
Remote, Whole-Body Interval Training Improves Muscular Endurance and Cardiac Autonomic Control in Young Adults
 , , ,
, , ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. HIIT
2.4. HRV
2.5. Maximal Push-Up Test
2.6. Statistical Analysis
3. Results
3.1. Exercise Program
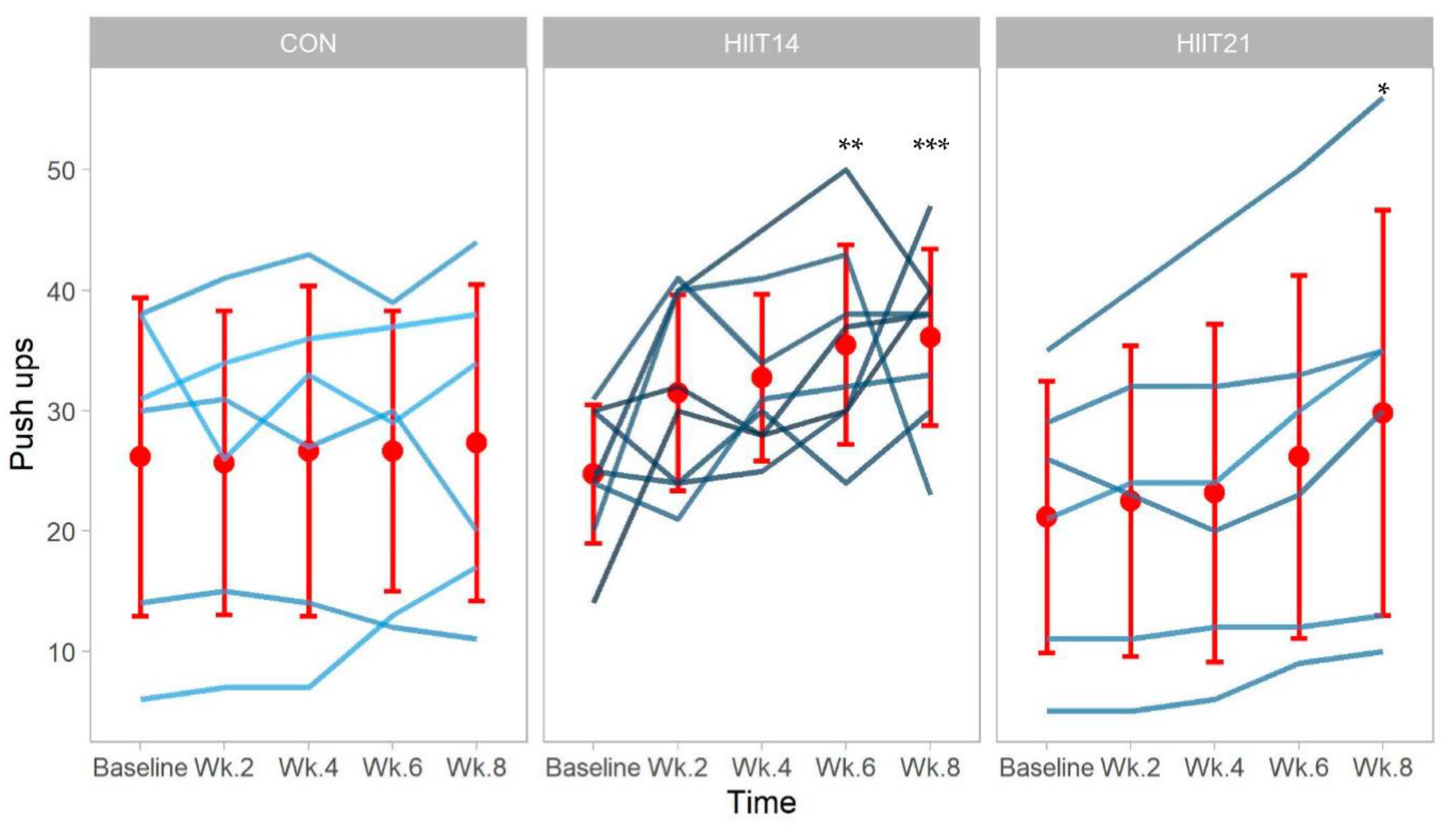
3.2. Muscular Endurance
3.3. Heart Rate Variability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef] [PubMed]
- Jorstad, H.T.; Piek, J.J. Physical inactivity in times of a pandemic: Another curve to flatten. Neth. Heart J. 2021, 29, 241–242. [Google Scholar] [CrossRef] [PubMed]
- Hall, G.; Lavie, C.J.; Arena, R. A tale of two pandemics: How will COVID-19 and global trends in physical inactivity and sedentary behavior affect one another? Prog. Cardiovasc. Dis. 2021, 61, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Bucciarelli, V.; Nasi, M.; Bianco, F.; Seferovic, J.; Ivkovic, V.; Gallina, S.; Mattioli, A.V. Depression pandemic and cardiovascular risk in the COVID-19 era and long COVID syndrome: Gender makes a difference: Depression and cardiovascular risk in women during COVID-19 pandemic. Trends Cardiovasc. Med. 2022, 32, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Wong, B.; El-Jack, S.; Armstrong, G. Pandemic control: Getting to the heart of unintended consequences. N. Z. Med. J. 2020, 133, 153–156. [Google Scholar]
- Maffetone, P.B.; Laursen, P.B. The Perfect Storm: Coronavirus (COVID-19) Pandemic Meets Overfat Pandemic. Front. Public Health 2020, 8, 135. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, A.; Chen, S.; Pasea, L.; Lai, A.G.; Katsoulis, M.; Denaxas, S.; Nafilyan, V.; Williams, B.; Wong, W.K.; Bakhai, A.; et al. Excess deaths in people with cardiovascular diseases during the COVID-19 pandemic. Eur. J. Prev. Cardiol. 2021, 28, 1599–1609. [Google Scholar] [CrossRef]
- Botly, L.C.P.; Martin-Rhee, M.; Kasiban, A.; Swartz, R.H.; Mulvagh, S.L.; Lindsay, M.P.; Goia, C.; Smith, E.E.; Hill, M.D.; Field, T.S.; et al. COVID-19 Pandemic: Global Impact and Potential Implications for Cardiovascular Disease in Canada. CJC Open 2020, 2, 265–272. [Google Scholar] [CrossRef]
- Suzuki, Y.; Maeda, N.; Hirado, D.; Shirakawa, T.; Urabe, Y. Physical activity changes and its risk factors among community-dwelling japanese older adults during the COVID-19 epidemic: Associations with subjective well-being and health-related quality of life. Int. J. Environ. Res. Public Health 2020, 17, 6591. [Google Scholar] [CrossRef]
- Lowensteyn, I.; Coupal, L.; Zowall, H.; Grover, S.A. The cost-effectiveness of exercise training for the primary and secondary prevention of cardiovascular disease. J. Cardiopulm. Rehabil. Prev. 2000, 20, 147–155. [Google Scholar] [CrossRef]
- Ricci, F.; Izzicupo, P.; Moscucci, F.; Sciomer, S.; Maffei, S.; Di Baldassarre, A.; Mattioli, A.V.; Gallina, S. Recommendations for Physical Inactivity and Sedentary Behavior During the Coronavirus Disease (COVID-19) Pandemic. Front. Public Health 2020, 8, 199. [Google Scholar] [CrossRef] [PubMed]
