
The Effects of Pedestrian Environment on Ambulation with a Walking Frame in Elderly Individuals: A Survey and Experimental Study

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Investigation of Pedestrian Environment Encountered by Elderly Individuals Walking with a Walking Frame
2.2. Quantitative Research in a Typical Pedestrian Environment
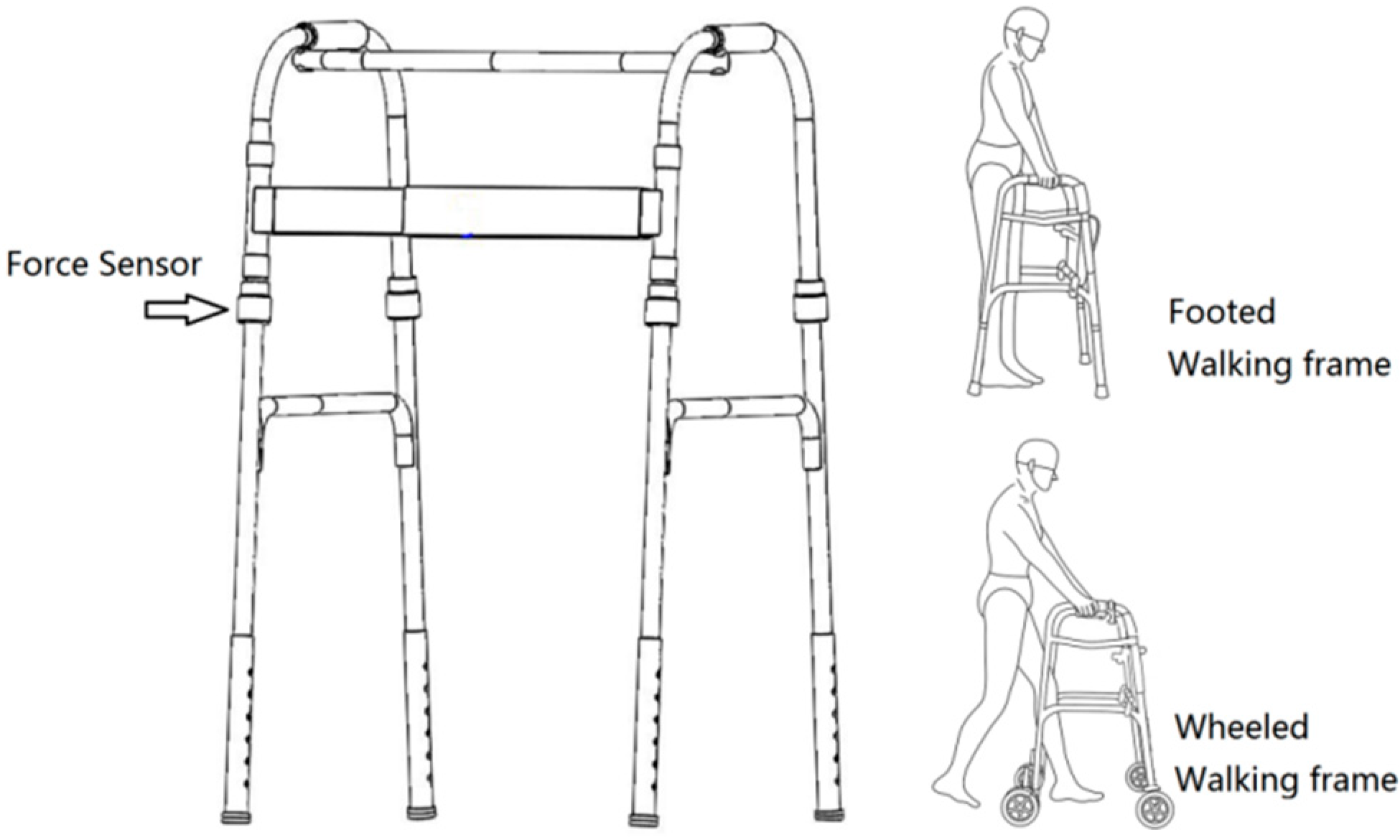
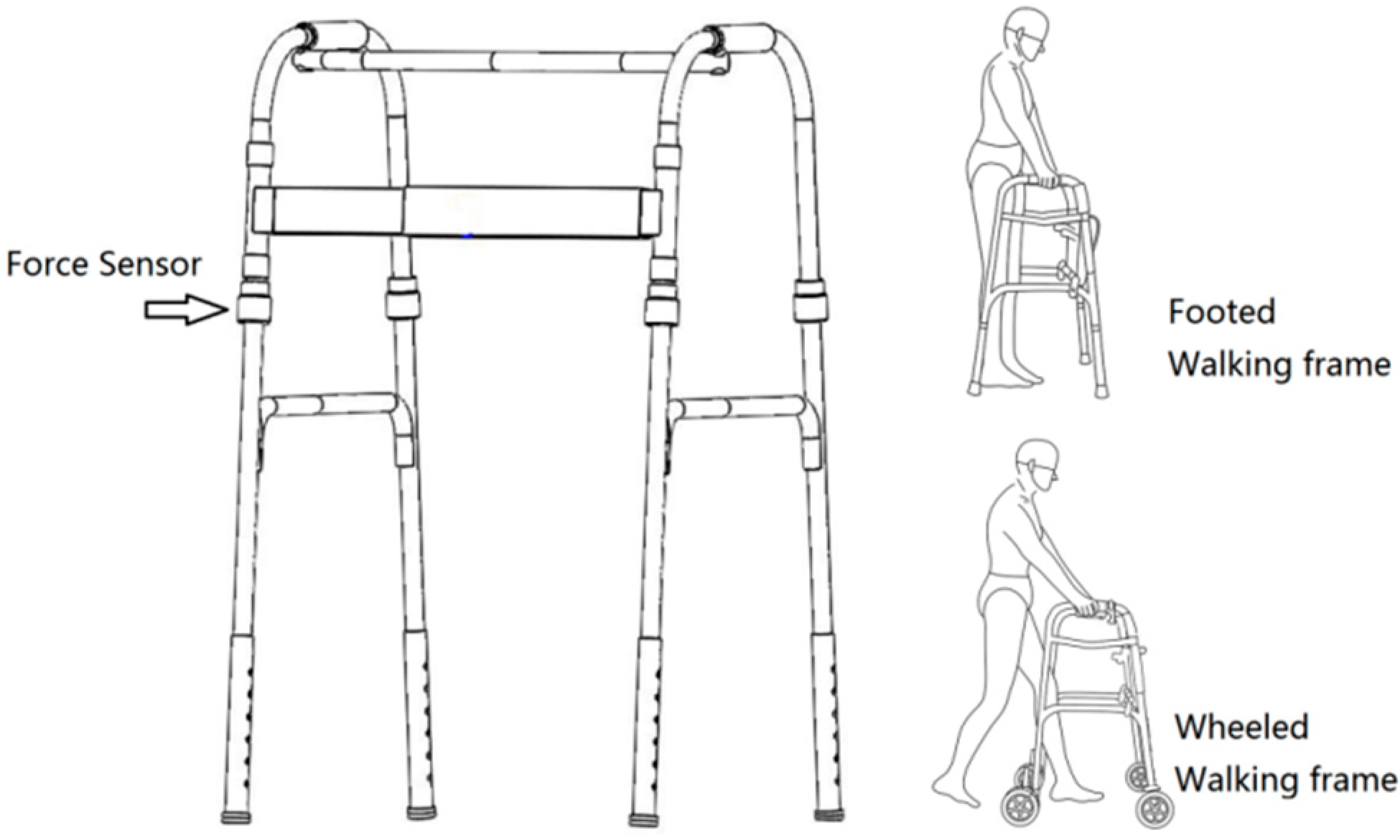
2.2.1. Experimental Materials
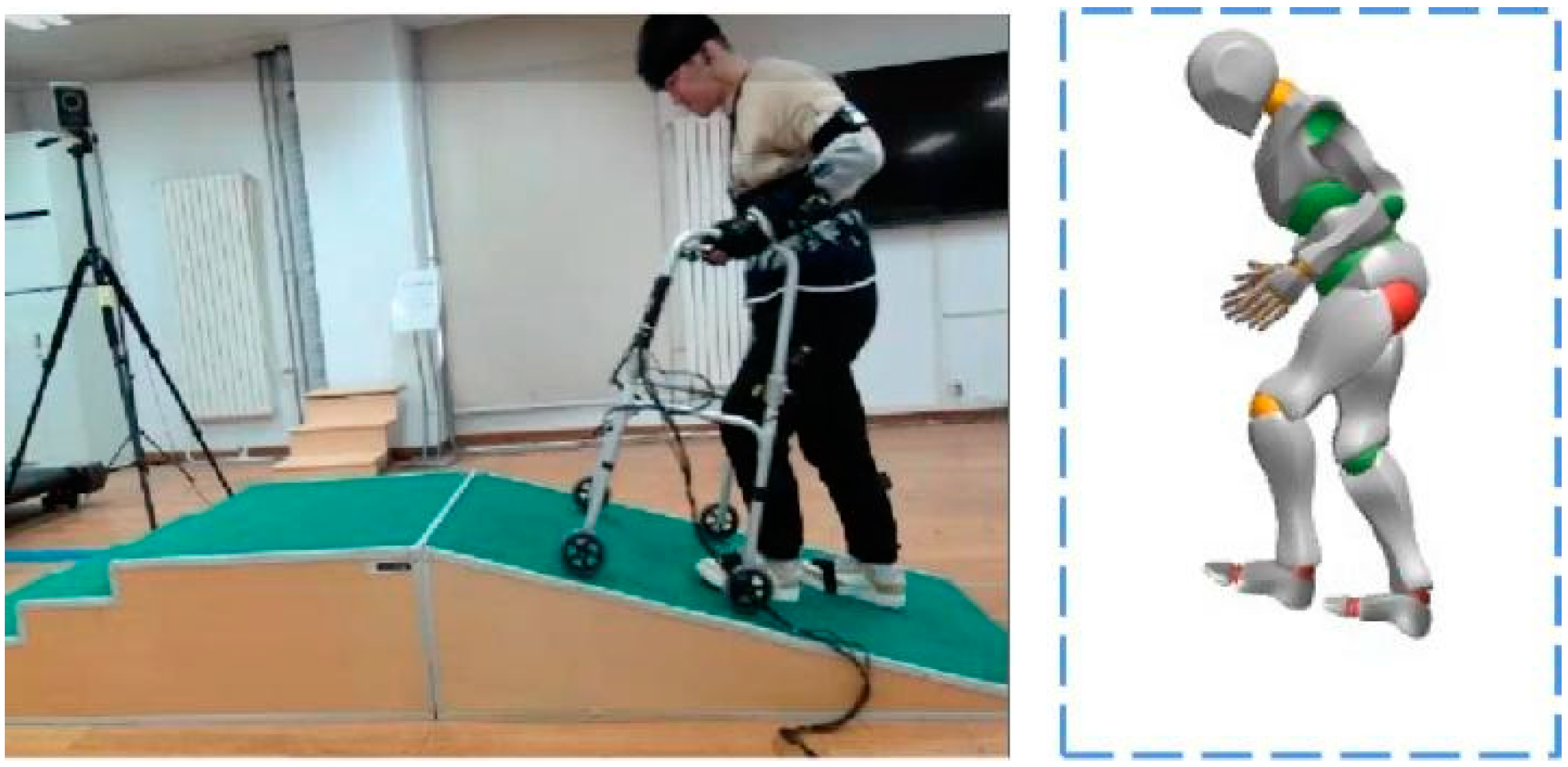
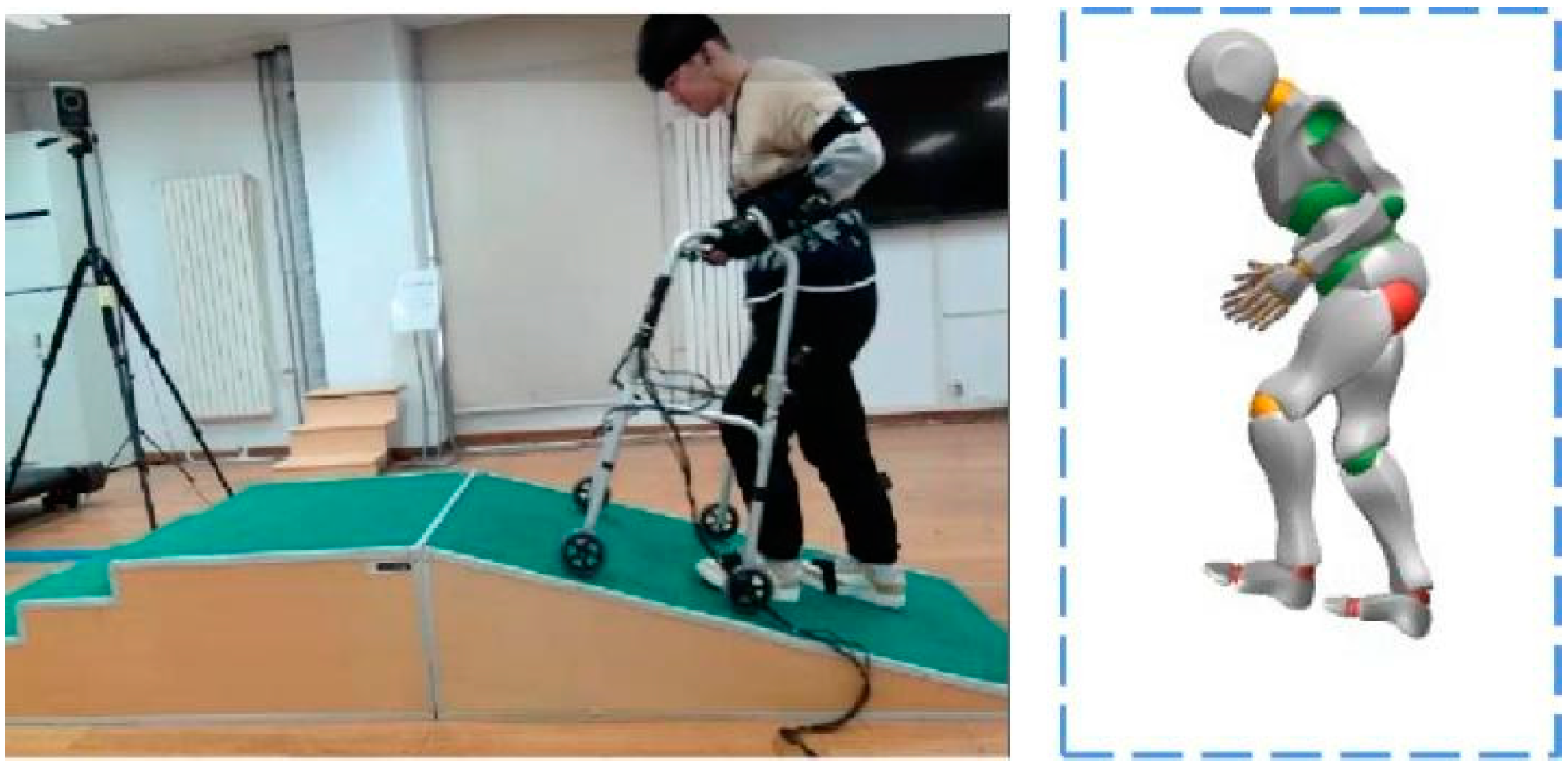
2.2.2. Experimental Methods
3. Results
3.1. Empirical Results from the Community
3.1.1. Problems with the Environment for Elderly Individuals
3.1.2. Behaviors of Elderly Individuals in the Different Cases
3.2. A Controlled Study Results in a Laboratory Scenario
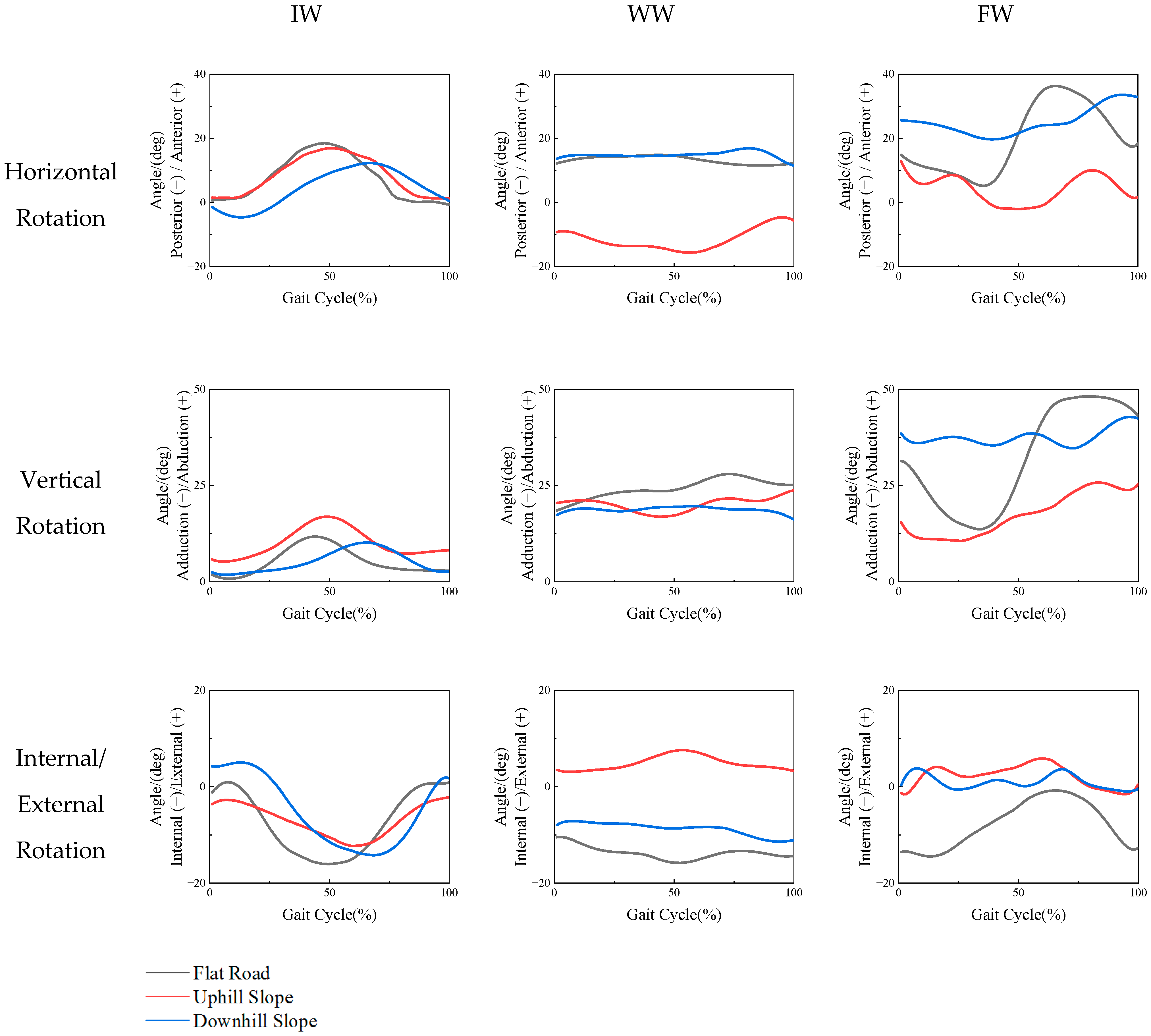
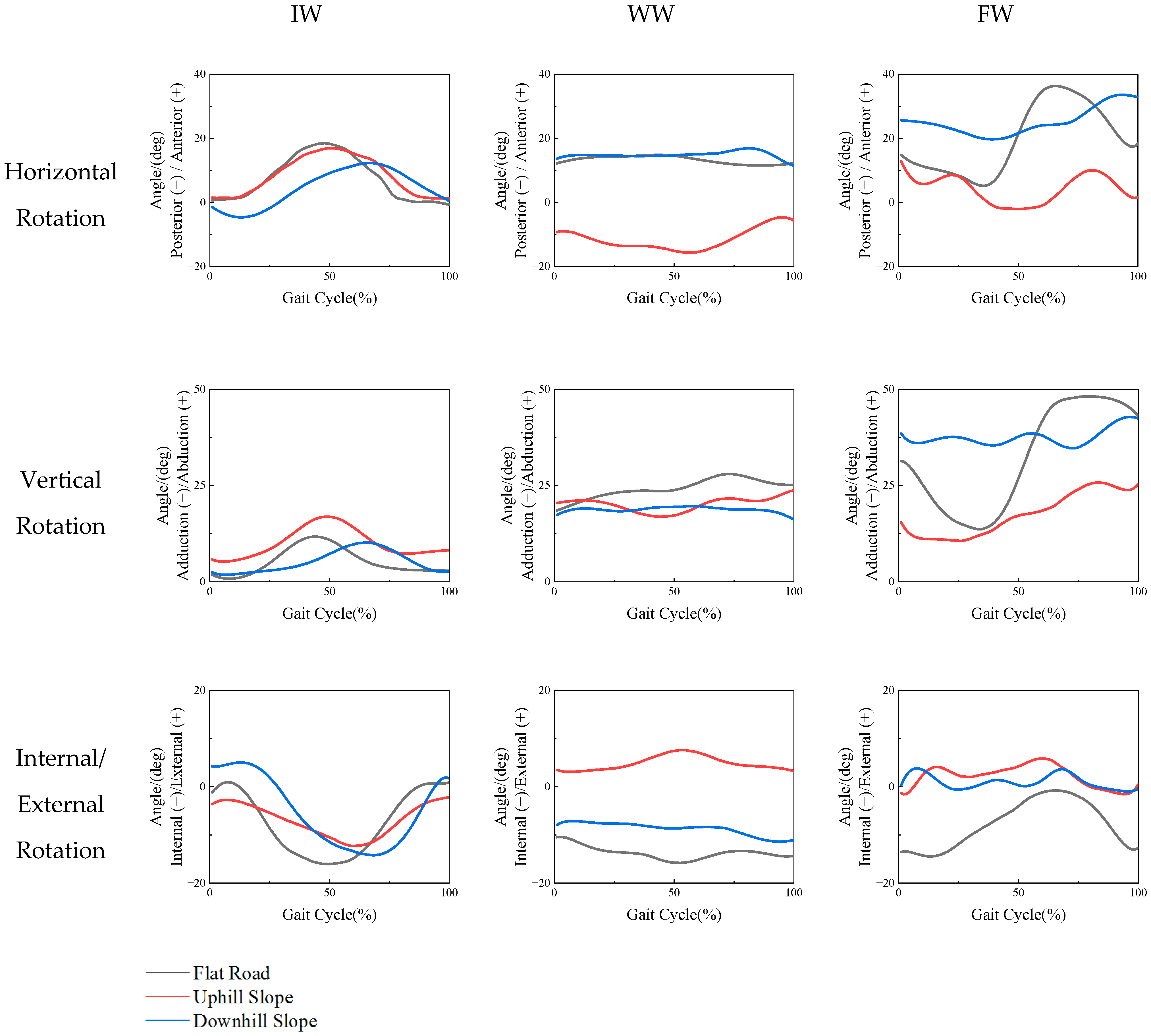
3.2.1. Shoulder Motion Characteristics
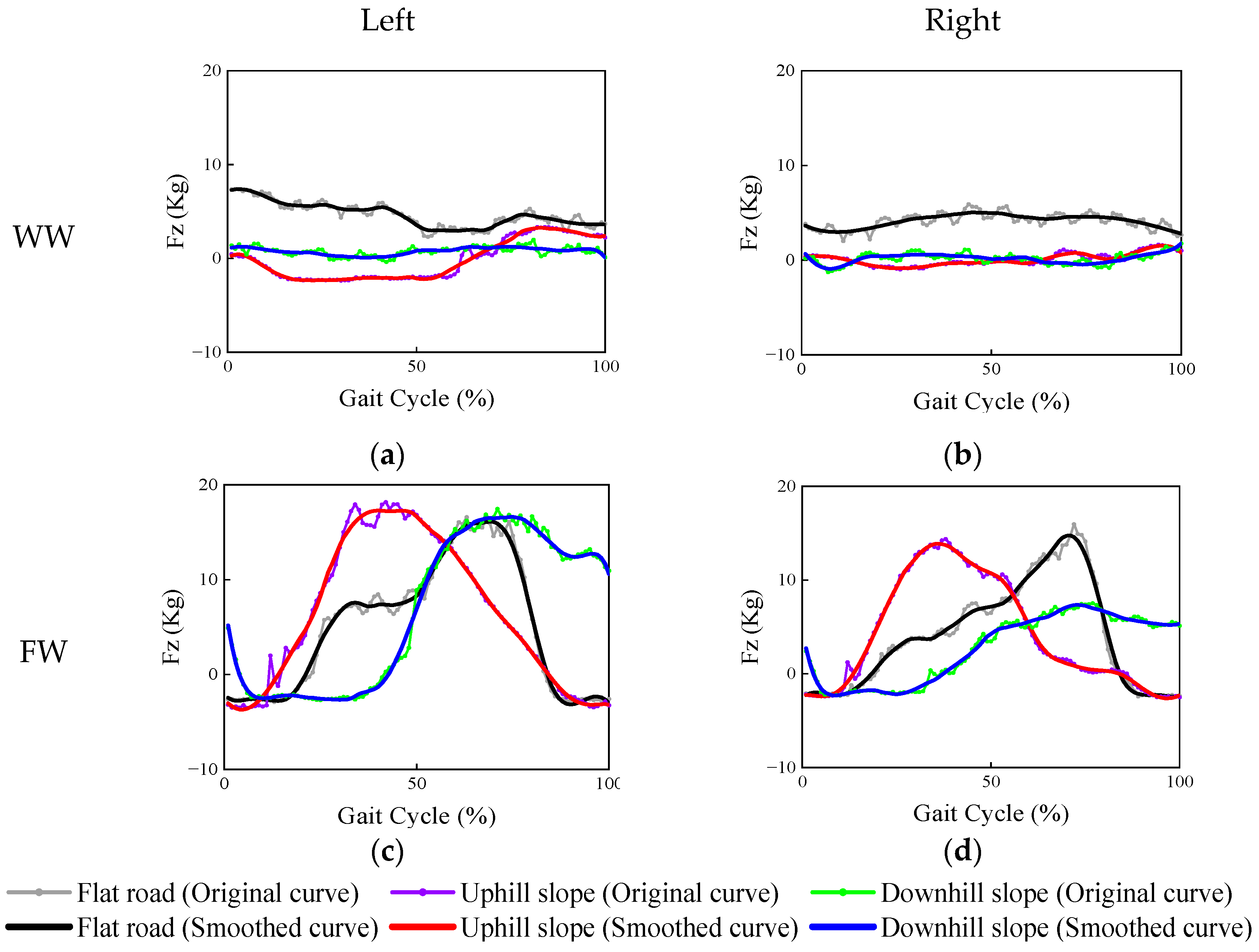
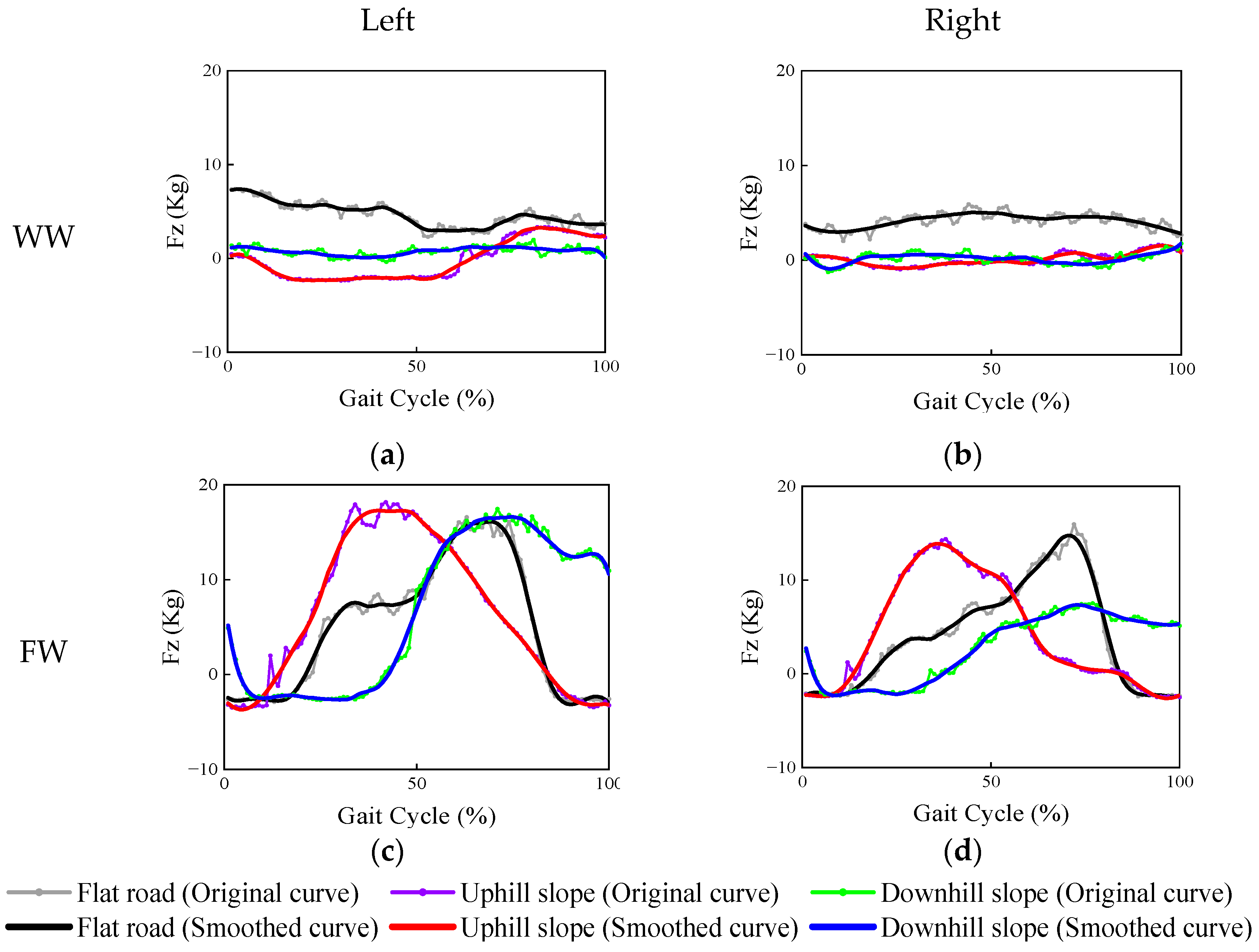
3.2.2. Supporting Force Characteristics
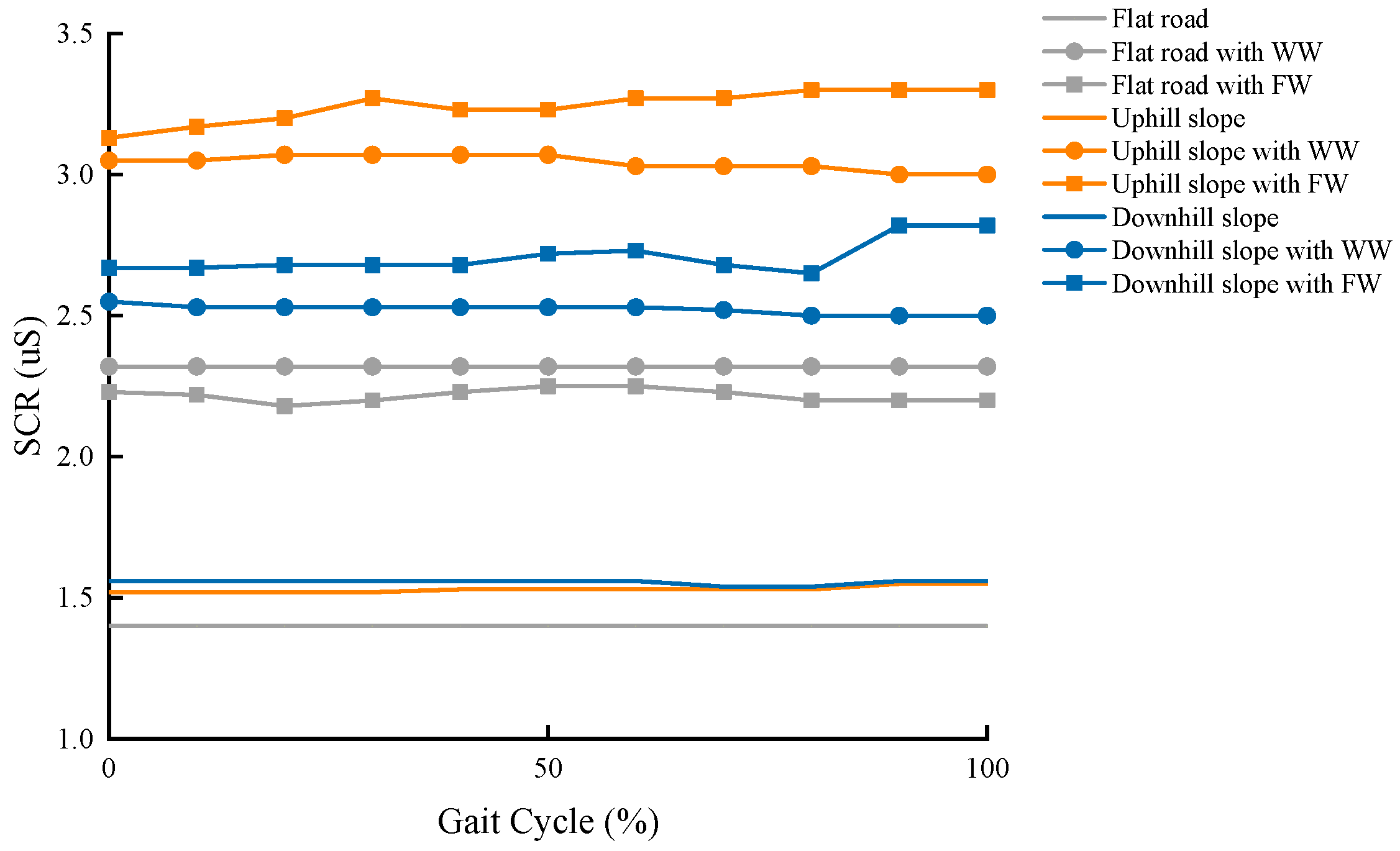
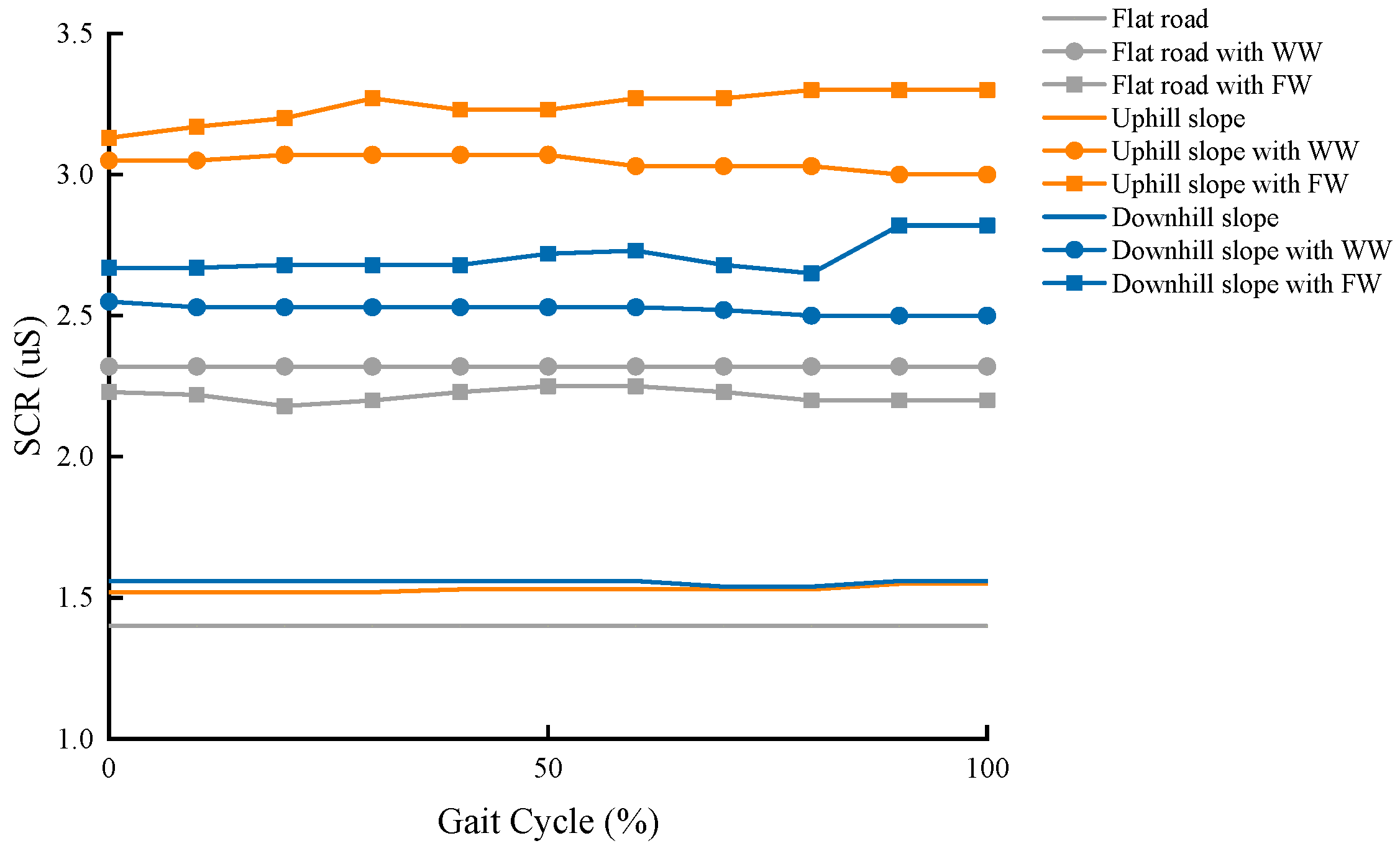
3.2.3. SCR Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Papadopoulos, D. The Role of Well-Being, Spirituality, and Religiosity for Successful Aging in Late Life: A Brief Review. Adv. Aging Res. 2020, 9, 23–31. [Google Scholar] [CrossRef] [Green Version]
- Wang, T.; Merlet, J.-P.; Sacco, G.; Robert, P.; Turpin, J.-M.; Teboul, B.; Marteu, A.; Guerin, O. Walking analysis of young and elderly people by using an intelligent walker ANG. Robot. Auton. Syst. Part A 2016, 75, 96–106. [Google Scholar] [CrossRef] [Green Version]
- Rahaman, M.S.; Mei, Y.; Hamilton, M.; Salim, F.D. CAPRA: A contour-based accessible path routing algorithm. Inf. Sci. 2017, 385–386, 157–173. [Google Scholar] [CrossRef]
- Takanokura, M. Optimal handgrip height of four-wheeled walker on various road conditions to reduce muscular load for elderly users with steady walking. J. Biomech. 2010, 43, 843–848. [Google Scholar] [CrossRef] [PubMed]
