Systematic Literature Review on Economic Evaluations and Health Economic Models in Metastatic Castration-Sensitive Prostate Cancer

 , , , , and
, , , , and
Simple Summary
Abstract

1. Introduction
2. Materials and Methods
3. Results
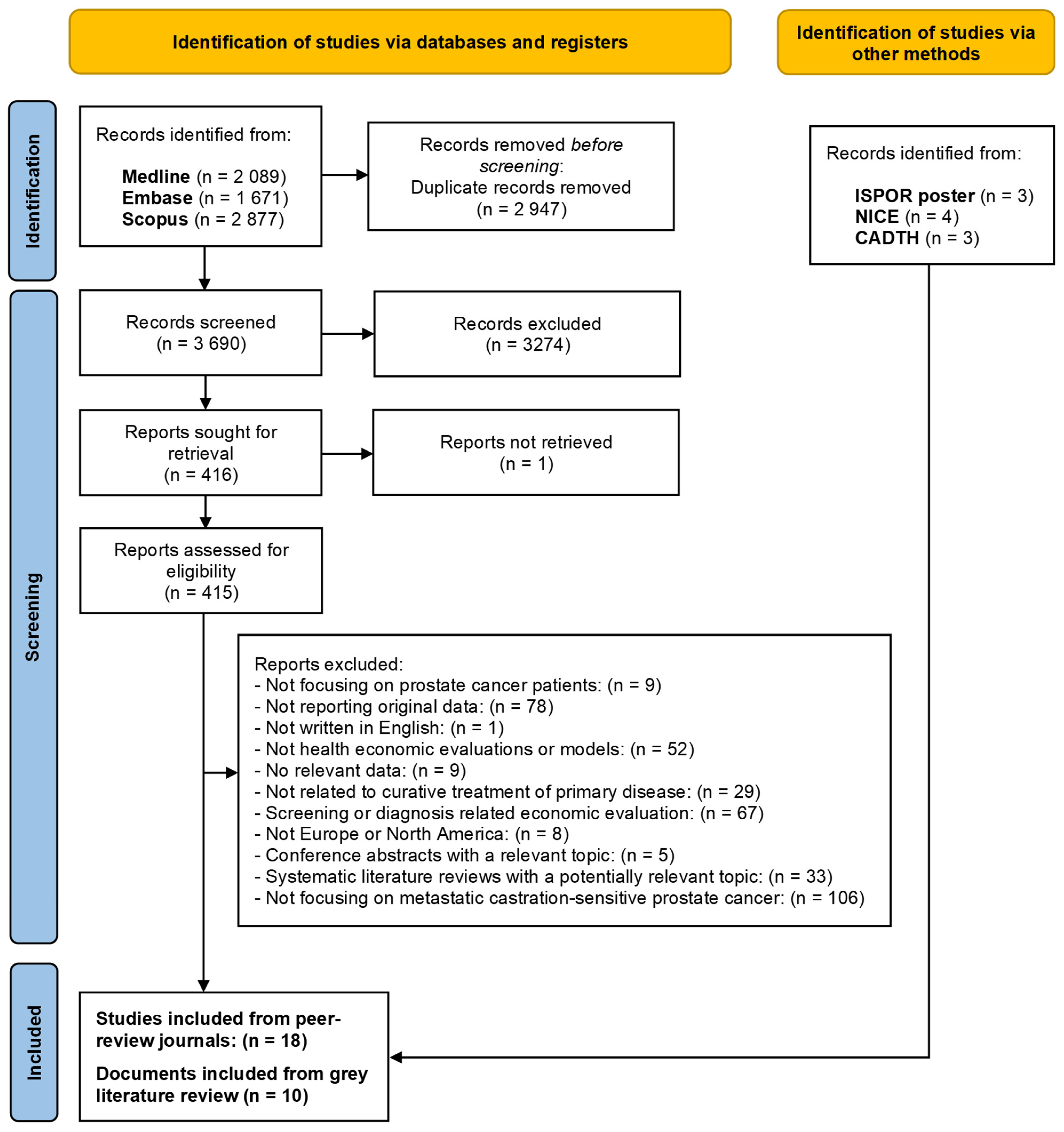
3.1. Literature Findings
3.2. Health Economic Evaluations from Peer-Reviewed Publications
3.2.1. Markov Simulation Models on mCSPC
3.2.2. Hybrid Economic Model mCSPC
3.2.3. Markov Cohort Models/Partitioned Survival Models on mCSPC
3.3. Health Economic Evaluations from Conference Posters
3.4. Health Economic Evaluations from HTA Bodies
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADT | Androgen Deprivation Therapy |
| ARPI | Androgen Receptor Pathway Inhibitors |
| CADTH | Canadian Agency for Drugs & Technologies in Health |
| GenAI | Generative Artificial Intelligence |
| HTA | Health Technology Assessment |
| ISPOR | International Society for Pharmacoeconomics and Outcomes Research |
| LHRH | Luteinizing hormone-releasing hormone |
| LYG | Life Years Gained |
| mCRPC | Metastatic Castration-Resistant Prostate Cancer |
| mCSPC | Metastatic Castration-Sensitive Prostate Cancer |
| mHRPC | Metastatic Hormone-Resistant Prostate Cancer |
| mHSPC | Metastatic Hormone-Sensitive Prostate Cancer |
| NICE | National Institute for Health and Care Excellence |
| PC | Prostate Cancer |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| QALY | Quality-Adjusted Life-Year |
Appendix A

{kind=link}
{kind=link}
| P (patient/population) | patients with prostate cancer |
| I (intervention/indicator) | all systemic treatment patterns (studies on screening or diagnosis will be excluded) |
| C (comparison) | all systemic treatment patterns (studies on screening or diagnosis will be excluded) |
| O (outcomes of interest) | data related to health economic evaluations and models |
| S (study design/setting) |
|
| Search No. | Concepts | Search String |
|---|---|---|
| #1 | Patient | (“prostate”[Title/Abstract] OR “prostatic”[Title/Abstract]) AND (“cancer”[Title/Abstract] OR “neoplasm”[Title/Abstract] OR “tumor”[Title/Abstract] OR “tumour”[Title/Abstract]) |
| #2 | Outcome | (cost[Title/Abstract] AND effectiveness[Title/Abstract]) OR cost-effectiveness[Title/Abstract] OR “cost-effectiveness analys*”[Title/Abstract] OR cea[Title/Abstract] OR (cost[Title/Abstract] AND benefit[Title/Abstract]) OR cost-benefit[Title/Abstract] OR “cost-benefit analys*”[Title/Abstract] OR cba[Title/Abstract] OR (cost[Title/Abstract] AND utility[Title/Abstract]) OR cost-utility[Title/Abstract] OR “cost-utility analys*”[Title/Abstract] OR cua[Title/Abstract] OR “incremental cost effectiveness ratio”[Title/Abstract] OR “incremental cost-effectiveness ratio”[Title/Abstract] OR icer[Title/Abstract] OR “discrete event simulation”[Title/Abstract] OR markov[Title/Abstract] OR “decision tree”[Title/Abstract] OR (economic[Title/Abstract] AND (model*[Title/Abstract] OR analys*[Title/Abstract] OR evaluation[Title/Abstract])) OR “health technology assessment”[Title/Abstract] OR hta[Title/Abstract] OR ((health[Title/Abstract] AND economic[Title/Abstract]) AND (model*[Title/Abstract] OR analys*[Title/Abstract] OR evaluation[Title/Abstract])) OR “event history model”[Title/Abstract] OR microsimulation[Title/Abstract] OR “Monte Carlo”[Title/Abstract] OR “Monte-Carlo”[Title/Abstract] OR “patient level simulation”[Title/Abstract] OR “patient-level simulation”[Title/Abstract] OR “deterministic sensitivity analys*”[Title/Abstract] OR “probabilistic sensitivity analys*”[Title/Abstract] OR “simulation model*”[Title/Abstract] OR “transition probabilit*”[Title/Abstract] OR “Tornado diagram”[Title/Abstract] |
| #3 | Combined search | #1 AND #2 |
| #4 | Filters | Limit to 2008–2023 |
| #5 | Filters | Limit to English (2089 hits) |
| Search No. | Concepts | Search String |
|---|---|---|
| #1 | Patient | (prostate:ti,ab,kw OR prostatic:ti,ab,kw) AND (cancer:ti,ab,kw OR neoplasm:ti,ab,kw OR tumor:ti,ab,kw OR tumour:ti,ab,kw) |
| #2 | Outcome | cost:ti,ab,kw AND effectiveness:ti,ab,kw OR ‘cost effectiveness’:ti,ab,kw OR ‘cost-effectiveness analys*’:ti,ab,kw OR cea:ti,ab,kw OR (cost:ti,ab,kw AND benefit:ti,ab,kw) OR ‘cost benefit’:ti,ab,kw OR ‘cost-benefit analys*’:ti,ab,kw OR cba:ti,ab,kw OR (cost:ti,ab,kw AND utility:ti,ab,kw) OR ‘cost utility’:ti,ab,kw OR ‘cost-utility analys*’:ti,ab,kw OR cua:ti,ab,kw OR ‘incremental cost effectiveness ratio’:ti,ab,kw OR ‘incremental cost-effectiveness ratio’:ti,ab,kw OR icer:ti,ab,kw OR ‘discrete event simulation’:ti,ab,kw OR markov:ti,ab,kw OR ‘decision tree’:ti,ab,kw OR (economic:ti,ab,kw AND (model*:ti,ab,kw OR analys*:ti,ab,kw OR evaluation:ti,ab,kw)) OR ‘health technology assessment’:ti,ab,kw OR hta:ti,ab,kw OR (health:ti,ab,kw AND economic:ti,ab,kw AND (model*:ti,ab,kw OR analys*:ti,ab,kw OR evaluation:ti,ab,kw)) OR ‘event history model’:ti,ab,kw OR microsimulation:ti,ab,kw OR ‘monte carlo’:ti,ab,kw OR ‘monte-carlo’:ti,ab,kw OR ‘patient level simulation’:ti,ab,kw OR ‘patient-level simulation’:ti,ab,kw OR ‘deterministic sensitivity analys*’:ti,ab,kw OR ‘probabilistic sensitivity analys*’:ti,ab,kw OR ‘simulation model*’:ti,ab,kw OR ‘transition probabilit*’:ti,ab,kw OR ‘tornado diagram’:ti,ab,kw |
| #3 | Combined search | #1 AND #2 |
| #4 | Filters | Limit to 2008–2023 |
| #5 | Filters | Limit to English |
| #6 | Filters | Limit to article (1067 hits) |
| Search No. | Concepts | Search String |
|---|---|---|
| #1 | Patient | TITLE-ABS-KEY (prostate OR prostatic) AND (cancer OR neoplasm OR tumor OR tumour) |