- Swain, D.; Brawner, C. ACSM’s Resource Manual for Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Baltimore, MD, USA, 2014. [Google Scholar]
- Yang, Y.J. An Overview of Current Physical Activity Recommendations in Primary Care. Korean J. Fam. Med. 2019, 40, 135–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szabo, D.A. The Importance of Cardiorespiratory Fitness and Physical Activity among Adulthood Stages—Review. Stud. Univ. Babeş-Bolyai Educ. Artis Gymnast. 2021, 66, 85–101. [Google Scholar] [CrossRef]
- López-Bueno, R.; Calatayud, J.; Andersen, L.L.; Balsalobre-Fernández, C.; Casaña, J.; Casajús, J.A.; Smith, L.; López-Sánchez, G.F. Immediate impact of the COVID-19 confinement on physical activity levels in Spanish adults. Sustainability 2020, 12, 5708. [Google Scholar] [CrossRef]
- Hoare, E.; Stavreski, B.; Jennings, G.; Kingwell, B. Exploring Motivation and Barriers to Physical Activity among Active and Inactive Australian Adults. Sports 2017, 5, 47. [Google Scholar] [CrossRef] [Green Version]
- Thum, J.S.; Parsons, G.; Whittle, T.; Astorino, T.A. High-intensity interval training elicits higher enjoyment than moderate intensity continuous exercise. PLoS ONE 2017, 12, e0166299. [Google Scholar] [CrossRef] [Green Version]
- Gillen, J.B.; Gibala, M.J. Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Appl. Physiol. Nutr. Metab. Physiol. Appl. Nutr. Métabolisme 2014, 412, 409–412. [Google Scholar] [CrossRef]
- Klika, B.; Jordan, C. High-intensity circuit training using body weight: Maximum results with minimal investment. ACSM’s Health Fit. J. 2013, 17, 8–13. [Google Scholar] [CrossRef] [Green Version]
- Schleppenbach, L.N.; Ezer, A.B.; Gronemus, S.A.; Widenski, K.R.; Braun, S.I.; Janot, J.M. Speed- and Circuit-Based High-Intensity Interval Training on Recovery Oxygen Consumption. Int. J. Exerc. Sci. 2017, 10, 942–953. [Google Scholar]
- Gibala, M.J.; Gillen, J.B.; Percival, M.E. Physiological and Health-Related Adaptations to Low-Volume Interval Training: Influences of Nutrition and Sex. Sport. Med. 2014, 44, 127–137. [Google Scholar] [CrossRef] [Green Version]
- Luong, A.; Goodyke, M.; Dunn, S.L.; Baynard, T.; Bronas, U. ActiGraph and Short-term Heart Rate Variability Study Protocol: Amended for the COVID-19 Pandemic. J. Cardiovasc. Nurs. 2021, 36, 599–608. [Google Scholar] [CrossRef] [PubMed]
- Shaji, S.; Pathinarupothi, R.K.; Rangan, E.S.; Menon, K.A.U.; Ramesh, M.V. Heart Lung Health Monitor: Remote At-Home Patient Surveillance for Pandemic Management. In Proceedings of the 2021 IEEE Global Humanitarian Technology Conference (GHTC), Seattle, WA, USA, 19–23 October 2021; pp. 127–130. [Google Scholar] [CrossRef]
