
Effectiveness of Whole-Body High-Intensity Interval Training on Health-Related Fitness: A Systematic Review and Meta-Analysis

 ,
,  ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment and Risk of Bias
2.5. Data Synthesis and Statistical Analysis
3. Results
3.1. Search Results
3.2. Quality Assessment and Risk of Bias

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Population | Groups | Interventions | Exercise Intervention Protocols | Outcomes | |||
|---|---|---|---|---|---|---|---|---|
| Session Duration (min) | IT Work/Rest Ratio | Frequency | Total Training Time (min) | |||||
| Healthy participants | ||||||||
| Ballesta-Garcia, 2019 [11] | Healthy adults | WB-HIIT vs. WB-MIIT vs. CTL |
| WB-HIIT: 18–40 WB-MIIT: 18–50 | WB-HIIT: 60–90″/120–150″ | WB-HIIT: 16 wks, 2×/wk WB-MIIT: 16 wks, 2×/wk | WB-HIIT: 928 WB-MIIT: 1088 | MSF |
| Ballesta-Garcia, 2020 [12] | Healthy adults | WB-HIIT vs. WB-MIIT vs. CTL |
| WB-HIIT: 18–40 WB-MIIT: 18–50 | WB-HIIT: 60–90″/120–150″ | WB-HIIT: 16 wks, 2×/wk WB-MIIT: 16 wks, 2×/wk | WB-HIIT: 928 WB-MIIT: 1088 | CRF |
| Blackwell et al., 2017 [20] | Healthy adults | WB-HIIT vs. HIIT |
| WB-HIIT: 11 HIIT: 11 | WB-HIIT: 60″/90″ HIIT: 60″/90″ | WB-HIIT: 4 wks, 3×/wk HIIT: 4 wks, 3×/w | WB-HIIT: 132 HIIT: 132 | CRF, Metabolic risk factors |
| * Connolly et al., 2020 [18] | Healthy adults | WB-HIIT vs. CTL |
| WB-HIIT: 15 | WB-HIIT: 30″ low/20″ moderate/10″ high intensity | WB-HIIT: 12 wks, 3×/wk | WB-HIIT: 540 | Metabolic risk factors |
| Engel et al., 2019 [22] | Healthy adults | WB-HIIT vs. CTL |
| WB-HIIT: 30 | WB-HIIT: 20″/10″ | WB-HIIT: 8 wks, 2×/wk | WB-HIIT: 480 | MSF, Metabolic risk factors |
| Evangelista et al., 2019 [23] | Healthy adults | WB-HIIT vs. VICT |
| WB-HIIT: 20 VICT: 20 | WB-HIIT: 30″/30″ | WB-HIIT: 6 wks, 3×/wk VICT: 6 wks, 3×/wk | WB-HIIT: 360 VICT: 360 | Fat mass, Fat-free mass, MSF |
| Evangelista et al., 2021 [24] | Healthy adults | WB-HIIT vs. CTL |
| WB-HIIT: 21 | WB-HIIT: 40″/20″ | Wb-HIIT: 6 wks, 3×/wk | WB-HIIT: 378 | CRF, MSF |
| Islam et al., 2019 [25] | Healthy adults | WB-HIIT vs. VICT vs. CTL |
| WB-HIIT: 4 VICT: 30 | WB-HIIT: 20″/10″ | WB-HIIT: 4 wks, 4×/wk VICT: 4 wks, 4×/wk | WB-HIIT: 60 VICT: 480 | CRF, MSF |
| Jimenez-Garcia et al., 2019 [21] | Healthy adults | WB-HIIT vs. WB-MIIT vs. CTL |
| WB-HIIT: 25 WB-MIIT: 25 | WB-HIIT: 4′/3′ WB-MIIT: 4′/3′ | WB-HIIT: 12 wks, 2×/wk WB-MIIT: 12 wks, 2×/wk | WB-HIIT: 600 WB-MIIT: 600 | Fat mass, Fat-free mass, MSF |
| Lu et al., 2021 [26] | Healthy adults | WB-HIIT vs. HIIT |
| WB-HIIT: 4 HIIT: 4 | WB-HIIT: 20″/10″ HIIT:30″/30″ | WB-HIIT: 12 wks, 3×/wk HIIT: 12 wks, 3×/wk | WB-HIIT: 144 HIIT: 144 | CRF, Fat mass, Fat-free mass, MSF |
| * McRae et al., 2012 [16] | Healthy adults | WB-HIIT vs. VICT vs. CTL |
| WB-HIIT: 4 VICT: 30 | WB-HIIT: 20″/10″ | WB-HIIT: 4 wks, 4×/wk CT: 4 wks, 4×/wk | WB-HIIT: 48 CT: 480 | CRF, MSF |
| Menz et al., 2019 [27] | Healthy adults | WB-HIIT vs. HIIT |
| WB-HIIT: 12–16 HIIT: 12–16 | WB-HIIT: 20″/10″ HIIT: 20″/10″ | WB-HIIT: 4 wks, 3–4×/wk HIIT: 4 wks, 3–4×/wk | WB-HIIT: 191 HIIT: 191 | CRF, Fat mass, Fat-free mass, MSF |
| Micielska et al., 2019 [28] | Healthy adults | WB-HIIT vs. CTL |
| WB-HIIT: 25 | WB-HIIT: 30″/10″ | WB-HIIT: 5 wks, 3×/wk CTL: 2 sessions | WB-HIIT: 325 CTL: 50 | CRF, Fat mass, Fat-free mass |