| #2 | Outcome | TITLE-ABS-KEY ((cost AND effectiveness) OR cost-effectiveness OR “cost-effectiveness analys*” OR cea OR (cost AND benefit) OR cost-benefit OR “cost-benefit analys*” OR cba OR (cost AND utility) OR cost-utility OR “cost-utility analys*” OR cua OR “incremental cost effectiveness ratio” OR “incremental cost-effectiveness ratio” OR icer OR “discrete event simulation” OR markov OR “decision tree” OR (economic AND (model* OR analys* OR evaluation)) OR “health technology assessment” OR hta OR ((health AND economic) AND (model* OR analys* OR evaluation)) OR “event history model” OR microsimulation OR “Monte Carlo” OR “Monte-Carlo” OR “patient level simulation” OR “patient-level simulation” OR “deterministic sensitivity analys*” OR “probabilistic sensitivity analys*” OR “simulation model*” OR “transition probabilit*” OR “Tornado diagram”) |
| #3 | Combined search | #1 AND #2 |
| #4 | Filters | Limit to 2008–2024 |
| #5 | Filters | Limit to English |
| #6 | Filters | Limit to subject area: medicine |
| #7 | Filters | Limit to article (2877 hits) |
| Grey Literature Sources |
|---|
|
Appendix B
| Type of bias | Issues addressed | Iannazzo, 2011 [24] | Hird, 2020 [25] | Lester-Coll, 2021 [26] | |||
| Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | ||
| PART A. Overall checklist for bias in economic evaluation | |||||||
| Narrow perspective bias | Was a societal perspective adopted? If not, has a different perspective been justified? | Yes | Italian National Health Service perspective | Yes | healthcare payer perspective | Yes | US payer perspective |
| Inefficient comparator bias | Was the best alternative chosen as comparator? Was current practice chosen as a comparator? Have all comparators been described in sufficient detail? | Yes | Yes | Yes | |||
| Cost measurement omission bias | Were all costs relevant to the disease and intervention identified and considered? | Yes | Yes | Yes | |||
| Intermittent data collection bias | Was the resource use measured continuously? | Yes | Yes | partly | |||
| Invalid valuation bias | Is the price calculation presented in a detailed manner? Have reference prices been used? | Yes | Yes | Yes | |||
| Ordinal ICER bias | Have cardinal scales for the outcomes measure in a CEA been used? | Yes | Yes | cost/QALY | Yes | cost/QALY | |
| Double-counting bias | Are variables adequately checked for double-counting? | Yes | Yes | ||||
| Inappropriate discounting bias | Have discounting rates from guidelines been applied? | Yes | 3.50% | Yes | 1.50% | Yes | 3% |
| Limited sensitivity analysis bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered in sufficient detail? | Partly | PSA | partly | One-way sensitivity analyses | Yes | PSA, DSA, scenarios |
| Sponsor bias | Have sponsorships been disclosed? Is the study protocol freely accessible? | Partly | partly | Unclear | |||
| Reporting and dissemination bias | Has the study/trial been listed in a trial register? Have all results been reported according to the study protocol? | Unclear | Unclear | Unclear | |||
| PART B. Model-specific aspects of bias in economic evaluation | |||||||
| I Bias related to structure | |||||||
| Structural assumptions bias | Is the model structure in line with coherent theory? Do treatment pathways reflect the nature of disease? | Yes | Yes | Yes | |||
| No treatment comparator bias | Is there an adequate comparator, i.e., care as usual? | Yes | Yes | Yes | |||
| Wrong model bias | Is the model chosen adequate regarding the decision problem? | Yes | Yes | Yes | |||
| Limited time horizon bias | Was a lifetime horizon chosen? Were shorter time horizons adequately justified? | Yes | Yes | Lifetime | Yes | Lifetime | |
| II Bias related to data | |||||||
| Bias related to data identification | Are the methods of data identification transparent? Are all choices justified adequately? Do the input parameters come from high-quality and well-designed studies? | Yes | yes | Yes | |||
| Bias related to baseline data | Are probabilities, for example, based on natural history data? Is transformation of rates into transition probabilities done accurately? | Unclear | yes | Yes | |||
| Bias related to treatment effects | Are relative treatment effects synthesized using appropriate meta-analytic techniques? Are extrapolations documented and well justified? Are alternative assumptions explored regarding extrapolation? | Yes | partly | Yes | |||
| Bias related to quality-of-life weights (utilities) | Are the utilities incorporated appropriate for the specific decision problem? | N/A | LYG used, not QALY | Yes | Yes | ||
| Non-transparent data incorporation bias | Is the process of data incorporation transparent? Are all data and their sources described in detail? | Yes | yes | Yes | |||
| Limited scope bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered? | Partly | partly | Yes | |||
| III Bias related to consistency | |||||||
| Bias related to internal consistency | Has internal consistency in terms of mathematical logic been evaluated? | Unclear | yes | Yes | |||
| Type of bias | Issues addressed | Lu, 2012 [27] | |
| Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | ||
| PART A. Overall checklist for bias in economic evaluation | |||
| Narrow perspective bias | Was a societal perspective adopted? If not, has a different perspective been justified? | Yes | UK NHS perspective |
