Pacini, G.; Patane, M.; Alessandri, E.; Smith, V.; Cutolo, M. Macrophage M1/M2 polarization and rheumatoid arthritis: A systematic review. Autoimmun. Rev. 2019, 18, 102397. [Google Scholar] [CrossRef]
- Quero, L.; Tiaden, A.N.; Hanser, E.; Roux, J.; Laski, A.; Hall, J.; Kyburz, D. miR-221-3p Drives the Shift of M2-Macrophages to a Pro-Inflammatory Function by Suppressing JAK3/STAT3 Activation. Front. Immunol. 2019, 10, 3087. [Google Scholar] [CrossRef]
- Loetscher, P.; Seitz, M.; Clark-Lewis, I.; Baggiolini, M.; Moser, B. Monocyte chemotactic proteins MCP-1, MCP-2, and MCP-3 are major attractants for human CD4+ and CD8+ T lymphocytes. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 1994, 8, 1055–1060. [Google Scholar] [CrossRef]
- Iikuni, N.; Okamoto, H.; Yoshio, T.; Sato, E.; Kamitsuji, S.; Iwamoto, T.; Momohara, S.; Taniguchi, A.; Yamanaka, H.; Minota, S.; et al. Raised monocyte chemotactic protein-1 (MCP-1)/CCL2 in cerebrospinal fluid of patients with neuropsychiatric lupus. Ann. Rheum. Dis. 2006, 65, 253–256. [Google Scholar] [CrossRef]
- Koch, A.E.; Kunkel, S.L.; Harlow, L.A.; Johnson, B.; Evanoff, H.L.; Haines, G.K.; Burdick, M.D.; Pope, R.M.; Strieter, R.M. Enhanced production of monocyte chemoattractant protein-1 in rheumatoid arthritis. J. Clin. Investig. 1992, 90, 772–779. [Google Scholar] [CrossRef]
- Harigai, M.; Hara, M.; Yoshimura, T.; Leonard, E.J.; Inoue, K.; Kashiwazaki, S. Monocyte chemoattractant protein-1 (MCP-1) in inflammatory joint diseases and its involvement in the cytokine network of rheumatoid synovium. Clin. Immunol. Immunopathol. 1993, 69, 83–91. [Google Scholar] [CrossRef]
- Straub, R.H.; Rauch, L.; Rauh, L.; Pongratz, G. Sympathetic inhibition of IL-6, IFN-gamma, and KC/CXCL1 and sympathetic stimulation of TGF-beta in spleen of early arthritic mice. Brain Behav. Immun. 2011, 25, 1708–1715. [Google Scholar] [CrossRef] [PubMed]
- Ritzman, A.M.; Hughes-Hanks, J.M.; Blaho, V.A.; Wax, L.E.; Mitchell, W.J.; Brown, C.R. The chemokine receptor CXCR2 ligand KC (CXCL1) mediates neutrophil recruitment and is critical for development of experimental Lyme arthritis and carditis. Infect. Immun. 2010, 78, 4593–4600. [Google Scholar] [CrossRef]
- Tseng, S.; Reddi, A.H.; Di Cesare, P.E. Cartilage Oligomeric Matrix Protein (COMP): A Biomarker of Arthritis. Biomark. Insights 2009, 4, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Posey, K.L.; Hecht, J.T. The role of cartilage oligomeric matrix protein (COMP) in skeletal disease. Curr. Drug Targets 2008, 9, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Pardo, A.; Selman, M. MMP-1: The elder of the family. Int. J. Biochem. Cell Biol. 2005, 37, 283–288. [Google Scholar] [CrossRef]
- Bode, W.; Fernandez-Catalan, C.; Grams, F.; Gomis-Ruth, F.X.; Nagase, H.; Tschesche, H.; Maskos, K. Insights into MMP-TIMP interactions. Ann. N. Y. Acad. Sci. 1999, 878, 73–91. [Google Scholar] [CrossRef]
- Vincenti, M.P. The matrix metalloproteinase (MMP) and tissue inhibitor of metalloproteinase (TIMP) genes. Transcriptional and posttranscriptional regulation, signal transduction and cell-type-specific expression. Methods Mol. Biol. 2001, 151, 121–148. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Fisher, K.H.; Snowden, J.A.; Danson, S.J.; Brown, S.; Zeidler, M.P. Methotrexate Is a JAK/STAT Pathway Inhibitor. PLoS ONE 2015, 10, e0130078. [Google Scholar] [CrossRef] [PubMed]
- Gremese, E.; Alivernini, S.; Tolusso, B.; Zeidler, M.P.; Ferraccioli, G. JAK inhibition by methotrexate (and csDMARDs) may explain clinical efficacy as monotherapy and combination therapy. J. Leukoc. Biol. 2019, 106, 1063–1068. [Google Scholar] [CrossRef]
- Brand, D.D.; Latham, K.A.; Rosloniec, E.F. Collagen-induced arthritis. Nat. Protoc. 2007, 2, 1269–1275. [Google Scholar] [CrossRef]
