Design and Development of a Device (Sifilotto®) for Tumour Tracking in Cervical Cancer Patients Undergoing Robotic Arm LINAC Stereotactic Body Radiation Therapy Boost: Background to the STARBACS Study

 , , ,
, , ,  , and
, and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Aims of Invention
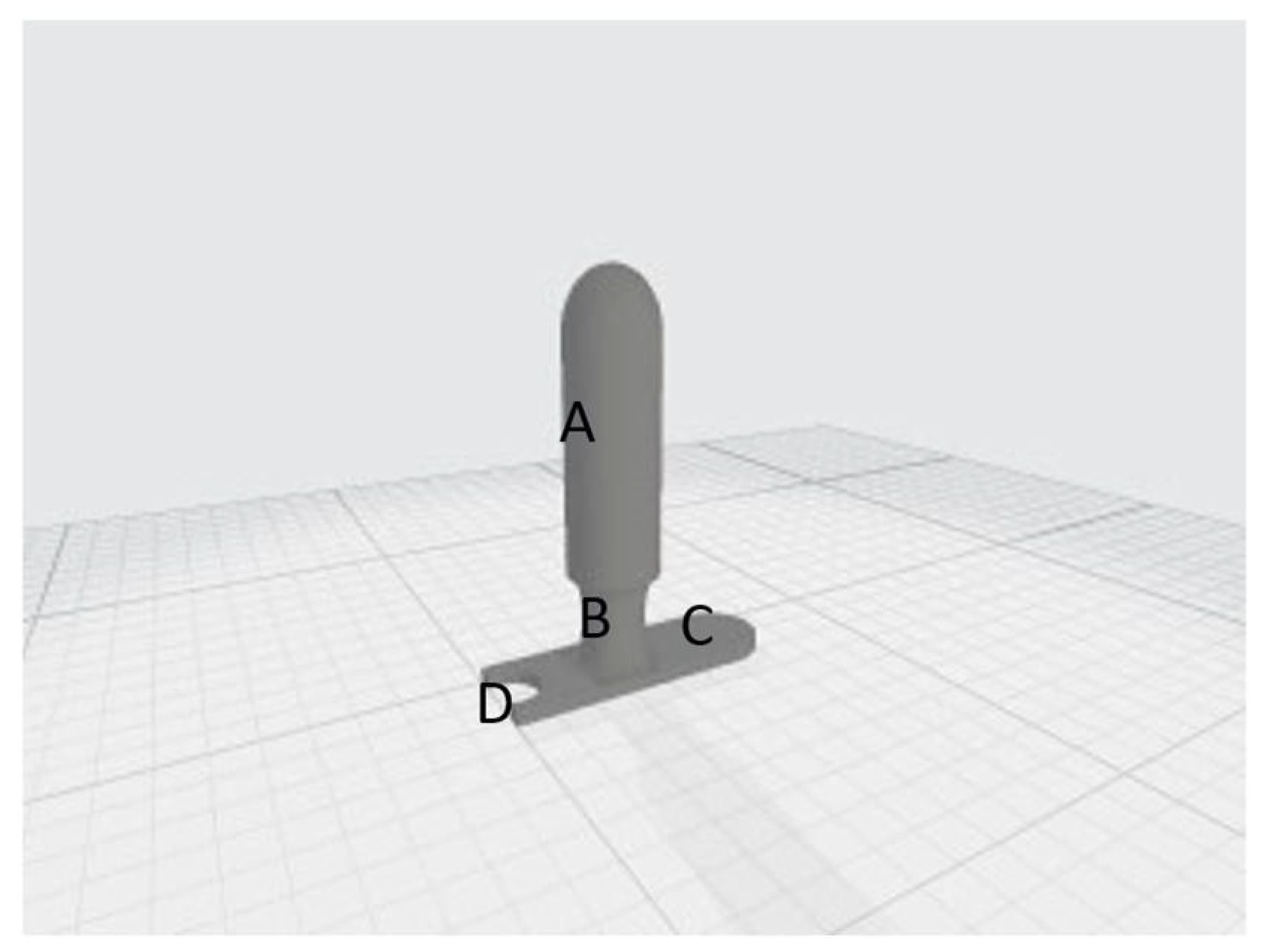
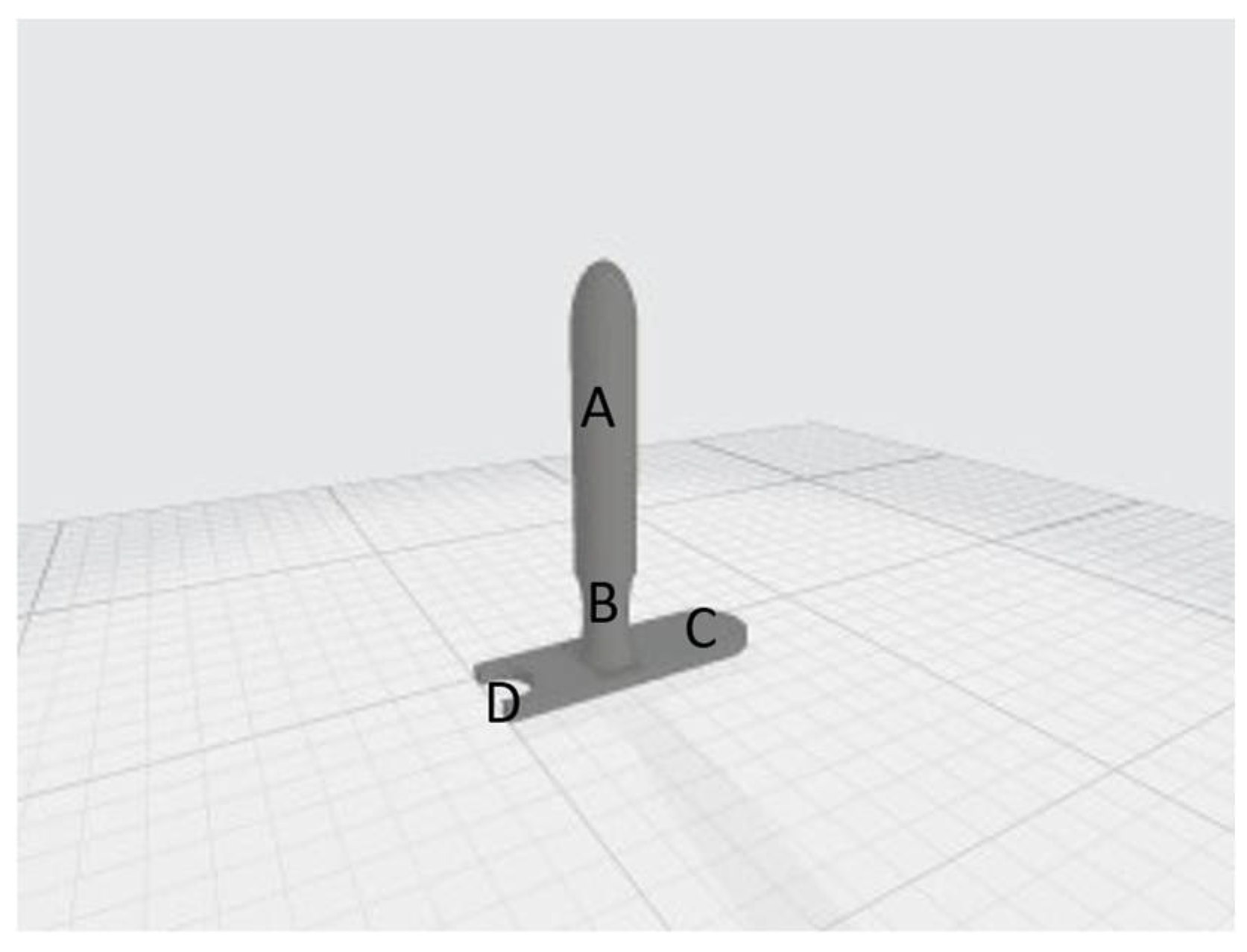
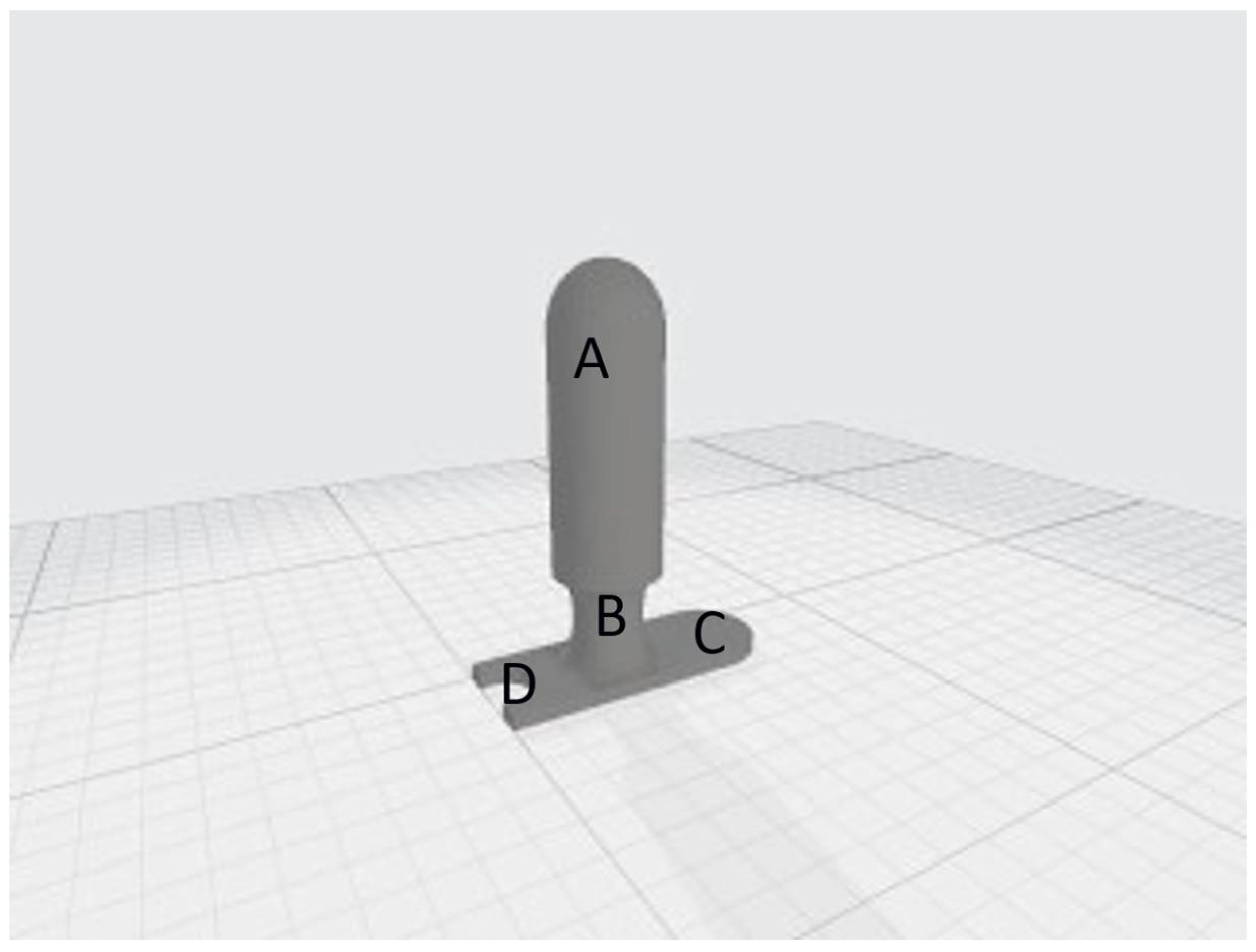
2.2. Design
- Each fiducial should be positioned at least 12 mm from the centre of the target;
- A minimum fiducial spacing of 18 mm;
- An inclination of 45° with respect to the horizontal axis of the target centre;
- An inclination of at least 15° with respect to the long axis of the fiducial.
