
Reduced Shear Stress and Longer Blood Flow Time Occur in Both Severe Focal and Mild Diffuse LAD Lesions: Angiograms Alone Don’t Always Reveal Their True Impact on Blood Flow

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. CCTA Protocol
2.3. Computational Fluid Dynamics
2.4. Statistical Analysis
3. Results
3.1. General Population
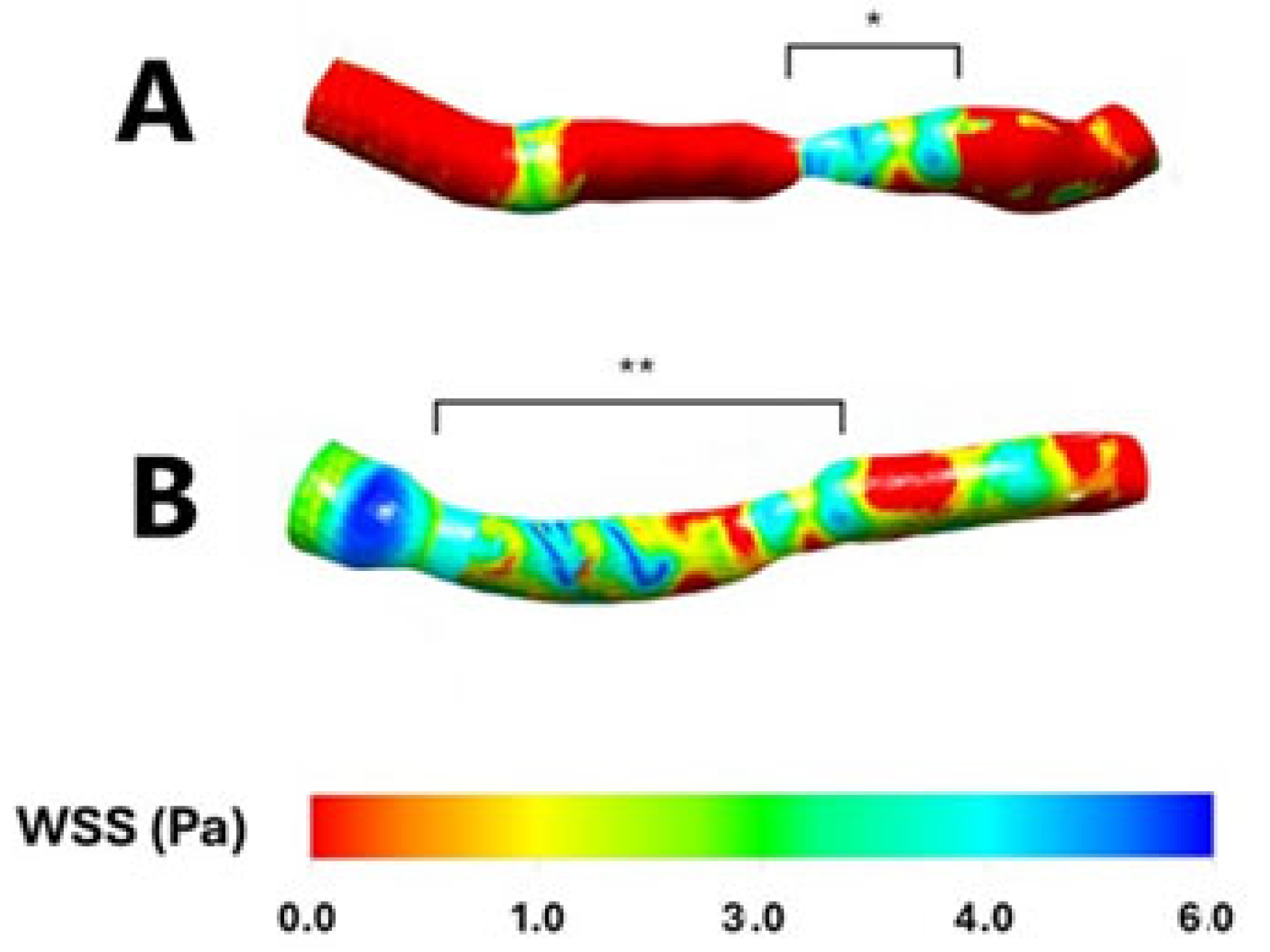
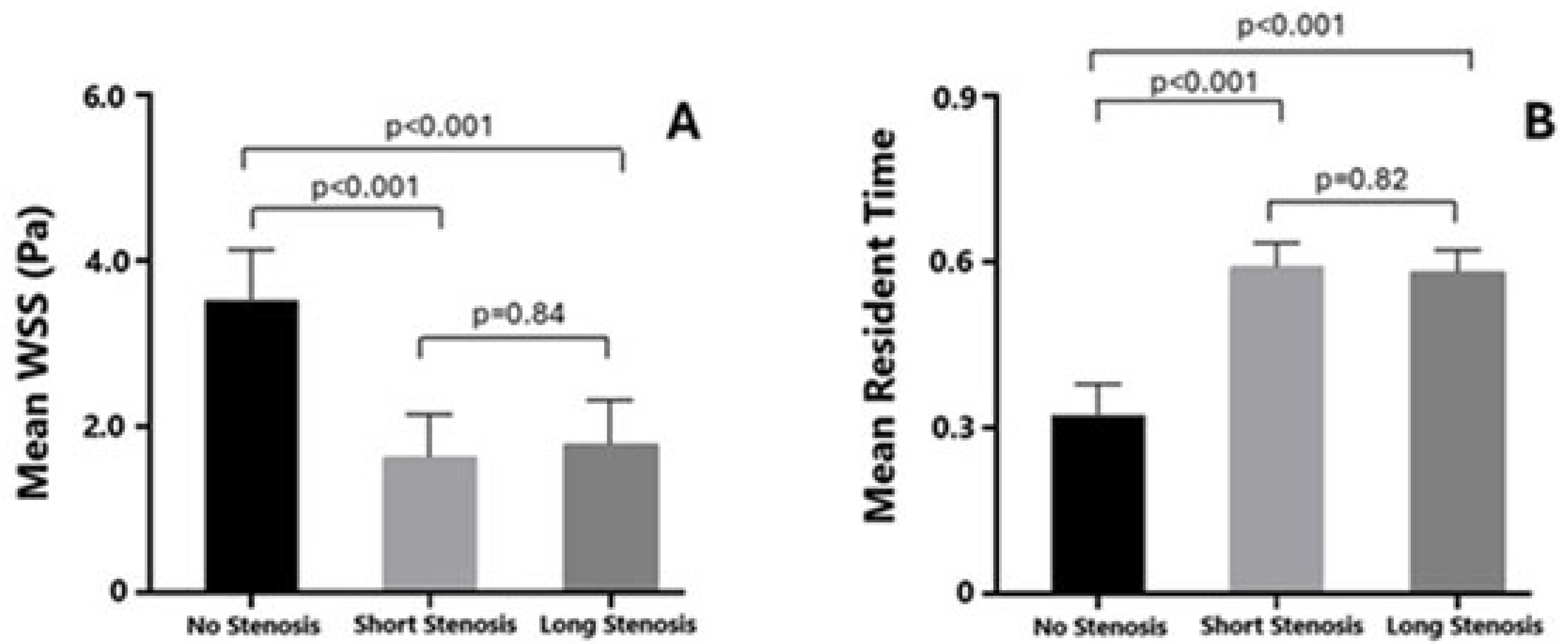
3.2. WSS
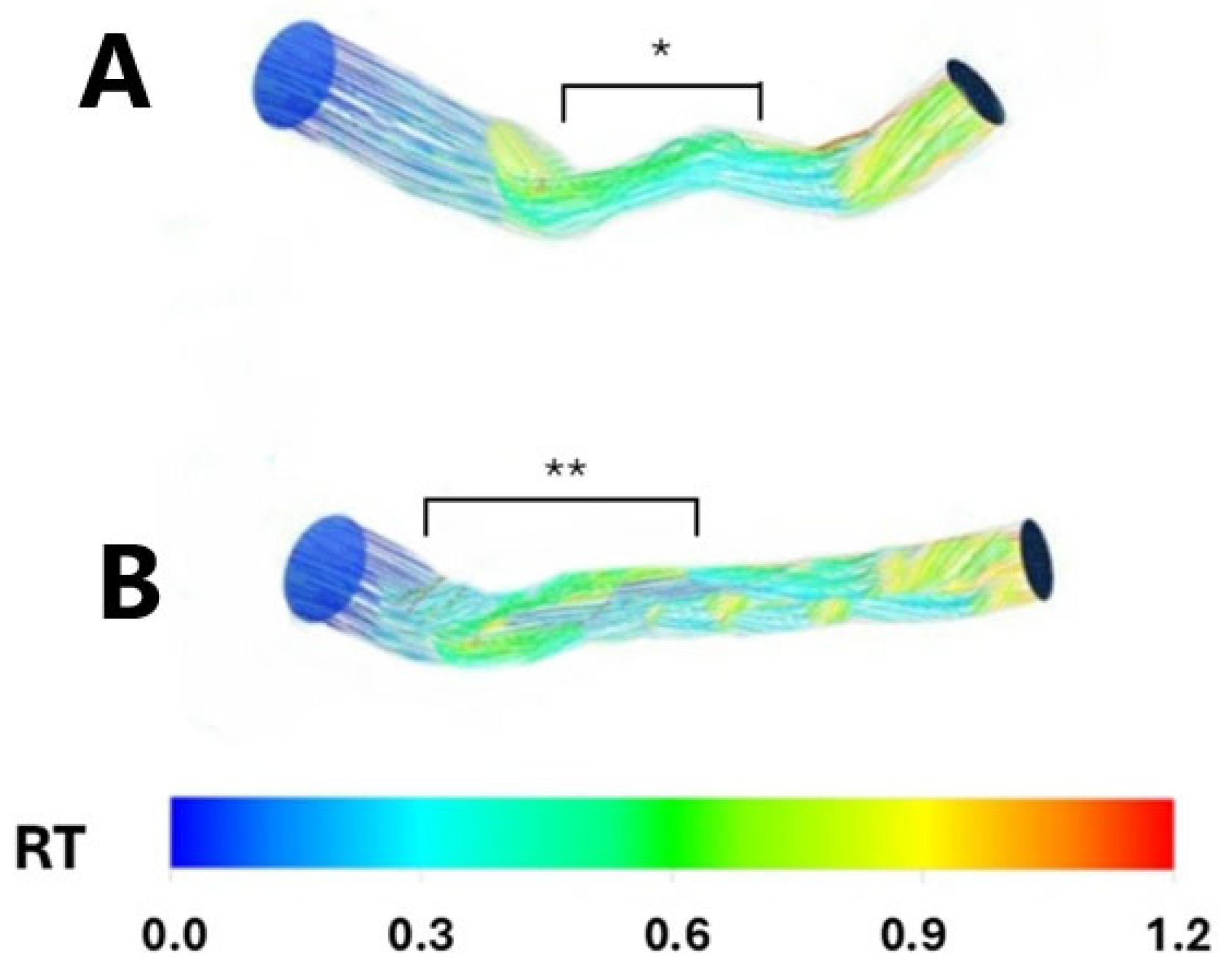
3.3. RT
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CCTA | Computed Tomography Angiography |
| CFD | Computational Fluid Dynamic |
| FFR | Fractional Flow Reserve |
| LAD | Left Anterior Descending |
| RT | Resident Time |
| WSS | Wall Shear Stress |
References
- Collet, C.; Grundeken, M.J.; Asano, T.; Onuma, Y.; Wijns, W.; Serruys, P.W. State of the art: Coronary angiography. EuroIntervention 2017, 13, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Tonino, P.A.; De Bruyne, B.; Pijls, N.H.; Siebert, U.; Ikeno, F.; van’ t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; Oldroyd, K.G.; et al. FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N. Engl. J. Med. 2009, 360, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Pijls, N.H.; Fearon, W.F.; Tonino, P.A.; Siebert, U.; Ikeno, F.; Bornschein, B.; van’t Veer, M.; Klauss, V.; Manoharan, G.; Engstrøm, T.; et al. FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention in patients with multivessel coronary artery disease: 2-year follow-up of the FAME (Fractional Flow Reserve Versus Angiography for Multivessel Evaluation) study. J. Am. Coll. Cardiol. 2010, 56, 177–184. [Google Scholar] [PubMed]
