
CARDIOSIM©: The First Italian Software Platform for Simulation of the Cardiovascular System and Mechanical Circulatory and Ventilatory Support

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
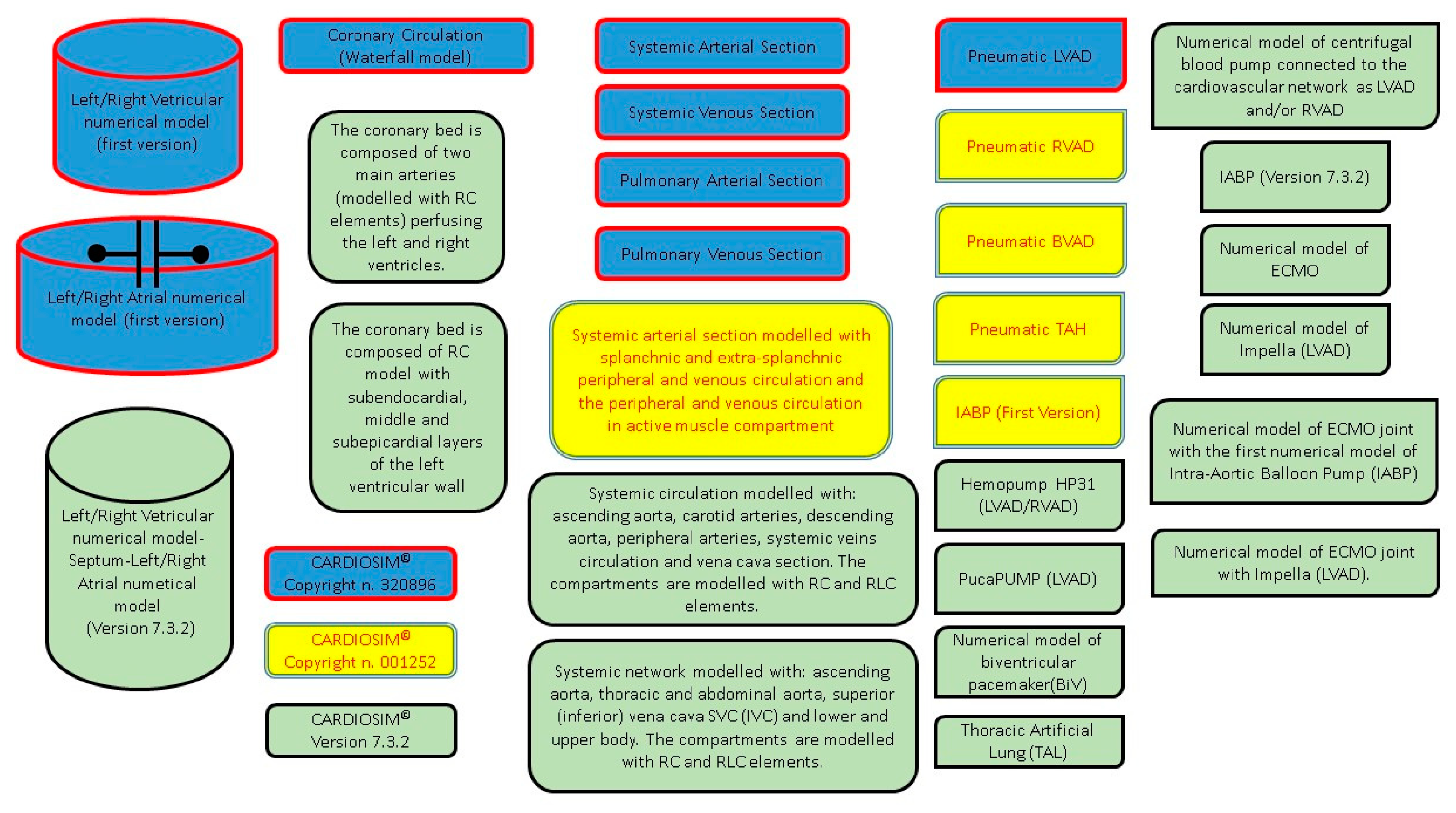
2.1. Historical Overview
2.2. Numerical Models of Ventricles, Atria and Septum
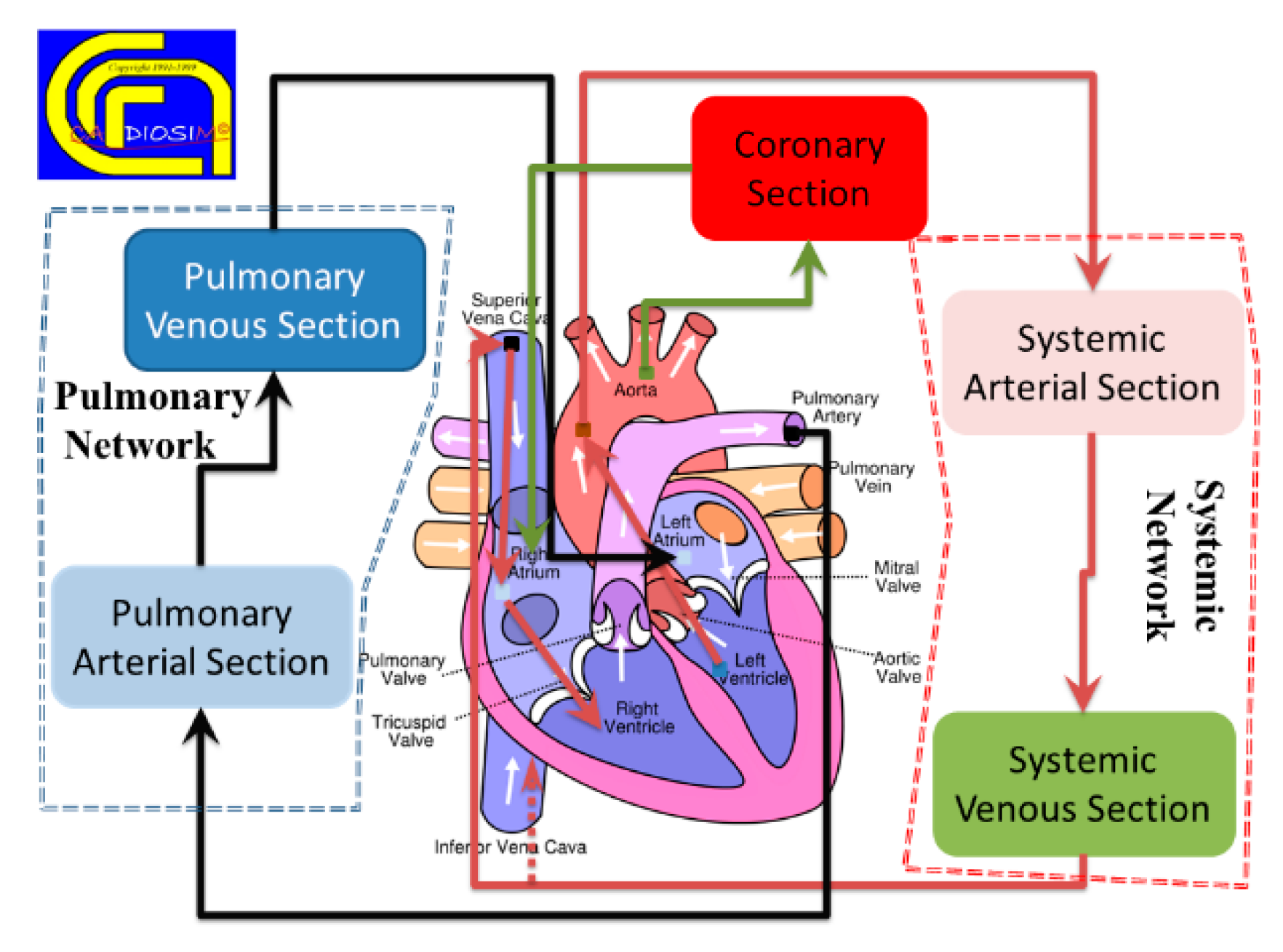
2.3. Numerical Model of Systemic and Pulmonary Circulation
2.4. Numerical Model of the Coronary Circulation
2.5. Mechanical Ventilatory Assistance

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Version | Second Version | Version 7.3.2 |
|---|---|---|
| Systemic arterial section modeled with modified Windkessel (RLC) or three-cell model [10,40]. | Systemic arterial section modeled with modified Windkessel (RLC) or three-ell model. (R is a resistance, L is an inertance and C is a compliance) | Systemic arterial section modeled with modified Windkessel (RLC) or three-cell model. |
| Systemic venous section modeled with RC elements. | Systemic venous section modeled with RC elements. | Systemic venous section modeled with RC elements. |
| -------- | Systemic arterial module reproducing the behavior of both splanchnic and extra-splanchnic bed (both with 2-WM elements) and peripheral/venous circulation in active muscle compartment (using 2-WM elements). | Systemic arterial module reproducing the behavior of both splanchnic and extra-splanchnic bed (both with 2-WM elements) and peripheral/venous circulation in active muscle compartment (using 2-WM elements). |
