Planned Liver Stereotactic Body Radiotherapy for Residual Colorectal Cancer Liver Metastases After Surgery: A Single-Arm Retrospective Study

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Treatment Procedures
2.2.1. Systemic Treatment
2.2.2. Surgical Interventions
2.2.3. SBRT Techniques
2.3. Endpoint Assessment
2.4. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
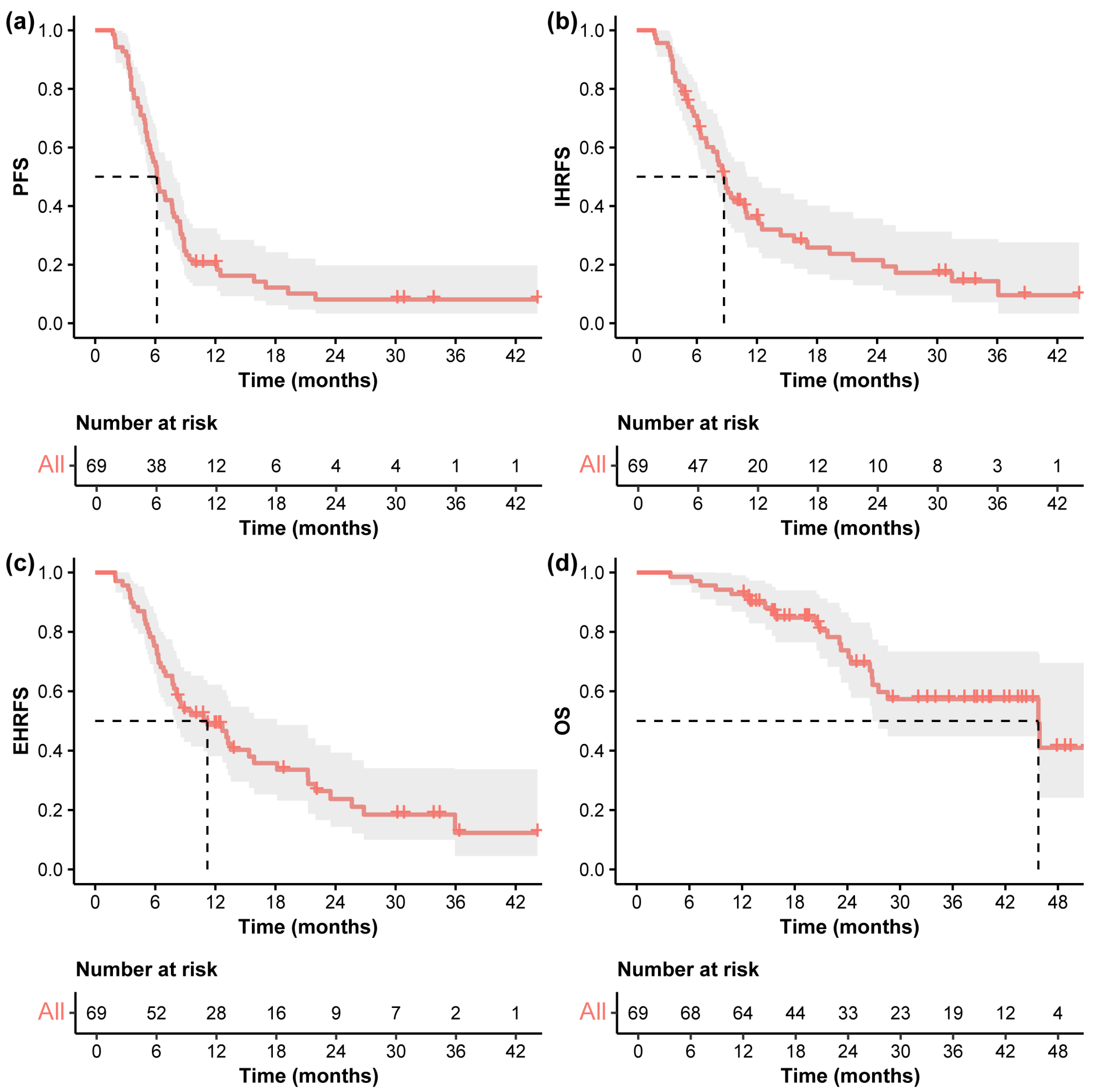
3.2. Oncological Outcomes
3.3. Pattern of Progression
3.4. Prognostic Analysis for Survival Outcomes
3.5. Toxicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, D.A.; Poston, G.J. Colorectal liver metastases: Current and future perspectives. Future Oncol. 2006, 2, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Vinet, E. Regional treatment of metastasis: Surgery of colorectal liver metastases. Ann. Oncol. 2004, 15 (Suppl. 4), iv103–iv106. [Google Scholar] [CrossRef] [PubMed]
- Uhlig, J.; Lukovic, J.; Dawson, L.A.; Patel, R.A.; Cavnar, M.J.; Kim, H.S. Locoregional Therapies for Colorectal Cancer Liver Metastases: Options Beyond Resection. Am. Soc. Clin. Oncol. Educ. Book 2021, 41, 133–146. [Google Scholar] [CrossRef]
- Cervantes, A.; Adam, R.; Roselló, S.; Arnold, D.; Normanno, N.; Taïeb, J.; Seligmann, J.; De Baere, T.; Osterlund, P.; Yoshino, T.; et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 10–32. [Google Scholar] [CrossRef]
- Liu, M.; Wang, Y.; Wang, K.; Bao, Q.; Wang, H.; Jin, K.; Liu, W.; Yan, X.; Xing, B. Combined ablation and resection (CARe) for resectable colorectal cancer liver Metastases-A propensity score matching study. Eur. J. Surg. Oncol. 2023, 49, 106931. [Google Scholar] [CrossRef]
- Han, K.; Kim, J.H.; Yang, S.G.; Park, S.H.; Choi, H.K.; Chun, S.Y.; Kim, P.N.; Park, J.; Lee, M. A Single-Center Retrospective Analysis of Periprocedural Variables Affecting Local Tumor Progression after Radiofrequency Ablation of Colorectal Cancer Liver Metastases. Radiology 2021, 298, 212–218. [Google Scholar] [CrossRef]
- Lee, H.J.; Lee, M.W.; Ahn, S.H.; Cha, D.I.; Ko, S.E.; Kang, T.W.; Song, K.D.; Rhim, H. Percutaneous radiofrequency ablation of solitary hepatic metastases from colorectal cancer: Risk factors of local tumor progression-free survival and overall survival. Ultrasonography 2022, 41, 728–739. [Google Scholar] [CrossRef]
- Puijk, R.S.; Dijkstra, M.; van den Bemd, B.A.T.; Ruarus, A.H.; Nieuwenhuizen, S.; Geboers, B.; Timmer, F.E.F.; Schouten, E.A.C.; de Vries, J.J.J.; van der Meijs, B.B.; et al. Improved Outcomes of Thermal Ablation for Colorectal Liver Metastases: A 10-Year Analysis from the Prospective Amsterdam CORE Registry (AmCORE). Cardiovasc. Interv. Radiol. 2022, 45, 1074–1089. [Google Scholar] [CrossRef]