| Inefficient comparator bias | Was the best alternative chosen as a comparator? Was current practice chosen as a comparator? Have all comparators been described in sufficient detail? | Yes | |
| Cost measurement omission bias | Were all costs relevant to the disease and intervention identified and considered? | Yes | |
| Intermittent data collection bias | Was the resource use measured continuously? | Yes | |
| Invalid valuation bias | Is the price calculation presented in a detailed manner? Have reference prices been used? | Yes | |
| Ordinal ICER bias | Have cardinal scales for the outcome measure in a CEA been used? | Yes | cost/QALY |
| Double-counting bias | Are variables adequately checked for double-counting? | Yes | |
| Inappropriate discounting bias | Have discounting rates from guidelines been applied? | Yes | 3.50% |
| Limited sensitivity analysis bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered in sufficient detail? | Yes | PSA and DSA done |
| Sponsor bias | Have sponsorships been disclosed? Is the study protocol freely accessible? | partly | |
| Reporting and dissemination bias | Has the study/trial been listed in a trial register? Have all results been reported according to the study protocol? | Unclear | |
| PART B. Model-specific aspects of bias in economic evaluation | |||
| I Bias related to structure | |||
| Structural assumptions bias | Is the model structure in line with coherent theory? Do treatment pathways reflect the nature of disease? | Yes | |
| No treatment comparator bias | Is there an adequate comparator, i.e., care as usual? | Yes | |
| Wrong model bias | Is the model chosen adequate regarding the decision problem? | Yes | |
| Limited time horizon bias | Was a lifetime horizon chosen? Were shorter time horizons adequately justified? | Yes | 10 years |
| II Bias related to data | |||
| Bias related to data identification | Are the methods of data identification transparent? Are all choices justified adequately? Do the input parameters come from high-quality and well-designed studies? | Partly | |
| Bias related to baseline data | Are probabilities, for example, based on natural history data? Is transformation of rates into transition probabilities done accurately? | Yes | |
| Bias related to treatment effects | Are relative treatment effects synthesized using appropriate meta-analytic techniques? Are extrapolations documented and well justified? Are alternative assumptions explored regarding extrapolation? | Partly | |
| Bias related to quality-of-life weights (utilities) | Are the utilities incorporated appropriate for the specific decision problem? | Yes | |
| Non-transparent data incorporation bias | Is the process of data incorporation transparent? Are all data and their sources described in detail? | Yes | |
| Limited scope bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered? | Yes | |
| III Bias related to consistency | |||
| Bias related to internal consistency | Has internal consistency in terms of mathematical logic been evaluated? | Unclear | |
| Type of bias | Issues addressed | Barbier, 2022 [28] | Pelloux-Prayer, 2021 [33] | Ramamurthy, 2019 [34] | Saad, 2022 [35] | Sathianathen, 2019 [36] | |||||
| Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | ||
| PART A. Overall checklist for bias in economic evaluation | |||||||||||
| Narrow perspective bias | Was a societal perspective adopted? If not, has a different perspective been justified? | Yes | Payer perspective | Yes | French public healthcare system perspective | Yes | US payer perspective | Yes | Canadian public payer perspective | Yes | US payer perspective |
| Inefficient comparator bias | Was the best alternative chosen as a comparator? Was current practice chosen as a comparator? Have all comparators been described in sufficient detail? | Yes | Yes | Yes | Yes | Yes | |||||
| Cost measurement omission bias | Were all costs relevant to the disease and intervention identified and considered? | Yes | Yes | Yes | Yes | Yes | |||||
| Intermittent data collection bias | Was the resource use measured continuously? | Yes | Yes | Unclear | Yes | Unclear | |||||
| Invalid valuation bias | Is the price calculation presented in a detailed manner? Have reference prices been used? | Yes | Yes | Partly | Yes | Yes | |||||
| Ordinal ICER bias | Have cardinal scales for the outcome measure in a CEA been used? | Yes | cost/QALY | Yes | Yes | Yes | Yes | ||||
| Double-counting bias | Are variables adequately checked for double-counting? | Yes | Yes | Yes | Yes | Unclear | |||||
| Inappropriate discounting bias | Have discounting rates from guidelines been applied? | Yes | 3% | Yes | 2.50% | No | Yes | 1.50% | Yes | 3% | |
| Limited sensitivity analysis bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered in sufficient detail? | Yes | PSA, DSA, many scenarios | Partly | DSA | Yes | PSA, DSA, and scenario analysis | Partly | PSA and scenario analysis | Yes | PSA, DSA, and scenario analysis |
| Sponsor bias | Have sponsorships been disclosed? Is the study protocol freely accessible? | partly | No | No | Partly | Partly | |||||
| Reporting and dissemination bias | Has the study/trial been listed in a trial register? Have all results been reported according to the study protocol? | Unclear | Unclear | Unclear | Unclear | Unclear | |||||
| PART B. Model-specific aspects of bias in economic evaluation | |||||||||||
| I Bias related to structure | |||||||||||
| Structural assumptions bias | Is the model structure in line with coherent theory? Do treatment pathways reflect the nature of disease? | Yes | Yes | Yes | Yes | Yes | |||||