- Wakita, K.; Huang, J.; Di, P.; Sekiyama, K.; Fukuda, T. Human-Walking-Intention-Based Motion Control of an Omnidirectional-Type Cane Robot. IEEE/ASME Trans. Mechatron. 2011, 18, 285–296. [Google Scholar] [CrossRef]
- Wennberg, H.; Hydén, C.; Ståhl, A. Barrier-free outdoor environments: Older peoples’ perceptions before and after implementation of legislative directives. Transp. Policy 2010, 17, 464–474. [Google Scholar] [CrossRef]
- Amaya, V.; Moulaert, T.; Gwiazdzinski, L.; Vuillerme, N. Assessing and Qualifying Neighborhood Walkability for Older Adults: Construction and Initial Testing of a Multivariate Spatial Accessibility Model. Int. J. Environ. Res. Public Health 2022, 19, 1808. [Google Scholar] [CrossRef]
- Miura, T.; Yabu, K.-I.; Ikematsu, S.; Kano, A.; Ueda, M.; Suzuki, J.; Sakajiri, M.; Ifukube, T. Barrier-free walk: A social sharing platform of barrier-free information for sensory/physically-impaired and aged people. In Proceedings of the IEEE International Conference on Systems, Seoul, Korea, 14–17 October 2012; pp. 2927–2932. [Google Scholar] [CrossRef]
- Sehgal, M.; Jacobs, J.; Biggs, W.S. Mobility Assistive Device Use in Older Adults. Am. Fam. Physician 2021, 103, 737–744. [Google Scholar]
- Cheng, T.; Kenney, L.; Amor, J.D.; Thies, S.B.; Costamagna, E.; James, C.; Holloway, C. Characterisation of rollator use using inertial sensors. Health Technol. Lett. 2016, 3, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Martins, M.M.; Santos, C.P.; Frizera-Neto, A.; Ceres, R. Assistive mobility devices focusing on Smart Walkers: Classification and review. Robot. Auton. Syst. 2012, 60, 548–562. [Google Scholar] [CrossRef] [Green Version]
- Fareed, N.; Southerland, L.T.; Rao, B.M.; Sieck, C.J. Geriatric assistive devices improve older patient engagement and clinical care in an emergency department. Am. J. Emerg. Med. 2020, 46, 656–658. [Google Scholar] [CrossRef] [PubMed]
- Bateni, H.; Maki, B.E. Assistive devices for balance and mobility: Benefits, demands, and adverse consequences. Arch. Phys. Med. Rehabil. 2005, 86, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, N.A.; Clarke, P.; Carr, E. Physical activity in older adults in a combined functional circuit and walking program. Geriatr. Nurs. 2016, 37, 353–359. [Google Scholar] [CrossRef] [PubMed]
