
Budgetary Allocations and Government Response to COVID-19 Pandemic in South Africa and Nigeria


Abstract
:1. Introduction
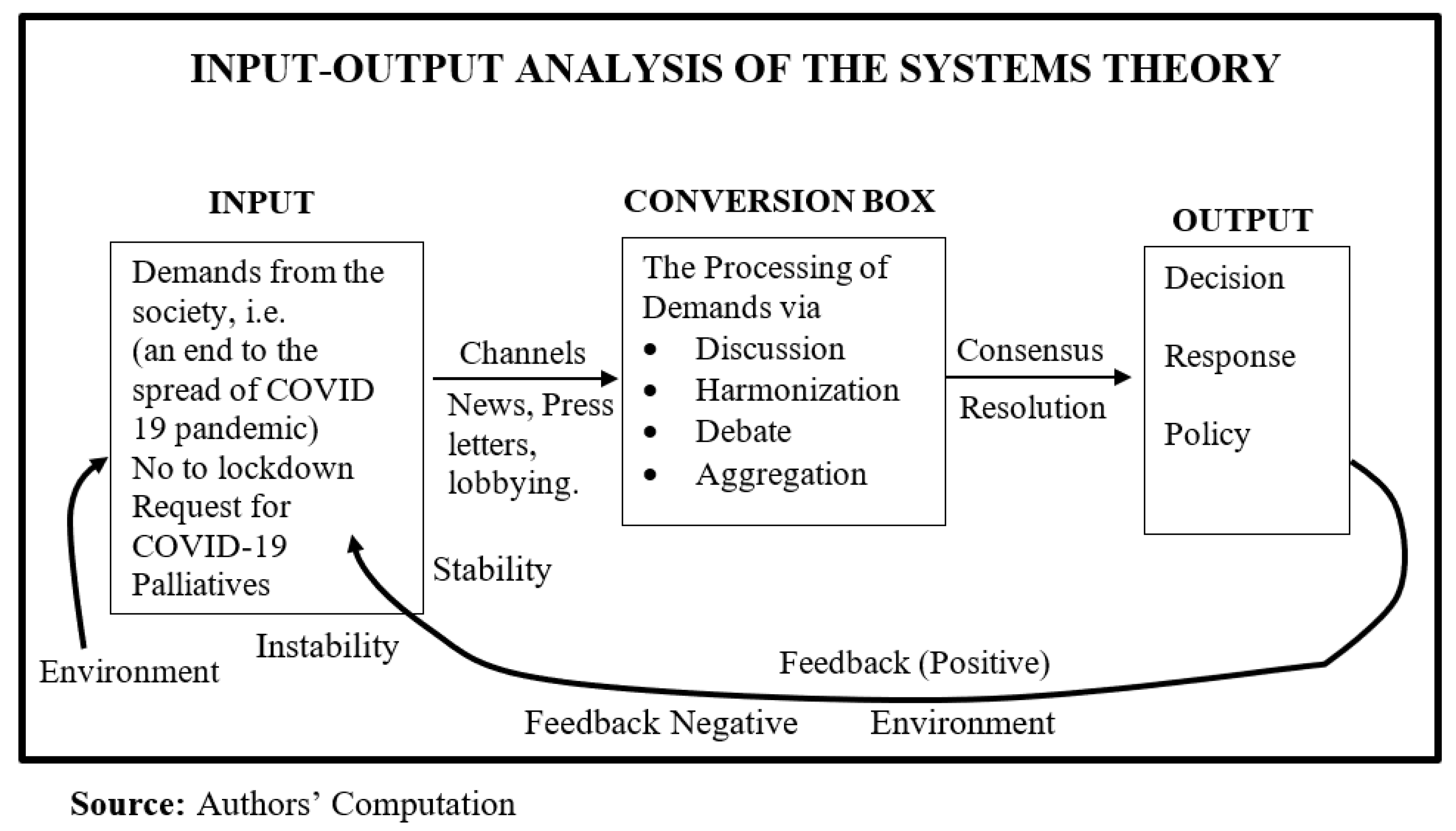
2. Theoretical Explanation of the Nexus between Budgetary Allocations and the Response of the Government to the COVID-19 Pandemic
3. Mapping the Nexus between Budgetary Allocation and the Response of the Government to the COVID-19 Pandemic in South Africa and Nigeria
4. South African Response Perspective
4.1. The State of the Budget
4.2. The Nigerian Response Perspective
5. Highlighting Possible “Takeaways” in the Response Strategy of South Africa and Nigeria to the COVID-19 Pandemic
6. Conclusions
Limitations and Implications
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
| 1 | Human Right Watch. COVID-19 Exposes Healthcare Shortfalls. 2020. Available online https://www.hrw.org/news/2020/06/08/africa-COVID-19-exposes-healthcare-shortfalls (accessed on 15 November 2021). |
| 2 | World Bank. COVID-19 to Plunge Global Economy into Worst Recession since World War II. Press Release, 8 June 2020. Washington DC. Available online: https://www.worldbank.org/en/news/press-release/2020/06/08/covid-19-to-plunge-global-economy-into-worst-recession-since-world-war-ii (accessed on 17 April 2022). |
| 3 | South Africa National Treasury. Building a Bridge to Recovery beyond COVID-19. 2020. Available online: https://www.google.com/search?sxsrf=ALeKk022ludwcNGreU9ax6YH5DDG1yROGg%3A1605234693409&sou (accessed on 13 November 2021). |
| 4 | Okunola, A. 2020. Five Challenges facing health care workers in Nigeria as they tackle COVID-19. Global Citizen. Available from: https://www.globalcitizen.org/en/content/challenges-for-health-care-workers-nigeria-covid/ (accessed on 5 November 2021). |
| 5 | World Health Organization (WHO). 2020. State of Health Financing in the African Region. Brazzaville: WHO Regional Office for Africa. Available online: https://www.afro.who.int/sites/default/files/2017-06/state-of-health-financing-afro.pdf (accessed on 17 April 2022). |
| 6 | UN Women. 2020. Gender Equality Matters in COVID-19 Response. Available online: https://www.unwomen.org/en/news/in-focus/in-focus-gender-equality-in-covid-19-response?gclid=Cj0KCQjwgYSTBhDKARIsAB8KuktDSWFOP0E1lG5YTKC3Nf6oMceJy_684VKA-WEm4M0h2OggBR5KRCEaAitBEALw_wcB (accessed on 11 April 2022). |
| 7 | WHO. 2020. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novelcoronavirus-2019 (accessed on 15 April 2022). |