| No treatment comparator bias | Is there an adequate comparator, i.e., care as usual? | Yes | Yes | Yes | Yes | Yes | |||||
| Wrong model bias | Is the model chosen adequate regarding the decision problem? | Yes | Yes | Yes | Yes | Yes | |||||
| Limited time horizon bias | Was a lifetime horizon chosen? Were shorter time horizons adequately justified? | Yes | 30 years | Yes | Partly | 3 years | Yes | 15 years | Yes | Lifetime | |
| II Bias related to data | |||||||||||
| Bias related to data identification | Are the methods of data identification transparent? Are all choices justified adequately? Do the input parameters come from high-quality and well-designed studies? | Yes | Yes | Yes | Yes | Yes | |||||
| Bias related to baseline data | Are probabilities, for example, based on natural history data? Is transformation of rates into transition probabilities done accurately? | Yes | Yes | Yes | Yes | Yes | |||||
| Bias related to treatment effects | Are relative treatment effects synthesized using appropriate meta-analytic techniques? Are extrapolations documented and well justified? Are alternative assumptions explored regarding extrapolation? | Yes | Yes | Yes | Yes | Yes | |||||
| Bias related to quality of life weights (utilities) | Are the utilities incorporated appropriate for the specific decision problem? | Yes | N/A | Life years used, not QALY | Yes | Yes | Yes | ||||
| Non-transparent data incorporation bias | Is the process of data incorporation transparent? Are all data and their sources described in detail? | Yes | Yes | Yes | Yes | Yes | |||||
| Limited scope bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered? | Yes | Partly | Yes | Partly | Yes | |||||
| III Bias related to consistency | |||||||||||
| Bias related to internal consistency | Has internal consistency in terms of mathematical logic been evaluated? | Unclear | Unclear | Unclear | Unclear | Unclear | |||||
| Type of bias | Issues addressed | Sung, 2021 [37] | Wang, 2022 [39] | Yoo, 2023 [38] | Zhang, 2021 [40] | ||||||
| Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | ||||
| PART A. Overall checklist for bias in economic evaluation | |||||||||||
| Narrow perspective bias | Was a societal perspective adopted? If not, has a different perspective been justified? | Yes | US payer perspective | Yes | US payer perspective | Yes | US public (Veterans Affairs) payer perspective | Yes | from the US and Chinese payers’ perspectives | ||
| Inefficient comparator bias | Was the best alternative chosen as a comparator? Was current practice chosen as a comparator? Have all comparators been described in sufficient detail? | Yes | Yes | Yes | Yes | ||||||
| Cost measurement omission bias | Were all costs relevant to the disease and intervention identified and considered? | Yes | Yes | Yes | Yes | ||||||
| Intermittent data collection bias | Was the resource use measured continuously? | Unclear | Unclear | Unclear | Unclear | ||||||
| Invalid valuation bias | Is the price calculation presented in a detailed manner? Have reference prices been used? | Yes | Yes | Yes | Yes | ||||||
| Ordinal ICER bias | Have cardinal scales for the outcome measure in a CEA been used? | Yes | Yes | Yes | Yes | ||||||
| Double-counting bias | Are variables adequately checked for double-counting? | Yes | Yes | Yes | unclear | ||||||
| Inappropriate discounting bias | Have discounting rates from guidelines been applied? | Yes | 3% | Yes | 3% | Yes | 3% | Yes | 3% for China and 3.5% for US | ||
| Limited sensitivity analysis bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered in sufficient detail? | Yes | PSA, DSA, and scenario analysis | Yes | PSA and DSA | Partly | PSA and DSA | Partly | PSA and DSA done | ||
| Sponsor bias | Have sponsorships been disclosed? Is the study protocol freely accessible? | No | Partly | Partly | Partly | ||||||
| Reporting and dissemination bias | Has the study/trial been listed in a trial register? Have all results been reported according to the study protocol? | Unclear | Unclear | Unclear | Unclear | ||||||
| PART B. Model-specific aspects of bias in economic evaluation | |||||||||||
| I Bias related to structure | |||||||||||
| Structural assumptions bias | Is the model structure in line with coherent theory? Do treatment pathways reflect the nature of disease? | Yes | Yes | Yes | Yes | ||||||
| No treatment comparator bias | Is there an adequate comparator, i.e., care as usual? | Yes | Yes | Yes | Yes | ||||||
| Wrong model bias | Is the model chosen adequate regarding the decision problem? | Yes | Yes | Yes | Yes | ||||||
| Limited time horizon bias | Was a lifetime horizon chosen? Were shorter time horizons adequately justified? | Yes | Lifetime | Yes | Lifetime | Yes | 10 years | Yes | 20 years | ||
| II Bias related to data | |||||||||||
| Bias related to data identification | Are the methods of data identification transparent? Are all choices justified adequately? Do the input parameters come from high-quality and well-designed studies? | Yes | Yes | Yes | Yes | ||||||
| Bias related to baseline data | Are probabilities, for example, based on natural history data? Is transformation of rates into transition probabilities done accurately? | Yes | Yes | Yes | Yes | ||||||
| Bias related to treatment effects | Are relative treatment effects synthesized using appropriate meta-analytic techniques? Are extrapolations documented and well justified? Are alternative assumptions explored regarding extrapolation? | Yes | Yes | Yes | Yes | ||||||