- Mcquade, K.J.; Finley, M.; Oliveira, A.S. Upper extremity joint stresses during walkerassisted ambulation in post-surgical patients. Braz. J. Phys. Ther. 2011, 15, 332–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ishikura, T. Biomechanical analysis of weight bearing force and muscle activation levels in the lower extremities during gait with a walker. Acta Med. Okayama 2001, 55, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Zhao, Y.; Salem, Y.; Miller, K.; Quiben, M.; Liu, H. Postural effect on gait characteristics by using rolling walkers. Geriatr. Nurs. 2020, 41, 916–920. [Google Scholar] [CrossRef] [PubMed]
- Baniasad, M.; Farahmand, F.; Arazpour, M.; Zohoor, H. Role and Significance of Trunk and Upper Extremity Muscles in Walker-Assisted Paraplegic Gait: A Case Study. Top. Spinal Cord Inj. Rehabil. 2018, 24, 18–27. [Google Scholar] [CrossRef] [PubMed]
- Simoneau, G.; Hambrook, G.; Bachschmidt, R.; Harris, G. Quantifying upper extremity efforts when using a walking frame. In Proceedings of the Pediatric Gait, A New Millennium in Clinical Care and Motion Analysis Technology, Chicago, IL, USA, 22 July 2000; pp. 210–216. [Google Scholar] [CrossRef]
- Dozono, K.; Hachisuka, A.; Wada, F.; Hachisuka, K. Peripheral Neuropathies in Nonparetic Upper Extremities of Stroke Patients Induced by Excessive Use of a Walking Device. J. Stroke Cerebrovasc. Dis. 2015, 24, 1841–1847. [Google Scholar] [CrossRef]
- Stevens, J.C.; Beard, C.M.; O’Fallon, W.M.; Kurland, L.T. Conditions Associated with Carpal Tunnel Syndrome. Mayo Clin. Proc. 1992, 67, 541–548. [Google Scholar] [CrossRef]
- Maki, B.E.; Holliday, P.J.; Topper, A.K. A Prospective Study of Postural Balance and Risk of Falling in An Ambulatory and Independent Elderly Population. J. Gerontol. 1994, 49, M72–M84. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.; Kang, S.R.; Yang, G.; Hong, C.U.; Lee, H.J.; Oh, D.Y.; Kwon, T.K. Preliminary study on verifying the detection of gait intention based on knee joint anterior displacement of gait slopes. Bio-Med. Mater. Eng. 2015, 26, S583–S592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashizume, T.; Kitagawa, H.; Mohri, T.; Fujisawa, S. Evaluation of Physical Load while Propelling a Manual Wheelchair on Slope. In Proceedings of the JSME Annual Conference on Robotics and Mechatronics (Robomec), Okayama, Japan, 26–28 May 2011. [Google Scholar] [CrossRef]
- Chini, L.T.; Pereira, D.S.; Nunes, A.A. Validation of the Fall Risk Tracking Tool (FRRISque) in elderly community dwellers. Cienc. Saude Coletiva 2019, 24, 2845–2858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thies, S.B.; Bates, A.; Costamagna, E.; Kenney, L.; Granat, M.; Webb, J.; Howard, D.; Baker, R.; Dawes, H. Are older people putting themselves at risk when using their walking frames? BMC Geriatr. 2020, 20, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Pool, E.R.; Sander, D. Chapter 5—Emotional learning: Measuring how affective values are acquired and updated. In Emotion Measurement, 2nd ed.; Meiselman, H.L., Ed.; Woodhead Publishing: Sawston, Cambridge, UK, 2021; pp. 133–165. [Google Scholar] [CrossRef]
- Benedek, M.; Kaernbach, C. A continuous measure of phasic electrodermal activity. J. Neurosci. Methods 2010, 190, 80–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figner, B.; Murphy, R.O. Using skin conductance in judgment and decision making research. In A Handbook of Process Tracing Methods for Decision Research; Schulte-Mecklenbeck, M., Kühberger, A., Ranyard, R., Eds.; Psychology Press: New York, NY, USA, 2011; pp. 163–184. [Google Scholar]
- Dolu, N.; Elalmiş, D.D.; Keloğlan, S. Examination of Attention Level in Nurses Working Night Shifts in terms of the Rela-tionship between Electrodermal Activity and Sex Hormones. Nöro Psikiyatr. Arşivi 2013, 50, 197–201. [Google Scholar] [CrossRef]
- Hambrook, G.W.; Simoneau, G.G.; Bachschmidt, R.A.; Harris, G.F. Biomechanical effect of changes in walker height and position on sagittal plane elbow dynamics for rehabilitation purposes. In Proceedings of the International Conference of the IEEE Engineering in Medicine & Biology Society, Hong Kong, China, 29 October–1 November 1998. [Google Scholar] [CrossRef]