| 8 | Harding, A. 2020. South Africa’s Ruthlessly Efficient Fight against Coronavirus. BBC News, April 3. Available online: https://www.bbc.com/news/world-africa-52125713 (accessed on 5 March 2022). |
| 9 | Onyekwena, C., and Ekeruche, A. M. 2020. Understanding the impact of the COVID-19 outbreak on the Nigerian economy. Brookings Institute. Available online: https://www.brookings.edu/blog/africa-in-focus/2020/04/08/understanding-the-impact-of-the-covid-19-outbreak-on-the-nigerian-economy/ (accessed on 17 April 2022). |
| 10 | Simplice A. Asongu & Samba Diop & Joseph Nnanna. 2020. Health Vulnerability versus Economic Resilience to the Covid-19 pandemic: Global Evidence. Working Papers of the African Governance and Development Institute. 20/074, African Governance and Development Institute. Available online: https://ideas.repec.org/p/agd/wpaper/20-074.html (accessed on 21 April 2022). |
| 11 | IMF. 2021. Policy Response to COVID-19. Available online: https://www.imf.org/en/Topics/imf-and-covid19/Policy-Responses-to-COVID-19#S. (accessed on 21 April 2022). |
| 12 | World Bank. 2022. Current Health Expenditure as a percent of GDP. Available online: https://data.worldbank.org/indicator/SH.XPD.CHEX.GD.ZS (accessed on 21 April 2022). |
| 13 | South Africa Reserved Bank. COVID-19: South African Government Financial Assistance Measures. 2020. Available online: https://www.whitecase.com/publications/alert/COVID-19-south-african-government-financial-assistance-m (accessed on 13 November 2021). |
| 14 | WHO. 2020. Coronavirus Disease (COVID-19) Pandemic. Available online: https://www.who.int/emergencies/diseases/novelcoronavirus-2020 (accessed on 21 April 2022). |
| 15 | Naude, W., and Cameron, M. 2020. Failing to Pull Together: South Africa’s Troubled Response to COVID-19. IZA Discussion Paper no. 13436. Bonn: IZA Institute of Labour Economics. |
| 16 | Adejoro, L. 2020. COVID-19 Deaths: Nigeria Ranked Third Highest in Africa. Punch Newspaper. Available online: https://healthwise.punchng.com/COVID-19-deaths-nigeria-ranked-third-highest-in-africa/ (accessed on 20 March 2022). |
| 17 | Adekoya, F., Muanya, C., Chijioke, N., Ibirogba, F., Okwe, M. 2018. Analysts Unveil Highs, Lows of 2019 Budget. The Guardian. Available online: https://guardian.ng/news/analysts-unveil-highs-lows-of-2019-budget/ (accessed on 14 March 2022). |
| 18 | Folorunsho, A. 2020. Health Workers Condemn Reduction of 2020 Health Budget by 50%. Punch Newspaper, June 6. Available online: https://healthwise.punchng.com/health-workers-condemn-reduction-of-2020-health-budget-by-50/ (accessed on 4 March 2022). |