| --------- | --------- | Systemic circulation modeled with: ascending aorta, carotid arteries, descending aorta, peripheral arteries, systemic veins circulation and vena cava section. The compartments are modeled with RC and RLC elements. |
| --------- | --------- | Systemic network modeled with: ascending, thoracic and abdominal aorta; superior (inferior) vena cava SVC (IVC); and lower and upper body [51]. The compartments are modeled with RC and RLC elements. |
| First Version | Second Version | Version 7.3.2 |
|---|---|---|
| Waterfall model [6,7]. | Waterfall model. | Waterfall model. |
| -------- | RC model. The two resistances in series mimic the arteriolar, capillary and venous resistance. The capacitance mimics the large intramyocardial compliance. | RC model. The wo resistances in series mimic the arteriolar, capillary and venous resistance. The capacitance mimics the large intramyocardial compliance. |
| -------- | -------- | The coronary bed is composed of two main arteries (modeled with RC elements) perfusing the left and right ventricles. |
| -------- | -------- | RC model with subendocardial, middle and subepicardial layers of the left ventricular wall [52]. |
2.6. Mechanical Circulatory Assist Devices
- Central veno-arterial ECMO (VARA-DA-ECMO): ECMO draws blood from the right atrium (RA) and ejects it into the descending aorta (DA).