| Murawska-Cialowicz et al., 2020 [29] | Healthy adults | WB-HIIT vs. CTL |
| WB-HIIT: 40 | WB-HIIT: 20″/10″ | WB-HIIT: 8 wks, 2×/wk | WB-HIIT: 640 | CRF, Fat mass, Fat-free mass |
| Schaun et al., 2018 [13] | Healthy adults | WB-HIIT vs. HIIT vs. VICT |
| WB-HIIT: 8 HIIT: 8 VICT: 30 | WB-HIIT: 20″/10″ HIIT: 20″/10″ | WB-HIIT: 16 wks, 3×/wk HIIT: 16 wks, 3×/wk VICT: 16 wks, 3×/wk | WB-HIIT: 384 HIIT: 384 VICT: 1440 | CRF, Fat mass |
| Schaun et al., 2019 [14] | Healthy adults | WB-HIIT vs. HIIT vs. VICT |
| WB-HIIT: 8 HIIT: 8 VICT: 30 | WB-HIIT: 20″/10″ HIIT: 20″/10″ | WB-HIIT: 16 wks, 3×/wk HIIT: 16 wks, 3×/wk VICT: 16 wks, 3×/wk | WB-HIIT: 384 HIIT: 384 VICT: 1440 | MSF |
| Schmidt et al., 2016 [30] | Healthy adults | WB-HIIT vs. CTL |
| WB-HIIT 7: 1 × 7 WB-HIIT 14: 1 × 7 (wk 1–4), 2 × 7 (wk 5–8) | WB-HIIT: 30″/10″ | WB-HIIT 7: 8 wks, 3×/wk WB-HIIT 14: 8 wks, 3×/wk | WB-HIIT 7: 168 WB-HIIT 14: 252 | CRF, Fat mass, MSF |
| Sperlich et al., 2018 [31] | Healthy adults | WB-HIIT LV vs. WB-HIIT HV vs. CTL |
| WB-HIIT LV: 1 × 6 WB-HIIT HV: 2 × 6 | WB-HIIT LV: Not specified (6 min circuit) WB-HIIT HV: Not specified (6 min circuit) | WB-HIIT LV: 4 wks, 7×/wk WB-HIIT HV: 4 wks, 14×/wk | WB-HIIT LV: 168 WB-HIIT HV: 336 | CRF, Fat mass, Fat-free mass, MSF |
| * Wilke et al., 2019 [17] | Healthy adults | WB-HIIT vs. MICT |
| WB-HIIT: 30 MICT: 50 | WB-HIIT: 20″/10″ | WB-HIIT: 6 wks, 3×/wk MICT: 6 wks, 3×/wk | WB-HIIT: 540 MICT: 900 | CRF, MSF |
| Specific populations | ||||||||
| Batrakoulis et al., 2018 [32] | Obese women | WB-HIIT vs. CTL |
| WB-HIIT: 23–41 | WB-HIIT: 20″/40″ | WB-HIIT: 20 wks, 3×/wk | WB-HIIT: 1761 | CRF, Fat mass, Fat-free mass, MSF |
| Jung et al., 2019 [33] | Women with sarcopenia | WB-HIIT vs. CTL |
| WB-HIIT: 25–55 | WB-HIIT: 10″/5″ | WB-HIIT: 12 wks, 3×/wk | WB-HIIT: 1440 | Fat mass, Fat-free mass |
| Scott et al., 2019 [34] | Obese adults | WB-HIIT vs. HIIT vs. MICT |
| WB-HIIT: 8–16 HIIT: 8–16 MICT: 30–50 | WB-HIIT: 60″/60″ HIIT: 60″/60″ | WB-HIIT: 12 wks, 3×/wk HIIT: 12 wks, 3×/wk MICT: 12 wks, 3×/wk | WB-HIIT: 432 HIIT: 432 MICT: 1440 | CRF, Fat mass, Fat-free mass, Metabolic risk factors |
| Study | Number of Participants | Male/Female | Age (Mean ± SD) | Cardiorespiratory Fitness | Body Composition | Musculoskeletal Fitness | Metabolic Risk Factors |
|---|---|---|---|---|---|---|---|
| Healthy participants | |||||||
| Ballesta-Garcia, 2019 [11] | 54 | 0/54 |
| - | - | Arm curl (rep): WB-HIIT↑ WB-MIIT ↔ CTL↑ 30s sit to stand (rep): WB-HIIT↑ WB-MIIT ↑ CTL↓ Timed up and go (s) WB-HIIT↓ WB-MIIT ↓ CTL↑ One leg stand (left) (s): WB-HIIT↑ WB-MIIT ↔ CTL↔ One leg stand (right) (s): WB-HIIT↔ WB-MIIT ↔ CTL↔ Right handgrip (kg): WB-HIIT↔ WB-MIIT ↔ CTL↔ Left handgrip (kg): WB-HIIT↔ WB-MIIT ↔ CTL↔ | - |
| Ballesta-Garcia, 2020 [12] | 54 | 0/54 |
| VO2max: WB-HIIT↑ WB-MIIT ↑ CTL↔ | - | - | - |
| Blackwell et al., 2017 [20] | 12 | - |
| VO2max: WB-HIIT↑ HIIT↑ | - | - | SBP (mmHg): WB-HIIT↔ HIIT↔ DBP (mmHg): WB-HIIT↔ HIIT↔ |
| * Connolly et al., 2020 [18] | 24 | 0/24 |
| - | - | - | SBP (mmHg): WB-HIIT↔ CTL↔ DBP (mmHg): WB-HIIT↔ CTL↔ Fasting glucose (mmol/L): WB-HIIT↔ CTL↔ HDL-C (mmol/L): WB-HIIT↑ CTL↔ LDL-C (mmol/L): WB-HIIT↔ CTL↔ Visceral fat (cm3): WB-HIIT↔ CTL↔ |
| Engel et al., 2019 [22] | 20 | 10/10 |