2.3. Fabrication
3. Results
3.1. Radiological Tests
- Step 1. “CT test”: This involved the acquisition of CT simulation scans with the applicator positioned horizontally (as for endovaginal insertion) on a radiolucent solid water base and transmission of the images to the Treatment Planning System (TPS). During Step 1, the following were verified: correct insertion and positioning of the fiducials in the slots, verification of the rigid body and fiducial interval parameters. Figure 5 shows the CT images acquired and displayed on the TPS during the verification of the above parameters.
- Step 2. “x-ray imaging test”: This step includes the acquisition of verification x-ray images with the applicator positioned horizontally on a radiolucent solid water base. In Step 2, the x-ray images were acquired using two cameras located inside the bunker, on the right and left of the bed, at 190 cm from the floor and at an angle of 45° with respect to the floor. Thanks to the correspondence check with the DRR on the TPS, it was verified that the rigid body and fiducial interval parameters were correctly respected. In Step 2, it was also verified that both cameras clearly detected all four fiducials without any interference from the PLA material used in the construction. Figure 6 shows the x-ray image captured and displayed on the console monitor during the control of the parameters described above.
3.2. In Vivo Tests
4. Discussion
4.1. Robotic Arm Linear Accelerators (R-LINACs)
- Axis: Indications of translations and rotations. These are represented on the screen with arrows pointing in a positive or negative direction on icons of the human body and corresponding to the patient’s orientation in the treatment plan.
- Calculated: Deviations (in millimetres or degrees) between X-ray imaging and DRR calculated by the tracking algorithm.
- Applied: Correction movements sent to the processing machine. These values can be verified by re-acquiring the image or can be directly displayed during treatment administration in the delivery phase.
- The invasiveness of the fiducial insertion procedure;
- The risk of error in treatment reproducibility due to the migratory tendency of fiducials;
- The increase in the total treatment time due to aligning difficulties given by the intramucosal implant;
- The high costs due to the use of at least four fiducials per patient (cost of a single fiducial: EUR 55–150).
4.2. Costs Analysis
4.3. Quality Assurance
5. Conclusions
6. Patents
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| SOC | Standard Of Care |
| cCRT | concurrent ChemoRadiotherapy |
| cCIRT | concurrent ChemoImmunoRadiotherapy |
| LINAC | Linear Accelerator |
| STARBACS | STereotActic Radiotherapy Boost in locally Advanced Cervical carcinoma patientS |
| SCC | Squamous Cervical carcinoma |
| HPV | Human Papilloma Virus |
| LACC | Locally Advanced Cervical Cancer |
| ICBT | intracavitary brachytherapy |
| NACT | neoadjuvant chemotherapy |
| LC | Local control |
| EBRT | external beam radiotherapy |
| OaR | organs at risk |
| SBRT | stereotactic body radiotherapy |
| SGRT | surface guided radiation therapy |
| CT | Computed Tomography |
| DRR | Digital Reconstructed Radiography |
| MRI | Magnetic Resonance Image |
| 18-fdg-PET | 18-fluorodeoxyxglucose-positron emission tomography |
| CTV | Clinical Target Volume |
| SIB | Simultaneous integrated boost |