- Veno-venous ECMO (VVIVC-SVC-ECMO): ECMO draws blood from the inferior vena cava (IVC) and ejects it into the superior vena cava (SVC).
- Veno-arterial ECMO (VAFV-TA-ECMO): ECMO draws blood from the femoral vein (FV) and ejects it into the thoracic aorta (TA).
2.7. Clinical Application of CARDIOSIM©
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lumens, J.; Leenders, G.E.; Cramer, M.J.; De Boeck, B.W.; Doevendans, P.A.; Prinzen, F.W.; Delhaas, T. Mechanistic evaluation of echocardiographic dyssynchrony indices: Patient data combined with multiscale computer simulations. Circ. Cardiovasc. Imaging 2012, 5, 491–499. [Google Scholar] [CrossRef]
- Pedrizzetti, G.; Domenichini, F. Left Ventricular Fluid Mechanics: The Long Way from Theoretical Models to Clinical Applications. Ann. Biomed. Eng. 2015, 43, 26–40. [Google Scholar] [CrossRef] [PubMed]
- Bluestein, D. Utilizing Computational Fluid Dynamics in Cardiovascular Engineering and Medicine—What You Need to Know. Its Translation to the Clinic/Bedside. Artif. Organs 2017, 41, 117–121. [Google Scholar] [CrossRef]
- Morris, P.D.; Narracott, A.; von Tengg-Kobligk, H.; Silva Soto, D.A.; Hsiao, S.; Lungu, A.; Evans, P.; Bressloff, N.W.; Lawford, P.V.; Hose, D.R.; et al. Computational fluid dynamics modelling in cardiovascular medicine. Heart 2016, 102, 18–28. [Google Scholar] [CrossRef]
- Doshi, D.; Burkhoff, D. Cardiovascular Simulation of Heart Failure. Pathophysiology and Therapeutics. J. Card. Fail. 2016, 22, 303–311. [Google Scholar] [CrossRef]
- Duanmu, Z.; Yin, M.; Fan, X.; Yang, X.; Luo, X. A patient-specific lumped-parameter model of coronary circulation. Sci Rep. 2018, 8, 874. [Google Scholar] [CrossRef]
- Ferrari, G.; Di Molfetta, A.; Zieliński, K.; Fresiello, L. Circulatory modelling as a clinical decision support and an educational tool. Biomed. Data J. 2015, 1, 45–50. [Google Scholar] [CrossRef][Green Version]
- De Lazzari, C.; Genuini, I.; Pisanelli, D.M.; D’Ambrosi, A.; Fedele, F. Interactive simulator for e-Learning environments: A teaching software for health care professionals. BioMed. Eng. OnLine 2014, 13, 172. [Google Scholar] [CrossRef]
- De Lazzari, C.; Pirckhalava, M. (Eds.) Cardiovascular and Pulmonary Artificial Organs: Educational Training Simulators; Consiglio Nazionale delle Ricerche (CNR) Press: Rome, Italy, 2017. [Google Scholar]
- Ferrari, G.; De Lazzari, C.; Mimmo, R.; Tosti, G.; Ambrosi, D. A modular numerical model of the cardiovascular system for studying and training in the field of cardiovascular physiopathology. J. Biomed. Eng. 1992, 14, 91–107. [Google Scholar] [CrossRef]
- De Lazzari, C.; Darowski, M.; Wolski, P.; Ferrari, G.; Tosti, G. In vivo and simulation study of artificial ventilation effects on energetic variables in cardiosurgical patients. Methods Inf. Med. 2005, 44, 98–105. [Google Scholar] [PubMed]
- De Lazzari, C.; Quatember, B. Cardiac energetics in presence of lung assist devices: In silico study. Model. Num. Sim. Mater. Sci. 2016, 6, 41–57. [Google Scholar]
- De Lazzari, C. Interaction between the septum and the left (right) ventricular free wall in order to evaluate the effects on coronary blood flow: Numerical simulation. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 1359–1368. [Google Scholar] [CrossRef] [PubMed]
- Kozarski, M.; Ferrari, G.; Zieliński, K.; Górczyńska, K.; Palko, K.J.; Tokarz, A.; Darowski, M. Open loop hybrid circulatory model: The effect of the arterial lumped parameter loading structure on selected ventricular and circulatory variables. Biocybernet. Biomed. Eng. 2008, 28, 17–27. [Google Scholar]
- Fresiello, L.; Ferrari, G.; Di Molfetta, A.; Zieliński, K.; Tzallas, A.; Jacobs, S.; Darowski, M.; Kozarski, M.; Meyns, B.; Katertsidis, N.S.; et al. A cardiovascular simulator tailored for training and clinical uses. J. Biomed. Inf. 2015, 57, 100–112. [Google Scholar] [CrossRef] [PubMed]
- Capoccia, M.; Marconi, S.; De Lazzari, C. Decision-making in advanced heart failure patients requiring LVAD insertion: Can preoperative simulation become the way forward? A case study. J. Biomed. Eng. Inf. 2018, 4, 8. [Google Scholar]
- Capoccia, M.; Marconi, S.; Singh, S.A.; Pisanelli, D.M.; De Lazzari, C. Simulation as a Preoperative Planning Approach in Advanced Heart Failure Patients. A Retrospective Clinical Analysis. BioMed. Eng. OnLine 2018, 17, 52. [Google Scholar] [CrossRef] [PubMed]
- Suga, H.; Sagawa, K. Mathematical interrelationship between instantaneous ventricular pressure–volume ratio and myocardial force–velocity relation. Ann. Biomed. Eng. 1972, 1, 160–181. [Google Scholar] [CrossRef] [PubMed]