- Amygdalos, I.; Hitpass, L.; Schmidt, F.; Josephs, G.; Bednarsch, J.; Berres, M.L.; Lüdde, T.; Olde Damink, S.W.M.; Ulmer, T.F.; Neumann, U.P.; et al. Survival after combined resection and ablation is not inferior to that after resection alone, in patients with four or more colorectal liver metastases. Langenbeck’s Arch. Surg. 2023, 408, 343. [Google Scholar] [CrossRef]
- Wach, M.M.; Washburn, L.A.; Alvikas, J.; Qu, L.T.; Zhang, M.; Etherington, M.S.; Rieser, C.; Haykal, T.; Pingpank, J.F.; Zureikat, A.H.; et al. Combined hepatic resection and ablation for high burden of colorectal liver metastases demonstrates safety and durable survival. HPB 2024, 26, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Joo, J.H.; Park, J.H.; Kim, J.C.; Yu, C.S.; Lim, S.B.; Park, I.J.; Kim, T.W.; Hong, Y.S.; Kim, K.P.; Yoon, S.M.; et al. Local Control Outcomes Using Stereotactic Body Radiation Therapy for Liver Metastases From Colorectal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 876–883. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Comito, T.; Barni, S.; Pancera, G.; Scorsetti, M.; Ghidini, A.; SBRT for CRC liver metastases. Stereotactic body radiotherapy for colorectal cancer liver metastases: A systematic review. Radiother. Oncol. 2018, 129, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Folkert, M.R.; Meyer, J.J.; Aguilera, T.A.; Yokoo, T.; Sanford, N.N.; Rule, W.G.; Mansour, J.; Yopp, A.; Polanco, P.; Hannan, R.; et al. Long-Term Results of a Phase 1 Dose-Escalation Trial and Subsequent Institutional Experience of Single-Fraction Stereotactic Ablative Radiation Therapy for Liver Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2021, 109, 1387–1395. [Google Scholar] [CrossRef]
- Stera, S.; Miebach, G.; Buergy, D.; Dreher, C.; Lohr, F.; Wurster, S.; Rödel, C.; Marcella, S.; Krug, D.; Frank, A.G.; et al. Liver SBRT with active motion-compensation results in excellent local control for liver oligometastases: An outcome analysis of a pooled multi-platform patient cohort. Radiother. Oncol. 2021, 158, 230–236. [Google Scholar] [CrossRef]
- Rodríguez, M.R.; Chen-Zhao, X.; Hernando, O.; Flamarique, S.; Fernández-Letón, P.; Campo, M.; López, M.; Rodríguez, M.; Zucca, D.; Martínez, D.; et al. SBRT-SG-01: Final results of a prospective multicenter study on stereotactic body radiotherapy for liver metastases. Clin. Transl. Oncol. 2024, 26, 1790–1797. [Google Scholar] [CrossRef]
- Fong, Y.; Fortner, J.; Sun, R.L.; Brennan, M.F.; Blumgart, L.H. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer: Analysis of 1001 consecutive cases. Ann. Surg. 1999, 230, 309–321. [Google Scholar] [CrossRef]
- Sasaki, K.; Morioka, D.; Conci, S.; Margonis, G.A.; Sawada, Y.; Ruzzenente, A.; Kumamoto, T.; Iacono, C.; Andreatos, N.; Guglielmi, A.; et al. The Tumor Burden Score: A New “Metro-ticket” Prognostic Tool For Colorectal Liver Metastases Based on Tumor Size and Number of Tumors. Ann. Surg. 2018, 267, 132–141. [Google Scholar] [CrossRef]