- Lee, Y.H.; Hur, S.H.; Sohn, J.; Lee, H.M.; Park, N.H.; Cho, Y.K.; Park, H.S.; Yoon, H.J.; Kim, H.; Nam, C.W.; et al. Impact of home-based exercise training with wireless monitoring on patients with acute coronary syndrome undergoing percutaneous coronary intervention. J. Korean Med. Sci. 2013, 28, 564–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiyono, K.; Junichiro, H.; Watanabe, E.; Yamamoto, Y. Heart Rate Variability (HRV) and Sympathetic Nerve Activity. In Clinical Assessment of the Autonomic Nervous System; Springer: Tokyo, Japan, 2017; pp. 147–159. ISBN 9784431560128. [Google Scholar]
- Acharya, U.R.; Joseph, K.P.; Kannathal, N.; Lim, C.M.; Suri, J.S. Heart rate variability: A review. Med. Biol. Eng. Comput. 2006, 44, 1031–1051. [Google Scholar] [CrossRef]
- Thayer, J.F.; Yamamoto, S.S.; Brosschot, J.F. The relationship of autonomic imbalance, heart rate variability and cardiovascular disease risk factors. Int. J. Cardiol. 2010, 141, 122–131. [Google Scholar] [CrossRef] [PubMed]
- Vrachimis, A.; Hadjicharalambous, M.; Tyler, C. The Effect of Circuit Training on Resting Heart Rate Variability, Cardiovascular Disease Risk Factors and Physical Fitness in Healthy Untrained Adults. Health 2016, 8, 144–155. [Google Scholar] [CrossRef] [Green Version]
- Koko, K.R.; McCauley, B.D.; Gaughan, J.P.; Fromer, M.W.; Nolan, R.S.; Hagaman, A.L.; Brown, S.A.; Hazelton, J.P. Spectral analysis of heart rate variability predicts mortality and instability from vascular injury. J. Surg. Res. 2018, 224, 64–71. [Google Scholar] [CrossRef]
- Cipryan, L. The effect of fitness level on cardiac autonomic regulation, IL-6, total antioxidant capacity, and muscle damage responses to a single bout of high-intensity interval training. J. Sport Health Sci. 2016, 7, 363–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haensel, A.; Mills, P.J.; Nelesen, R.A.; Ziegler, M.G.; Dimsdale, J.E. The relationship between heart rate variability and inflammatory markers in cardiovascular diseases. Psychoneuroendocrinology 2008, 33, 1305–1312. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and heart rate variability: A meta-analysis and review of the literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [Green Version]
- Miller, J.G.; Chahal, R.; Kirshenbaum, J.S.; Ho, T.C.; Gifuni, A.J.; Gotlib, I.H. Heart rate variability moderates the effects of COVID-19-related stress and family adversity on emotional problems in adolescents: Testing models of differential susceptibility and diathesis stress. Dev. Psychopathol. 2021, 1–12. [Google Scholar] [CrossRef]
- Makovac, E.; Carnevali, L.; Medina, S.; Sgoifo, A.; Petrocchi, N.; Ottaviani, C. Safe in my heart: Resting heart rate variability longitudinally predicts emotion regulation, worry, and sense of safeness during COVID-19 lockdown. Stress 2022, 25, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M.; Gindre, C. Cardiac parasympathetic regulation: Respective associations with cardiorespiratory fitness and training load. Am. J. Physiol. Heart Circ. Physiol. 2006, 291, H451–H458. [Google Scholar] [CrossRef] [PubMed]
