


Interactive Compensation Effects of Physical Activity and Sleep on Mental Health: A Longitudinal Panel Study among Chinese College Students during the COVID-19 Pandemic


Abstract
1. Introduction
2. Study Design and Methods
2.1. Design
2.2. Participants
2.3. Measures
2.3.1. Physical Activity
2.3.2. Sleep Status
2.3.3. Mental Health
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics and Descriptive Analysis
3.2. Effects of Different PA Levels and Sleep Health Status on Mental Health
3.3. Relationships between Different Intensity PA and Mental Health under Varying Sleep Health Status
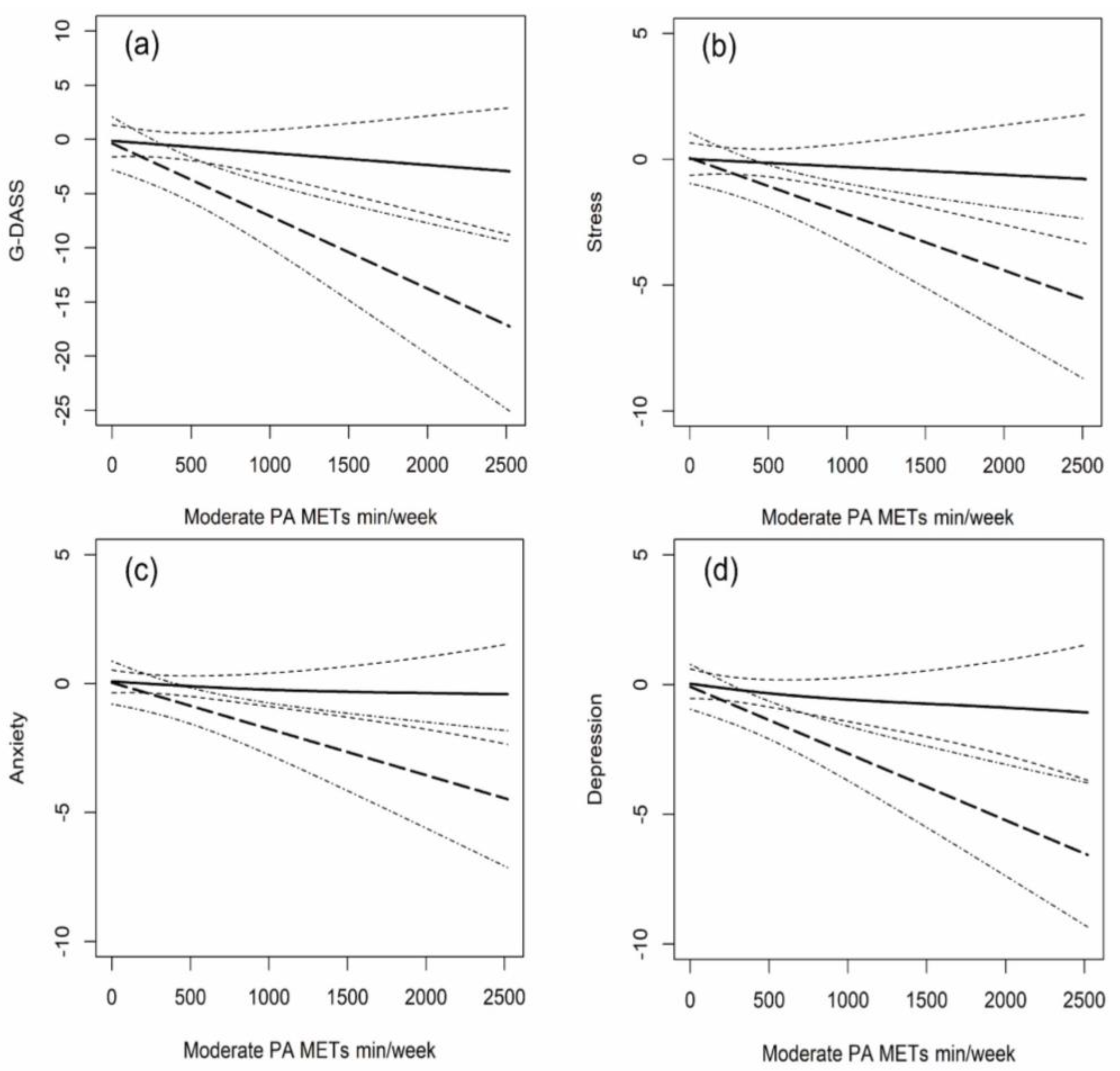
3.4. Dose-Response Relationship between Moderate Intensity PA and Mental Health under Varying Sleep Health Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kieling, C.; Baker-Henningham, H.; Belfer, M.; Conti, G.; Ertem, I.; Omigbodun, O.; Rohde, L.A.; Srinath, S.; Ulkuer, N.; Rahman, A. Child and Adolescent Mental Health Worldwide: Evidence for Action. Lancet 2011, 378, 1515–1525. [Google Scholar] [CrossRef]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and Physical Activity for Older Adults. Med. Sci. Sport. Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef] [PubMed]
- Warburton, D.E.R. Health Benefits of Physical Activity: The Evidence. Can. Med. Assoc. J. 2006, 174, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Pascoe, M.; Bailey, A.P.; Craike, M.; Carter, T.; Patten, R.; Stepto, N.; Parker, A. Physical Activity and Exercise in Youth Mental Health Promotion: A Scoping Review. BMJ Open Sport Exerc. Med. 2020, 6, e000677. [Google Scholar] [CrossRef]
- Macera, C.A.; Hootman, J.M.; Sniezek, J.E. Major Public Health Benefits of Physical Activity. Arthritis Rheum. 2003, 49, 122–128. [Google Scholar] [CrossRef]
- Bell, S.L.; Audrey, S.; Gunnell, D.; Cooper, A.; Campbell, R. The Relationship between Physical Activity, Mental Wellbeing and Symptoms of Mental Health Disorder in Adolescents: A Cohort Study. Int. J. Behav. Nutr. Phys. Act. 2019, 16, 138. [Google Scholar] [CrossRef]
- Conn, V.S. Depressive Symptom Outcomes of Physical Activity Interventions: Meta-Analysis Findings. Ann. Behav. Med. 2010, 39, 128–138. [Google Scholar] [CrossRef]
- Loprinzi, P.D. Objectively Measured Light and Moderate-to-Vigorous Physical Activity Is Associated with Lower Depression Levels among Older US Adults. Aging Ment. Health 2013, 17, 801–805. [Google Scholar] [CrossRef]
- Gothe, N.P.; Ehlers, D.K.; Salerno, E.A.; Fanning, J.; Kramer, A.F.; McAuley, E. Physical Activity, Sleep and Quality of Life in Older Adults: Influence of Physical, Mental and Social Well-Being. Behav. Sleep Med. 2020, 18, 797–808. [Google Scholar] [CrossRef]
- Chekroud, A.M.; Trugerman, A. The Opportunity for Exercise to Improve Population Mental Health. JAMA Psychiatry 2019, 76, 1206–1207. [Google Scholar] [CrossRef]