| Bias related to quality-of-life weights (utilities) | Are the utilities incorporated appropriate for the specific decision problem? | Yes | Yes | Yes | Yes | ||||||
| Non-transparent data incorporation bias | Is the process of data incorporation transparent? Are all data and their sources described in detail? | Yes | Yes | Yes | Yes | ||||||
| Limited scope bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered? | Yes | Partly | Partly | Partly | ||||||
| III Bias related to consistency | |||||||||||
| Bias related to internal consistency | Has internal consistency in terms of mathematical logic been evaluated? | Unclear | Yes | Unclear | Unclear | ||||||
| Type of bias | Issues addressed | Beca, 2019 [29] | Bleser, 2020 [30] | Parikh, 2020 [31] | Parmar, 2021 [32] | ||||||
| Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | Relevant to study Yes/No/Partly/Unclear/NA | How did you deal with this bias? (description of strategy and rationale) | ||||
| PART A. Overall checklist for bias in economic evaluation | |||||||||||
| Narrow perspective bias | Was a societal perspective adopted? If not, has a different perspective been justified? | Yes | Canadian public payer perspective | Yes | Health care system (NHI & patient co-payment) | Yes | US payer | Yes | Health care system | ||
| Inefficient comparator bias | Was the best alternative chosen as a comparator? Was current practice chosen as a comparator? Have all comparators been described in sufficient detail? | Yes | Yes | Yes | Yes | ||||||
| Cost measurement omission bias | Were all costs relevant to the disease and intervention identified and considered? | Yes | Yes | Yes | Yes | ||||||
| Intermittent data collection bias | Was the resource use measured continuously? | Yes | Yes | Yes | Yes | ||||||
| Invalid valuation bias | Is the price calculation presented in a detailed manner? Have reference prices been used? | Yes | Yes | Yes | Yes | ||||||
| Ordinal ICER bias | Have cardinal scales for the outcome measure in a CEA been used? | Yes | cost/QALY; cost/LYG | Yes | cost/QALY | Yes | QALY (net monetary benefit values) | Yes | QALY, LYG | ||
| Double-counting bias | Are variables adequately checked for double-counting? | Yes | Partly | Yes | Yes | ||||||
| Inappropriate discounting bias | Have discounting rates from guidelines been applied? | Yes | 1.50% | Yes | 3% (cost) and 1.5% (benefits) | Yes | 3% | Yes | 1.50% | ||
| Limited sensitivity analysis bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered in sufficient detail? | Partly | One-way sensitivity analysis | Yes | PSA, DSA, scenarios | Yes | PSA and DSA done | Partly | Scenarios | ||
| Sponsor bias | Have sponsorships been disclosed? Is the study protocol freely accessible? | No | Partly | Unclear | Unclear | ||||||
| Reporting and dissemination bias | Has the study/trial been listed in a trial register? Have all results been reported according to the study protocol? | Unclear | Unclear | Unclear | Unclear | ||||||
| PART B. Model-specific aspects of bias in economic evaluation | |||||||||||
| I Bias related to structure | |||||||||||
| Structural assumptions bias | Is the model structure in line with coherent theory? Do treatment pathways reflect the nature of disease? | Yes | Yes | Yes | Yes | ||||||
| No treatment comparator bias | Is there an adequate comparator, i.e., care as usual? | Yes | Yes | Yes | Yes | ||||||
| Wrong model bias | Is the model chosen adequate regarding the decision problem? | Yes | Yes | Yes | Yes | ||||||
| Limited time horizon bias | Was a lifetime horizon chosen? Were shorter time horizons adequately justified? | Yes | 15 years | Partly | 5 years | Yes | 10 years | Yes | Lifetime | ||
| II Bias related to data | |||||||||||
| Bias related to data identification | Are the methods of data identification transparent? Are all choices justified adequately? Do the input parameters come from high-quality and well-designed studies? | Yes | Partly | Yes | Yes | ||||||
| Bias related to baseline data | Are probabilities, for example, based on natural history data? Is transformation of rates into transition probabilities done accurately? | Yes | Yes | Yes | Yes | ||||||
| Bias related to treatment effects | Are relative treatment effects synthesized using appropriate meta-analytic techniques? Are extrapolations documented and well justified? Are alternative assumptions explored regarding extrapolation? | Yes | Partly | Yes | Yes | ||||||
| Bias related to quality-of-life weights (utilities) | Are the utilities incorporated appropriate for the specific decision problem? | Yes | Yes | Yes | Yes | ||||||
| Non-transparent data incorporation bias | Is the process of data incorporation transparent? Are all data and their sources described in detail? | Yes | Yes | Yes | Yes | ||||||
| Limited scope bias | Have the four principles of uncertainty (methodological, structural, heterogeneity, and parameter) been considered? | Partly | Yes | Yes | Partly | ||||||
| III Bias related to consistency | |||||||||||
| Bias related to internal consistency | Has internal consistency in terms of mathematical logic been evaluated? | Unclear | Unclear | Unclear | Unclear | ||||||
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J. Clin. 2025, 75, 10. [Google Scholar] [CrossRef] [PubMed]
- European Cancer Information System. Cancer Statistics. 2022. Available online: https://ecis.jrc.ec.europa.eu/en (accessed on 22 October 2024).