| 19 | Owoseye, A. 2018. Budget 2019: Buhari Proposes N315 Billion Recurrent Health Expenditure. Premium Times, December 20. Available online: https://www.premiumtimesng.com/health/health-news/302067-budget-2019-buhari-proposes-n315-billion-recurrent-health-expenditure.html (accessed on 14 April 2022). |
| 20 | Nigeria Centre for Disease Control. 2020. COVID-19 Outbreak in Nigeria: Situation Reports. Available online https://ncdc.gov.ng/diseases/sitreps (accessed on 5 February 2022). |
| 21 | Dixit, S., Ogundeji, Y. K., Onwujekw, O. 2020. How well has Nigeria responded to COVID-19? Brookings Future Development. The Centre for Policy Impact in Global Impact. Available online: http://centerforpolicyimpact.org/2020/07/28/how-well-has-nigeria-responded-to-COVID-19/ (accessed on 5 March 2022). |
| 22 | Strategic Comments. 2020. COVID-19 in Nigeria and South Africa. Strategic Comments 26: 7–9. Available online: http://go.iiss.org/stratcom (accessed on 13 November 2021). |
| 23 | Obiezu, T. COVID-19 Pandemic: Nigerians Justify Massive Looting of COVID-19 Supplies. 2020. Available online: https://www.voanews.com/COVID-19-pandemic/nigerians-justify-massive-looting-COVID-19-supplies (accessed on 14 November 2021). |
| 24 | Eboh, C. 2020. Nigerian doctors strike again over benefits amid coronavirus. The Reuters. Available online: https://www.reuters.com/article/us-health-coronavirus-nigeria-healthcare-idUSKBN25Z22N (accessed on 6 November 2021). |
| 25 | Benno, N. 2020. The COVID-19 Pandemic and Its Impact on Sub-Saharan African Economies. Centre for International Governance Innovation. Available online: https://www.cigionline.org/articles/covid-19-pandemic-and-its-impact-sub-saharan-african-economies/?utm_source=google_ads&utm_medium=grant&gclid=Cj0KCQjw0umSBhDrARIsAH7FCocnbeLurryVjxJ4-V9tyB-k8H4j2ZU67CvSI7K5VqLm0CP0MNtQBe4aAqGAEALw_wcB (accessed on 14 April 2022). |
| 26 | Earle, A., S. Sparkes, A. Soucat, J. Kutzin. 2021. Financing Common Goods for Health. Geneva: World Health Organization. Available online: https://www.who.int/publications/i/item/9789240034204 (accessed on 12 February 2022). |
References
- Adeniran, Adetayo Olaniyi, and Ben O’ben Sidiq. 2018. Economic Recession and the Way-Out: Nigeria as Case Study. Global Journal of Human-Social Science 8: 1–8. Available online: https://www.researchgate.net/publication/327387730_Economic_Recession_and_the_Way-Out_Nigeria_as_Case_Study (accessed on 21 April 2022).
