1. Introduction
In patients with sarcoidosis, the development of systemic inflammation and internal organ dysfunction are observed, which significantly reduces quality of life and worsens patient prognosis. One of the most common complications is considered to be small fiber neuropathy (SFN), a condition that remains significantly understudied [
1,
2,
3,
4]. Quite often, patients with lung sarcoidosis complain of a number of non-specific symptoms, such as weakness, sleep disorders, etc., which can significantly affect the patient’s quality of life, even in the absence of significant deviations from the pulmonary system.
The development of SFN is considered to be the result of cytokine-mediated inflammation, which is typical for various autoimmune diseases, including sarcoidosis [
5,
6,
7,
8]. Small nerve fiber damage is also observed in systemic lupus erythematosus, Sjogren’s syndrome, and fibromyalgia [
9,
10]. Considering the significant role of genetic predisposition and the possible provocative role of exogenous triggers in the development of this complication, SFN in patients with sarcoidosis can be considered as a part of the autoimmune/inflammatory syndrome that is induced by adjuvants (ASIA) [
11]. Several proven cases SFN have also been observed in patients suffering from the bacterial inflammation, e.g., Lyme disease and leprosy [
1,
2,
3,
4].
The prevalence of sarcoidosis varies throughout the world. In Japan, there is 1 case per 100,000 people, while in Scandinavian countries, the prevalence of sarcoidosis is as much as 63 cases per 100,000 people. In the Russian Federation, sarcoidosis is described to have a prevalence of 22 to 47 cases per 100,000 people, depending on the region [
12,
13,
14,
15]. The prevalence of SFN may also vary because it not only presents with neuropathic pains and paresthesias, but also with various symptoms of autonomic dysfunction, which may not be recognized as a neurologic complication [
16,
17,
18,
19,
20].
Currently, there are no generally accepted criteria for the diagnosis of SFN. The presence of a small nerve fiber dysfunction in a patient is mainly based on clinical criteria, such as a neurological examination and validated scales (the small fiber neuropathy screening list, for example) [
19,
21,
22,
23]. In addition, electroneuromyography can be performed to ensure that limited damage is induced in large nerve fibers. The “gold standard” for diagnostics is the immunofluorescence or immunohistochemistry of a skin biopsy that allows the density of the intraepidermal nerve fibers to be calculated. This technique requires special training and equipment and is time consuming [
24,
25,
26,
27,
28,
29,
30]. A preliminary clinical diagnosis of SFN in patients with sarcoidosis is important due to the low awareness of healthcare practitioners about this complication as well as to determine a quick assessment for neuropathic signs and to increase the performance of skin biopsies in diagnosing his condition.
2. Materials and Methods
A prospective comparative study was performed in 2018–2019 yy at the St. Petersburg Research Institute of Phthisiopulmonology and at the St. Petersburg City Public Health Institution “City Multi-disciplinary Hospital No. 2”. The study was approved by the independent ethics committee of the St. Petersburg Research Institute of Phthisiopulmonology (extracted from protocol No. 46.1 of 04/20/2018). All of the study participants signed an informed consent.
The study included 50 patients with lung sarcoidosis and healthy subjects (average age was 38.4 ± 7.2 y.o.). The first group consisted of patients with lung sarcoidosis (n = 25, average age 33.4 ± 8.5 y.o.) and healthy subjects (n = 25, average age 43.2 ± 11.7 y.o.). There were no statistically significant differences in gender and age in the patient groups. The inclusion criteria were age between 18 and 65 y.o. and signing the informed consent to participate in the study. The patients from group 1 were diagnosed with stage I-II sarcoidosis. The diagnosis of pulmonary sarcoidosis was performed according to the criteria of the American Thoracic Society (ATS), the European Respiratory Society (ERS), and the World Association of Sarcoidosis and Other Granulomatous Diseases (WASOG).
The exclusion criteria were systemic glucocorticoid therapy, the presence of Löfgren’s syndrome a chronic disease course (for patients with sarcoidosis), the presence of other infectious diseases (HIV, hepatitis C), a history of cancer that was treated with chemotherapy, the presence of other diseases (diabetes, hypothyroidism, renal failure, vitamin deficiency or overdose), the use of medications (metronidazole, ni-trofurantoin, linezolid, flecainide, statins) as well as a medical history of autoimmune diseases.