- Naganuma, T.; Latib, A.; Costopoulos, C.; Takagi, K.; Naim, C.; Sato, K.; Miyazaki, T.; Kawaguchi, M.; Panoulas, V.F.; Basavarajaiah, S.; et al. The role of intravascular ultrasound and quantitative angiography in the functional assessment of intermediate coronary lesions: Correlation with fractional flow reserve. Cardiovasc. Revasc. Med. 2014, 15, 3–7. [Google Scholar] [CrossRef]
- Kang, D.Y.; Ahn, J.M.; Kim, Y.W.; Moon, J.Y.; Lee, J.S.; Koo, B.K.; Lee, P.H.; Park, D.W.; Kang, S.J.; Lee, S.W.; et al. Impact of Coronary Lesion Geometry on Fractional Flow Reserve: Data from Interventional Cardiology Research In-Cooperation Society-Fractional Flow Reserve and Intravascular Ultrasound Registry. Circ. Cardiovasc. Imaging 2018, 11, e007087. [Google Scholar] [CrossRef]
- Jaffe, R.; Halon, D.A.; Roguin, A.; Rubinshtein, R.; Lewis, B.S. A Poiseuille-based coronary angiographic index for prediction of fractional flow reserve. Int. J. Cardiol. 2013, 167, 862–865. [Google Scholar] [CrossRef]
- Blanke, P.; Weir-McCall, J.R.; Achenbach, S.; Delgado, V.; Hausleiter, J.; Jilaihawi, H.; Marwan, M.; Nørgaard, B.L.; Piazza, N.; Schoenhagen, P.; et al. Computed tomography imaging in the context of transcatheter aortic valve implantation (TAVI)/transcatheter aortic valve replacement (TAVR): An expert consensus document of the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2019, 13, 1–20. [Google Scholar] [CrossRef]
- Boutsianis, E.; Dave, H.; Frauenfelder, T.; Poulikakos, D.; Wildermuth, S.; Turina, M.; Ventikos, Y.; Zund, G. Computational simulation of intracoronary flow based on real coronary geometry. Eur. J. Cardiothorac. Surg. 2004, 26, 248–256. [Google Scholar] [CrossRef]