- Liu, M.; Wang, K.; Wang, Y.; Bao, Q.; Wang, H.; Jin, K.; Liu, W.; Xing, B. Short- and long-term outcomes of hepatectomy combined with intraoperative radiofrequency ablation for patients with multiple primarily unresectable colorectal liver metastases: A propensity matching analysis. HPB 2021, 23, 1586–1594. [Google Scholar] [CrossRef]
- Wang, H.; Zheng, X.; Sun, J.; Zhu, X.; Dong, D.; Du, Y.; Feng, Z.; Gong, J.; Wu, H.; Geng, J.; et al. 4D-MRI assisted stereotactic body radiation therapy for unresectable colorectal cancer liver metastases. Clin. Transl. Radiat. Oncol. 2024, 45, 100714. [Google Scholar] [CrossRef]
- van der Lei, S.; Dijkstra, M.; Nieuwenhuizen, S.; Schulz, H.H.; Vos, D.J.W.; Versteeg, K.S.; Buffart, T.E.; Swijnenburg, R.J.; de Vries, J.J.J.; Bruynzeel, A.M.E.; et al. Unresectable Intermediate-Size (3–5 cm) Colorectal Liver Metastases: Stereotactic Ablative Body Radiotherapy Versus Microwave Ablation (COLLISION-XL): Protocol of a Phase II/III Multicentre Randomized Controlled Trial. Cardiovasc. Interv. Radiol. 2023, 46, 1076–1085. [Google Scholar] [CrossRef] [PubMed]
- McDermott, R.L.; Dunne, E.M.; Zhao, Y.; Bergman, A.; Liu, M.C.; Schellenberg, D.; Ma, R.M. Stereotactic Ablative Radiation Therapy for Colorectal Liver Metastases. Clin. Color. Cancer 2023, 22, 120–128. [Google Scholar] [CrossRef] [PubMed]
- Scorsetti, M.; Comito, T.; Clerici, E.; Franzese, C.; Tozzi, A.; Iftode, C.; Di Brina, L.; Navarria, P.; Mancosu, P.; Reggiori, G.; et al. Phase II trial on SBRT for unresectable liver metastases: Long-term outcome and prognostic factors of survival after 5 years of follow-up. Radiat. Oncol. 2018, 13, 234. [Google Scholar] [CrossRef] [PubMed]
- Tian, Y.; Wang, Y.; Wen, N.; Wang, S.; Li, B.; Liu, G. Prognostic factors associated with early recurrence following liver resection for colorectal liver metastases: A systematic review and meta-analysis. BMC Cancer 2024, 24, 426. [Google Scholar] [CrossRef]
- Joechle, K.; Vreeland, T.J.; Vega, E.A.; Okuno, M.; Newhook, T.E.; Panettieri, E.; Chun, Y.S.; Tzeng, C.D.; Aloia, T.A.; Lee, J.E.; et al. Anatomic Resection Is Not Required for Colorectal Liver Metastases with RAS Mutation. J. Gastrointest. Surg. 2020, 24, 1033–1039. [Google Scholar] [CrossRef]
- Cheng, K.C.; Yip, A.S. Prognostic factors of survival and a new scoring system for liver resection of colorectal liver metastasis. World J. Hepatol. 2022, 14, 209–223. [Google Scholar] [CrossRef]
- Mainali, B.B.; Valenzuela, C.D.; Moaven, O.; Stauffer, J.A.; Del Piccolo, N.R.; Cheung, T.; Corvera, C.U.; Wisneski, A.D.; Cha, C.H.; Zarandi, N.P.; et al. Resection versus resection with ablation: Analysis from the colorectal liver operative metastasis international collaborative. J. Surg. Oncol. 2024, 130, 516–522. [Google Scholar] [CrossRef]
- Vadisetti, S.N.; Kazi, M.; Patkar, S.; Mundhada, R.; Desouza, A.; Saklani, A.; Goel, M. Patterns and Predictors of Recurrence After Curative Resection of Colorectal Liver Metastasis (CRLM). J. Gastrointest. Cancer 2024, 55, 1559–1568. [Google Scholar] [CrossRef]