- Buchheit, M. Monitoring training status with HR measures: Do all roads lead to Rome? Front. Physiol. 2014, 5, 73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grant, C.C.; Murray, C.; Janse van Rensburg, D.C.; Fletcher, L. A comparison between heart rate and heart rate variability as indicators of cardiac health and fitness. Front. Physiol. 2013, 4, 337. [Google Scholar] [CrossRef] [Green Version]
- Fennell, C. Effects of Supervised Training Compared to Unsupervised Training on Physical Activity, Muscular Endurance, and Cardiovascular Parameters. MOJ Orthop. Rheumatol. 2016, 5, 00184. [Google Scholar] [CrossRef] [Green Version]
- Kokkinos, P. Physical fitness evaluation. Am. J. Lifestyle Med. 2015, 9, 308–317. [Google Scholar] [CrossRef]
- Segerström, A.B.; Holmbäck, A.M.; Elzyri, T.; Eriksson, K.-F.; Ringsberg, K.; Groop, L.; Thorsson, O.; Wollmer, P. Upper Body Muscle Strength and Endurance in Relation to Peak Exercise Capacity During Cycling in Healthy Sedentary Male Subjects. J. Strenght Cond. Res. 2011, 25, 1413–1417. [Google Scholar] [CrossRef]
- Soltani, M.; Baluchi, M.J.; Boullosa, D.; Daraei, A.; Doyle-Baker, P.K.; Saeidi, A.; Knechtle, B.; Dehbaghi, K.M.; Mollabashi, S.S.; VanDusseldorp, T.A.; et al. Effect of Intensity on Changes in Cardiac Autonomic Control of Heart Rate and Arterial Stiffness After Equated Continuous Running Training Programs. Front. Physiol. 2021, 12, 758299. [Google Scholar] [CrossRef]
- Songsorn, P.; Somnarin, K.; Jaitan, S.; Kupradit, A. The effect of whole-body high-intensity interval training on heart rate variability in insufficiently active adults. J. Exerc. Sci. Fit. 2022, 20, 48–53. [Google Scholar] [CrossRef]
- Task Force of the European Society of Cardiology; The North American Society of Pacing and Electrophysiology. Guidelines Heart rate variability. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Pescatello, L.; Riebe, D.; Thompson, P. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Marshall, P.; Al-Timman, J.; Riley, R.; Wright, J.; Williams, S.; Hainsworth, R.; Tan, L.B. Randomized controlled trial of home-based exercise training to evaluate cardiac functional gains. Clin. Sci. 2001, 101, 477–483. [Google Scholar] [CrossRef]
- Heydari, M.; Boutcher, Y.N.; Boutcher, S.H. High-intensity intermittent exercise and cardiovascular and autonomic function. Clin. Auton. Res. 2013, 23, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Alansare, A.; Alford, K.; Lee, S.; Church, T.; Jung, H. The Effects of High-Intensity Interval Training vs. Moderate-Intensity Continuous Training on Heart Rate Variability in Physically Inactive Adults. Int. J. Environ. Res. Public Health 2018, 15, 1508. [Google Scholar] [CrossRef] [Green Version]
- Joyner, M.J.; Green, D.J. Exercise protects the cardiovascular system: Effects beyond traditional risk factors. J. Physiol. 2009, 587, 5551–5558. [Google Scholar] [CrossRef]