| CNS | Central nervous system |
| DRG | Diagnosis related group |
Appendix A

References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Lorusso, D.; Xiang, Y.; Hasegawa, K.; Scambia, G.; Leiva, M.; Ramos-Elias, P.; Acevedo, A.; Sukhin, V.; Cloven, N.; Pereira de Santana Gomes, A.J.; et al. Pembrolizumab or Placebo with Chemoradiotherapy Followed by Pembrolizumab or Placebo for Newly Diagnosed, High-Risk, Locally Advanced Cervical Cancer (ENGOT-Cx11/GOG-3047/KEYNOTE-A18): A Randomised, Double-Blind, Phase 3 Clinical Trial. Lancet Lond. Engl. 2024, 403, 1341–1350. [Google Scholar] [CrossRef]
- Tanderup, K.; Eifel, P.J.; Yashar, C.M.; Pötter, R.; Grigsby, P.W. Curative Radiation Therapy for Locally Advanced Cervical Cancer: Brachytherapy Is NOT Optional. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 537–539. [Google Scholar] [CrossRef]
- Gupta, S.; Maheshwari, A.; Parab, P.; Mahantshetty, U.; Hawaldar, R.; Sastri Chopra, S.; Kerkar, R.; Engineer, R.; Tongaonkar, H.; Ghosh, J.; et al. Neoadjuvant Chemotherapy Followed by Radical Surgery Versus Concomitant Chemotherapy and Radiotherapy in Patients With Stage IB2, IIA, or IIB Squamous Cervical Cancer: A Randomized Controlled Trial. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2018, 36, 1548–1555. [Google Scholar] [CrossRef] [PubMed]
- McCormack, M.; Eminowicz, G.; Gallardo, D.; Diez, P.; Farrelly, L.; Kent, C.; Hudson, E.; Panades, M.; Mathew, T.; Anand, A.; et al. Induction Chemotherapy Followed by Standard Chemoradiotherapy versus Standard Chemoradiotherapy Alone in Patients with Locally Advanced Cervical Cancer (GCIG INTERLACE): An International, Multicentre, Randomised Phase 3 Trial. Lancet 2024, 404, 1525–1535. [Google Scholar] [CrossRef]
- Parisi, S.; Sciacca, M.; Ferrantelli, G.; Chillari, F.; Critelli, P.; Venuti, V.; Lillo, S.; Arcieri, M.; Martinelli, C.; Pontoriero, A.; et al. Locally Advanced Squamous Cervical Carcinoma (M0): Management and Emerging Therapeutic Options in the Precision Radiotherapy Era. Jpn. J. Radiol. 2024, 42, 354–366. [Google Scholar] [CrossRef]
- Ito, K.; Kito, S.; Nakajima, Y.; Shimizuguchi, T.; Ogawa, H.; Nihei, K.; Tanaka, H.; Kino, N.; Yasugi, T.; Karasawa, K. Determining the Recommended Dose of Stereotactic Body Radiotherapy Boost in Patients with Cervical Cancer Who Are Unsuitable for Intracavitary Brachytherapy: A Phase I Dose-Escalation Study. Jpn. J. Clin. Oncol. 2019, 49, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Sun, L.; Xu, W.; Wang, Q.; Yu, S.; Sun, J. Current Advances and Future Perspectives of 3D Printing Natural-Derived Biopolymers. Carbohydr. Polym. 2019, 207, 297–316. [Google Scholar] [CrossRef]
- Chen, Q.; Mangadlao, J.D.; Wallat, J.; De Leon, A.; Pokorski, J.K.; Advincula, R.C. 3D Printing Biocompatible Polyurethane/Poly(Lactic Acid)/Graphene Oxide Nanocomposites: Anisotropic Properties. ACS Appl. Mater. Interfaces 2017, 9, 4015–4023. [Google Scholar] [CrossRef]
- Asfia, A.; Novak, J.I.; Mohammed, M.I.; Rolfe, B.; Kron, T. A Review of 3D Printed Patient Specific Immobilisation Devices in Radiotherapy. Phys. Imaging Radiat. Oncol. 2020, 13, 30–35. [Google Scholar] [CrossRef]
- Tino, R.; Leary, M.; Yeo, A.; Kyriakou, E.; Kron, T.; Brandt, M. Additive Manufacturing in Radiation Oncology: A Review of Clinical Practice, Emerging Trends and Research Opportunities. Int. J. Extreme Manuf. 2020, 2, 012003. [Google Scholar] [CrossRef]