- Miller, D.I.; Morrison, W.E. Prediction of segmental parameters using the Hanavan human body model. Med. Sci. Sports Exerc. 1975, 7, 207–212. [Google Scholar] [CrossRef]
- Bauer, E.A.; Wilson, K.A.; MacNamara, A. 3.03—Cognitive and Affective Psychophysiology. In Comprehensive Clinical Psychology, 2nd ed.; Asmundson, G.J.G., Ed.; Elsevier: Oxford, UK, 2022; Volume 3, pp. 49–61. [Google Scholar] [CrossRef]
- Youdas, J.W.; Kotajarvi, B.J.; Padgett, D.J.; Kaufman, K.R. Partial weight-bearing gait using conventional assistive devices. Arch. Phys. Med. Rehabil. 2005, 86, 394–398. [Google Scholar] [CrossRef]
- Rosenberg, D.E.; Huang, D.L.; Simonovich, S.D.; Belza, B. Outdoor Built Environment Barriers and Facilitators to Activity among Midlife and Older Adults with Mobility Disabilities. Gerontologist 2013, 53, 268–279. [Google Scholar] [CrossRef] [Green Version]
- Edelstein, J. 36—Canes, Crutches, and Walkers. In Atlas of Orthoses and Assistive Devices, 5th ed.; Webster, J.B., Murphy, D.P., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 377–382. [Google Scholar] [CrossRef]
- Jain, N.B.; Higgins, L.D.; Katz, J.N.; Garshick, E. Association of Shoulder Pain With the Use of Mobility Devices in Persons With Chronic Spinal Cord Injury. Phys. Med. Rehabil. 2010, 2, 896–900. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; McGee, M.; Wang, W.; Persson, M. Comparison of gait characteristics between older rolling walker users and older potential walker users. Arch. Gerontol. Geriatr. 2009, 48, 276–280. [Google Scholar] [CrossRef] [PubMed]
- Bakhsh, W.; Nicandri, G. Anatomy and Physical Examination of the Shoulder. Sports Med. Arthrosc. Rev. 2018, 26, e10–e22. [Google Scholar] [CrossRef] [PubMed]
- Konop, K.A.; Strifling, K.M.; Krzak, J.; Graf, A.; Harris, G.F. Upper Extremity Joint Dynamics During Walker Assisted Gait: A Quantitative Approach Towards Rehabilitative Intervention. J. Exp. Clin. Med. 2011, 3, 213–217. [Google Scholar] [CrossRef]