| - | - | Leg press (rep): WB-HIIT↑ CTL↔ Chest press (rep): WB-HIIT↑ CTL↔ Pulldown (rep): WB-HIIT↑ CTL↔ Back extension (rep): WB-HIIT↔ CTL↔ Ventral plank (s): WB-HIIT↔ CTL↔ Left plank (s): WB-HIIT↑ CTL↔ Right plank (s): WB-HIIT↔ CTL↔ | SBP (mmHg): WB-HIIT↔, CTL↔ DBP (mmHg): WB-HIIT↔ CTL↔ |
| Evangelista et al., 2019 [23] | 25 | - |
| - | Fat mass (kg): WB-HIIT↔ VICT↔ Lean mass (kg): WB-HIIT↔ VICT↔ | Abdominal (rep): WB-HIIT↔ VICT↔ Horizontal jump (min): WB-HIIT↔ VICT↔ Push-ups (rep): WB-HIIT↔ VICT↔ | - |
| Evangelista et al., 2021 [24] | 34 | 34/0 |
| VO2max: WB-HIIT↑ CTL ↔ | - | Push-ups (rep): WB-HIIT↑ CTL↔ Sit-ups (rep): WB-HIIT↑ CTL↔ Burpees: WB-HIIT↑ CTL↔ Leg press 1RM (kg): WB-HIIT↑ CTL↔ | - |
| Islam et al., 2019 [25] | 68 | 52/16 |
| VO2max: WB-HIIT↔ VICT↑ CTL↔ | - | Push-ups (rep): WB-HIIT↑ VICT↔ CTL↔ Right plank (s): WB-HIIT↑ VICT↔ CTL↔ Left plank (s): WB-HIIT↔ VICT↔ CTL↔ Back extension (s): WB-HIIT↔ VICT↔ CTL↔ Sit up (s): WB-HIIT↔ VICT↔ CTL↔ | - |
| Jimenez-Garcia et al., 2019 [21] | 73 | 20/62 |
| - | Body fat (%): WB-HIIT↔ WB-MIIT↔ CTL↔ Muscle Mass (kg): WB-HIIT↔ WB-MIIT↔ CTL↔ | Handgrip (kg): WB-HIIT↑ MIFT↔ CTL↔ | - |
| Lu et al., 2021 [26] | 20 | 0/20 |
| VO2max WB-HIIT ↑ HIIT ↑ | Body fat (%): WB-HIIT↓ HIIT↓ Lean mass (kg): WB-HIIT↑ HIIT↑ | Sit-ups (rep): WB-HIIT↑ HIIT↔ Push-ups (rep): WB-HIIT↔ HIIT↔ Broad jump (cm): WB-HIIT↑ HIIT↔ | - |
| * McRae et al., 2012 [16] | 22 | 0/22 |
| VO2max: WB-HIIT↑ MICT↑ CTL↔ | - | Leg extension (rep): WB-HIIT↑ MICT↔ CTL↔ Lateral pulldowns (rep): WB-HIIT↔ MICT↑ CTL↔ Chest press (rep): WB-HIIT↑ MICT↔ CTL↔ Push-ups (rep): WB-HIIT↑ MICT↔ CTL↔ Sit-ups (rep): WB-HIIT↑ MICT↔ CTL↔ Back extension (rep): WB-HIIT↑ MICT↔ CTL↔ | - |
| Menz et al., 2019 [27] | 15 | 4/11 |
| VO2max: WB-HIIT↑ HIIT↑ | Body fat (%): WB-HIIT↔ HIIT↔ Muscle percentage (%): WB-HIIT↔ HIIT↔ | Push-ups (rep): WB-HIIT↔ HIIT↔ Toes to bar (rep): WB-HIIT↑ HIIT↔ Burpees (rep): WB-HIIT↔ HIIT↑ Broad Jump (m): WB-HIIT↔ HIIT↔ | - |
| Micielska et al., 2019 [28] | 33 | 0/33 |
| VO2max: WB-HIIT↑ CTL↔ | Fat mass (kg): WB-HIIT↔, CTL↔ Muscle mass (kg): WB-HIIT↔ CTL↔ | - | - |
| Murawska-Cialowicz et al., 2020 [29] | 25 | 25/0 |
| VO2max: WB-HIIT↑ CTL↔ | Fat mass (kg): WB-HIIT↓ CTL↓ Muscle mass (kg): WB-HIIT↑ CTL↔ | - | - |
| Schaun et al., 2018 [13] | 41 | 41/0 |
| VO2max: WB-HIIT↑ HIIT↑ VICT↑ | Body fat (%): WB-HIIT↓ HIIT↓ VICT↓ | - | - |
| Schaun et al., 2019 [14] | 41 | 41/0 |
| - | - | Counter movement jump height (cm): WB-HIIT↑ HIIT↑ VICT↑ Counter movement jump peak power (W): WB-HIIT↑ HIIT↑ VICT↔ Squat jump height (cm): WB-HIIT↑ HIIT↑ VICT↑ Squat jump peak power (W): WB-HIIT↑ HIIT↑ VICT↑ | - |
| Schmidt et al., 2016 [30] | 96 | 43/53 |
| VO2max Male: WB-HIIT 7↔ WB-HIIT 14↔ CTL↔ VO2max Female: WB-HIIT 7↔ WB-HIIT 14↑ CTL↔ | Body fat Male (%): WB-HIIT-7↔ WB-HIIT-14↔ CTL↔ Body fat Female (%): WB-HIIT-7↔ WB-HIIT-14↔ CTL↔ | Right handgrip Male (kg): WB-HIIT 7↔ WB-HIIT 14↑ CTL↔ Left handgrip Male (kg): WB-HIIT-7↑ WB-HIIT-14↔ CTL↔ Push-ups Male (rep): WB-HIIT-7↑ WB-HIIT-14↑ CTL↔ Right handgrip Female (kg): WB-HIIT-7↔ WB-HIIT-14↔ CTL↔ Left handgrip Female (kg): WB-HIIT-7↔ WB-HIIT-14↔ CTL↔ Push-ups Female (rep): WB-HIIT-7↑ WB-HIIT-14↑ CTL↔ | - |
| Sperlich et al., 2018 [31] | 24 | 10/14 |
| VO2max: WB-HIIT-LV↔ WB-HIIT-HV↔ CTL↔ | Fat mass (kg): WB-HIIT-LV↔ WB-HIIT-HV↔ CTL↔ Muscle percentage (%): WB-HIIT-LV↔ WB-HIIT-HV↔ CTL↔ | Push-ups (rep): WB-HIIT-LV↑ WB-HIIT-HV↑ CTL↔ Leg-levers (rep): WB-HIIT-LV ↑ WB-HIIT-HV↑ CTL ↔ Burpees (rep): WB-HIIT- LV ↑ WB-HIIT-HV↑ CTL↔ | - |