- Suga, H.; Sagawa, K.; Shoukas, A.A. Load independence of the instantaneous pressure–volume ratio of the canine left ventricle and effects of epinephrine and heart rate on the ratio. Circ. Res. 1973, 32, 314–322. [Google Scholar] [CrossRef]
- Suga, H.; Sagawa, K. Instantaneous pressure–volume relationships and their ratio in the excised, supported canine left ventricle. Circ. Res. 1974, 35, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Claessens, T.E.; Georgakopoulos, D.; Afanasyeva, M.; Vermeersch, S.J.; Millar, H.D.; Stergiopulos, N.; Westerhof, N.; Verdonck, P.R.; Segers, P. Nonlinear isochrones in murine left ventricular pressure–volume loops: How well does the time-varying elastance concept hold? Am. J. Physiol. Heart Circ. Physiol. 2006, 290, H1474–H1483. [Google Scholar] [CrossRef]
- Vandenberghe, S.; Segers, P.; Steendijk, P.; Meyns, B.; Dion, R.A.E.; Antaki, J.F.; Verdonck, P. Modelling ventricular function during cardiac assist: Does time-varying elastance work? ASAIO J. 2006, 52, 4–8. [Google Scholar] [CrossRef] [PubMed]
- Stergiopulos, N.; Meister, J.J.; Westerhof, N. Determinants of stroke volume and systolic and diastolic aortic pressure. Am. J. Physiol. Heart Circ. Physiol. 1996, 270, H2050–H2059. [Google Scholar] [CrossRef] [PubMed]
- Segers, P.; Stergiopulos, N.; Westerhof, N. Quantification of the contribution of cardiac and arterial remodelling to hypertension. Hypertension 2000, 36, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Segers, P.; Steendijk, P.; Stergiopulos, N.; Westerhof, N. Predicting systolic and diastolic aortic pressure and stroke volume in the intact sheep. J. Biomech. 2001, 34, 41–50. [Google Scholar] [CrossRef]
- Lankhaar, J.W.; Rövekamp, F.A.; Steendijk, P.; Faes, T.J.C.; Westerhof, B.E.; Kind, T.; Vonk-Noordegraaf, A.; Westerhof, N. Modelling the instantaneous pressure–volume relation of the left ventricle: A comparison of six models. Ann. Biomed. Eng. 2009, 37, 1710–1726. [Google Scholar] [CrossRef] [PubMed]
- Pironet, A.; Desaive, T.; Kosta, S.; Lucas, A.; Paeme, S.; Collet, A.; Pretty, C.G.; Kolh, P.; Dauby, P.C. A multi-scale cardiovascular system model can account for the load-dependence of the end-systolic pressure–volume relationship. Biomed. Eng. OnLine 2013, 12, 8. [Google Scholar] [CrossRef] [PubMed]
- Negroni, J.A.; Lascano, E.C. Concentration and elongation of attached cross-bridges as pressure determinants in a ventricular model. J. Mol. Cell. Cardiol. 1999, 31, 1509–1526. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Chase, J.G.; Nokes, R.I.; Shaw, G.M.; David, T. Velocity profile method for time varying resistance in minimal cardiovascular system models. Phys. Med. Biol. 2003, 48, 3375–3387. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.W.; Chase, J.G.; Nokes, R.I.; Shaw, G.M.; Wake, G. Minimal haemodynamic system model including ventricular interaction and valve dynamics. Med. Eng. Phys. 2004, 26, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Ramachandran, D.; Ware, D.L.; Ma, T.S.; Clark, J.W. Modelling left ventricular diastolic dysfunction: Classification and key indicators. Theor. Biol. Med. Model. 2011, 8, 14. [Google Scholar] [CrossRef] [PubMed]
- Luo, C.; Ware, D.L.; Zwischenberger, J.B.; Clark, J.W. A mechanical model of the human heart relating septal function to myocardial work and energy. Cardiovasc. Eng. 2008, 8, 174–184. [Google Scholar] [CrossRef] [PubMed]
- Olansen, J.B.; Clark, J.W.; Khoury, D.; Ghorbel, F.; Bidani, A. A closed-loop model of the canine cardiovascular system that includes ventricular interaction. Comput. Biomed. Res. 2000, 33, 260–295. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Chung, D.C.; Niranjan, S.C.; Clark, J.W., Jr.; Bidani, A.; Johnston, W.E.; Zwischenberger, J.B.; Traber, D.L. A dynamic model of ventricular interaction and pericardial influence. Am. J. Physiol. Heart Circ. Physiol. 1997, 272, H2942–H2962. [Google Scholar] [CrossRef] [PubMed]
- Ursino, M. Interaction between carotid baroregulation and the pulsating heart: A mathematical model. Am. J. Physiol. Heart Circ. Physiol. 1998, 275, H1733–H1747. [Google Scholar] [CrossRef]
- Wang, Y.; Loghmanpour, N.; Vandenberghe, S.; Ferreira, A.; Keller, B.; Gorcsan, J.; Antaki, J. Simulation of dilated heart failure with continuous flow circulatory support. PLoS ONE 2014, 9, e85234. [Google Scholar] [CrossRef]
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Available online: https://brevetti.cnr.it/reports/InfoTrovatoEn.jsp?nsrif=840&dip=4 (accessed on 29 May 2022).