- Vaynman, S.; Ying, Z.; Gomez-Pinilla, F. Hippocampal BDNF Mediates the Efficacy of Exercise on Synaptic Plasticity and Cognition. Eur. J. Neurosci. 2004, 20, 2580–2590. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, K.; Stojanovska, L.; Polenakovic, M.; Bosevski, M.; Apostolopoulos, V. Exercise and Mental Health. Maturitas 2017, 106, 48–56. [Google Scholar] [CrossRef] [PubMed]
- De Moor, M.H.M.; Boomsma, D.I.; Stubbe, J.H.; Willemsen, G.; de Geus, E.J.C. Testing Causality in the Association Between Regular Exercise and Symptoms of Anxiety and Depression. Arch. Gen. Psychiatry 2008, 65, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Lagerberg, D. Physical Activity and Mental Health in Schoolchildren: A Complicated Relationship: Commentaries. Acta Paediatr. 2007, 94, 1699–1701. [Google Scholar] [CrossRef]
- Biddle, S.J.H.; Asare, M. Physical Activity and Mental Health in Children and Adolescents: A Review of Reviews. Br. J. Sport. Med. 2011, 45, 886–895. [Google Scholar] [CrossRef]
- Ahn, S.; Fedewa, A.L. A Meta-Analysis of the Relationship Between Children’s Physical Activity and Mental Health. J. Pediatr. Psychol. 2011, 36, 385–397. [Google Scholar] [CrossRef]
- Shokri-Kojori, E.; Wang, G.-J.; Wiers, C.E.; Demiral, S.B.; Guo, M.; Kim, S.W.; Lindgren, E.; Ramirez, V.; Zehra, A.; Freeman, C.; et al. β-Amyloid Accumulation in the Human Brain after One Night of Sleep Deprivation. Proc. Natl. Acad. Sci. USA 2018, 115, 4483–4488. [Google Scholar] [CrossRef]
- Wilson, K.T.; Bohnert, A.E.; Ambrose, A.; Davis, D.Y.; Jones, D.M.; Magee, M.J. Social, Behavioral, and Sleep Characteristics Associated with Depression Symptoms among Undergraduate Students at a Women’s College: A Cross-Sectional Depression Survey, 2012. BMC Women’s Health 2014, 14, 8. [Google Scholar] [CrossRef]
- Xie, L.; Kang, H.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep Drives Metabolite Clearance from the Adult Brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef]
- Sagaspe, P.; Sanchez-Ortuno, M.; Charles, A.; Taillard, J.; Valtat, C.; Bioulac, B.; Philip, P. Effects of Sleep Deprivation on Color-Word, Emotional, and Specific Stroop Interference and on Self-Reported Anxiety. Brain Cogn. 2006, 60, 76–87. [Google Scholar] [CrossRef]
- Dai, H.; Mei, Z.; An, A.; Lu, Y.; Wu, J. Associations of Sleep Problems with Health-Risk Behaviors and Psychological Well-Being among Canadian Adults. Sleep Health 2020, 6, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Dolezal, B.A.; Neufeld, E.V.; Boland, D.M.; Martin, J.L.; Cooper, C.B. Interrelationship between Sleep and Exercise: A Systematic Review. Adv. Prev. Med. 2017, 2017, 1364387. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Haegele, J.A.; Liu, H.; Yu, F. Academic Stress, Physical Activity, Sleep, and Mental Health among Chinese Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 7257. [Google Scholar] [CrossRef] [PubMed]
- D’Aurea, C.V.R.; Poyares, D.; Passos, G.S.; Santana, M.G.; Youngstedt, S.D.; Souza, A.A.; Bicudo, J.; Tufik, S.; de Mello, M.T. Effects of Resistance Exercise Training and Stretching on Chronic Insomnia. Braz. J. Psychiatry 2019, 41, 51–57. [Google Scholar] [CrossRef]