- Tat, C.C.; Jauw, V.L.; Parasuraman, S. Kinematics and Kinetics Studies on Upper Extremity during Walking Frame Ambula-tion. In Trends in Intelligent Robotics, Automation, and Manufacturing, IRAM 2012. Communications in Computer and In-Formation Science; Ponnambalam, S.G., Parkkinen, J., Ramanathan, K.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2012; Volume 330, pp. 206–215. [Google Scholar] [CrossRef]
- Tat, C.C.; Parasuraman, S.; Khan, M.A.; Elamvazuthi, I. Walking support system for Ageing Community. In Proceedings of the International Conference on Recent Trends in Electrical, Control and Communication, Malaysia, 20–22 March 2018. [Google Scholar] [CrossRef]
- Bachschmidt, R.; Harris, G.; Simoneau, G. Walker-assisted gait in rehabilitation: A study of biomechanics and instrumentation. IEEE Trans. Neural Syst. Rehabil. Eng. 2001, 9, 96–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pardo, R.; Winter, D.; Deathe, A. System for routine assessment of walker-assisted gait. Clin. Biomech. 1993, 8, 73–80. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number | Year | Area (Hectares) | Number of Buildings | Number of Public Activity Spaces |
|---|---|---|---|---|
| Community 1 | 1997 | 24 | 23 multi-story residential buildings and 5 high-rise residential buildings | 6 |
| Community 2 | 1991 | 19 | 18 multi-story residential buildings and 8 high-rise residential buildings | 4 |
| Community 3 | 1990 | 8 | 9 multi-story residential buildings and 3 high-rise residential buildings | 2 |
| Community 4 | 1995 | 14 | 21 multi-story residential buildings and no high-rise residential buildings | 4 |
| Community 5 | 1988 | 17 | 17 multi-story residential buildings and 8 high-rise residential buildings | 2 |
| Pedestrian Environments | Problems |
|---|---|
| Roads in the community | Coexistence of people and vehicles |
| Sidewalks are occupied | |
| Narrow sidewalk | |
| Deceleration belt hinders walking | |
| Drainage grate is close to deceleration belt | |
| Entrance of buildings | No sloped walkway at the building entrance |
| Inappropriate gradient of sloped road | |
| Sloped roads are occupied | |
| Aisle spaces are occupied | |