| * Wilke et al., 2019 [17] | 33 | 12/21 |
| VO2max: WB-HIIT↔ MICT↔ | - | Leg press 1RM (kg): WB-HIIT↑ MICT↔ Chest press 1RM (kg): WB-HIIT↑ MICT↔ Single leg hop distance (cm): WB-HIIT↔ MICT↔ Counter movement jump (cm): WB-HIIT↔ MICT↔ | - |
| Specific populations | |||||||
| Batrakoulis et al., 2018 [32] | 35 | 0/35 |
| VO2max: WB-HIIT↑ CTL↔ | Fat mass (kg): WB-HIIT↓ CTL↔ Fat-free mass (kg): WB-HIIT↑ CTL↔ | Leg press 1RM (kg): WB-HIIT↑ CTL↔ | - |
| Jung et al., 2019 [33] | 26 | 0/26 |
| - | Body fat (%): WB-HIIT↓ CTL↔ Fat-free mass (kg): WB-HIIT↑ CTL↔ | - | - |
| Scott et al., 2019 [34] | 32 | 13/19 |
| VO2max: WB-HIIT↑ HIIT↑ MICT↑ | Body fat (%): WB-HIIT↓ HIIT↓ MICT↓ Lean mass (kg): WB-HIIT↔ HIIT↔ MICT↔ | - | Fasting glucose (mmol/L): WB-HIIT↔ HIIT↔ MICT↔ HDL-C (mmol/L): WB-HIIT↔ HIIT↔ MICT↔ LDL-C (mmol/L): WB-HIIT↔ HIIT↔ MICT↔ SBP (mmHg): WB-HIIT↔ HIIT↔ MICT↔ DBP (mmHg): WB-HIIT↔ HIIT↔ MICT↔ Visceral fat (g): WB-HIIT↓ HIIT↓ MICT↓ |
| Studies | Inclusion Criteria | Random Allocation | Concealed Allocation | Groups Similar at Baseline | Blinded Participants | Blinded Therapist | Blinded Investigators | Data from >85% of Participants | Intention to Treat | Between Group Comparison | Estimation of Effect and Variability | TOTAL |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ballesta-Garcia, 2019 [11] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Ballesta-Garcia, 2020 [12] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Blackwell et al., 2017 [20] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Connolly et al., 2020 [18] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 6 |
| Engel et al., 2019 [22] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Evangelista et al., 2019 [23] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Evangelista et al., 2021 [24] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Islam et al., 2019 [25] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Jimenez-Garcia et al., 2019 [21] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 7 |
| Lu et al., 2021 [26] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| McRae et al., 2012 [16] | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 4 |
| Menz et al., 2019 [27] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Micielska et al., 2019 [28] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
| Murawska-Cialowicz et al., 2020 [29] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Schaun et al., 2018 [13] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Schaun et al., 2019 [14] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Schmidt et al., 2016 [30] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Sperlich et al., 2018 [31] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Wilke et al., 2019 [17] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Batrakoulis et al., 2018 [32] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Jung et al., 2019 [33] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 6 |
| Scott et al., 2019 [34] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 1 | 1 | 1 | 5 |
3.3. Characteristics of the Included Studies
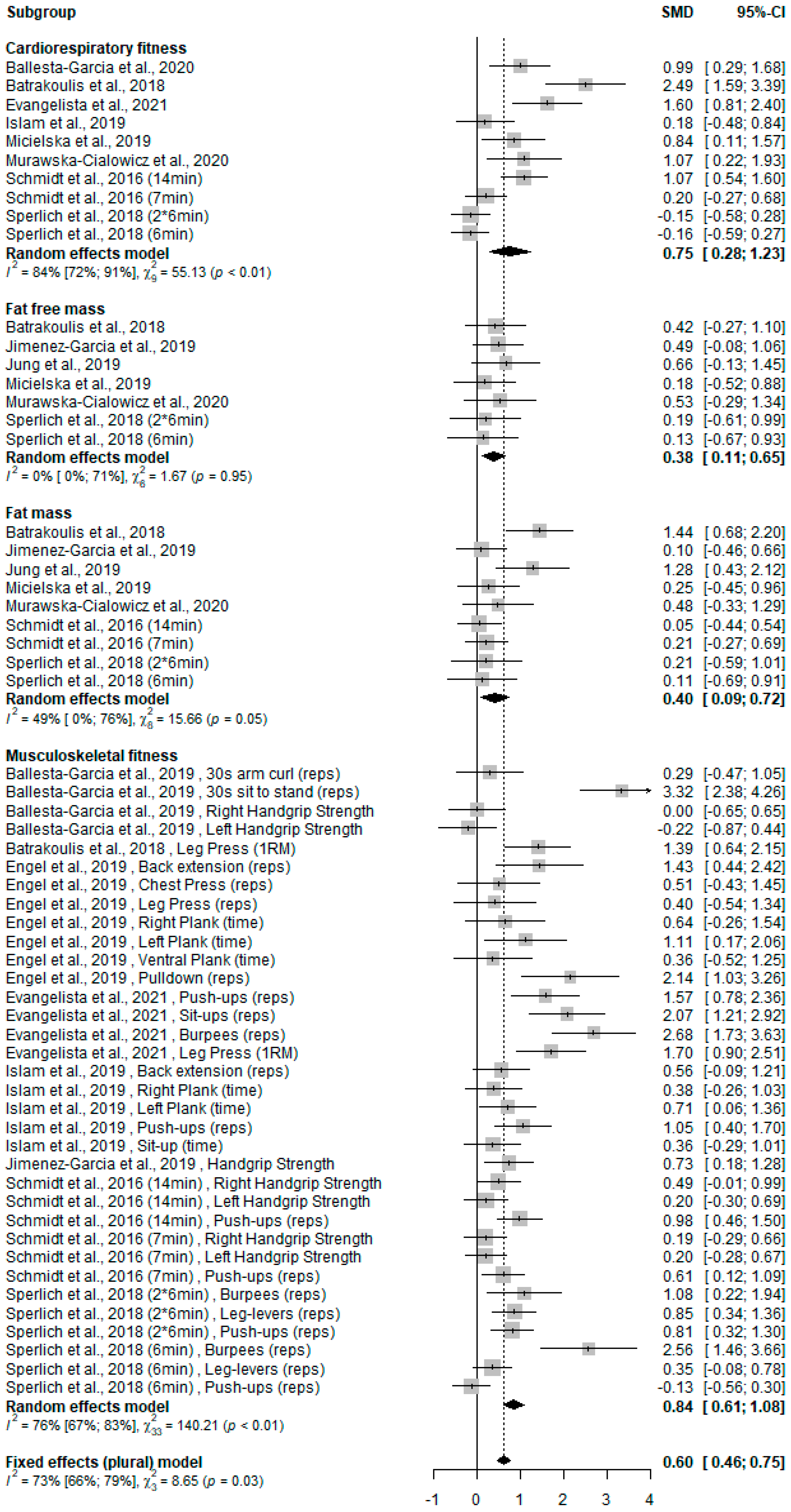
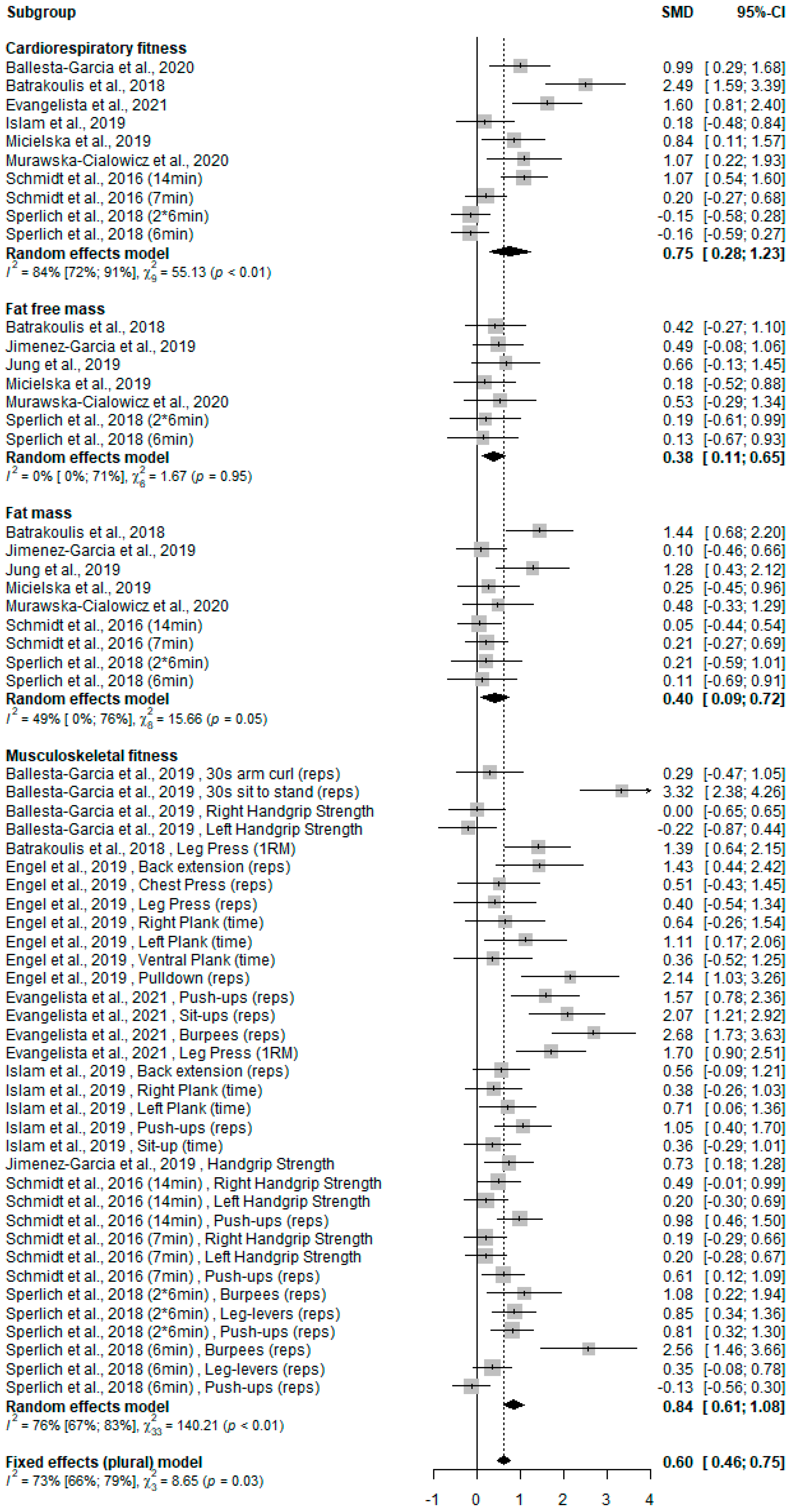
3.4. WB-HIIT Compared to No Exercise
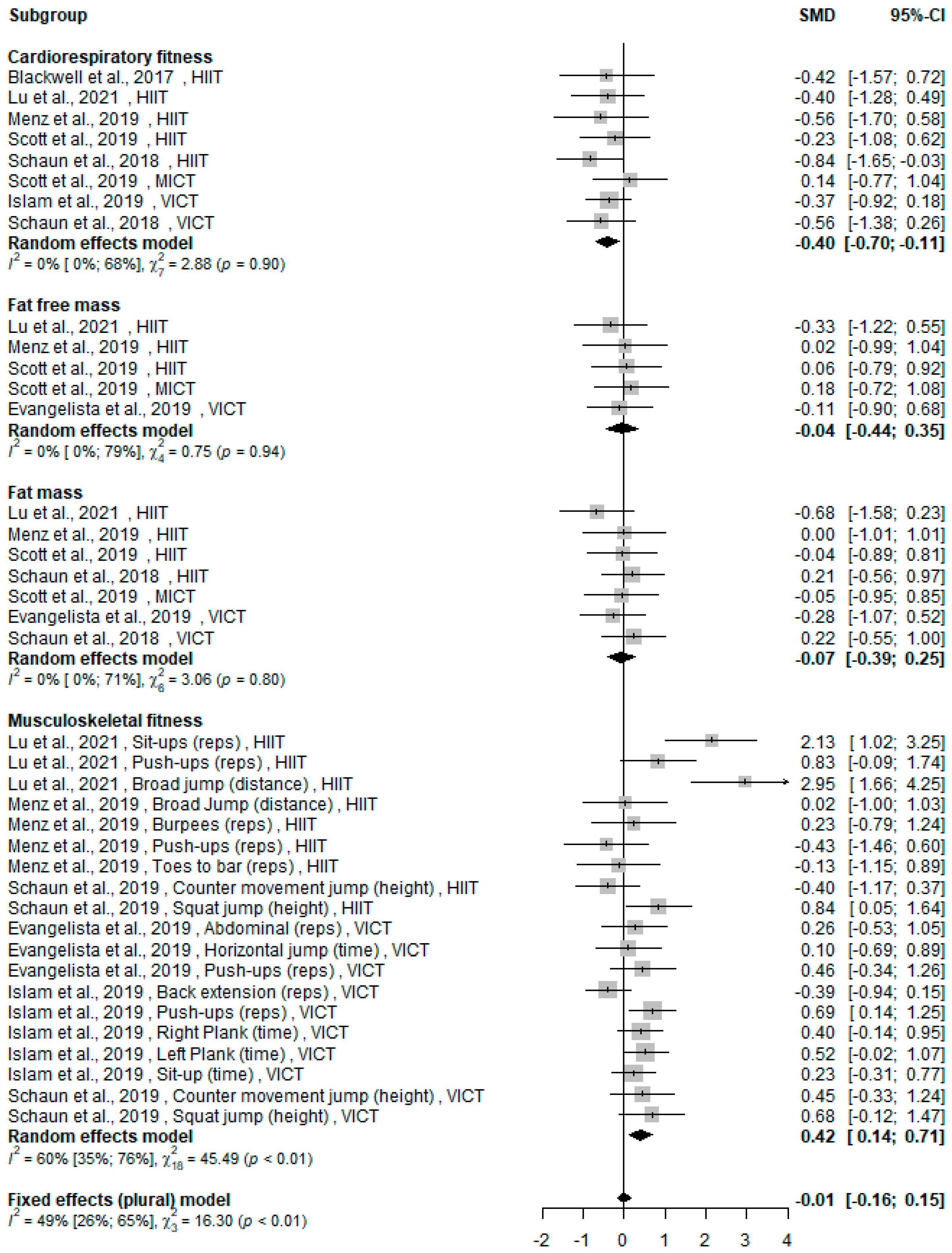
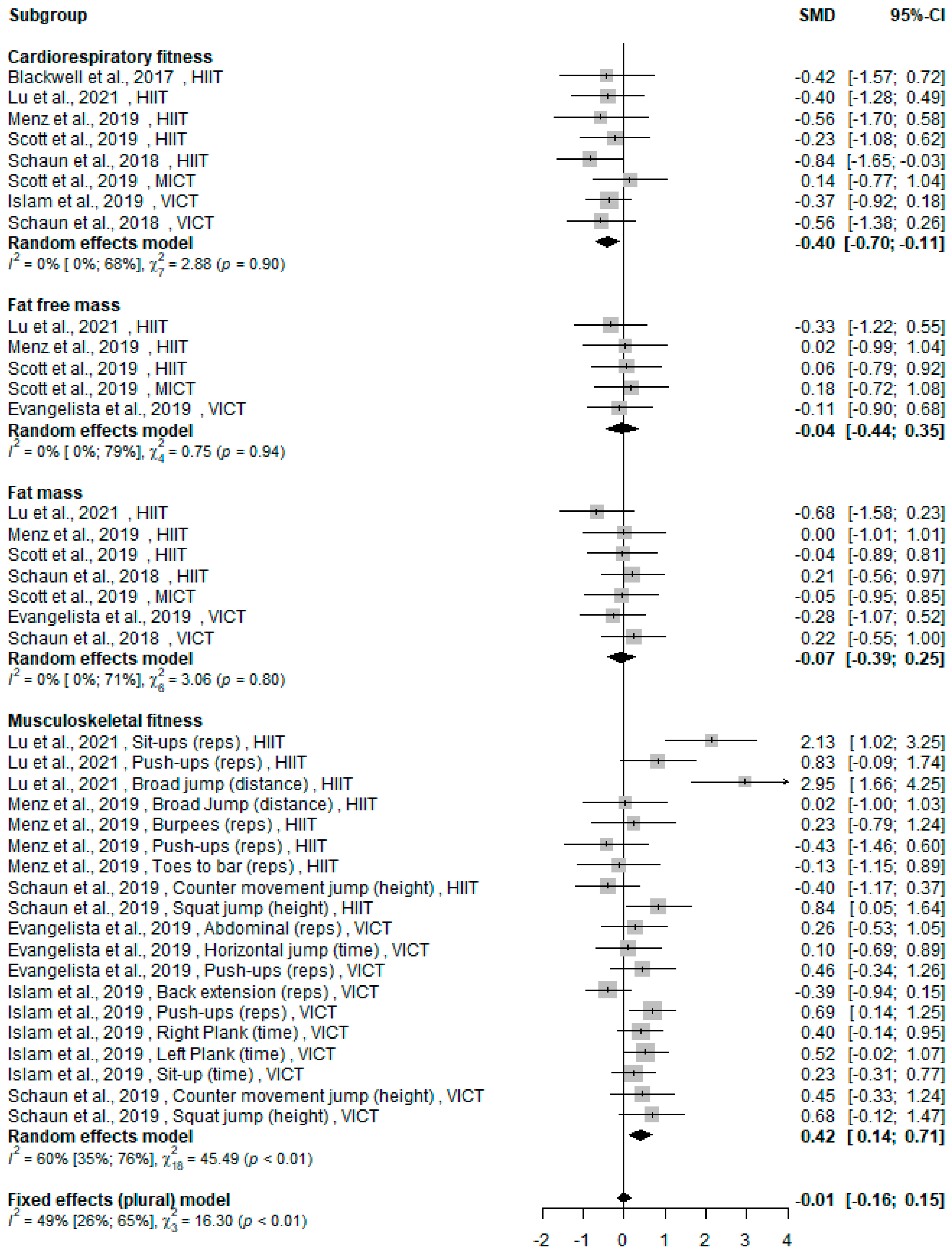