- Rigatelli, G.; Zuin, M.; Marchese, G.; Rodino, G.; Hiso, E.; Mileva, N.; Vassilev, D.; Pasquetto, G. Residence time in complex left main bifurcation disease after stenting. Cardiovasc. Revasc. Med. 2024, 61, 1–5. [Google Scholar] [CrossRef]
- Theodorakakos, A.; Gavaises, M.; Andriotis, A.; Zifan, A.; Liatsis, P.; Pantos, I.; Efstathopoulos, E.P.; Katritsis, D. Simulation of cardiac motion on non-Newtonian, pulsating flow development in the human left anterior descending coronary artery. Phys. Med. Biol. 2008, 53, 4875–4879. [Google Scholar] [CrossRef]
- Cho, Y.I.; Kensey, K.R. Effects of the non-Newtonian viscosity of blood on flows in a diseased arterial vessel. Part 1: Steady flows. Biorheology 1991, 28, 241–262. [Google Scholar] [CrossRef] [PubMed]
- Karino, T.; Goldsmith, H.L.; Motomiya, M.; Mabuchi, S.; Sohara, Y. Flow patterns in vessels of simple and complex geometries. Ann. N. Y. Acad. Sci. 1987, 516, 422–441. [Google Scholar] [CrossRef] [PubMed]
- Johnston, B.M.; Johnston, P.R.; Corney, S.; Kilpatrick, D. Non-Newtonian blood flow in human right coronary arteries: Steady state simulations. J. Biomech. 2004, 37, 709–720. [Google Scholar] [CrossRef] [PubMed]
- Zuin, M.; Chatzizisis, Y.S.; Beier, S.; Shen, C.; Colombo, A.; Rigatelli, G. Role of secondary flows in coronary artery bifurcations before and after stenting: What is known so far? Cardiovasc. Revasc. Med. 2023, 55, 83–87. [Google Scholar] [CrossRef]