- Van der Walt, M.; Crabtree, T.; Albantow, C. PLA as a Suitable 3D Printing Thermoplastic for Use in External Beam Radiotherapy. Australas. Phys. Eng. Sci. Med. 2019, 42, 1165–1176. [Google Scholar] [CrossRef]
- Peters, M.; de Leeuw, A.A.C.; Nomden, C.N.; Tanderup, K.; Kirchheiner, K.; Lindegaard, J.C.; Kirisits, C.; Haie-Meder, C.; Sturdza, A.; Fokdal, L.; et al. Risk Factors for Nodal Failure after Radiochemotherapy and Image Guided Brachytherapy in Locally Advanced Cervical Cancer: An EMBRACE Analysis. Radiother. Oncol. 2021, 163, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Pötter, R.; Tanderup, K.; Schmid, M.P.; Jürgenliemk-Schulz, I.; Haie-Meder, C.; Fokdal, L.U.; Sturdza, A.E.; Hoskin, P.; Mahantshetty, U.; Segedin, B.; et al. MRI-Guided Adaptive Brachytherapy in Locally Advanced Cervical Cancer (EMBRACE-I): A Multicentre Prospective Cohort Study. Lancet Oncol. 2021, 22, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Gerlach, S.; Schlaefer, A. Robotic Systems in Radiotherapy and Radiosurgery. Curr. Robot. Rep. 2022, 3, 9–19. [Google Scholar] [CrossRef]
- Pontoriero, A.; Iatì, G.; Aiello, D.; Pergolizzi, S. Stereotactic Radiotherapy in the Retreatment of Recurrent Cervical Cancers, Assessment of Toxicity, and Treatment Response: Initial Results and Literature Review. Technol. Cancer Res. Treat. 2016, 15, 759–765. [Google Scholar] [CrossRef]
- Parisi, S.; Ferini, G.; Cacciola, A.; Lillo, S.; Tamburella, C.; Santacaterina, A.; Bottari, A.; Brogna, A.; Ferrantelli, G.; Pontoriero, A.; et al. A Non-Surgical COMBO-Therapy Approach for Locally Advanced Unresectable Pancreatic Adenocarcinoma: Preliminary Results of a Prospective Study. Radiol. Med. 2022, 127, 214–219. [Google Scholar] [CrossRef]
- Parisi, S.; Ferini, G.; Lillo, S.; Brogna, A.; Chillari, F.; Ferrantelli, G.; Settineri, N.; Santacaterina, A.; Platania, A.; Leotta, S.; et al. Stereotactic Boost on Residual Disease after External-Beam Irradiation in Clinical Stage III Non-Small Cell Lung Cancer: Mature Results of Stereotactic Body Radiation Therapy Post Radiation Therapy (SBRTpostRT) Study. Radiol. Med. 2023, 128, 877–885. [Google Scholar] [CrossRef]
- Kairn, T.; Talkhani, S.; Charles, P.H.; Chua, B.; Lin, C.Y.; Livingstone, A.G.; Maxwell, S.K.; Poroa, T.; Simpson-Page, E.; Spelleken, E.; et al. Determining Tolerance Levels for Quality Assurance of 3D Printed Bolus for Modulated Arc Radiotherapy of the Nose. Phys. Eng. Sci. Med. 2021, 44, 1187–1199. [Google Scholar] [CrossRef]
- Sasaki, D.K.; McGeachy, P.; Alpuche Aviles, J.E.; McCurdy, B.; Koul, R.; Dubey, A. A Modern Mold Room: Meshing 3D Surface Scanning, Digital Design, and 3D Printing with Bolus Fabrication. J. Appl. Clin. Med. Phys. 2019, 20, 78–85. [Google Scholar] [CrossRef]
- Craft, D.F.; Kry, S.F.; Balter, P.; Salehpour, M.; Woodward, W.; Howell, R.M. Material Matters: Analysis of Density Uncertainty in 3D Printing and Its Consequences for Radiation Oncology. Med. Phys. 2018, 45, 1614–1621. [Google Scholar] [CrossRef] [PubMed]
- Kubota, Y.; Ohno, T.; Kawashima, M.; Murata, K.; Okonogi, N.; Noda, S.-E.; Tsuda, K.; Sakai, M.; Tashiro, M.; Nakano, T. Development of a Vaginal Immobilization Device: A Treatment-Planning Study of Carbon-Ion Radiotherapy and Intensity-Modulated Radiation Therapy for Uterine Cervical Cancer. Anticancer Res. 2019, 39, 1915–1921. [Google Scholar] [CrossRef] [PubMed]