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G.; Tombal, B.; Gillessen, S. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; et al. Prostate cancer, version 4.2023, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Cancer Netw. 2023, 21, 1067–1096. [Google Scholar] [CrossRef] [PubMed]
- Blas, L.; Shiota, M.; Eto, M. Current status and future perspective on the management of metastatic castration-sensitive prostate cancer. Cancer Treat. Res. Commun. 2022, 32, 100606. [Google Scholar] [CrossRef] [PubMed]
- Wala, J.; Nguyen, P.; Pomerantz, M. Early treatment intensification in metastatic hormone-sensitive prostate cancer. J. Clin. Oncol. 2023, 41, 3584–3590. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.; O’Brien, J.; Medhurst, E.; Lawrentschuk, N.; Murphy, D.; Azad, A. Current treatment options for newly diagnosed metastatic hormone-sensitive prostate cancer—A narrative review. Transl. Androl. Urol. 2021, 10, 3918. [Google Scholar] [CrossRef] [PubMed]
- Olsen, T.A.; Filson, C.P.; Richards, T.B.; Ekwueme, D.U.; Howard, D.H. The cost of metastatic prostate cancer in the United States. Urol. Pr. 2023, 10, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Bodrogi, J.; Kaló, Z. Principles of pharmacoeconomics and their impact on strategic imperatives of pharmaceutical research and development. Br. J. Pharmacol. 2010, 159, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Lorenzovici, L.; Szilberhorn, L.; Farkas-Raduly, S.; Gasparik, A.I.; Precup, A.M.; Nagy, A.G.; Niemann, C.U.; Aittokallio, T.; Kaló, Z.; Csanadi, M. Systematic literature review of economic evaluations of treatment alternatives in chronic lymphocytic leukemia. BioDrugs 2023, 37, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Chan, V.K.Y.; Yang, R.; Wong, I.C.K.; Li, X. Cost-effectiveness of poly ADP-ribose polymerase inhibitors in cancer treatment: A systematic review. Front. Pharmacol. 2022, 13, 891149. [Google Scholar] [CrossRef] [PubMed]
- Grochtdreis, T.; König, H.H.; Dobruschkin, A.; von Amsberg, G.; Dams, J. Cost-effectiveness analyses and cost analyses in castration-resistant prostate cancer: A systematic review. PLoS ONE 2018, 13, e0208063. [Google Scholar] [CrossRef] [PubMed]
- Butala, A.A.; Huang, C.C.; Bryant, C.M.; Henderson, R.H.; Hoppe, B.S.; Mendenhall, N.P.; Vapiwala, N.; Vega, R.B.M. Heterogeneity in Radiotherapeutic Parameter Assumptions in Cost-Effectiveness Analyses in Prostate Cancer: A Call for Uniformity. Value Health 2022, 25, 171–177. [Google Scholar] [CrossRef] [PubMed]
- Moussa, M.; Papatsoris, A.; Sryropoulou, D.; Chakra, M.A.; Dellis, A.; Tzelves, L. A pharmacoeconomic evaluation of pharmaceutical treatment options for prostate cancer. Expert. Opin. Pharmacother. 2021, 22, 1685–1728. [Google Scholar] [CrossRef] [PubMed]
- Norum, J.; Nieder, C. Treatments for metastatic prostate cancer (mPC): A review of costing evidence. Pharmacoeconomics 2017, 35, 1223–1236. [Google Scholar] [CrossRef] [PubMed]
- Hatoum, H.T.; Crawford, E.D.; Nielsen, S.K.; Lin, S.-J.; Marshall, D.C. Review of the economic evaluations of hormonal therapy for patients with locally advanced prostate cancer. Expert. Rev. Pharmacoecon. Outcomes Res. 2013, 13, 251–259. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.A.; Joshi, A.D.; Kaura, S.; Botteman, M.F. Pharmacoeconomics of bisphosphonates for skeletal-related event prevention in metastatic non-breast solid tumours. Pharmacoeconomics 2012, 30, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Pelloux-Prayer, R.; Bataillard, T.; Thiery-Vuillemin, A.; Vincent, A.; Fagnoni, P.; Nerich, V. Treatment of Patients with Metastatic Hormone-Sensitive Prostate Cancer: A Systematic Review of Economic Evaluations. Clin. Genitourin. Cancer 2022, 20, 594–602. [Google Scholar] [CrossRef] [PubMed]
- Yanev, I.; Gatete, J.; Aprikian, A.G.; Guertin, J.R.; Dragomir, A. The Health Economics of Metastatic Hormone-Sensitive and Non-Metastatic Castration-Resistant Prostate Cancer—A Systematic Literature Review with Application to the Canadian Context. Curr. Oncol. 2022, 29, 3393–3424. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Adarkwah, C.C.; van Gils, P.F.; Hiligsmann, M.; Evers, S.M. Risk of bias in model-based economic evaluations: The ECOBIAS checklist. Expert. Rev. Pharmacoecon. Outcomes Res. 2016, 16, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Iannazzo, S.; Pradelli, L.; Carsi, M.; Perachino, M. Cost-effectiveness analysis of LHRH agonists in the treatment of metastatic prostate cancer in Italy. Value Health 2011, 14, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Hird, A.E.; Magee, D.E.; Cheung, D.C.; Matta, R.; Kulkarni, G.S.; Nam, R.K. Abiraterone vs. docetaxel for metastatic hormone-sensitive prostate cancer: A microsimulation model. J. Assoc. Med. Microbiol. Infect Dis. Can. 2020, 14, E418–E427. [Google Scholar] [CrossRef] [PubMed]
- Lester-Coll, N.H.; Ades, S.; Yu, J.B.; Atherly, A.; Wallace, H.J., 3rd; Sprague, B.L. Cost-effectiveness of Prostate Radiation Therapy for Men With Newly Diagnosed Low-Burden Metastatic Prostate Cancer. JAMA Netw. Open 2021, 4, e2033787. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Peters, J.; Roome, C.; Stein, K. Cost-effectiveness analysis of degarelix for advanced hormone-dependent prostate cancer. BJU Int. 2012, 109, 1183–1192. [Google Scholar] [CrossRef] [PubMed]
- Barbier, M.C.; Tomonaga, Y.; Menges, D.; Yebyo, H.G.; Haile, S.R.; Puhan, M.A.; Schwenkglenks, M. Survival modelling and cost-effectiveness analysis of treatments for newly diagnosed metastatic hormone-sensitive prostate cancer. PLoS ONE 2022, 17, e0277282. [Google Scholar] [CrossRef] [PubMed]
- Beca, J.; Majeed, H.; Chan, K.K.W.; Hotte, S.J.; Loblaw, A.; Hoch, J.S. Cost-effectiveness of docetaxel in high-volume hormone-sensitive metastatic prostate cancer. J. Assoc. Med. Microbiol. Infect Dis. Can. 2019, 13, 396–403. [Google Scholar] [CrossRef] [PubMed]