- Folprecht, G.; Gruenberger, T.; Bechstein, W.; Raab, H.R.; Weitz, J.; Lordick, F.; Hartmann, J.T.; Stoehlmacher-Williams, J.; Lang, H.; Trarbach, T.; et al. Survival of patients with initially unresectable colorectal liver metastases treated with FOLFOX/cetuximab or FOLFIRI/cetuximab in a multidisciplinary concept (CELIM study). Ann. Oncol. 2014, 25, 1018–1025. [Google Scholar] [CrossRef]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Cremolini, C.; Antoniotti, C.; Rossini, D.; Lonardi, S.; Loupakis, F.; Pietrantonio, F.; Bordonaro, R.; Latiano, T.P.; Tamburini, E.; Santini, D.; et al. Upfront FOLFOXIRI plus bevacizumab and reintroduction after progression versus mFOLFOX6 plus bevacizumab followed by FOLFIRI plus bevacizumab in the treatment of patients with metastatic colorectal cancer (TRIBE2): A multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol. 2020, 21, 497–507. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.; Ren, L.; Liu, T.; Ye, Q.; Wei, Y.; He, G.; Lin, Q.; Wang, X.; Wang, M.; Liang, F.; et al. Bevacizumab Plus mFOLFOX6 Versus mFOLFOX6 Alone as First-Line Treatment for RAS Mutant Unresectable Colorectal Liver-Limited Metastases: The BECOME Randomized Controlled Trial. J. Clin. Oncol. 2020, 38, 3175–3184. [Google Scholar] [CrossRef] [PubMed]
- Bond, M.J.G.; Bolhuis, K.; Loosveld, O.J.L.; de Groot, J.W.B.; Droogendijk, H.; Helgason, H.H.; Hendriks, M.P.; Klaase, J.M.; Kazemier, G.; Liem, M.S.L.; et al. First-line systemic treatment strategies in patients with initially unresectable colorectal cancer liver metastases (CAIRO5): An open-label, multicentre, randomised, controlled, phase 3 study from the Dutch Colorectal Cancer Group. Lancet Oncol. 2023, 24, 757–771. [Google Scholar] [CrossRef] [PubMed]
- Valenzuela, C.D.; Moaven, O.; Solsky, I.B.; Stauffer, J.A.; Del Piccolo, N.R.; Cheung, T.; Corvera, C.U.; Wisneski, A.D.; Cha, C.H.; Pourhabibi Zarandi, N.; et al. Conditional Survival After Hepatectomy for Colorectal Liver Metastasis: Results from the Colorectal Liver Operative Metastasis International Collaborative (COLOMIC). Ann. Surg. Oncol. 2023, 30, 3413–3422. [Google Scholar] [CrossRef]
- Pourfaraji, S.M.; Moghadam, M.N.; Moradi, A.M.; Shirmard, F.O.; Mohammadzadeh, N.; Jafarian, A. Long-term survival after hepatic resection for colorectal liver metastases: A single-center study in Iran. BMC Surg. 2024, 24, 131. [Google Scholar] [CrossRef]
- Canseco, L.M.; Liu, Y.W.; Lu, C.C.; Lee, K.C.; Chen, H.H.; Hu, W.H.; Tsai, K.L.; Yang, Y.H.; Wang, C.C.; Hung, C.H. Survival Evidence of Local Control for Colorectal Cancer Liver Metastases by Hepatectomy and/or Radiofrequency Ablation. Cancers 2023, 15, 4434. [Google Scholar] [CrossRef]