- Duncan, M.J.; Rayward, A.T.; Holliday, E.G.; Brown, W.J.; Vandelanotte, C.; Murawski, B.; Plotnikoff, R.C. Effect of a Physical Activity and Sleep M-Health Intervention on a Composite Activity-Sleep Behaviour Score and Mental Health: A Mediation Analysis of Two Randomised Controlled Trials. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 45. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhang, H.; Ma, X.; Di, Q. Mental Health Problems during the COVID-19 Pandemics and the Mitigation Effects of Exercise: A Longitudinal Study of College Students in China. Int. J. Environ. Res. Public Health 2020, 17, 3722. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef]
- Macfarlane, D.J.; Lee, C.C.Y.; Ho, E.Y.K.; Chan, K.L.; Chan, D.T.S. Reliability and Validity of the Chinese Version of IPAQ (Short, Last 7 Days). J. Sci. Med. Sport 2007, 10, 45–51. [Google Scholar] [CrossRef]
- Ainsworth, B.E.; Haskell, W.L.; Whitt, M.C.; Irwin, M.L.; Swartz, A.M.; Strath, S.J.; O’Brien, W.L.; Bassett, D.R.; Schmitz, K.H.; Emplaincourt, P.O.; et al. Compendium of Physical Activities: An Update of Activity Codes and MET Intensities. Med. Sci. Sport. Exerc. 2000, 32, S498–S516. [Google Scholar] [CrossRef]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A New Instrument for Psychiatric Practice and Research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Tsai, P.-S.; Wang, S.-Y.; Wang, M.-Y.; Su, C.-T.; Yang, T.-T.; Huang, C.-J.; Fang, S.-C. Psychometric Evaluation of the Chinese Version of the Pittsburgh Sleep Quality Index (CPSQI) in Primary Insomnia and Control Subjects. Qual. Life Res. 2005, 14, 1943–1952. [Google Scholar] [CrossRef] [PubMed]
- Hinz, A.; Glaesmer, H.; Brähler, E.; Löffler, M.; Engel, C.; Enzenbach, C.; Hegerl, U.; Sander, C. Sleep Quality in the General Population: Psychometric Properties of the Pittsburgh Sleep Quality Index, Derived from a German Community Sample of 9284 People. Sleep Med. 2017, 30, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Carney, C.E.; Edinger, J.D.; Meyer, B.; Lindman, L.; Istre, T. Daily Activities and Sleep Quality in College Students. Chronobiol. Int. 2006, 23, 623–637. [Google Scholar] [CrossRef] [PubMed]
- Lovibond, P.F.; Lovibond, S.H. The Structure of Negative Emotional States: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Zanon, C.; Brenner, R.E.; Baptista, M.N.; Vogel, D.L.; Rubin, M.; Al-Darmaki, F.R.; Gonçalves, M.; Heath, P.J.; Liao, H.-Y.; Mackenzie, C.S.; et al. Examining the Dimensionality, Reliability, and Invariance of the Depression, Anxiety, and Stress Scale–21 (DASS-21) across Eight Countries. Assessment 2021, 28, 1531–1544. [Google Scholar] [CrossRef]
- Quek, T.; Ho, C.; Choo, C.; Nguyen, L.; Tran, B.; Ho, R. Misophonia in Singaporean Psychiatric Patients: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2018, 15, 1410. [Google Scholar] [CrossRef]