- Il Paziente “Virtuale” per la Formazione in Cardiologia. “Sapienza” University of Rome. Available online: https://www.uniroma1.it/it/node/35113 (accessed on 29 May 2022).
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Original Website Platform Regarding the Implementation of the Cardiovascular Software Simulator CARDIOSIM©. Available online: https://cardiosim.dsb.cnr.it/ (accessed on 29 May 2022).
- De Lazzari, C.; Ferrari, G.; Mimmo, R.; Tosti, G.; Ambrosi, D. A desktop computer model of the circulatory system for heart assistance simulation: Effect of an LVAD on energetic relationships inside the left ventricle. Med. Eng. Phys. 1994, 16, 97–103. [Google Scholar] [CrossRef]
- Sagawa, K.; Maughan, L.; Suga, H.; Sunagawa, K. Cardiac Contraction and the Pressure-Volume Relationships; Oxford University Press: New York, NY, USA, 1988. [Google Scholar]
- Maughan, W.L.; Sunagawa, K.; Sagawa, K. Ventricular systolic interdependence: Volume elastance model in isolated canine hearts. Am. J. Physiol. Heart Circ. Physiol. 1987, 253, H1381–H1390. [Google Scholar] [CrossRef]
- De Lazzari, C.; D’Ambrosi, A.; Tufano, F.; Fresiello, L.; Garante, M.; Sergiacomi, R.; Stagnitti, F.; Caldarera, C.M.; Alessandri, N. Cardiac Resynchronization Therapy: Could a numerical simulator be a useful tool in order to predict the response of the biventricular pacemaker synchronization? Eur. Rev. Med. Pharm. Sci. 2010, 14, 969–978. [Google Scholar]
- Shi, Y.; Lawford, P.; Hose, R. Review of 0-D and 1-D Models of Blood Flow in the Cardiovascular System. BioMed. Eng. OnLine 2011, 10, 33. [Google Scholar] [CrossRef]
- Liu, H.; Liu, S.; Ma, X.; Zhang, Y. A numerical model applied to the simulation of cardiovascular hemodynamics and operating condition of continuous-flow left ventricular assist device. Math. Biosci. Eng. 2020, 17, 7519–7543. [Google Scholar] [CrossRef]
- Bozkurt, S.; Safak, K.K. Evaluating the Hemodynamical Response of a Cardiovascular System under Support of a Continuous Flow Left Ventricular Assist Device via Numerical Modeling and Simulations. Comput. Math. Methods. Med. 2013, 2013, 986430. [Google Scholar] [CrossRef] [PubMed]
- Sorguven, E.; Bozkurt, S.; Baldock, C. Computer simulations can replace in-vivo experiments for implantable medical devices. Phys. Eng. Sci. Med. 2021, 44, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bozkurt, S. Mathematical modeling of cardiac function to evaluate clinical cases in adults and children. PLoS ONE 2019, 14, e0224663. [Google Scholar] [CrossRef]
- Zobel, G.; Dacar, D.; Rödl, S. Hemodynamic effects of different modes of mechanical ventilation in acute cardiac and pulmonary failure: An experimental study. Crit. Care Med. 1994, 22, 1624–1630. [Google Scholar] [CrossRef] [PubMed]
- Marini, J.J.; Culver, B.H.; Butler, J. Mechanical effect of lung distention with positive pressure on cardiac function. Am. Rev. Respir. Dis. 1981, 124, 382–386. [Google Scholar] [CrossRef]
- De Lazzari, B.; Iacovoni, A.; Mottaghy, K.; Capoccia, M.; Badagliacca, R.; Vizza, C.D.; De Lazzari, C. ECMO Assistance during Mechanical Ventilation: Effects Induced on Energetic and Haemodynamic Variables. Comput. Methods Progr. Biomed. 2021, 202, 106003. [Google Scholar] [CrossRef]
- De Lazzari, C.; L’Abbate, A.; Micalizzi, M.; Trivella, M.G.; Neglia, D. Effects of amlodipine and adenosine on coronary haemodynamics: In vivo study and numerical simulation. Comput. Methods Biomech. Biomed. Eng. 2014, 17, 1642–1652. [Google Scholar] [CrossRef]
- Darowski, M.; De Lazzari, C.; Ferrari, G. Cardiovascular variables changes during positive pressure ventilation—Computer simulation. Biocybern. Biomed. Eng. 1996, 16, 85–95. [Google Scholar]