- Zuin, M.; Rigatelli, G.; Vassilev, D.; Ronco, F.; Rigatelli, A.; Roncon, L. Computational fluid dynamic-derived wall shear stress of non-significant left main bifurcation disease may predict acute vessel thrombosis at 3-year follow-up. Heart Vessels 2020, 35, 297–306. [Google Scholar] [CrossRef]
- Chu, M.; von Birgelen, C.; Li, Y.; Westra, J.; Yang, J.; Holm, N.R.; Reiber, J.H.; Wijns, W.; Tu, S. Quantification of disturbed coronary flow by disturbed vorticity index and relation with fractional flow reserve. Atherosclerosis 2018, 273, 136–144. [Google Scholar] [CrossRef]
- Hashemi, J.; Patel, B.; Chatzizisis, Y.S.; Kassab, G.S. Study of Coronary Atherosclerosis Using Blood Residence Time. Front. Physiol. 2021, 12, 625420. [Google Scholar] [CrossRef]
- Ahn, J.M.; Kang, D.Y.; Lee, P.H.; Ahn, Y.K.; Kim, W.J.; Nam, C.W.; Jeong, J.O.; Chae, I.H.; Shiomi, H.; Kao, P.H.L.; et al. PREVENT Investigators. Preventive PCI or medical therapy alone for vulnerable atherosclerotic coronary plaque: Rationale and design of the randomized, controlled PREVENT trial. Am. Heart J. 2023, 264, 83–96. [Google Scholar] [CrossRef]
- Bacigalupi, E.; Pizzicannella, J.; Rigatelli, G.; Scorpiglione, L.; Foglietta, M.; Rende, G.; Mantini, C.; Fiore, F.M.; Pelliccia, F.; Zimarino, M. Biomechanical factors and atherosclerosis localization: Insights and clinical applications. Front. Cardiovasc. Med. 2024, 11, 1392702. [Google Scholar] [CrossRef]
- Wang, X.; Song, C.; Liu, H.; Zhou, L.; Zhang, L. Differences in severity of diffuse and focal coronary stenosis between visual and quantitative assessment. Front. Cardiovasc. Med. 2024, 11, 1501576. [Google Scholar] [CrossRef]