- Ramos, J.S.; Dalleck, L.C.; Borrani, F.; Beetham, K.S.; Mielke, G.I.; Dias, K.A.; Wallen, M.P.; Keating, S.E.; Fassett, R.G.; Coombes, J.S. High-intensity interval training and cardiac autonomic control in individuals with metabolic syndrome: A randomised trial. Int. J. Cardiol. 2017, 245, 245–252. [Google Scholar] [CrossRef]
- Grassi, G.; Vailati, S.; Bertinieri, G.; Seravalle, G.; Stella, M.L.; Dell’Oro, R.; Mancia, G. Heart rate as marker of sympathetic activity. J. Hypertens. 1998, 16, 1635–1639. [Google Scholar] [CrossRef]
- Shenoy, S.; Khandekar, P. A systematic review on the effect of high.intensity training on heart rate variability in sports professionals and healthy young adults. BLDE Univ. J. Health Sci. 2020, 5, 114. [Google Scholar] [CrossRef]
- Blackwell, J.; Atherton, P.; Smith, K.; Doleman, B.; Williams, J.P.; Lund, J.N.; Phillips, B.E. The efficacy of unsupervised home-based exercise regimens vs laboratory-based exercise training upon cardio-respiratory health facets. Physiol. Rep. 2017, 5, 13390. [Google Scholar] [CrossRef]
- Gettman, L.R.; Pollock, M.L.; Ward, A. Adherence to unsupervised exercise. Phys. Sportsmed. 1983, 11, 56–66. [Google Scholar] [CrossRef]
- DeBusk, R.F.; Stenestrand, U.; Sheehan, M.; Haskell, W.L. Training effects of long versus short bouts of exercise in healthy subjects. Am. J. Cardiol. 1990, 65, 1010–1013. [Google Scholar] [CrossRef]
- Drury, R.L.; Jarczok, M.; Owens, A.; Thayer, J.F. Wireless Heart Rate Variability in Assessing Community COVID-19. Front. Neurosci. 2021, 15, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Mayr Ojeda, E.; Castro, F.A.d.S.; Reich, M.; Astorino, T.A.; Benítez-Flores, S. Burpee Interval Training Is Associated with a More Favorable Affective Valence and Psychological Response Than Traditional High Intensity Exercise. Percept. Mot. Ski. 2022, 129, 767–786. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Lo Moro, G.; Voglino, G.; Bert, F.; Siliquini, R. Effects of COVID-19 lockdown on mental health and sleep disturbances in Italy. Int. J. Environ. Res. Public Health 2020, 17, 4779. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | CON (n = 6) | HIIT-14 (n = 8) | HIIT-21 (n = 6) |
|---|---|---|---|
| Age (years) * | 23.66 ± 2.6 | 20.85 ± 1.7 | 22.50 ± 2.5 |
| BMI (kg·m−2) * | 21.74 ± 2.7 | 30.87 ± 14.7 | 26.42 ± 6.8 |
| Physical activity (METs·min·wk−1) 1,* | 1416 ± 1389 | 1372 ± 834 | 2205 ± 1446 |
| Male to female ratio | 5/1 | 5/3 | 5/1 |
| Group | CON | HICT-14 | HICT-21 | p Values | ɳ2 | |||
|---|---|---|---|---|---|---|---|---|
| Time/Variable | Pre | Post | Pre | Post | Pre | Post | Time Treatment Interaction | Effect Size (95% CIs) |
| HR (bpm) | 68 ± 15 | 69 ± 6 | 63 ± 11 | 63 ± 13 | 83 ± 33 | 64 ± 14 | 0.886 0.523 0.074 | 0.21 (−2.06–42.73) |
| SDHR (bpm) | 5.38 ± 2.1 | 4.27 ± 1.4 | 4.88 ± 1.9 | 4.43 ± 1.8 | 7.11 ± 4.0 | 4.44 ± 1.2 | 0.315 0.898 0.650 | 0.13 (−2.25–3.56) |