According to the design of the study, the patients with sarcoidosis underwent a routine examination using X-ray, morphological, bacteriological, and molecular genetic methods. A neurological examination assessing superficial and deep pain sensitivity, muscle strength, and muscle-tonic reflexes was performed. For the clinical verification of the SFN, the validated questionnaire for the detection of small fiber neuropathy was used (Small Fiber Neuropathy Screening List, SFN-SL, ([
19],). The questionnaire consists of two parts and has 21 questions (
Table S1). Questions are ranked on a scale from 0 to 4 points each and evaluate both the frequency at which symptoms develop and their intensity. A moderate likelihood of neuropathy is established when the diagnostic threshold is reached at 22 points, and a high diagnostic threshold is determined at 48 points. With scores of less than 11 (points), the sensitivity is 100%, and the specificity is 31.0%. When scores of more than 18 are achieved, then the sensitivity is 19.0%, and the specificity is 100%.
A total of 23 patients with lung sarcoidosis agreed to undergo a skin punch biopsy (10 cm proximal to the external malleolus), which was then fixed in n Zamboni solution, and the performance of the enzyme immunoassay with the primary PGP 9.5 antibodies (Abcam) and the secondary AlexaFluor goat-anti rabbit antibodies 488 (Abcam) was evaluated. The results were compared to the normal values that were obtained in the worldwide normative reference study [
23].
Statistical analysis was performed using the Statistica 8.0 software package (Statsoft, USA). The distribution of patients into groups was carried out based on the presence of a verified diagnoses of pulmonary sarcoidosis or based on the absence of verified somatic diseases (for healthy subjects).
All of the data that were collected during the study were analyzed using descriptive statistical methods. Normally distributed data are presented in the form of the “mean ± standard deviation” formula. Data that were not normally distributed are presented in the form of the “median (interquartile range 25—75 quartiles)”, where the confidence interval was also calculated. Normality testing was performed using the Shapiro–Wilk test.
All of the data were analyzed using parametric and nonparametric statistical methods and the Chi-square test, and statistical comparison methods for two (Mann–Whitney U-test) and three (Kruskal–Wallis test) groups were performed; correlations were determined using the Spearman coefficient. Differences or association rates were considered to be statistically significant at a p < 0.05.
3. Results
The average score of the SFN screening list scale (SFN-SL) in patients with sarcoidosis was 2.0 (0.0;7.0), and in healthy volunteers, it was 0 (0;0) points (
Table 1).
Statistically significant differences were found in the results of patients with sarcoidosis and in the results of healthy subjects (p < 0.0001). Thus, in the first group, a higher average SFN-SL score was observed than it was in the second group, while the results of Groups 1 and 2 exceeded those of healthy individuals.
The main clinical symptoms of SFN were pain, changes in body temperature, impaired motility of the gastrointestinal tract and urinary system, and heart palpitations (
Table 2).
In patients with sarcoidosis, the most frequent clinical symptoms included impaired cardiovascular regulation (palpitations, dizziness), pain in the chest or in the extremities, and blurred vision. It is important to note that in 76% of patients with sarcoidosis, the clinical symptoms had a severity of no more than 1 point on the SFN-SL scale and, in most cases, these symptoms did not bother patients or lead to a decrease in quality of life (
Table 3).