3.5. WB-HIIT vs. Traditional Aerobic Training
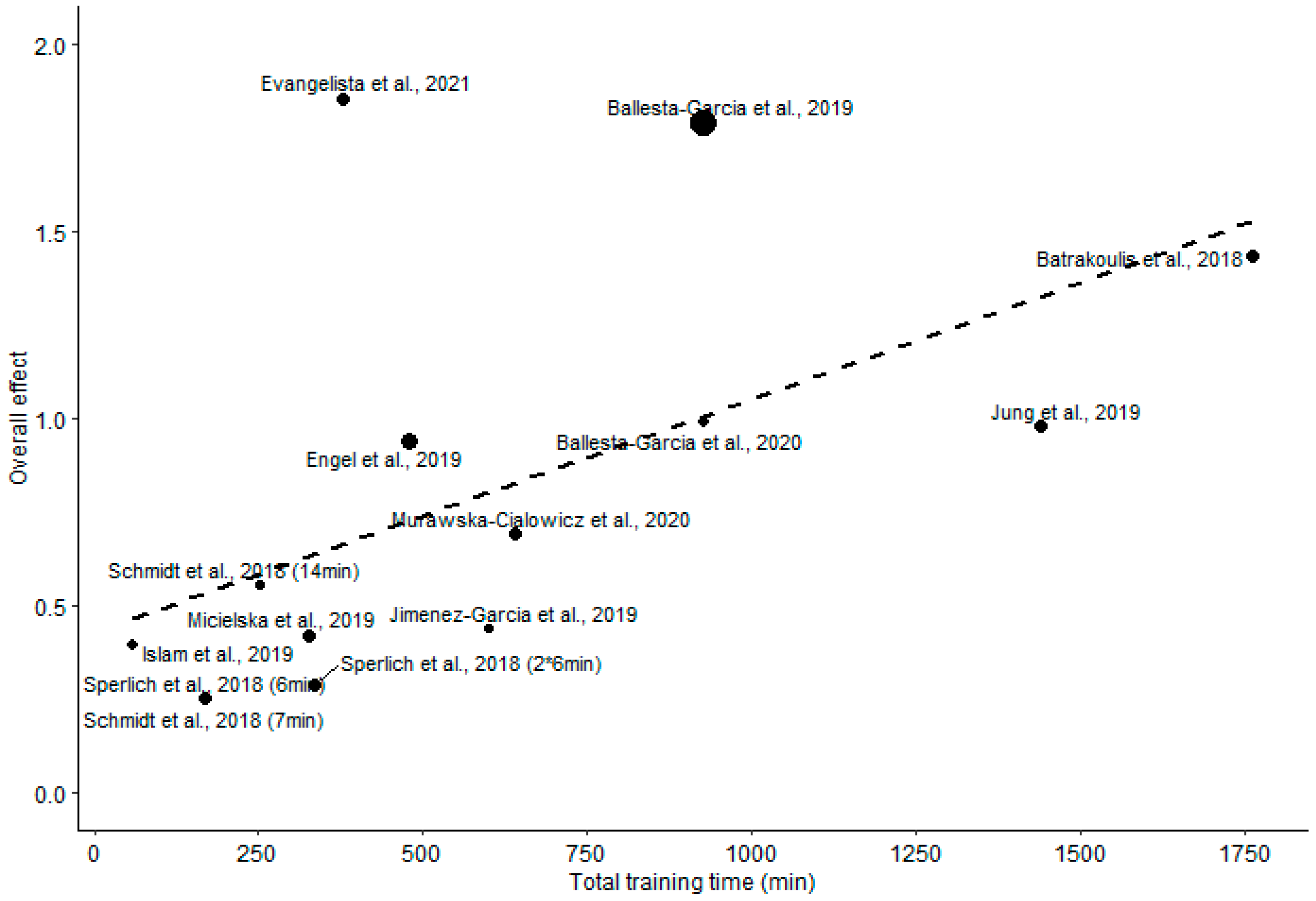
3.6. Total Training Time
4. Discussion
4.1. Cardiorespiratory Fitness
4.2. Fat Mass and Fat-Free Mass
4.3. Musculoskeletal Fitness
4.4. Metabolic Risk Factors
4.5. Limitations and Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spiteri, K.; Broom, D.; Bekhet, A.H.; de Caro, J.X.; Laventure, B.; Grafton, K. Barriers and Motivators of Physical Activity Participation in Middle-Aged and Older Adults—A Systematic Review. J. Aging Phys. Act. 2019, 27, 929–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feito, Y.; Heinrich, K.; Butcher, S.; Poston, W. High-Intensity Functional Training (HIFT): Definition and Research Implications for Improved Fitness. Sports 2018, 6, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, W.R. Worldwide survey of fitness trends for 2020. Acsm’s Health Fit. J. 2019, 23, 10–18. [Google Scholar] [CrossRef]
- Milanović, Z.; Sporis, G.; Weston, M. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J.; Mohr, L. Chronic effects of high-intensity functional training on motor function: A systematic review with multilevel meta-analysis. Sci. Rep. 2020, 10, 21680. [Google Scholar] [CrossRef]
- Machado, A.F.; Baker, J.S.; Junior, A.F.; Bocalini, D.S. High-intensity interval training using whole-body exercises: Training recommendations and methodological overview. Clin. Physiol. Funct. Imaging 2017, 39, 378–383. [Google Scholar] [CrossRef]
- Knapik, J.J. Injuries During High-Intensity Functional Training. J. Spéc. Oper. Med. A Peer Rev. J. SOF Med. Prof. 2021, 21, 112. [Google Scholar] [CrossRef]
- American College of Sport Medicine. ACSM’s Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer: Alphen aan den Rijn, The Netherlands, 2014. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. BMJ (Clin. Res. Ed.) 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Srikanthan, K.; Feyh, A.; Visweshwar, H.; Shapiro, J.I.; Sodhi, K. Systematic Review of Metabolic Syndrome Biomarkers: A Panel for Early Detection, Management, and Risk Stratification in the West Virginian Population. Int. J. Med. Sci. 2016, 13, 25–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballesta-García, I.; Martínez-González-Moro, I.; Rubio-Arias, J.Á.; Carrasco-Poyatos, M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Functional Ability and Body Mass Index in Middle-Aged and Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 4205. [Google Scholar] [CrossRef] [Green Version]
- Ballesta-García, I.; Martínez-González-Moro, I.; Ramos-Campo, D.J.; Carrasco-Poyatos, M. High-Intensity Interval Circuit Training Versus Moderate-Intensity Continuous Training on Cardiorespiratory Fitness in Middle-Aged and Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 1805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaun, G.Z.; Pinto, S.S.; Silva, M.R.; Dolinski, D.B.; Alberton, C.L. Whole-body high-intensity interval training induce similar car-diorespiratory adaptations compared with traditional high-intensity interval training and moderate-intensity continuous training in healthy men. J. Strength Cond. Res. 2018, 32, 2730–2742. [Google Scholar] [CrossRef] [PubMed]