- Bai, L.; Bai, Y.; Yang, Y.; Zhang, W.; Huang, L.; Ma, R.; Wang, L.; Duan, H.; Wan, Q. Baicalin alleviates collageninduced arthritis and suppresses TLR2/MYD88/NFkappaB p65 signaling in rats and HFLSRAs. Mol. Med. Rep. 2020, 22, 2833–2841. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Zhang, T.; Chen, J.; Cheng, W.; Chen, J.; Zheng, Z.; Lin, J.; Zhu, G.; Zhang, Y.; Bai, X.; et al. Downregulation of Hypoxia-Inducible Factor-1alpha by RNA Interference Alleviates the Development of Collagen-Induced Arthritis in Rats. Mol. Ther. Nucleic Acids 2020, 19, 1330–1342. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.S.; Hu, C.Y.; Chan, H.Y.; Liew, Y.Y.; Huang, H.P.; Lepescheux, L.; Bastianelli, E.; Baron, R.; Rawadi, G.; Clement-Lacroix, P. Anti-rheumatic activities of histone deacetylase (HDAC) inhibitors in vivo in collagen-induced arthritis in rodents. Br. J. Pharmacol. 2007, 150, 862–872. [Google Scholar] [CrossRef] [PubMed]
- Slaoui, M.; Fiette, L. Histopathology procedures: From tissue sampling to histopathological evaluation. Methods Mol. Biol. 2011, 691, 69–82. [Google Scholar] [CrossRef]
- Wang, C.R.; Chen, S.Y.; Wu, C.L.; Liu, M.F.; Jin, Y.T.; Chao, L.; Chao, J. Prophylactic adenovirus-mediated human kallistatin gene therapy suppresses rat arthritis by inhibiting angiogenesis and inflammation. Arthritis Rheum. 2005, 52, 1319–1324. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group Name and Number of Rats | Day 0 (First Immunization) | Day 7 (Second Immunization and Stat Point of Treatment) | Day 35 |
|---|---|---|---|
| Untreated Group (5) | Normal rats | Normal rats | End of Experiments |
| CIA * group (10) | CII-IFA * | CII-IFA+PBS * (1 ml/qd *) | |
| MTX * group (10) | CII-IFA | CII-IFA +MTX (0.2 mg/kg/qd) | |
| CS12192 group (10) | CII-IFA | CII-IFA +CS12192 (40 mg/kg/bid *) | |
| MTX + CS1219 group (10) | CII-IFA | CII-IFA +MTX (0.2 mg/kg/qd) + CS12192 (40 mg/kg/qd) |
| Gene (Rat) | Forward (5′-3′) | Reverse (5′-3′) |
|---|---|---|
| TNF-α | GTCGTAGCAAACCACCAAGC | CCACCAGTTGGTTGTCTTTGA |
| IL-1β | CTGCCAAGTCAGGTCTCTCA | AGGTAAGTGGTTGCCTGTCA |
| CCL2 | CCTGCTGCTACTCATTCACTG | ACAGCTTCTTTGGGACACCT (94) |
| IL-6 | AGTGGCTAAGGACCAAGACC | ACCACAGTGAGGAATGTCCA (136) |
| CXCL1 | CTCCAGCCACACTCCAACAGA | CACCCTAACACAAAACACGAT |
| IL-17a | GAAGGCCCTCAGACTACCTC | GTGCCTCCCAGATCACAGAA (96) |
| Comp | GGGATGGACACCAAGACTCC | TCATCACAGGCATCACCCTT (97) |
| MMP9 | CCCTACTGCTGGTCCTTCTG | CTTCCAATACCGACCGTCCT(36) |
| IL-1R | TTCAGGGCACACATGTCCTA | ATGATCTGGTGGCAGTCACA (126) |
| Timp-1 | CATGGAGAGCCTCTGTGGAT | TATGCCAGGGAACCAGGAAG (125) |
| β-actin | CAACGGCTCCGGCATGTGC | CTCTTGCTCTGGGCCTCG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, Z.; Hu, Y.; Dai, J.; He, L.; He, J.; Xu, B.; Han, X.; Zhong, F.; Lan, H.; Wang, Q. CS12192, a Novel JAK3/JAK1/TBK1 Inhibitor, Synergistically Enhances the Anti-Inflammation Effect of Methotrexate in a Rat Model of Rheumatoid Arthritis. Int. J. Mol. Sci. 2022, 23, 13394. https://doi.org/10.3390/ijms232113394
Fang Z, Hu Y, Dai J, He L, He J, Xu B, Han X, Zhong F, Lan H, Wang Q. CS12192, a Novel JAK3/JAK1/TBK1 Inhibitor, Synergistically Enhances the Anti-Inflammation Effect of Methotrexate in a Rat Model of Rheumatoid Arthritis. International Journal of Molecular Sciences. 2022; 23(21):13394. https://doi.org/10.3390/ijms232113394
Chicago/Turabian StyleFang, Zhengyu, Yiping Hu, Jiajing Dai, Lianhua He, Juan He, Bihua Xu, Xinle Han, Fubo Zhong, Huiyao Lan, and Qingwen Wang. 2022. "CS12192, a Novel JAK3/JAK1/TBK1 Inhibitor, Synergistically Enhances the Anti-Inflammation Effect of Methotrexate in a Rat Model of Rheumatoid Arthritis" International Journal of Molecular Sciences 23, no. 21: 13394. https://doi.org/10.3390/ijms232113394
APA StyleFang, Z., Hu, Y., Dai, J., He, L., He, J., Xu, B., Han, X., Zhong, F., Lan, H., & Wang, Q. (2022). CS12192, a Novel JAK3/JAK1/TBK1 Inhibitor, Synergistically Enhances the Anti-Inflammation Effect of Methotrexate in a Rat Model of Rheumatoid Arthritis. International Journal of Molecular Sciences, 23(21), 13394. https://doi.org/10.3390/ijms232113394