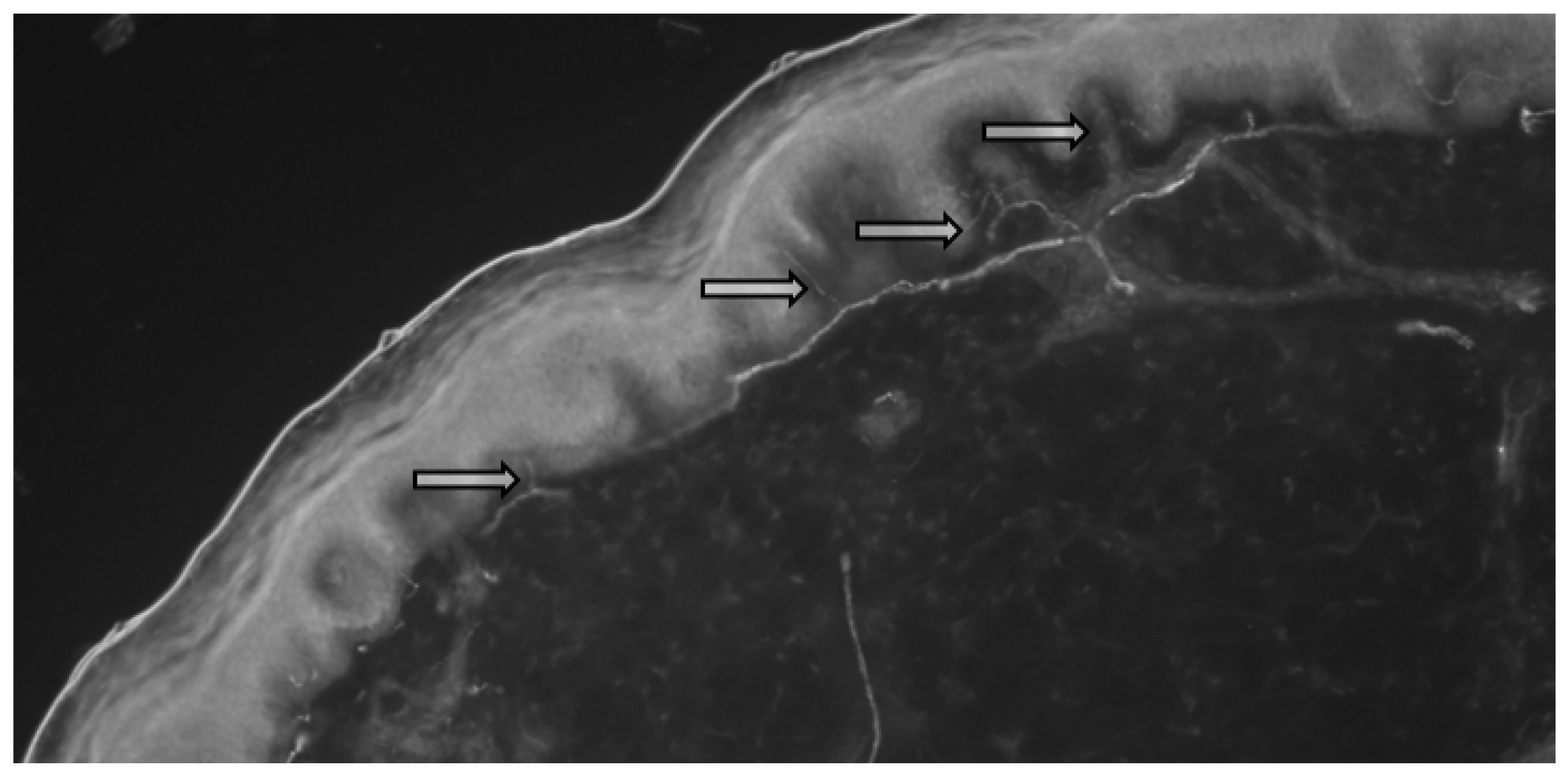
A total of 13 biopsy specimens were obtained from the patients with sarcoidosis, where the intraepidermal density (IEFD) of the small nerve fibers was calculated (
Figure 1 and
Figure 2).
A total of 13 of the biopsies were obtained from patients with sarcoidosis (
Table 4). The calculations of the intraepidermal density of the small fibers were performed in accordance with the values obtained from the worldwide normative reference study [
23].
Thus, in all of the examined patients, the number of small nerve fibers was within normal limits but below average values. A negative, statistically significant correlation was revealed between the IEND results and in the SFN-SL scores of patients with sarcoidosis (Spearman’s nonparametric rank correlation coefficient, r = −0.3508, p = 0.0102). Additionally, a negative, statistically significant correlation between the IEND and SFN-SL score was described (Spearman coefficient, r = −0.3508, p = 0.0102).