- Agunyai, Samuel Chukwudi, and Victor Ojakorotu. 2021. The Nigerian Legislative Committee System, Corruption, and Constituency Woes Lessons Nigerians Can Learn from the Singaporean Legislative Committee System. Taiwan Journal of Democracy 17: 97–123. Available online: http://www.tfd.org.tw/export/sites/tfd/files/publication/journal/097-124_Samuel_Chukwudi_Agunyai.pdf (accessed on 21 April 2022).
- Amusan, Lere, and Samuel Chuwudi Agunyai. 2021. The COVID-19 pandemic and the crisis of lockdowns in Nigeria: The household food security perspective. Africa’s Public Service Delivery and Performance Review 9: 484. [Google Scholar] [CrossRef]
- Awofeso, Olu, and Paul Akere Irabor. 2020. Assessment of Government Response to Socioeconomic Impact of Covid-19 Pandemic in Nigeria. Journal of Social and Political Sciences 3: 677–86. [Google Scholar] [CrossRef]
- Chowdhury, Rajiv, Kevin Heng, Md Shajedur Rahman Shawon, Gabriel Goh, Daisy Okonofua, Carolina Ochoa-Rosales, Valentina Gonzalez-Jaramillo, Abbas Bhuiya, Daniel Reidpath, Shamini Prathapan, and et al. 2020. Dynamic interventions to control COVID-19 pandemic: A multivariate prediction modelling study comparing 16 worldwide countries. European Journal of Epidemiology 35: 389–99. [Google Scholar] [CrossRef] [PubMed]
- David, Francis, Valodia Imraan, and Webster Edward. 2020. Politics, Policy, and Inequality in South Africa Under COVID-19. Journal of Political Economy 9: 342–55. [Google Scholar] [CrossRef]
- De Groot, Jiska, and Charlotte Lemanski. 2021. COVID-19 responses: Infrastructure inequality and privileged capacity to transform everyday life in South Africa. Environment and Urbanization 33: 255–72. Available online: https://journals.sagepub.com/doi/pdf/10.1177/0956247820970094 (accessed on 21 April 2022).
- De Villiers, Charl, Daniel Cerbone, and Wayne Van Zijl. 2020. The South African Government’s response to COVID-19. Journal of Public Budgeting, Accounting & Financial Management. Available online: https://www.researchgate.net/publication/343725334_De_Villiers_C_Cerbone_D_Van_Zijl_W_2020_The_South (accessed on 12 March 2022).