- Le, T.A.; Le, M.Q.T.; Dang, A.D.; Dang, A.K.; Nguyen, C.T.; Pham, H.Q.; Vu, G.T.; Hoang, C.L.; Tran, T.T.; Vuong, Q.-H.; et al. Multi-Level Predictors of Psychological Problems among Methadone Maintenance Treatment Patients in Difference Types of Settings in Vietnam. Subst. Abus. Treat. Prev. Policy 2019, 14, 39. [Google Scholar] [CrossRef]
- Verbeke, G.; Fieuws, S. The Effect of Miss-Specified Baseline Characteristics on Inference for Longitudinal Trends in Linear Mixed Models. Biostatistics 2006, 8, 772–783. [Google Scholar] [CrossRef][Green Version]
- Vicendese, D.; Olenko, A.; Dharmage, S.; Tang, M.; Abramson, M.; Erbas, B. Modelling and Predicting Low Count Child Asthma Hospital Readmissions Using General Additive Models. Open J. Epidemiol. 2013, 3, 125–134. [Google Scholar] [CrossRef][Green Version]
- Wood, S.N. Stable and Efficient Multiple Smoothing Parameter Estimation for Generalized Additive Models. J. Am. Stat. Assoc. 2004, 99, 673–686. [Google Scholar] [CrossRef]
- Feng, Q.; Zhang, Q.; Du, Y.; Ye, Y.; He, Q. Associations of Physical Activity, Screen Time with Depression, Anxiety and Sleep Quality among Chinese College Freshmen. PLoS ONE 2014, 9, e100914. [Google Scholar] [CrossRef] [PubMed]
- Ghrouz, A.K.; Noohu, M.M.; Dilshad Manzar, M.; Warren Spence, D.; BaHammam, A.S.; Pandi-Perumal, S.R. Physical Activity and Sleep Quality in Relation to Mental Health among College Students. Sleep Breath 2019, 23, 627–634. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, B.C.; Monteiro, S.; Candida, M.; Adler, N.; Paes, F.; Rocha, N.; Nardi, A.E.; Murillo-Rodriguez, E.; Machado, S. Relationship Between Brain-Derived Neurotrofic Factor (Bdnf) and Sleep on Depression: A Critical Review. Clin. Pract. Epidemiol. Ment. Health 2017, 13, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Patki, G.; Solanki, N.; Atrooz, F.; Allam, F.; Salim, S. Depression, Anxiety-like Behavior and Memory Impairment Are Associated with Increased Oxidative Stress and Inflammation in a Rat Model of Social Stress. Brain Res. 2013, 1539, 73–86. [Google Scholar] [CrossRef]
- Vollert, C.; Zagaar, M.; Hovatta, I.; Taneja, M.; Vu, A.; Dao, A.; Levine, A.; Alkadhi, K.; Salim, S. Exercise Prevents Sleep Deprivation-Associated Anxiety-like Behavior in Rats: Potential Role of Oxidative Stress Mechanisms. Behav. Brain Res. 2011, 224, 233–240. [Google Scholar] [CrossRef]
- Elosua, R.; Molina, L.; Fito, M.; Arquer, A.; Sanchez-Quesada, J.L.; Covas, M.I.; Ordoñez-Llanos, J.; Marrugat, J. Response of Oxidative Stress Biomarkers to a 16-Week Aerobic Physical Activity Program, and to Acute Physical Activity, in Healthy Young Men and Women. Atherosclerosis 2003, 167, 327–334. [Google Scholar] [CrossRef]
- Kozakiewicz, M.; Rowiński, R.; Kornatowski, M.; Dąbrowski, A.; Kędziora-Kornatowska, K.; Strachecka, A. Relation of Moderate Physical Activity to Blood Markers of Oxidative Stress and Antioxidant Defense in the Elderly. Oxidative Med. Cell. Longev. 2019, 2019, 5123628. [Google Scholar] [CrossRef]