| Sloped road is directly connected to vehicle road | |
| Barrier-free sloped road with pipe shaft | |
| Public activity Spaces | A height difference between the space and the sidewalk |
| Sloped roads are occupied by vehicles | |
| Uneven ground | |
| Paving of small facing bricks on the ground | |
| Dazzling lights on the ground | |
| Uneven pavement caused by water pipes |
| Environment Problems | Performance |
|---|---|
| Incoherent and disorganized accessibility | Accessible designs that directed elderly individuals to their destination are often not coherent enough. Generally, the following need to be properly connected: entrance to the residential building → roads → entrance to the destination or public square. |
| Poor traffic layouts | Mixed modality routes were used by pedestrians and vehicles; some sidewalks are too narrow; and more than half of a sidewalk was blocked by trees. As a result, there might be insufficient space for an elderly person to use a walking aid. |
| Not enough attention is given to the details and there may be hidden dangers | The key parts of some accessible routes were poorly designed and may contain hidden dangers. |
| Poor or disorganized management of public spaces | Ramps were frequently blocked, which hinders the travel of elderly individuals. |
| Cases | Behaviors of Elderly Individuals |
|---|---|
| On level ground | Some elderly people can remain upright when using a walker, whereas others, due to their poorer sense of balance, lean their upper body toward the walking frame while walking. |
| On uneven ground | Due to their poorer sense of balance, elderly people are more likely to fall. Moreover, the walking frame would swing and become difficult to control. |
| Going uphill or downhill, climbing the stairs | Due to their weaker and less well-coordinated leg muscles, elderly individuals were clumsier when moving uphill and downhill or going up and down stairs. Since it is difficult to carry a walking frame forward, old people need others to bring the frame to the destination. They walk slowly forward while holding onto a handrail. If there is no handrail, they would need someone to support them. After walking, they have to sit down and rest. |