4. Discussion
In our study, complaints that are typical for the small fiber neuropathy were described in 60% of the patients with sarcoidosis. Small fiber neuropathy can manifest with a wide range of symptoms, including autonomic and sensory dysfunction. The most common clinical manifestations that were observed in our study in the patients with sarcoidosis were impaired cardiovascular regulation (36% of cases), e.g., the development of palpitations and dizziness. In 32% of cases, patients noted pain in the chest or limbs, which was often accompanied by allodynia, a subjective perception of tactile touch as pain. In some cases, this can result in sleep disturbances due to the pain sensations that are caused by bed linen touching the skin. Another symptom that is often noted by patients with sarcoidosis is blurred vision, which is described in 20% of cases. A physician needs to clarify whether these visual impairments are transient or permanent in nature in order to determine a differential diagnosis of ophthalmic pathology. In the neuropathy of small fibers, blurred vision is transient, arising while overworking or during physical exertion. Gastrointestinal tract disorders are less commonly reported with patients with sarcoidosis. In 12% of the cases, the patients complained of impaired intestinal motility, with the development of both diarrhea and constipation, which occurred simultaneously with the onset of sarcoidosis. This also includes subjective complaints of swallowing dysfunction, which is associated with both impaired muscle innervation and with the progression of mouth dryness.
While a negative, statistically significant correlation between the IEND and SFN-SL scores was described in both groups (Spearman coefficient, r = −0.3508, p = 0.0102, and r = −0.7382, p = 0.0064), a decrease in the density of the small nerve fibers in patients with pulmonary sarcoidosis was more prominent.
A major limitation of this study was that conventional nerve conduction studies and autonomic function tests were not performed. The small sample size also could also be considered as a limitation.
Thus, the neuropathy of small fibers seems to be a widespread pathology that results in the development of multiple organ dysfunction. Disorders in small fiber neuropathy, along with the typical complaints of patients with lung sarcoidosis, such as cough and shortness of breath, can significantly contribute to a decrease in the quality of life. At the same time, when focusing on the main complaints as well as on instrumental and laboratory deviations, clinicians often do not attach the necessary importance to the manifestations of SFN. It is necessary to identify the main causes that are responsible for a patient’s quality of life deteriorating in order to determine a treatment strategy and to improve the prognosis of the patient’s disease [
31,
32].
Given the low awareness of both medical specialists and patients about the development of this complication and the difficulties that are involved in its diagnosis, further study into this issue is required.
In patients with pulmonary sarcoidosis, small fiber neuropathy may develop as a result of systemic immune-mediated inflammation. The validated questionnaires and histologic verification of the diagnosis help to establish the severity of the neuropathy of small fibers to determine the prognosis and to plan the treatment strategy.
Author Contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by N.G., A.M. and V.S. Patient selection and supervision were performed by Y.Z., M.P., E.B. and D.K. General supervision was carried out by A.S. and P.Y. General research concept, guidance, and article review was performed by Y.S. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by a grant from the Government of the Russian Federation (contract No. 14W03.31.0009 dated 13 February 2017) on the allocation of the grant for the state support of scientific researchers conducted under the guidance of leading scientists.