- Devereux, Stephen, Christophe Béné, and John Hoddinott. 2020. Conceptualising COVID-19′s impacts on household food security. International Society for Plant Pathology and Springer Nature 12: 769–72. [Google Scholar] [CrossRef]
- Easton, David. 1965. A Systems Analysis of Political Life. New York: Wiley. [Google Scholar] [CrossRef]
- Ejiogu, Amanze, Obiora Okechukwu, and Chibuzo Ejiogu. 2020. Nigerian Budgetary Response to the COVID-19 Pandemic and its Shrinking Fiscal Space: Financial Sustainability, Employment, Social Inequality and Business Implications. Journal of Public Budgeting, Accounting & Financial Management 32: 919–28. [Google Scholar] [CrossRef]
- Ezeani, Emma Onyebuchi. 2005. Fundamentals of Public Administration. Enugu: Zik-Chuks Publishers, Snaap Press Ltd. [Google Scholar]
- Fisher, John R. 2011. Systems theory and structural functionalism. In 21st Century Political Science: A Reference Handbook. Edited by John T. Ishiyama and Marijke Breuning. Thousand Oaks: SAGE, pp. 71–80. [Google Scholar]
- Gershuny, Jonathan, Oriel Sullivan, Almudena Sevilla, Marga Vega-Rapun, Francesca Foliano, Juana Lamote de Grignon, Teresa Harms, and Pierre Walthery. 2021. A new perspective from time use research on the effects of social restrictions on COVID-19 behavioural infection risk. PLoS ONE 16: e0245551. [Google Scholar] [CrossRef]
- Gilbert, Marius, Giulia Pullano, and Francesco Pinotti. 2020. Preparedness and vulnerability of African countries against importations of COVID-19: A modelling study. The Journal of Lancet. Available online: https://www.mdlinx.com/journal-summary/preparedness-and-vulnerability-of-african-countries-against-importations-of-COVID-19-a-modelling/js-7610488 (accessed on 13 November 2021).
- Guleid, Fatuma Hassan, Robinson Oyando, Evelyn Kabia, Audrey Mumbi, Samuel Akech, and Edwin Barasa. 2021. A bibliometric analysis of COVID-19 research in Africa. BMJ Global Health 6: e005690. [Google Scholar] [CrossRef]
- Gumbo, Olivia. 2020. COVID 19 lock-down measures on Zimbabwean populace. Advances in Social Sciences Research Journal 7: 797–814. [Google Scholar] [CrossRef]
- Haider, Najmul, Abdinasir Yusuf Osman, Audrey Gadzekpo, George O. Akipede, Danny Asogun, Rashid Ansumana, Richard John Lessells, Palwasha Khan, Muzamil Mahdi Abdel Hamid, Dorothy Yeboah-Manu, and et al. 2020. Lockdown measures in response to COVID-19 in nine sub-Saharan African countries. BMJ Global Health 5: e003319. [Google Scholar] [CrossRef]
- Hassan, Imad, Fatima Obaid, Roa Ahmed, Lobna Abdelrahman, Sara Adam, Omiema Adam, Mohammed Alfatih Yousif, Khobieb Mohammed, and Tayseer Kashif. 2020. A Systems Thinking approach for responding to the COVID-19 pandemic. East Mediterr Health Journal 26: 872–76. [Google Scholar] [CrossRef] [PubMed]
- Karamouzian, Mohammad, and Navid Madani. 2020. COVID-19 response in the Middle East and North Africa: Challenges and paths forward. Lancet Global Health 8: e886–e887. [Google Scholar] [CrossRef]
- Klantschnig, Gernot, and Chieh Huang. 2019. Fake drugs: Health, wealth and regulation in Nigeria. Review of African Political Economy 46: 442–58. [Google Scholar] [CrossRef]
- Kollamparambil, Umakrishnan, and Adeola Oyenubi. 2021. Behavioural response to the Covid-19 pandemic in South Africa. PLoS ONE 16: e0250269. [Google Scholar] [CrossRef] [PubMed]
- Lone, Shabir Ahmad, and Aijaz Ahmad. 2020. COVID-19 pandemic—An African perspective. Emerging Microbes & Infections 9: 1300–8. [Google Scholar] [CrossRef]
- Margraf, Jurgen, Julia Brailovskaia, and Silvia Schneider. 2020. Behavioral measures to fight COVID-19: An 8-country study of perceived usefulness, adherence and their predictors. PLoS ONE 15: e0243523. [Google Scholar] [CrossRef]
- Massinga, Loembé Massinga, Akhona Tshangela, Stephanie Jane Salyer, Jay Karma Varma, Ahmed Ogwell Ouma, and John Nkengasong. 2020. COVID-19 in Africa: The spread and response. Nature Medicine 26: 999–1003. [Google Scholar] [CrossRef]
- Mboweni, Tito Titus. 2020. 2020 Supplementary Budget Speech, Supplementary Budget Speech to Parliament. June 24. Available online: https://www.gov.za/speeches/minister-tito-mboweni-2020-supplementary-budget-speech-24-jun-2020-0000 (accessed on 13 November 2021).