- Schaun, G.Z.; Pinto, S.S.; Brasil, B.; Nunes, G.N.; Alberton, C.L. Neuromuscular adaptations to sixteen weeks of whole-body high-intensity interval training compared to ergometer-based interval and continuous training. J. Sports Sci. 2019, 37, 1561–1569. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, R.; Turicchi, J.; Beaulieu, K.; Scott, S.; Matu, J.; Deighton, K.; Finlayson, G.; Stubbs, R.J. How well do activity monitors estimate energy expenditure? A systematic review and meta-analysis of the validity of current technologies. Br. J. Sports Med. 2018, 54, 332–340. [Google Scholar] [CrossRef] [PubMed]
- McRae, G.; Payne, A.; Zelt, J.G.; Scribbans, T.D.; Jung, M.E.; Little, J.P.; Gurd, B.J. Extremely low volume, whole-body aerobic- resistance training improves aerobic fitness and muscular endurance in females. App. Physiol Nutr. Metab. 2012, 37, 1124–1131. [Google Scholar] [CrossRef]
- Wilke, J.; Kaiser, S.; Niederer, D.; Kalo, K.; Engeroff, T.; Morath, C.; Vogt, L.; Banzer, W. Effects of high-intensity functional circuit training on motor function and sport motivation in healthy, inactive adults. Scand. J. Med. Sci. Sports 2019, 29, 144–153. [Google Scholar] [CrossRef] [Green Version]
- Connolly, L.J.; Scott, S.; Morencos, C.M.; Fulford, J.; Jones, A.M.; Knapp, K.; Krustrup, P.; Bailey, S.J.; Bowtell, J.L. Impact of a novel home-based exercise intervention on health indicators in inactive premenopausal women: A 12-week randomised controlled trial. Eur. J. Appl. Physiol. 2020, 120, 771–782. [Google Scholar] [CrossRef]
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- Blackwell, J.; Atherton, P.J.; Smith, K.; Doleman, B.; Williams, J.P.; Lund, J.; Phillips, B. The efficacy of unsupervised home-based exercise regimens in comparison to supervised laboratory-based exercise training upon cardio-respiratory health facets. Physiol. Rep. 2017, 5, e13390. [Google Scholar] [CrossRef]
- Jiménez-García, J.D.J.; Martínez-Amat, A.; De La Torre-Cruz, M.J.; Fábrega-Cuadros, R.; Díaz, D.C.; Aibar-Almazán, A.; Achalandabaso-Ochoa, A.; Hita-Contreras, F. Suspension Training HIIT Improves Gait Speed, Strength and Quality of Life in Older Adults. Int. J. Sports Med. 2019, 40, 116–124. [Google Scholar] [CrossRef]
- Engel, F.A.; Rappelt, L.; Held, S.; Donath, L. Can High-Intensity Functional Suspension Training over Eight Weeks Improve Resting Blood Pressure and Quality of Life in Young Adults? A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2019, 16, 5062. [Google Scholar] [CrossRef] [Green Version]
- Evangelista, A.L.; Teixeira, C.V.L.S.; Machado, A.F.; Pereira, P.E.; Rica, R.L.; Bocalini, D.S. Effects of a short-term of whole-body, high-intensity, intermittent training program on morphofunctional parameters. J. Bodyw. Mov. Ther. 2019, 23, 456–460. [Google Scholar] [CrossRef] [PubMed]
- Evangelista, A.L.; Brigatto, F.A.; De Camargo, J.B.; Braz, T.V.; Bocalini, D.S.; Teixeira, C.V.; Paunksnis, M.R.; Barros, B.M.; Santos, L.M.; Carnevali, L.C., Jr. Effect of a short-term whole-body high-intensity interval training on fitness, morphological, and functional parameters in untrained individuals. J. Sports Med. Phys. Fit. 2021. [Google Scholar] [CrossRef] [PubMed]