- Górczynska, K.; Ferrari, G.; De Lazzari, C.; Mimmo, R.; Tosti, G.; Clemente, F.; Englisz, M.; Guaragno, M. The influence of selected left ventricular and systemic parameters on cardiovascular hemodynamics and energetics—ModeIIing study. Biocybern. Biomed. Eng. 2000, 20, 35–47. [Google Scholar]
- Colquitt, R.B.; Colquhoun, D.A.; Thiele, R.H. In silico modelling of physiologic systems. Best Pr. Res. Clin. Anaesthesiol. 2011, 25, 499–510. [Google Scholar] [CrossRef]
- De Lazzari, C.; Darowski, M.; Ferrari, G.; Clemente, F. Energetic parameter changes with mechanical ventilation in conjunction with BVAD assistance. J. Med. Eng. Technol. 2002, 26, 63–70. [Google Scholar] [CrossRef] [PubMed]
- Darowski, M.; De Lazzari, C.; Ferrari, G.; Clemente, F.; Guaragno, M. The influence of simultaneous intraaortic balloon pumping and mechanical ventilation on hemodynamic parameters—Numerical simulation. Front. Med. Biol. Eng. 1999, 9, 155–174. [Google Scholar] [PubMed]
- De Lazzari, C.; Darowski, M.; Ferrari, G.; Clemente, F.; Guaragno, M. Ventricular energetics during mechanical ventilation and intraaortic balloon pumping--computer simulation. J. Med. Eng. Technol. 2001, 25, 103–111. [Google Scholar] [CrossRef] [PubMed]
- De Lazzari, C.; Darowski, M.; Ferrari, G.; Pisanelli, D.M.; Tosti, G. Modelling in the study of interaction of Hemopump device and artificial ventilation. Comput. Biol. Med. 2006, 36, 1235–1251. [Google Scholar] [CrossRef]
- De Lazzari, C.; Darowski, M.; Ferrari, G.; Pisanelli, D.M.; Tosti, G. The impact of rotary blood pump in conjunction with mechanical ventilation on ventricular energetic parameters—Numerical simulation. Methods Inf. Med. 2006, 45, 574–583. [Google Scholar]
- De Lazzari, C.; Genuini, I.; Quatember, B.; Fedele, F. Mechanical ventilation and thoracic artificial lung assistance during mechanical circulatory support with PUCA pump: In silico study. Comput. Methods Programs Biomed. 2014, 3, 642–654. [Google Scholar] [CrossRef]
- De Lazzari, B.; Iacovoni, A.; Capoccia, M.; Papa, S.; Badagliacca, R.; Filomena, D.; De Lazzari, C. Ventricular and Atrial Pressure-Volume Loops: Analysis of the Effects Induced by Right Centrifugal Pump Assistance. Bioengineering 2022, 9, 181. [Google Scholar] [CrossRef]
- De Lazzari, C.; De Lazzari, B.; Iacovoni, A.; Marconi, S.; Papa, S.; Capoccia, M.; Badagliacca, R.; Vizza, C.D. Intra-Aortic Balloon Counterpulsation Timing: A New Numerical Model for Programming and Training in the Clinical Environment. Comput. Methods Programs Biomed. 2020, 194, 105537. [Google Scholar] [CrossRef]
- De Lazzari, C.; Neglia, D.; Ferrari, G.; Bernini, F.; Micalizzi, M.; L’Abbate, A.; Trivella, M.G. Computer simulation of coronary flow waveforms during caval occlusion. Methods Inf. Med. 2009, 48, 113–122. [Google Scholar] [CrossRef]
- De Lazzari, C.; Capoccia, M.; Marconi, S. How can LVAD support influence ventricular energetics parameters in advanced heart failure patients? A retrospective study. Comput. Methods Programs Biomed. 2019, 172, 117–126. [Google Scholar] [CrossRef]
- De Lazzari, C.; Marconi, S.; Capoccia, M.; Papa, S.; Badagliacca, R.; Vizza, C.D. A 0-D Model to Predict the Relationship between Resistance and Compliance inPulmonary Arterial Hypertension. In Proceedings of the 31st European Modeling and Simulation Symposium, Lisbon, Portugal, 18–20 September 2019; pp. 23–28, ISBN 978-88-85741-25-6. [Google Scholar]
- De Lazzari, C.; Stalteri, D. 2011–2019, CARDIOSIM© Website. Available online: https://cardiosim.dsb.cnr.it/Esperimenti/Patient2 (accessed on 29 May 2022).