Institutional Review Board Statement
All human studies have been approved by the independent ethics committee of the St. Petersburg Research Institute of Phthisiopulmonology (extract from protocol No. 46.1 of 20 April 2018) and have been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to their containing information that could compromise the privacy of research participants.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Abdelrazek, M.A.; Chwalisz, B.; Oaklander, A.L.; Venna, N. Evidence of small-fiber neuropathy (SFN) in two patients with unexplained genital sensory loss and sensory urinary cystopathy. J. Neurol. Sci. 2017, 380, 82–84. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, J.; Bingham, C.O. Non-length-dependent and length-dependent small-fiber neuropathies associated with tumor necrosis factor (TNF) inhibitor therapy in patients with rheumatoid arthritis: Expanding the spectrum of neurological disease associated with TNF-inhibitors. Semin. Arthr. Rheum. 2014, 43, 638–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blackmore, D.; Siddiqi, Z.A. Diagnostic Criteria for Small Fiber Neuropathy. J. Clin. Neuromuscul. Dis. 2017, 18, 125–131. [Google Scholar] [CrossRef]
- Brouwer, B.A.; Bakkers, M.; Hoeijmakers, J.G.J.; Faber, C.J.; Merkies, I.S.J. Improving assessment in small fiber neuropathy. J. Peripher. Nerv. Syst. 2015, 20, 333–340. [Google Scholar] [CrossRef]
- Bakkers, M.; Merkies, I.S.J.; Lauria, G.; Devigili, G.; Penza, P.; Lombardi, R.; Hermans, M.C.E.; van Nes, S.I.; De Baets, M.; Faber, C.G. Intraepidermal nerve fiber density and its application in sarcoidosis. Neurology 2009, 73, 1142–1148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patterson, K.C.; Chen, E.S. The pathogenesis of pulmonary sarcoidosis and implications for treatment. Chest 2018, 153, 1432–1442. [Google Scholar] [CrossRef] [PubMed]
- Bindoli, S.; Dagan, A.; Torres-Ruiz, J.J. Sarcoidosis and autoimmunity: From Genetic background to environmental factors. Isr. Med. Assoc. J. 2016, 18, 197–202. [Google Scholar]
- Starshinova, A.; Zinchenko, Y.; Filatov, M.; Denisova, N.; Istomina, E.; Landa, S.; Burdakov, V.; Churilov, L.; Sapozhnikova, N.; Pavlova, M.; et al. Specific features of immune forming complexes in patients with sarcoidosis and pulmonary tuberculosis. Immunol. Res. 2018, 7, 1–7. [Google Scholar]
- Cazzato, D.; Lauria, G. Small fiber neuropathy. Curr. Opin. Neurol. 2017, 30, 490–499. [Google Scholar] [CrossRef] [PubMed]
- Chiang, M.-C.; Tseng, M.-T.; Pan, C.-L.; Chao, C.-C.; Hsie, S.-T. Progress in the treatment of small fiber peripheral neuropathy. Expert Rev. Neurother. 2015, 15, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; Quaresma, M.; Bragazzi, N.L.; Cervera, R.; Tervaert, J.W.C.; Amital, H.; Shoenfeld, Y. The autoimmune/inflammatory syndrome induced by adjuvants (ASIA)/Shoenfeld’s syndrome: Descriptive analysis of 300 patients from the international ASIA syndrome registry. Clin. Rheumatol. 2017, 37, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Fingerlin, T.E.; Hamzeh, N.; Maier, L.A. Genetics of Sarcoidosis. Clin. Chest Med. 2015, 36, 569–584. [Google Scholar] [CrossRef]
- Newman, L.S.; Rose, C.S.; Bresnitz, E.A.; Rossman, M.D.; Barnard, J.; Frederick, M.; Terrin, M.L.; Weinberger, S.E.; Moller, D.R.; McLennan, G.; et al. A Case Control Etiologic Study of Sarcoidosis. Am. J. Respir. Crit. Care Med. 2004, 170, 1324–1330. [Google Scholar] [CrossRef] [PubMed]
- Kobak, S.; Sever, F.; Sivrikoz, O.N.; Orman, M. Sarcoidois: Is it only a mimicker of primary rheumatic disease? A single center experience. Ther. Adv. Musculoskelet. Dis. 2014, 6, 3–7. [Google Scholar] [CrossRef] [Green Version]