- Islam, H.; Siemens, T.L.; Matusiak, J.B.; Sawula, L.; Bonafiglia, J.T.; Preobrazenski, N.; Jung, M.E.; Gurd, B.J. Cardiorespiratory fitness and muscular endurance responses immediately and 2 months after a whole-body Tabata or vigorous-intensity continuous training intervention. Appl. Physiol. Nutr. Metab. 2020, 45, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Wiltshire, H.D.; Baker, J.S.; Wang, Q. The Effects of Running Compared with Functional High-Intensity Interval Training on Body Composition and Aerobic Fitness in Female University Students. Int. J. Environ. Res. Public Health 2021, 18, 11312. [Google Scholar] [CrossRef]
- Menz, V.; Marterer, N.; Amin, S.B.; Faulhaber, M.; Hansen, A.B.; Lawley, J.S. Functional Vs. Running Low-Volume High-Intensity Interval Training: Effects on VO2max and Muscular Endurance. J. Sports Sci. Med. 2019, 18, 497–504. [Google Scholar]
- Micielska, K.; Gmiat, A.; Zychowska, M.; Kozlowska, M.; Walentukiewicz, A.; Lysak-Radomska, A.; Jaworska, J.; Rodziewicz, E.; Duda-Biernacka, B.; Ziemann, E. The beneficial effects of 15 units of high-intensity circuit training in women is modified by age, baseline insulin resistance and physical capacity. Diabetes Res. Clin. Pract. 2019, 152, 156–165. [Google Scholar] [CrossRef]
- Murawska-Cialowicz, E.; Wolanski, P.; Zuwala-Jagiello, J.; Feito, Y.; Petr, M.; Kokstejn, J.; Stastny, P.; Goliński, D. Effect of HIIT with Tabata Protocol on Serum Irisin, Physical Performance, and Body Composition in Men. Int. J. Environ. Res. Public Health 2020, 17, 3589. [Google Scholar] [CrossRef]
- Schmidt, D.; Anderson, K.; Graff, M.; Strutz, V. The effect of high-intensity circuit training on physical fitness. J. Sports Med. Phys. Fit. 2015, 56, 534–540. [Google Scholar]
- Sperlich, B.; Hahn, L.-S.; Edel, A.; Behr, T.; Helmprobst, J.; Leppich, R.; Wallmann-Sperlich, B.; Holmberg, H.-C. A 4-Week Intervention Involving Mobile-Based Daily 6-Minute Micro-Sessions of Functional High-Intensity Circuit Training Improves Strength and Quality of Life, but Not Cardio-Respiratory Fitness of Young Untrained Adults. Front. Physiol. 2018, 9, 423. [Google Scholar] [CrossRef] [Green Version]
- Batrakoulis, A.; Jamurtas, A.Z.; Georgakouli, K.; Draganidis, D.; Deli, C.K.; Papanikolaou, K.; Avloniti, A.; Chatzinikolaou, A.; Leontsini, D.; Tsimeas, P.; et al. High intensity, circuit-type integrated neuromuscular training alters energy balance and reduces body mass and fat in obese women: A 10-month training-detraining randomized controlled trial. PLoS ONE 2018, 13, e0202390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, W.-S.; Kim, Y.-Y.; Park, H.-Y. Circuit Training Improvements in Korean Women with Sarcopenia. Percept. Mot. Ski. 2019, 126, 828–842. [Google Scholar] [CrossRef] [PubMed]
- Scott, S.N.; Shepherd, S.O.; Hopkins, N.; Dawson, E.A.; Strauss, J.A.; Wright, D.J.; Cooper, R.G.; Kumar, P.; Wagenmakers, A.J.M.; Cocks, M. Home-hit improves muscle capillarisation and eNOS/NAD(P)Hoxidase protein ratio in obese individuals with elevated cardiovascular disease risk. J. Physiol. 2019, 597, 4203–4225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, G.; Wang, R.; Chen, P.; Huang, S.C.; Donnelly, J.E.; Mehlferber, J.P. Dose–response relationship of cardiorespiratory fitness adaptation to controlled endurance training in sedentary older adults. Eur. J. Prev. Cardiol. 2015, 23, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, T.; Saotome, K.; Seino, S.; Shimojo, N.; Matsushita, A.; Iemitsu, M.; Ohshima, H.; Tanaka, K.; Mukai, C. Effects of a Low-Volume Aerobic-Type Interval Exercise on VO2max and Cardiac Mass. Med. Sci. Sports Exerc. 2014, 46, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Sultana, R.N.; Sabag, A.; Keating, S.E.; Johnson, N.A. The Effect of Low-Volume High-Intensity Interval Training on Body Com-position and Cardiorespiratory Fitness: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 1687–1721. [Google Scholar] [CrossRef]