- Sakai, K.; Mizukami, T.; Leipsic, J.; Belmonte, M.; Sonck, J.; Nørgaard, B.L.; Otake, H.; Ko, B.; Koo, B.K.; Maeng, M.; et al. Coronary Atherosclerosis Phenotypes in Focal and Diffuse Disease. JACC Cardiovasc. Imaging 2023, 16, 1452–1464. [Google Scholar] [CrossRef]
- Scarsini, R.; Fezzi, S.; Leone, A.M.; De Maria, G.L.; Pighi, M.; Marcoli, M.; Tavella, D.; Pesarini, G.; Banning, A.P.; Barbato, E.; et al. Functional Patterns of Coronary Disease: Diffuse, Focal, and Serial Lesions. JACC Cardiovasc. Interv. 2022, 15, 2174–2191. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Focal Significant Stenosis N = 16 | Diffuse–Long Non-Significant Stenosis N = 14 | p | |
|---|---|---|---|
| Demographics | |||
| Age (years) | 53 [45–66] | 55 [46–68] | 0.82 |
| Men, n (%) | 10 (62.5) | 9 (64.2) | 0.92 |
| BMI (Kg/m2) | 27 [25–31] | 27 [25–32] | 0.65 |
| Cardiovascular risk factors | |||
| Hypertension, n (%) | 12 (75.0) | 11 (78.5) | 0.82 |
| Current Smokers, n (%) | 4 (25.0) | 3 (21.4) | 0.81 |
| Previous Smokers, n (%) | 3 (18.7) | 3 (21.4) | 0.85 |
| Baseline lipid profile | |||
| Total cholesterol (mg/dL) | 182.3 [166.2–209.5] | 183.4 [167.6–211.8] | 0.81 |
| Triglycerides (mg/dL) | 113.8 [86.9–162.3] | 115.1 [89.3–165.1] | 0.76 |
| High-density lipoprotein (mg/dL) | 40.3 [33.1–55.7] | 42.3 [35.2–59.1] | 0.79 |
| Low-density lipoprotein (mg/dL) | 119.4 [104.3–145.6] | 118.0 [105.9–152.4] | 0.86 |
| Flow | |||
| Hear Rate (bpm) at image acquisition | 68.1 ± 7.5 | 69.2 ± 8.3 | 0.70 |
| EDV (ml) | 75.4 ± 18.2 | 74.3 ± 19.4 | 0.87 |
| ESV (ml) | 31.0 ± 7.6 | 30.2 ± 8.1 | 0.78 |
| LAD anatomical characteristics | |||
| LAD D.ref. (mm) | 3.46 ± 0.7 | 3.47 ± 0.7 | 0.83 |