- Bassingthwaighte, J.; Hunter, P.; Noble, D. The cardiac physiome: Perspectives for the future. Exp. Physiol. 2009, 94, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Zimmerman, J.; Steinfeld, A.; Carey, L.; Antaki, J.F. Investigating the heart pump implant decision process: Opportunities for decision support tools to help. ACM Trans. Comput. Hum. Interact. 2016, 2016, 4477–4488. [Google Scholar] [PubMed]
- Arts, T.; Delhaas, T.; Bovendeerd, P.; Verbeek, X.; Prinzen, F.W. Adaptation to mechanical load determines shape and properties of heart and circulation: The circadapt model. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H1943–H1954. [Google Scholar] [CrossRef] [PubMed]
- Lumens, J.; Delhaas, T. Cardiovascular modelling in pulmonary arterial hypertension: Focus on mechanisms and treatment of right heart failure using the circadapt model. Am. J. Cardiol. 2012, 110, 39S–48S. [Google Scholar] [CrossRef]
- Lumens, J. Creating your own virtual patient with circadapt simulator. Eur. Heart J. 2014, 35, 335–337. [Google Scholar]
- Lumens, J.; Delhaas, T.; Kirn, B.; Arts, T. Three-wall segment (triseg) model describing mechanics and hemodynamics of ventricular interaction. Ann. Biomed. Eng. 2009, 37, 2234–2255. [Google Scholar] [CrossRef]
- Arts, T.; Lumens, J.; Kroon, W.; Delhaas, T. Control of whole heart geometry by intramyocardial mechano-feedback: A model study. PLoS Comput. Biol. 2012, 8, e1002369. [Google Scholar] [CrossRef]
- Arts, T.; Reesink, K.; Kroon, W.; Delhaas, T. Simulation of adaptation of blood vessel geometry to flow and pressure: Implications for arterio-venous impedance. Mech. Res. Commun. 2011, 42, 15–21. [Google Scholar] [CrossRef]
- Lumens, J.; Arts, T.; Marcus, J.T.; Vonk-Noordegraaf, A.; Delhaas, T. Early-diastolic left ventricular lengthening implies pulmonary hypertension-induced right ventricular decompensation. Cardiovasc. Res. 2012, 96, 286–295. [Google Scholar] [CrossRef]
- Lumens, J.; Ploux, S.; Strik, M.; Gorcsan, J., 3rd; Cochet, H.; Derval, N.; Strom, M.; Ramanathan, C.; Ritter, P.; Haissaguerre, M.; et al. Comparative electromechanical and hemodynamic effects of left ventricular and biventricular pacing in dyssynchronous heart failure: Electrical resynchronization versus left–right ventricular interaction. J. Am. Coll. Cardiol. 2013, 62, 2395–2403. [Google Scholar] [CrossRef]
- Larrabide, I.; Blanco, P.J.; Urquiza, S.A.; Dari, E.A.; Vénere, M.J.; de Souza e Silva, N.A.; Feijóo, R.A. HeMoLab—Haemodynamics Modelling Laboratory: An application for modelling the human cardiovascular system. Comput. Biol. Med. 2012, 42, 993–1004. [Google Scholar] [CrossRef] [PubMed]
- Blanco, P.J.; Clausse, A.; Feijóo, R.A. Homogenization of the Navier–stokes equations by means of the multi-scale virtual power principle. Comput. Methods Appl. Mech. Eng. 2017, 315, 760–779. [Google Scholar] [CrossRef]
- HeMoLab (Hemodynamics Modelling Laboratory). Available online: http://hemolab.lncc.br/ (accessed on 29 May 2022).
- Harvi. Interactive Software Simulator of Cardiovascular Physiology. Available online: http://www.pvloops.com (accessed on 29 May 2022).