| Obstacles | They often stopped and took a short break before walking again. |
| Carrying heavy objects | Due to the weakened functioning of their body, especially in terms of the muscles, bones, and nervous system, elderly people could not carry heavy objects. |
| Getting up after sitting down for a long time | With atrophied leg muscles, especially calf muscles, and osteoporosis, it might be difficult to change from a sitting to a standing position. An elderly person can easily lose their balance. When an elderly person rises after sitting or squatting for a long time, they may feel dizzy. |
| Long duration of walking | Old people often move in a stop-and-start manner. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, J.; He, C.; Mo, Z.; Guo, J.; Ji, R.; Wang, Y.; Tao, C.; Fan, Y. The Effects of Pedestrian Environment on Ambulation with a Walking Frame in Elderly Individuals: A Survey and Experimental Study. Int. J. Environ. Res. Public Health 2022, 19, 9327. https://doi.org/10.3390/ijerph19159327
Yang J, He C, Mo Z, Guo J, Ji R, Wang Y, Tao C, Fan Y. The Effects of Pedestrian Environment on Ambulation with a Walking Frame in Elderly Individuals: A Survey and Experimental Study. International Journal of Environmental Research and Public Health. 2022; 19(15):9327. https://doi.org/10.3390/ijerph19159327
Chicago/Turabian StyleYang, Jiemeng, Chen He, Zhongjun Mo, Junchao Guo, Run Ji, Yu Wang, Chunjing Tao, and Yubo Fan. 2022. "The Effects of Pedestrian Environment on Ambulation with a Walking Frame in Elderly Individuals: A Survey and Experimental Study" International Journal of Environmental Research and Public Health 19, no. 15: 9327. https://doi.org/10.3390/ijerph19159327
APA StyleYang, J., He, C., Mo, Z., Guo, J., Ji, R., Wang, Y., Tao, C., & Fan, Y. (2022). The Effects of Pedestrian Environment on Ambulation with a Walking Frame in Elderly Individuals: A Survey and Experimental Study. International Journal of Environmental Research and Public Health, 19(15), 9327. https://doi.org/10.3390/ijerph19159327