- Muhammad, Faisal, Jamil Hassan Abdulkareem, and ABM Alauddin Chowdhury. 2017. Major public health problems in Nigeria: A review. South East Asia Journal of Public Health 7: 6–11. [Google Scholar] [CrossRef]
- Nachega, Jean, Rhoda Atteh, Chikwe Ihekweazu, Nadia A. Sam-Agudu, Prisca Adejumo, Sabin Nsanzimana, Edson Rwagasore, Jeanine Condo, Masudah Paleker, Hassan Mahomed, and et al. 2021. Contact Tracing and the COVID-19 Response in Africa: Best Practices, Key Challenges, and Lessons Learned from Nigeria, Rwanda, South Africa, and Uganda. The American Journal of Tropical Medicine and Hygiene 104: 1179–87. [Google Scholar] [CrossRef]
- Oleribe, Obinna O., Jenny Momoh, Benjamin S. C. Uzochukwu, Francisco Mbofana, Akin Adebiyi, Thomas Barbera, Roger Williams, and Simon D. Taylor-Robinson. 2019. Identifying Key Challenges Facing Healthcare Systems in Africa and Potential Solutions. International Journal of General Medicine 12: 395–403. [Google Scholar] [CrossRef] [Green Version]
- Ozili, Peterson K. 2020. COVID-19 Pandemic and Economic Crisis: The Nigerian Experience and Structural Causes. SSRN Electronic Journal, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Pan, An, Li Liu, Chaolong Wang, Huan Guo, Xingjie Hao, Qi Wang, Jiao Huang, Na He, Hongjie Yu, Xihong Lin, and et al. 2020. Association of public health interventions with the epidemiology of the COVID-19 outbreak in Wuhan, China. Journal of the American Medical Association. Available online: https://jamanetwork.com/journals/jama/fullar.-article/2764658 (accessed on 11 April 2022).
- Staunton, Ciara, Carmen Swanepoel, and Melodie Labuschagine. 2020. Between a rock and a hard place: COVID-19 and South Africa’s response. Journal of Law and the Biosciences 7: lsaa052. [Google Scholar] [CrossRef] [PubMed]
- Tessema, Gizachew A., Yohannes Kinfu, Berihun Assefa Dachew, Azeb Gebresilassie Tesema, Yibeltal Assefa, Kefyalew Addis Alene, Atsede Fantahun Aregay, Mohammed Biset Ayalew, Woldesellassie M. Bezabhe, Ayele Geleto Bali, and et al. 2021. The COVID-19 pandemic and healthcare systems in Africa: A scoping review of preparedness, impact and response. BMJ Global Health 6: e007179. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Year | 2018 | 2019 |
|---|---|---|
| Countries | % Share of the GDP | % Share of the GDP |
| South Africa | 8.8 | 9.1 |
| Nigeria | 3.09 | 3.03 |
| Main Budget Framework | ||
|---|---|---|
| R Billion/Percentage of GDP | 2020/21 Budget 2020 | Revised |
| Main Budget Revenue | 1398.0 25.5% | 1099.5 22.6% |
| Main Budget Expenditure | 1766.0 32.52 | 1809.2 37.2% |
| Non-Interest Expenditure | 1536.7 28% | 1572.7 32.4% |
| Debt Service Costs | 229.3 4.2% | 236.4 4.9% |
| Main Budget Balance | −368.0 −6.8% | −709.7 −14.6% |