- De Bleser, E.; Willems, R.; Decaestecker, K.; Annemans, L.; De Bruycker, A.; Fonteyne, V.; Lumen, N.; Ameye, F.; Billiet, I.; Joniau, S.; et al. A Trial-Based Cost-Utility Analysis of Metastasis-Directed Therapy for Oligorecurrent Prostate Cancer. Cancers 2020, 12, 132. [Google Scholar] [CrossRef] [PubMed]
- Parikh, N.R.; Chang, E.M.; Nickols, N.G.; Rettig, M.B.; Raldow, A.C.; Steinberg, M.L.; Koontz, B.F.; Vapiwala, N.; Deville, C.; Feng, F.Y.; et al. Cost-Effectiveness of Metastasis-Directed Therapy in Oligorecurrent Hormone-Sensitive Prostate Cancer. Int. J. Radiat. Oncol. 2020, 108, 917–926. [Google Scholar] [CrossRef] [PubMed]
- Parmar, A.; Timilshina, N.; Emmenegger, U.; Smoragiewicz, M.; Sander, B.; Alibhai, S.; Chan, K.K.W. A cost-utility analysis of apalutamide for metastatic castration-sensitive prostate cancer. J. Assoc. Med. Microbiol. Infect Dis. Can. 2022, 16, E126–E131. [Google Scholar] [CrossRef] [PubMed]
- Pelloux-Prayer, R.; Schiele, P.; Oudard, S.; Gravis, G.; Kleinclauss, F.; Crehange, G.; Hennequin, C.; Morgans, A.K.; Geoffrois, L.; Limat, S.; et al. Cost-effectiveness Analysis of Innovative Therapy for Patients with Newly Diagnosed Hormone-Sensitive Metastatic Prostate Cancer. Clin. Genitourin. Cancer 2021, 19, e326–e333. [Google Scholar] [CrossRef] [PubMed]
- Ramamurthy, C.; Handorf, E.A.; Correa, A.F.; Beck, J.R.; Geynisman, D.M. Cost-effectiveness of abiraterone versus docetaxel in the treatment of metastatic hormone naïve prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2019, 37, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Saad, F.; Chilelli, A.; Hui, B.; Muratov, S.; Ganguli, A.; North, S.; Shayegan, B. Cost-effectiveness of enzalutamide versus apalutamide versus androgen deprivation therapy alone for the treatment of metastatic castration-sensitive prostate cancer in Canada. J. Med. Econ. 2022, 25, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Sathianathen, N.J.; Alarid-Escudero, F.; Kuntz, K.M.; Lawrentschuk, N.; Bolton, D.M.; Murphy, D.G.; Kim, S.P.; Konety, B.R. A cost-effectiveness analysis of systemic therapy for metastatic hormone-sensitive prostate cancer. Eur. Urol. Oncol. 2019, 2, 649–655. [Google Scholar] [CrossRef] [PubMed]
- Sung, W.W.; Choi, H.C.; Luk, P.H.; So, T.H. A cost-effectiveness analysis of systemic therapy for metastatic hormone-sensitive prostate cancer. Front. Oncol. 2021, 11, 627083. [Google Scholar] [CrossRef] [PubMed]
- Yoo, M.; Nelson, R.E.; Haaland, B.; Dougherty, M.; Cutshall, Z.A.; Kohli, R.; Beckstead, R.; Kohli, M. Cost-effectiveness analysis of 7 treatments in metastatic hormone-sensitive prostate cancer: A public-payer perspective. J. Natl. Cancer Inst. 2023, 115, 1374–1382. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Hong, H.; Alexander, G.C.; Brawley, O.W.; Paller, C.J.; Ballreich, J. Cost-Effectiveness of Systemic Treatments for Metastatic Castration-Sensitive Prostate Cancer: An Economic Evaluation Based on Network Meta-Analysis. Value Health J. Int. Soc. Pharmacoecon. Outcomes Res. 2022, 25, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Zhang, P.-F.; Xie, D.; Li, Q. Adding Enzalutamide to First-Line Treatment for Metastatic Hormone-Sensitive Prostate Cancer: A Cost-Effectiveness Analysis. Front. Public. Heal 2021, 9, 608375. [Google Scholar] [CrossRef] [PubMed]
- de Paredes Esteban, J.C.G.; Del Rey, E.J.A.; Díez, R.A. Docetaxel in hormone-sensitive advanced prostate cancer; GENESIS-SEFH evaluation reporta. Farm. Hosp. 2017, 41, 550–558. [Google Scholar] [CrossRef]
- Katta, A.; Hansen, R.N. EE47 Cost-Effectiveness of Abiraterone, Enzalutamide, and Apalutamide in Metastatic CaFstration-Sensitive Prostate Cancer (MCSPC): A Partitioned-Survival Model. Value Health 2023, 26, S68. [Google Scholar] [CrossRef]
- Madani, O. HTA157 Reflection on Medicines That Have Recently Come Off Patent and Have Been Rejected by NICE in the Past 20 Years: A Case Study of Abiraterone for Treating Newly Diagnosed Metastatic Hormone Sensitive Prostate Cancer (MHSPC). Value Health 2023, 26, S349. [Google Scholar] [CrossRef]
- Nwogu, I.B.; Nedzesky, J.; Carlson, J.J. EE261 Cost-Effectiveness of Adding Darolutamide to Docetaxel and Androgen Deprivation Therapy in the Treatment of Metastatic Hormone-Sensitive Prostrate Cancer. Value Health 2023, 26, S106. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence (NICE). Darolutamide with Androgen Deprivation Therapy and Docetaxel for Treating Hormone-Sensitive Metastatic Prostate Cancer [TA903]. 2023. Available online: https://www.nice.org.uk/guidance/ta903 (accessed on 2 May 2024).
- National Institute for Health and Care Excellence (NICE). Apalutamide with Androgen Deprivation Therapy for Treating Hormone-Sensitive Metastatic Prostate Cancer [TA741]. 2021. Available online: https://www.nice.org.uk/guidance/ta741 (accessed on 2 May 2024).
- National Institute for Health and Care Excellence (NICE). Abiraterone for Treating Newly Diagnosed High-Risk Hormone-Sensitive Metastatic Prostate Cancer (TA721). 2021. (Updated: 18 August 2021). Available online: https://www.nice.org.uk/guidance/ta721 (accessed on 2 May 2024).
- National Institute for Health and Care Excellence (NICE). Enzalutamide for Treating Hormone-Sensitive Metastatic Prostate Cancer [TA712]. 2021. Available online: https://www.nice.org.uk/guidance/ta712 (accessed on 2 May 2024).
- Canadian Agency for Drugs & Technologies in Health (CADTH). Darolutamide. 2023. Available online: https://www.cadth.ca/darolutamide (accessed on 2 May 2024).
- Canadian Agency for Drugs & Technologies in Health (CADTH). Enzalutamide (Xtandi) for Metastatic Castration Sensitive Prostate Cancer—Details. 2020. Available online: https://www.cadth.ca/enzalutamide-xtandi-metastatic-castration-sensitive-prostate-cancer-details (accessed on 2 May 2024).
- Canadian Agency for Drugs & Technologies in Health (CADTH). Apalutamide (Erleada) for Metastatic Castration-Sensitive Prostate Cancer—Details. 2019. Available online: https://www.cadth.ca/apalutamide-erleada-metastatic-castration-sensitive-prostate-cancer-details (accessed on 2 May 2024).