| LAD stenosis diameter (%) | 84.6 ± 4.3 | 42.9 ± 4.5 | <0.001 |
| LAD stenosis length (mm) | 18.2 ± 1.1 | 38.9 ± 1.0 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rigatelli, G.; Zuin, M.; Mileva, N.; Vassilev, D.; Marchese, G.; Hiso, E.; Bertolini, A.; Bilato, C. Reduced Shear Stress and Longer Blood Flow Time Occur in Both Severe Focal and Mild Diffuse LAD Lesions: Angiograms Alone Don’t Always Reveal Their True Impact on Blood Flow. Pathophysiology 2025, 32, 28. https://doi.org/10.3390/pathophysiology32020028
Rigatelli G, Zuin M, Mileva N, Vassilev D, Marchese G, Hiso E, Bertolini A, Bilato C. Reduced Shear Stress and Longer Blood Flow Time Occur in Both Severe Focal and Mild Diffuse LAD Lesions: Angiograms Alone Don’t Always Reveal Their True Impact on Blood Flow. Pathophysiology. 2025; 32(2):28. https://doi.org/10.3390/pathophysiology32020028
Chicago/Turabian StyleRigatelli, Gianluca, Marco Zuin, Niva Mileva, Dobrin Vassilev, Giuseppe Marchese, Ervis Hiso, Andrea Bertolini, and Claudio Bilato. 2025. "Reduced Shear Stress and Longer Blood Flow Time Occur in Both Severe Focal and Mild Diffuse LAD Lesions: Angiograms Alone Don’t Always Reveal Their True Impact on Blood Flow" Pathophysiology 32, no. 2: 28. https://doi.org/10.3390/pathophysiology32020028
APA StyleRigatelli, G., Zuin, M., Mileva, N., Vassilev, D., Marchese, G., Hiso, E., Bertolini, A., & Bilato, C. (2025). Reduced Shear Stress and Longer Blood Flow Time Occur in Both Severe Focal and Mild Diffuse LAD Lesions: Angiograms Alone Don’t Always Reveal Their True Impact on Blood Flow. Pathophysiology, 32(2), 28. https://doi.org/10.3390/pathophysiology32020028