- Callahan, M.J.; Parr, E.B.; Hawley, J.A.; Camera, D.M. Can High-Intensity Interval Training Promote Skeletal Muscle Anabolism? Sports Med. 2021, 51, 405–421. [Google Scholar] [CrossRef] [PubMed]
- Honorato, R.D.C.; Franchini, E.; Lara, J.P.R.; Fonteles, A.I.; Pinto, J.C.B.D.L.; Mortatti, A.L. Differences in Handgrip Strength-Endurance and Muscle Activation Between Young Male Judo Athletes and Untrained Individuals. Res. Q. Exerc. Sport 2021, 92, 1–10. [Google Scholar] [CrossRef]
- Heinrich, K.M.; Becker, C.; Carlisle, T.; Gilmore, K.; Hauser, J.; Frye, J.; Harms, C.A. High-intensity functional training improves functional movement and body composition among cancer survivors: A pilot study. Eur. J. Cancer Care 2015, 24, 812–817. [Google Scholar] [CrossRef]
- Beaudart, C.; Rolland, Y.; Cruz-Jentoft, A.J.; Bauer, J.M.; Sieber, C.; Cooper, C.; Al-Daghri, N.; De Carvalho, I.A.; Bautmans, I.; Bernabei, R.; et al. Assessment of Muscle Function and Physical Performance in Daily Clinical Practice. Calcif. Tissue Int. 2019, 105, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Komar, J.; Ong, C.Y.Y.; Choo, C.Z.Y.; Chow, J.Y. Perceptual-motor skill transfer: Multidimensionality and specificity of both general and specific transfers. Acta Psychol. 2021, 217, 103321. [Google Scholar] [CrossRef] [PubMed]
- MacInnis, M.J.; Gibala, M.J. Physiological adaptations to interval training and the role of exercise intensity. J. Physiol. 2017, 595, 2915–2930. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. Available online: http://www.prisma-statement.org (accessed on 7 March 2022). [CrossRef] [PubMed]

| Parameters | K | Beta (SE) | p Value |
|---|---|---|---|
| Overall effect | 14 | 0.036 (0.012) | 0.004 |
| Cardiorespiratory fitness | 10 | 0.078 (0.024) | 0.001 |
| Fat-free mass | 7 | 0.012 (0.018) | 0.41 |
| Fat mass | 9 | 0.048 (0.012) | <0.001 |
| Musculoskeletal fitness | 10 | 0.030 (0.018) | 0.1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scoubeau, C.; Bonnechère, B.; Cnop, M.; Faoro, V.; Klass, M. Effectiveness of Whole-Body High-Intensity Interval Training on Health-Related Fitness: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 9559. https://doi.org/10.3390/ijerph19159559
Scoubeau C, Bonnechère B, Cnop M, Faoro V, Klass M. Effectiveness of Whole-Body High-Intensity Interval Training on Health-Related Fitness: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(15):9559. https://doi.org/10.3390/ijerph19159559
Chicago/Turabian StyleScoubeau, Corentin, Bruno Bonnechère, Miriam Cnop, Vitalie Faoro, and Malgorzata Klass. 2022. "Effectiveness of Whole-Body High-Intensity Interval Training on Health-Related Fitness: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 15: 9559. https://doi.org/10.3390/ijerph19159559
APA StyleScoubeau, C., Bonnechère, B., Cnop, M., Faoro, V., & Klass, M. (2022). Effectiveness of Whole-Body High-Intensity Interval Training on Health-Related Fitness: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 19(15), 9559. https://doi.org/10.3390/ijerph19159559