- Bartfay, W.; Bartfay, E. A Case–Control Study Examining the Effects of Active Versus Sedentary Lifestyles on Measures of Body Iron Burden and Oxidative Stress in Postmenopausal Women. Biol. Res. Nurs. 2014, 16, 38–45. [Google Scholar] [CrossRef]
- Asztalos, M.; De Bourdeaudhuij, I.; Cardon, G. The Relationship between Physical Activity and Mental Health Varies across Activity Intensity Levels and Dimensions of Mental Health among Women and Men. Public Health Nutr. 2010, 13, 1207–1214. [Google Scholar] [CrossRef]
- Sylvester, B.D.; Ahmed, R.; Amireault, S.; Sabiston, C.M. Changes in Light-, Moderate-, and Vigorous-Intensity Physical Activity and Changes in Depressive Symptoms in Breast Cancer Survivors: A Prospective Observational Study. Support Care Cancer 2017, 25, 3305–3312. [Google Scholar] [CrossRef]
- Van Berkel, J.; Proper, K.I.; van Dam, A.; Boot, C.R.; Bongers, P.M.; van der Beek, A.J. An Exploratory Study of Associations of Physical Activity with Mental Health and Work Engagement. BMC Public Health 2013, 13, 558. [Google Scholar] [CrossRef] [PubMed]
- Gerber, M.; Brand, S.; Herrmann, C.; Colledge, F.; Holsboer-Trachsler, E.; Pühse, U. Increased Objectively Assessed Vigorous-Intensity Exercise Is Associated with Reduced Stress, Increased Mental Health and Good Objective and Subjective Sleep in Young Adults. Physiol. Behav. 2014, 135, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Sink, K.M.; Espeland, M.A.; Castro, C.M.; Church, T.; Cohen, R.; Dodson, J.A.; Guralnik, J.; Hendrie, H.C.; Jennings, J.; Katula, J.; et al. Effect of a 24-Month Physical Activity Intervention vs. Health Education on Cognitive Outcomes in Sedentary Older Adults: The LIFE Randomized Trial. JAMA 2015, 314, 781–790. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variables | 1st | 2nd | 3rd | 4th | p |
|---|---|---|---|---|---|
| N = 59 | N = 66 | N = 66 | N = 66 | ||
| Categorical variables, | |||||
| N (%) | |||||
| Gender | |||||
| Males | 18 (30.51) | 25 (37.88) | 25 (37.88) | 25 (37.88) | 0.78 |
| Females | 41 (69.49) | 41 (62.12) | 41 (62.12) | 41 (62.12) | |
| Race | |||||
| Han | 55 (93.22) | 61 (92.42) | 61 (92.42) | 61 (92.42) | 0.98 |
| Minority | 4 (6.78) | 5 (7.58) | 5 (7.58) | 5 (7.58) | |
| Residence | |||||
| City | 44 (74.58) | 51 (77.27) | 51 (77.27) | 51 (77.27) | 0.98 |
| Countryside | 15 (25.42) | 15 (22.73) | 15 (22.73) | 15 (22.73) | |
| PA level | |||||
| Inactive | 15 (25.42) | 10 (15.15) | 7 (10.61) | 3 (4.55) | 0.16 |
| Low | 14 (23.73) | 19 (28.79) | 22 (33.33) | 21 (31.82) | |
| Moderate | 23 (38.98) | 29 (43.94) | 27 (40.91) | 31 (46.97) | |
| High | 7 (11.87) | 8 (12.12) | 10 (15.15) | 11 (16.66) | |
| Sleep status | |||||
| Healthy | 50 (84.75) | 38 (57.58) | 34 (51.52) | 54 (81.82) | <0.001 |
| Unhealthy | 9 (15.25) | 28 (42.42) | 32 (48.48) | 12 (18.18) | |
| Continuous variables, | |||||
| Mean ± SD | |||||
| Age | 20.46 ± 2.07 | 20.70 ± 2.10 | 20.70 ± 2.10 | 20.70 ± 2.10 | 0.56 |
| BMI | 21.0 ± 3.02 | 21.1 ± 2.92 | 21.1 ± 2.92 | 21.1 ± 2.92 | 0.81 |