| IBI (ms) | 921 ± 188.8 | 877 ± 80.2 | 979 ± 194.7 | 990 ± 206.7 | 789 ± 202.9 | 981 ± 221.7 * | 0.551 0.278 0.029 * | 0.19 (−378.25–15.68) |
| SDNN (ms) | 67.94 ± 12.8 | 54.53 ± 21.1 | 68.62 ± 20.8 | 66.00 ± 22.0 | 62.99 ± 28.5 | 73.38 ± 43.0 | 0.166 0.419 0.085 | 0.128 (−51.05–3.45) |
| RMSSD (ms) | 55.35 ± 17.5 | 48.73 ± 19.4 | 71.85 ± 24.4 | 69.79 ± 30.3 | 59.48 ± 25.4 | 81.68 ± 52.0 | 0.617 0.205 0.794 | 0.14 (−39.84–30.71) |
| pNN50 (%) | 31.38 ± 18.6 | 22.73 ± 19.2 | 39.75 ± 13.7 | 38.78 ± 16.7 | 35.67 ± 21.5 | 41.67 ± 24.3 | 0.330 0.126 0.511 | 0.08 (−31.24–15.86) |
| VLF (ms2) | 351.89 ± 309.65 | 101.75 ± 57.7 | 262.54 ± 257.2 | 338.85 ± 213.4 | 101.32 ± 89.2 | 384.47 ± 539.9 * | 0.117 0.134 0.021 | 0.26 (−980–−86.52) |
| LF (ms2) | 3097.72 ± 1956.6 | 2029.85 ± 1314.5 | 2030.98 ± 1309.3 | 2153.78 ± 1460.3 | 3034.96 ± 3910.17 | 3049.26 ± 4082.2 | 0.216 0.928 0.372 | 0.07 (−351767–−1353.35) |
| HF (ms2) | 1815.67 ± 1469.4 | 1480.04 ± 1637.2 | 2192.97 ± 1348.8 | 1935.80 ± 2080.4 | 962.15 ± 1243.1 | 2394.34 ± 2386.9 | 0.680 0.632 0.131 | 0.16 (−4088.42–552.77) |
| LF (n.u.) | 62.33 ± 20.9 | 60.05 ± 20.5 | 48.54 ± 10.1 | 56.31 ± 15.1 | 68.68 ± 20.4 | 51.70 ± 12.9 | 0.681 0.395 0.068 | 0.34 (9.91–39.59) |
| HF (n.u.) | 37.65 ± 20.9 | 39.92 ± 20.5 | 51.43 ± 10.1 | 43.65 ± 15.0 | 31.24 ± 20.44 | 48.24 ± 12.9 | 0.683 0.396 0.068 | 0.34 (−39.61–−9.94) |
| LF/HF | 2.37 ± 1.7 | 2.42 ± 2.2 | 1.00 ± 0.3 | 1.70 ± 1.4 | 5.51 ± 7.1 § | 1.22 ± 0.72 * | 0.973 0.667 0.05 | 0.12 (0.07–8.61) |
| Total Power (ms2) | 5265.55 ± 2127.7 | 3612.21 ± 2274.1 | 4487.46 ± 2721.1 | 4429.49 ± 3560.4 | 5075.99 ± 4332.4 | 5828.81 ± 6082.8 | 0.253 0.686 0.239 | 0.08 (−6495.34–1683.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Suárez, P.C.; Canton-Martínez, E.; Rentería, I.; Moura Antunes, B.; Machado-Parra, J.P.; Aburto-Corona, J.A.; Gómez-Miranda, L.M.; Jiménez-Maldonado, A. Remote, Whole-Body Interval Training Improves Muscular Endurance and Cardiac Autonomic Control in Young Adults. Int. J. Environ. Res. Public Health 2022, 19, 13897. https://doi.org/10.3390/ijerph192113897
García-Suárez PC, Canton-Martínez E, Rentería I, Moura Antunes B, Machado-Parra JP, Aburto-Corona JA, Gómez-Miranda LM, Jiménez-Maldonado A. Remote, Whole-Body Interval Training Improves Muscular Endurance and Cardiac Autonomic Control in Young Adults. International Journal of Environmental Research and Public Health. 2022; 19(21):13897. https://doi.org/10.3390/ijerph192113897
Chicago/Turabian StyleGarcía-Suárez, Patricia Concepción, Ermilo Canton-Martínez, Iván Rentería, Barbara Moura Antunes, Juan Pablo Machado-Parra, Jorge Alberto Aburto-Corona, Luis Mario Gómez-Miranda, and Alberto Jiménez-Maldonado. 2022. "Remote, Whole-Body Interval Training Improves Muscular Endurance and Cardiac Autonomic Control in Young Adults" International Journal of Environmental Research and Public Health 19, no. 21: 13897. https://doi.org/10.3390/ijerph192113897