- Ecker, B.L.; Lee, J.; Saadat, L.V.; Aparicio, T.; Buisman, F.E.; Balachandran, V.P.; Drebin, J.A.; Hasegawa, K.; Jarnagin, W.R.; Kemeny, N.E.; et al. Recurrence-free survival versus overall survival as a primary endpoint for studies of resected colorectal liver metastasis: A retrospective study and meta-analysis. Lancet Oncol. 2022, 23, 1332–1342. [Google Scholar] [CrossRef]
- Otake, S.; Goto, T. Stereotactic Radiotherapy for Oligometastasis. Cancers 2019, 11, 133. [Google Scholar] [CrossRef]
- Lievens, Y.; Guckenberger, M.; Gomez, D.; Hoyer, M.; Iyengar, P.; Kindts, I.; Méndez Romero, A.; Nevens, D.; Palma, D.; Park, C.; et al. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document. Radiother. Oncol. 2020, 148, 157–166. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Patient Characteristic | Patients, No. (%) |
|---|---|
| Age, median (range) | 58 (30–72) |
| Gender | |
| Male | 47 (68.1%) |
| Female | 22 (31.9%) |
| ECOG PS | |
| 0 | 59 (85.5%) |
| 1 | 10 (14.5%) |
| Primary tumor location | |
| Right colon | 7 (10.1%) |
| Left colon | 41 (59.4%) |
| Rectum | 21 (30.4%) |
| T stage | |
| 2 | 2 (2.9%) |
| 3 | 52 (75.4%) |
| 4 | 15 (21.7%) |
| N stage | |
| 0 | 15 (21.7%) |
| 1 | 39 (56.5%) |
| 2 | 15 (21.7%) |
| Gene testing | |
| Wild-type | 42 (60.9%) |
| RAS mutation | 24 (34.8%) |
| BRAF mutation | 4 (5.8%) |
| Timing of liver metastases | |
| Synchronous metastases | 60 (87.0%) |
| Metachronous metastases | 9 (13.0%) |
| Number of CRLMs per patient, median (range) | 11 (2–58) |
| Distribution of liver metastases | |
| Unilobar metastases | 8 (11.6%) |
| Bilobar metastases | 61 (88.4%) |
| Location of extrahepatic metastatic sites | |
| None | 55 (79.7%) |
| Lung | 8 (11.6%) |
| Others | 6 (8.7%) |
| Treatment Parameters | Patients/Lesions, No. (%) |
|---|---|
| Pre-treatment systemic therapy | |
| First-line | 49 (71.0%) |
| Second-line | 20 (29.0%) |
| Best response of pre-treatment systemic therapy | |
| Partial response | 44 (63.8%) |
| Stable disease | 25 (36.2%) |
| Post-treatment systemic therapy | |
| No | 10 (14.5%) |
| Yes | 59 (85.5%) |
| Type of surgical approach | |
| CARe | 43 (62.3%) |
| Hepatectomy | 26 (37.7%) |
| Interval between surgery and SBRT, median (range) | 6.6 weeks (3.1–15.3) |
| ≤5 weeks | 10 (14.5%) |
| 5–10 weeks | 50 (72.5%) |
| >10 weeks | 9 (13.0%) |
| Number of CRLMs treated by different surgical approaches per patient | |
| CARe, median (range) | 13 (3–57) |
| Hepatectomy, median (range) | 5 (1–10) |
| Number of CRLMs treated by SBRT per patient, median (range) | 1 (1–5) |
| Size of CRLMs treated by SBRT, median (range) | 14 mm (5–42) |
| <10 mm | 22 (17.9%) |
| 10–19 mm | 60 (48.8%) |
| 20–29 mm | 27 (22.0%) |
| ≥30 mm | 14 (11.4%) |
| ITV, median (range) | 13.1 cm3 (0.7–90.1) |
| <5.0 cm3 | 20 (16.3%) |
| 5.0–24.9 cm3 | 71 (57.7%) |
| 25.0–49.9 cm3 | 24 (19.5%) |
| ≥50.0 cm3 | 8 (6.5%) |
| PTV, median (range) | 38.5 cm3 (4.0–173.4) |
| <20.0 cm3 | 16 (13.0%) |
| 20.0–59.9 cm3 | 74 (60.2%) |