- Drori, T.; Givaty, G.; Chapman, J.; Lidar, M.; Langevitz, P.; Shoenfeld, Y.; Cohen, O.S. Extrapyramidal sings in neurosarcoidosis versus multiple sclerosis: Is TNF alpha the link? Immunobiology 2018, 223, 259–263. [Google Scholar] [CrossRef]
- Musaelyan, A.; Lapin, S.; Nazarov, V.; Tkachenko, O.; Gilburd, B.; Mazing, A.; Mikhailova, L.; Shoenfeld, Y. Vimentin as antigenic target in autoimmunity: A comprehensive review. Autoimmun. Rev. 2018, 17, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Dori, A.; Lopate, G.; Choksi, R.; Pestronk, A. Myelinated and unmyelinated endoneurial axon quantitation and clinical correlation. Muscle Nerve 2016, 53, 198–204. [Google Scholar] [CrossRef]
- Dori, A.; Lopate, G.; Keeling, R.; Pestronk, A. Myovascular innervation: Axon loss in small-fiber neuropathies. Muscle Nerve 2015, 51, 514–521. [Google Scholar] [CrossRef]
- Hoitsma, E.; de Vries, J.; Drent, M. The small fiber neuropathy screening list: Construction and cross-validation in sarcoidosis. Respir. Med. 2010, 105, 95–100. [Google Scholar] [CrossRef] [Green Version]
- Hovaguimian, A.; Gibbons, C.H. Diagnosis and Treatment of Pain in Small Fiber Neuropathy. Curr. Pain Headache Rep. 2011, 15, 193–200. [Google Scholar] [CrossRef] [Green Version]
- Lauria, G.; Bakkers, M.; Schmitz, C.; Lombardi, R.; Penza, P.; Devigili, G.; Smith, A.G.; Hsieh, S.-T.; Mellgren, S.I.; Umapathi, T.; et al. Intraepidermal nerve fiber density at the distal leg: A worldwide normative reference study. J. Peripher. Nerv. Syst. 2010, 15, 202–207. [Google Scholar] [CrossRef]
- Lauria, G.; Lombardi, R.; Camozzi, F.; Devigili, G. Skin biopsy for the diagnosis of peripheral neuropathy. Histopathology 2009, 54, 273–285. [Google Scholar] [CrossRef] [PubMed]
- Lauria, G.; Merkies, I.S.G.; Faber, C.G. Small fiber neuropathy. Curr. Opin. Neurol. 2012, 25, 542–549. [Google Scholar] [CrossRef]
- Levin, T.D.; Saperstein, D.S. Routine use of punch biopsy to diagnose small fiber neuropathy in fibromyalgia patient. Clin. Rheumatol. 2015, 34, 413–417. [Google Scholar] [CrossRef] [Green Version]
- McArthur, J.C. Painful Small Fiber Neuropathies. CONTINUUM Lifelong Learn. Neurol. 2012, 18, 106–125. [Google Scholar] [CrossRef]
- McCarthy, B.G.; Hsieh, S.T.; Stocks, A.; Hauer, P.; Macko, C.; Cornblath, D.R.; Griffin, J.W.; McArthur, J.C. Cutaneous innervation in sensory neuropathies: Evaluation by skin biopsy. Neurology 1995, 45, 1848–1855. [Google Scholar] [CrossRef] [PubMed]
- Oaklander, A.L. Immunotherapy Prospects for Painful Small-Fiber Sensory Neuropathies and Ganglionopathies. Neurotherapeutics 2016, 13, 108–111. [Google Scholar] [CrossRef] [Green Version]
- Peteira, M.P.; Muhl, S.; Pogatzki-Zahn, E.M.; Agelopoulos, K.; Stander, S. Intraepidermal Nerve Fiber Density: Diagnostic and Therapeutic Relevance in the Management of Chronic Pruritus: A Review. Dermatol. Ther. 2016, 6, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Provitera, V.; Gibbons, C.H.; Wendelschafer-Crabb, G.; Donadio, V.; Vitale, D.F.; Stancanelli, A.; Caporaso, G.; Liguori, R.; Wang, N.; Santoro, L.; et al. A multi-center, multinational age- and gender-adjusted normative dataset for immunofluorescent intraepidermal nerve fiber density at the distal leg. Eur. J. Neurol. 2016, 23, 333–338. [Google Scholar] [CrossRef]
- Sene, D. Small fiber neuropathy: Diagnosis, causes and treatment. Jt. Bone Spine 2018, 85, 553–559. [Google Scholar] [CrossRef] [PubMed]
- Drent, M.; Lower, E.E.; De Vries, J. Sarcoidosis-Associated Fatigue. Eur. Respir. J. 2012, 40, 255–263. [Google Scholar] [CrossRef] [Green Version]
- Saketkoo, L.A.; Russell, A.M.; Jensen, K.; Mandizha, J.; Tavee, J.; Newton, J.; Rivera, F.; Howie, M.; Reese, R.; Goodman, M.; et al. Health-Related Quality of Life (HRQoL) in Sarcoidosis: Diagnosis, Management, and Health Outcomes. Diagnostics 2021, 11, 1089. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 


{kind=link}
{kind=link}