| Primary Balance | −138.7 −2.6% | −473.2 −9.7% |
| R. Million | 2020/21 | |
|---|---|---|
| 1 | Support to Vulnerable households for 6 months | 40,891 |
| 2 | Health | 21,544 |
| 3 | Support to Municipalities | 20,034 |
| 4 | Other Frontline Services | 13,623 |
| 5 | Basic and Higher Education | 12,541 |
| 6 | Small and Informal Business Support and Job creation and Protection | 6061 |
| 7 | Support to Public entities | 5964 |
| 8 | Other COVID-19 Interventions | 1766 |
| Allocated for COVID-19 Fiscal relief package | 122,425 | |
| 9 | Land Bank Equity Investment | 3000 |
| 10 | Provisional Allocations for COVID-19 Fiscal Relief | 19,575 |
| Total | 145,000 |
| Country | Test per 1000 | As at the Dates | Absolute Change | Relative Change |
|---|---|---|---|---|
| Chile | 1877.31 | 14 April 2022 | +1877.14 | +1,097,742% |
| Argentina | 780.63 | 13 April 2022 | +780.61 | +5,575,814% |
| US | 2574.77 | 9 April 2022 | +2574.77 | +257,476,800% |
| Canada | 1580.05 | +1580.04 | +39,501,100% | |
| South Africa | 402.05 | 14 April 2022 | +402.05 | +20,102,350% |
| Nigeria | 23.21 | 7 April 2022 | +23.19 | +96,608% |
| UK | 7227.15 | 13 April 2022 | +7224.88 | +317,577% |
| Italy | 3445.80 | 14 April 2022 | +3445.73 | +4,785,731% |
| India | 596.24 | 14 April 2022 | +596.24 | +11,924,760% |
| South Korea | 1789.36 | 14 April 2022 | +1789.13 | +774,516% |
| Australia | 2643.47 | 14 April 2022 | +2643.21 | +1,001,216% |
| Norway | 2022.24 | 13 April 2022 | +2021.52 | +280,767% |
| Country | Confirmed Cases | Confirmed Fatality | Current Health Expending as per % GDP |
|---|---|---|---|
| US | 80.5 M | 987,000 | 16.77 |
| India | 21.8 M | 172,000 | 10.15 |
| Brazil | 30.2 M | 662,000 | 9.59 |
| France | 26.8 M | 141,000 | 11.06 |
| South Africa | 3.74 M | 100,000 | 9.11 |
| Nigeria | 256,000 | 3143 | 3.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chukwudi, A.S.; Victor, O. Budgetary Allocations and Government Response to COVID-19 Pandemic in South Africa and Nigeria. J. Risk Financial Manag. 2022, 15, 252. https://doi.org/10.3390/jrfm15060252
Chukwudi AS, Victor O. Budgetary Allocations and Government Response to COVID-19 Pandemic in South Africa and Nigeria. Journal of Risk and Financial Management. 2022; 15(6):252. https://doi.org/10.3390/jrfm15060252
Chicago/Turabian StyleChukwudi, Agunyai Samuel, and Ojakorotu Victor. 2022. "Budgetary Allocations and Government Response to COVID-19 Pandemic in South Africa and Nigeria" Journal of Risk and Financial Management 15, no. 6: 252. https://doi.org/10.3390/jrfm15060252
APA StyleChukwudi, A. S., & Victor, O. (2022). Budgetary Allocations and Government Response to COVID-19 Pandemic in South Africa and Nigeria. Journal of Risk and Financial Management, 15(6), 252. https://doi.org/10.3390/jrfm15060252