| 60.0–99.9 cm3 | 23 (18.7%) |
| ≥100.0 cm3 | 10 (8.1%) |
| BED10 per lesion, median (range) | 100.0 Gy (71.4–132.0) |
| ≥100.0 Gy | 70 (56.9%) |
| <100.0 Gy | 53 (43.1%) |
| Variables | Univariate | Multivariate | |
|---|---|---|---|
| p-Value | HR (95% CI) | p-Value | |
| Gender (male vs. female) | 0.690 | ||
| Age (years) | 0.856 | ||
| Primary tumor | |||
| Location (left-sided vs. right-sided) | 0.589 | ||
| Stage (N1–2 vs. N0) | 0.272 | ||
| RAS/BRAF status (mutation vs. wild-type) | 0.004 | 4.49 (1.69–11.95) | 0.003 |
| Liver metastases | |||
| Synchronous vs. metachronous | 0.498 | ||
| Distribution (bilobar vs. unilobar) | 0.158 | ||
| Number of lesions | 0.218 | ||
| Maximum lesion size at diagnosis (mm) | 0.590 | ||
| Extrahepatic metastases | |||
| None | Ref | Ref | Ref |
| Lung | 0.789 | 0.98 (0.21–4.48) | 0.978 |
| Others | <0.001 | 15.73 (4.06–60.96) | <0.001 |
| CEA (ng/mL) | 0.010 | 1.00 (1.00–1.01) | 0.041 |
| Pre-treatment therapy | |||
| First-line vs. second-line | 0.509 | ||
| Best response (SD vs. PR) | 0.128 | ||
| Grade 1 No. (%) | Grade 2 No. (%) | Grade 3 No. (%) | |
|---|---|---|---|
| Leukopenia | 17 (24.6%) | 15 (21.7%) | 2 (2.9%) |
| Neutropenia | 15 (21.7%) | 13 (18.8%) | 0 (0.0%) |
| Thrombocytopenia | 10 (14.5%) | 4 (5.8%) | 1 (1.4%) |
| Anemia | 13 (18.8%) | 1 (1.4%) | 0 (0.0%) |
| Elevated ALT/AST | 10 (14.5%) | 1 (1.4%) | 0 (0.0%) |
| Hyperbilirubinemia | 7 (10.1%) | 0 (0.0%) | 0 (0.0%) |
| Abdominal pain | 0 (0.0%) | 1 (1.4%) | 0 (0.0%) |
| Diarrhea | 3 (4.3%) | 0 (0.0%) | 0 (0.0%) |
| Nausea | 6 (8.7%) | 0 (0.0%) | 0 (0.0%) |
| Fatigue | 4 (5.8%) | 0 (0.0%) | 0 (0.0%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, S.; Dong, D.; Zheng, X.; Wang, H.; Wang, K.; Xing, B.; Wang, W. Planned Liver Stereotactic Body Radiotherapy for Residual Colorectal Cancer Liver Metastases After Surgery: A Single-Arm Retrospective Study. Curr. Oncol. 2025, 32, 347. https://doi.org/10.3390/curroncol32060347
Li S, Dong D, Zheng X, Wang H, Wang K, Xing B, Wang W. Planned Liver Stereotactic Body Radiotherapy for Residual Colorectal Cancer Liver Metastases After Surgery: A Single-Arm Retrospective Study. Current Oncology. 2025; 32(6):347. https://doi.org/10.3390/curroncol32060347
Chicago/Turabian StyleLi, Sixuan, Dezuo Dong, Xuan Zheng, Hongzhi Wang, Kun Wang, Baocai Xing, and Weihu Wang. 2025. "Planned Liver Stereotactic Body Radiotherapy for Residual Colorectal Cancer Liver Metastases After Surgery: A Single-Arm Retrospective Study" Current Oncology 32, no. 6: 347. https://doi.org/10.3390/curroncol32060347
APA StyleLi, S., Dong, D., Zheng, X., Wang, H., Wang, K., Xing, B., & Wang, W. (2025). Planned Liver Stereotactic Body Radiotherapy for Residual Colorectal Cancer Liver Metastases After Surgery: A Single-Arm Retrospective Study. Current Oncology, 32(6), 347. https://doi.org/10.3390/curroncol32060347