- Santamore, W.P.; Burkhoff, D. Haemodynamic consequences of ventricular interaction as assessed by model analysis. Am. J. Physiol. Heart Circ. Physiol. 1991, 260, H146–H157. [Google Scholar] [CrossRef]
- Burkhoff, D.; Tyberg, J.V. Why does pulmonary venous pressure rise after onset of left ventricular dysfunction: A theoretical analysis. Am. J. Physiol. Heart Circ. Physiol. 1993, 265, H1819–H1828. [Google Scholar] [CrossRef]
- Updegrove, A.; Wilson, N.M.; Merkow, J.; Lan, H.; Marsden, A.L.; Shadden, S.C. SimVascular: An Open Source Pipeline for Cardiovascular Simulation. Ann. Biomed. Eng. 2017, 45, 525–541. [Google Scholar] [CrossRef]
- Lan, H.; Updegrove, A.; Wilson, N.M.; Maher, G.D.; Shadden, S.C.; Marsden., A.L. A Re-Engineered Software Interface and Workflow for the Open-Source SimVascular Cardiovascular Modelling Package. J Biomech. Eng. 2018, 140, 024501. [Google Scholar] [CrossRef] [PubMed]
- Saltarocchi, S. Simulation in Advanced Heart Failure with a View to Selection and Optimization of Device Therapy. Ph.D. Thesis, Sapienza University, Rome, Italy, 2018. [Google Scholar]






| First Version | Second Version | Version 7.3.2 |
|---|---|---|
| Ventricular filling and ejection phases are modeled separately to reproduce the behavior of the left and right ventricles. The time-varying elastance theory is used to reproduce the contraction and ejection phases [10,40]. | Ventricular filling and ejection phases are modeled separately to reproduce the behavior of the left and right ventricles. The time-varying elastance theory is used to reproduce the contraction and ejection phases. | Ventricular filling and ejection phases are modeled separately to reproduce the behavior of the left and right ventricles. The time-varying elastance theory is used to reproduce the contraction and ejection phases. |
| A linear capacity assuming a constant value is used to reproduce the behavior of both the right and left atria [10,40]. Only a passive phase of the atria (left and right) can be reproduced using a compliance with a constant value. | A linear capacity assuming a constant value is used to reproduce the behavior of both the right and left atria [10,40]. Only a passive phase of the atria (left and right) can be reproduced using a compliance with a constant value. | A linear capacity assuming a constant value is used to reproduce the behavior of both the right and left atria [10,40]. Only a passive phase of the atria (left and right) can be reproduced using a compliance with a constant value. |
| -------- | -------- | Both ventricles are modeled according to the time-varying elastance concept [13,19,41,42]. |
| -------- | -------- | Both atria are modeled according to the time-varying elastance concept [13,19,41,42]. |
| -------- | -------- | The time-varying elastance theory is used to reproduce the septal activity [13,19,41,42]. |
| The time-varying interventricular and interatrial septum is modeled [13]. |
| First Version | Second Version | Version 7.3.2 |
|---|---|---|
| Numerical model of pneumatic left ventricular assist device (LVAD) [40]. | Numerical model of pneumatic left ventricular assist device (LVAD). | Numerical model of pneumatic left ventricular assist device (LVAD). |
| -------- | Numerical model of pneumatic right ventricular assist device (RVAD). | Numerical model of pneumatic right ventricular assist device (RVAD). |
| -------- | Numerical model of pneumatic biventricular assist device (BVAD) [56]. | Numerical model of pneumatic biventricular assist device (BVAD). |
| --------- | Numerical model of pneumatic total artificial heart (TAH). | Numerical model of pneumatic total artificial heart (TAH). |
| --------- | First numerical model of intra-aortic balloon pump (IABP) [57,58]. | First numerical model of intra-aortic balloon pump (IABP). |
| --------- | --------- | Numerical model of intra-arterial axial flow blood pump (Hemopump® HP31) connected to the cardiovascular network as LVAD and/or RVAD [59,60]. |
| --------- | --------- | Numerical model of pulsatile LVAD blood flow (PUCA pump) [61]. |
| --------- | --------- | Numerical model of biventricular pacemaker (BiV) [43]. |
| --------- | --------- | Numerical model of thoracic artificial lung (TAL) [62]. |
| --------- | --------- | Numerical model of centrifugal blood pump connected to the cardiovascular network as LVAD and/or RVAD [62]. |
| --------- | --------- | Second numerical model of intra-aortic balloon pump (IABP) [63]. |
| --------- | --------- | Numerical model of Impella (LVAD)*. |
| --------- | --------- | Numerical model of extra-corporeal membrane oxygenation [51]. |
| --------- | --------- | Numerical model of ECMO coupled with the first numerical model of intra-aortic balloon pump (IABP) *. |
| --------- | --------- | Numerical model of ECMO coupled with Impella (LVAD) *. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Lazzari, B.; Badagliacca, R.; Filomena, D.; Papa, S.; Vizza, C.D.; Capoccia, M.; De Lazzari, C. CARDIOSIM©: The First Italian Software Platform for Simulation of the Cardiovascular System and Mechanical Circulatory and Ventilatory Support. Bioengineering 2022, 9, 383. https://doi.org/10.3390/bioengineering9080383
De Lazzari B, Badagliacca R, Filomena D, Papa S, Vizza CD, Capoccia M, De Lazzari C. CARDIOSIM©: The First Italian Software Platform for Simulation of the Cardiovascular System and Mechanical Circulatory and Ventilatory Support. Bioengineering. 2022; 9(8):383. https://doi.org/10.3390/bioengineering9080383
Chicago/Turabian StyleDe Lazzari, Beatrice, Roberto Badagliacca, Domenico Filomena, Silvia Papa, Carmine Dario Vizza, Massimo Capoccia, and Claudio De Lazzari. 2022. "CARDIOSIM©: The First Italian Software Platform for Simulation of the Cardiovascular System and Mechanical Circulatory and Ventilatory Support" Bioengineering 9, no. 8: 383. https://doi.org/10.3390/bioengineering9080383
APA StyleDe Lazzari, B., Badagliacca, R., Filomena, D., Papa, S., Vizza, C. D., Capoccia, M., & De Lazzari, C. (2022). CARDIOSIM©: The First Italian Software Platform for Simulation of the Cardiovascular System and Mechanical Circulatory and Ventilatory Support. Bioengineering, 9(8), 383. https://doi.org/10.3390/bioengineering9080383