- Niraula, S.; Le, L.W.; Tannock, I.F. Treatment of prostate cancer with intermittent versus continuous androgen deprivation: A systematic review of randomized trials. J. Clin. Oncol. 2013, 31, 2029–2036. [Google Scholar] [CrossRef] [PubMed]
- Grisay, G.; Turco, F.; Litiere, S.; Fournier, B.; Patrikidou, A.; Gallardo, E.; McDermott, R.; Alanya, A.; Gillessen, S.; Tombal, B. EORTC 2238 “De-Escalate”: A pragmatic trial to revisit intermittent androgen deprivation therapy in the era of new androgen receptor pathway inhibitors. Front. Oncol. 2024, 14, 1391825. [Google Scholar] [CrossRef] [PubMed]
- Ávila, C.; González-Montero, J.; Rojas, C.I.; Madan, R.A.; Burotto, M. Current landscape in first-line treatment of metastatic hormone sensitive prostate cancer: A cost-effectiveness focused review. Oncologist 2025, 30, oyaf095. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.T.; Ameyaw, D.; Obeng, G.D.; Amuah, R.; Józwiak-Hagymásy, J.; Dóczi, T.; Mezei, D.; Németh, B.; Tordai, A.; Alanya, A.; et al. Systematic Literature Review on Economic Evaluations and Health Economic Models in the Field of Metastatic Castration-Sensitive Prostate Cancer. In Proceedings of the Conference Poster Presented at ISPOR Europe 2024 Conference, Barcelona, Spain, 17–20 November 2024. [Google Scholar]
- Handorf, E.A.; Beck, J.R.; Correa, A.; Ramamurthy, C.; Geynisman, D.M. Cost-effectiveness analysis for therapy sequence in advanced cancer: A microsimulation approach with application to metastatic prostate cancer. Med. Decis. Mak. 2023, 43, 949–960. [Google Scholar] [CrossRef] [PubMed]
- Sathianathen, N.J.; Lawrentschuk, N.; Konety, B.; Azad, A.A.; Corcoran, N.M.; Bolton, D.M.; Murphy, D.G. Cost Effectiveness of Systemic Treatment Intensification for Metastatic Hormone-sensitive Prostate Cancer: Is Triplet Therapy Cost Effective? Eur. Urol. Oncol. 2024, 7, 870–876. [Google Scholar] [CrossRef] [PubMed]
- Kramer, K.K.; Schmidt-Hegemann, N.S.; Westhofen, T.; Foglar, M.; Ricke, J.; Westphalen, C.B.; Unterrainer, M.; Kunz, W.G.; Mehrens, D. Cost-effectiveness analysis of additional local prostate radio therapy in metastatic prostate cancer from a medicare perspective. Radiat. Oncol. 2024, 19, 167. [Google Scholar] [CrossRef] [PubMed]
| Ref. | Investigated Therapies | Modelling Approach | Study Outcome | Study Country | Time Horizon |
|---|---|---|---|---|---|
| Iannazzo, 2011 [24] |
|
| Cost/life-month gained | Italy | Lifetime |
| Hird, 2020 [25] |
|
| Cost/QALY | Canada | Lifetime |
| Lester-Coll, 2021 [26] |
|
| Cost/QALY | USA | 37 months to mirror the trial + Lifetime |
| Lu, 2012 [27] |
|
| Cost/QALY | United Kingdom | 10 years |
| Barbier, 2022 [28] |
|
| Cost/QALY | Switzerland | 30 years |
| Bleser, 2020 [30] |
|
| Cost/QALY | Belgium | 5 years |
| Parikh, 2020 [31] |
|
| Net Monetary Benefit | USA | 10 years |
| Pelloux-Prayer, 2021 [33] | Asymptomatic or mildly symptomatic patients
|
| Cost/LYG | France | Lifetime |
| Ramamurthy, 2019 [34] |
|
| Cost/progression-free quality-adjusted life years | USA | 3 years |
| Saad, 2022 [35] |
|
| Cost/QALY | Canada | 15 years |
| Sathianathen, 2019 [36] |
|
| Cost/QALY | USA | Lifetime |
| Sung, 2021 [37] |
|
| Cost/QALY | USA & China | Lifetime |
| Zhang, 2021 [40] |
|
| Cost/QALY | USA & China | 20 years |
| Beca, 2019 [29] |
|
| Cost/QALYCost/LYG | Canada | 15 years |
| Parmar, 2022 [32] |
|
| Cost/QALYCost/LYG | Canada | Lifetime |
| Yoo, 2023 [38] |
|
| Cost/QALY | USA | 10 years |
| Wang, 2022 [39] |
|
| Cost/QALY | USA | Lifetime |
| Esteban, 2017 [41] |
|
| Cost/LYG | Spain | Non-applicable |
| Ref. | Investigated Therapies | Modelling Approach | Study Outcome | Study Country | Time Horizon |
| Katta, 2023 [42] |
|
| Cost/QALY | USA | Lifetime |
| Madani, 2023 [43] |
|
| Cost/QALY | UK | Lifetime |
| Nwogu, 2023 [44] |
|
| Cost/QALY | USA | Lifetime |
| References | Investigated Therapies | Modelling Approach | Study Outcome | Time Horizon |
|---|---|---|---|---|
| TA903, 2023 [45] |
|
| Cost/QALY | Lifetime |
| TA741, 2021 [46] |
|
| Cost/QALY | Lifetime |
| TA721, 2021 [47] |
|
| Cost/QALY | 20 years |
| TA712, 2021 [48] |
|
| Cost/QALY | Lifetime |
| References | Investigated Therapies | Modelling Approach | Study Outcome | Time Horizon |
|---|---|---|---|---|
| PC0294-000 [49] |
|
| Cost/QALY | Lifetime |
| PC0209-000 [50] |
|
| Cost/QALY | 15 years |
| PC0200-000 [51] |
|
| Cost/QALY | 20 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, T.T.; Ameyaw, D.; Obeng, G.D.; Amuah, R.; Józwiak-Hagymásy, J.; Dóczi, T.; Mezei, D.; Németh, B.; Tordai, A.; Alanya, A.; et al. Systematic Literature Review on Economic Evaluations and Health Economic Models in Metastatic Castration-Sensitive Prostate Cancer. Curr. Oncol. 2025, 32, 412. https://doi.org/10.3390/curroncol32080412
Nguyen TT, Ameyaw D, Obeng GD, Amuah R, Józwiak-Hagymásy J, Dóczi T, Mezei D, Németh B, Tordai A, Alanya A, et al. Systematic Literature Review on Economic Evaluations and Health Economic Models in Metastatic Castration-Sensitive Prostate Cancer. Current Oncology. 2025; 32(8):412. https://doi.org/10.3390/curroncol32080412
Chicago/Turabian StyleNguyen, Thanh Tu, David Ameyaw, George Dennis Obeng, Rose Amuah, Judit Józwiak-Hagymásy, Tamás Dóczi, Dóra Mezei, Bertalan Németh, Attila Tordai, Ahu Alanya, and et al. 2025. "Systematic Literature Review on Economic Evaluations and Health Economic Models in Metastatic Castration-Sensitive Prostate Cancer" Current Oncology 32, no. 8: 412. https://doi.org/10.3390/curroncol32080412
APA StyleNguyen, T. T., Ameyaw, D., Obeng, G. D., Amuah, R., Józwiak-Hagymásy, J., Dóczi, T., Mezei, D., Németh, B., Tordai, A., Alanya, A., Grisay, G., & Csanádi, M. (2025). Systematic Literature Review on Economic Evaluations and Health Economic Models in Metastatic Castration-Sensitive Prostate Cancer. Current Oncology, 32(8), 412. https://doi.org/10.3390/curroncol32080412