| Light PA | 426.99 ± 553.11 | 327.50 ± 312.91 | 436.80 ± 516.49 | 505.25 ± 441.33 | 0.17 |
| Moderate PA | 360.34 ± 541.42 | 250.30 ± 374.19 | 383.94 ± 498.25 | 418.00 ± 538.27 | 0.24 |
| Vigorous PA | 280.68 ± 760.49 | 354.55 ± 613.40 | 294.55 ± 545.96 | 384.61 ± 849.67 | 0.53 |
| PSQI | 4.07 ± 2.00 | 5.74 ± 2.59 | 6.08 ± 1.99 | 3.76 ± 2.36 | 0.51 |
| Stress | 11.93 ± 3.08 | 12.32 ± 3.61 | 11.85 ± 3.86 | 11.74 ± 4.28 | 0.60 |
| Anxiety | 10.37 ± 2.71 | 10.41 ± 2.77 | 10.20 ± 2.81 | 10.09 ± 2.86 | 0.49 |
| Depression | 10.54 ± 3.19 | 10.59 ± 3.16 | 10.65 ± 3.12 | 10.83 ± 3.53 | 0.61 |
| Global DASS | 32.85 ± 7.82 | 33.42 ± 8.74 | 32.70 ± 9.04 | 32.67 ± 9.94 | 0.79 |
| Healthy Sleep Status | Unhealthy Sleep Status | |||
|---|---|---|---|---|
| Β | p | β | p | |
| G-DASS | ||||
| 100 × Light PA (METs-min/week) | 0.055 | 0.619 | −0.002 | 0.993 |
| 100 × Moderate PA (METs-min/week) | −0.153 | 0.185 | −0.470 | 0.011 * |
| 100 × Vigorous PA (METs-min/week) | −0.162 | 0.077 | −0.134 | 0.299 |
| Stress | ||||
| 100 × Light PA (METs-min/week) | 0.038 | 0.433 | 0.013 | 0.883 |
| 100 × Moderate PA (METs-min/week) | −0.070 | 0.166 | −0.184 | 0.021 * |
| 100 × Vigorous PA (METs-min/week) | −0.067 | 0.095 | −0.062 | 0.248 |
| Anxiety | ||||
| 100 × Light PA (METs-min/week) | 0.0001 | 0.998 | 0.032 | 0.654 |
| 100 × Moderate PA (METs-min/week) | −0.033 | 0.343 | −0.136 | 0.033 * |
| 100 × Vigorous PA (METs-min/week) | −0.039 | 0.165 | −0.057 | 0.194 |
| Depression | ||||
| 100 × Light PA (METs-min/week) | 0.010 | 0.814 | −0.05 | 0.462 |
| 100 × Moderate PA (METs-min/week) | −0.049 | 0.276 | −0.156 | 0.012 * |
| 100 × Vigorous PA (METs-min/week) | −0.053 | 0.137 | −0.019 | 0.683 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Liu, J.; Zhang, Y.; Ke, L.; Liu, R. Interactive Compensation Effects of Physical Activity and Sleep on Mental Health: A Longitudinal Panel Study among Chinese College Students during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 12323. https://doi.org/10.3390/ijerph191912323
Zhang Y, Liu J, Zhang Y, Ke L, Liu R. Interactive Compensation Effects of Physical Activity and Sleep on Mental Health: A Longitudinal Panel Study among Chinese College Students during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(19):12323. https://doi.org/10.3390/ijerph191912323
Chicago/Turabian StyleZhang, Yao, Jianxiu Liu, Yi Zhang, Limei Ke, and Ruidong Liu. 2022. "Interactive Compensation Effects of Physical Activity and Sleep on Mental Health: A Longitudinal Panel Study among Chinese College Students during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 19: 12323. https://doi.org/10.3390/ijerph191912323
APA StyleZhang, Y., Liu, J., Zhang, Y., Ke, L., & Liu, R. (2022). Interactive Compensation Effects of Physical Activity and Sleep on Mental Health: A Longitudinal Panel Study among Chinese College Students during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(19), 12323. https://doi.org/10.3390/ijerph191912323