- Schuh, J.C.L.; Funk, K.A. Compilation of International Standards and Regulatory Guidance Documents for Evaluation of Biomaterials, Medical Devices, and 3-D Printed and Regenerative Medicine Products. Toxicol. Pathol. 2019, 47, 344–357. [Google Scholar] [CrossRef]
- Chepelev, L.; Wake, N.; Ryan, J.; Althobaity, W.; Gupta, A.; Arribas, E.; Santiago, L.; Ballard, D.H.; Wang, K.C.; Weadock, W.; et al. Radiological Society of North America (RSNA) 3D Printing Special Interest Group (SIG): Guidelines for Medical 3D Printing and Appropriateness for Clinical Scenarios. 3D Print. Med. 2018, 4, 11. [Google Scholar] [CrossRef] [PubMed]
- Rindelaub, J.D.; Baird, Z.; Lindner, B.A.; Strantz, A.A. Identifying Extractable Profiles from 3D Printed Medical Devices. PLoS ONE 2019, 14, e0217137. [Google Scholar] [CrossRef]
- Samuelsson, A.; Mercke, C.; Johansson, K.-A. Systematic Set-up Errors for IMRT in the Head and Neck Region: Effect on Dose Distribution. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2003, 66, 303–311. [Google Scholar] [CrossRef]
- Manning, M.A.; Wu, Q.; Cardinale, R.M.; Mohan, R.; Lauve, A.D.; Kavanagh, B.D.; Morris, M.M.; Schmidt-Ullrich, R.K. The Effect of Setup Uncertainty on Normal Tissue Sparing with IMRT for Head-and-Neck Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 1400–1409. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Pain 1 | Burning 1 | Discomfort 1 | Psychological Impact 1 |
|---|---|---|---|---|
| 1 | 5 | 7 | 4 | 4 |
| 2 | 3 | 2 | 3 | 3 |
| 3 | 2 | 2 | 3 | 2 |
| 4 | 4 | 4 | 2 | 2 |
| 5 | 3 | 3 | 1 | 2 |
| 6 | 2 | 2 | 1 | 1 |
| 7 | 2 | 7 | 2 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisi, S.; Ferrantelli, G.; Santacaterina, A.; Russi, E.G.; Chillari, F.; Napoli, C.; Brogna, A.; Siragusa, C.; Sciacca, M.; Pontoriero, A.; et al. Design and Development of a Device (Sifilotto®) for Tumour Tracking in Cervical Cancer Patients Undergoing Robotic Arm LINAC Stereotactic Body Radiation Therapy Boost: Background to the STARBACS Study. Curr. Oncol. 2025, 32, 354. https://doi.org/10.3390/curroncol32060354
Parisi S, Ferrantelli G, Santacaterina A, Russi EG, Chillari F, Napoli C, Brogna A, Siragusa C, Sciacca M, Pontoriero A, et al. Design and Development of a Device (Sifilotto®) for Tumour Tracking in Cervical Cancer Patients Undergoing Robotic Arm LINAC Stereotactic Body Radiation Therapy Boost: Background to the STARBACS Study. Current Oncology. 2025; 32(6):354. https://doi.org/10.3390/curroncol32060354
Chicago/Turabian StyleParisi, Silvana, Giacomo Ferrantelli, Anna Santacaterina, Elvio Grazioso Russi, Federico Chillari, Claudio Napoli, Anna Brogna, Carmelo Siragusa, Miriam Sciacca, Antonio Pontoriero, and et al. 2025. "Design and Development of a Device (Sifilotto®) for Tumour Tracking in Cervical Cancer Patients Undergoing Robotic Arm LINAC Stereotactic Body Radiation Therapy Boost: Background to the STARBACS Study" Current Oncology 32, no. 6: 354. https://doi.org/10.3390/curroncol32060354
APA StyleParisi, S., Ferrantelli, G., Santacaterina, A., Russi, E. G., Chillari, F., Napoli, C., Brogna, A., Siragusa, C., Sciacca, M., Pontoriero, A., Iatì, G., & Pergolizzi, S. (2025). Design and Development of a Device (Sifilotto®) for Tumour Tracking in Cervical Cancer Patients Undergoing Robotic Arm LINAC Stereotactic Body Radiation Therapy Boost: Background to the STARBACS Study. Current Oncology, 32(6), 354. https://doi.org/10.3390/curroncol32060354