TreC_Metha: A Digital Application to Enhance Patient Agency, Therapy Compliance and Quality of Life in Metastatic Breast Cancer Patients


Abstract
1. Introduction
1.1. Background
1.2. Role of Digital Tools in Breast Cancer and Previous Works
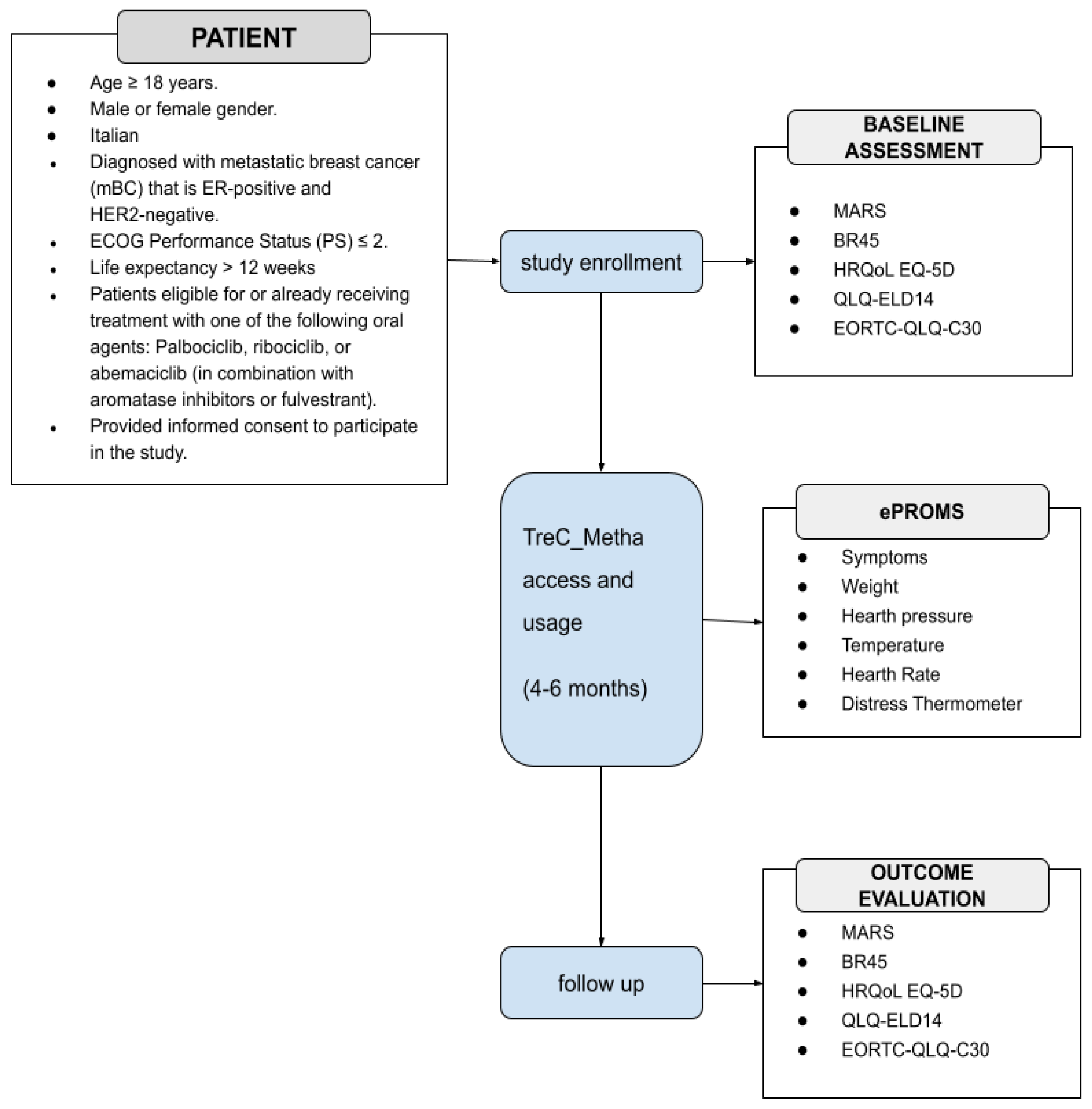
1.3. Study Aim
- Home therapy administration diaries;
- Monitoring of drug toxicities and disease-related symptoms;
- Systems to improve adherence (through alerts and/or educational support);
- Support for mental health aspects;
- Information on symptoms of disease and on collateral effects of its therapies;
- Educational support on promoting and improving lifestyles;
- Administering and gathering questionnaires to assess communication comprehension, well-being, satisfaction, and quality of life;
- Use of a chat between doctor/healthcare personnel and patient;
- Recording personal narratives.
- The perceived value of the overall solution following a value-based care approach by: disease awareness questionnaire before and after use of the platform; distress thermometer use; final satisfaction questionnaire; QoL measures questionnaire;
- The cost–benefit outcomes of implementing this solution in terms of number of people that could benefit against the overall cost (e.g., reduction in unplanned and unnecessary admissions to hospital, in general, and to the emergency department in particular; reduction in hospital admissions or their duration due to treatment side effects; reduction in patient transport at hospital expense).

{kind=link}
{kind=link}
{kind=link}
| Objectives for Patients | |
|---|---|
| Education | Provision of training, educational resources, and motivational support during periods of treatment, as well as during therapeutic breaks. |
| Patient Empowerment | The utilization of a diary has been identified as a method to stimulate active involvement in healthcare and decision-making, as well as the incorporation of patient-reported outcome measures (PROMs) and patient-reported experience measures (PREMs). |
| QoL Measurement | The utilization of PROMs and PREMs encompassing QoL scales allows for the evaluation of physical and mental health. |
| Objectives for the Healthcare Team | |
| Data Utilization | Collection and use of patient-generated health data (PGHD), such as self-reported side effects, to adjust treatment plans. |
| Improved Communication | Improvement of communication and co-operation between healthcare providers. |
| Intervention Tracking | The maintenance of comprehensive records of interventions during the course of the care process. |
| Objectives for healthcare organizations | |
| Reduction in unplanned and unnecessary admissions to the hospital, in general, and to the emergency department in particular; Reduction in hospital admissions or their duration due to treatment side effects (e.g., toxicity); Reduction in patient transport at hospital expense | |
2. Materials and Methods
3. Results
3.1. Survey and Focus Groups Results
3.2. Analysis of the Clinical Process
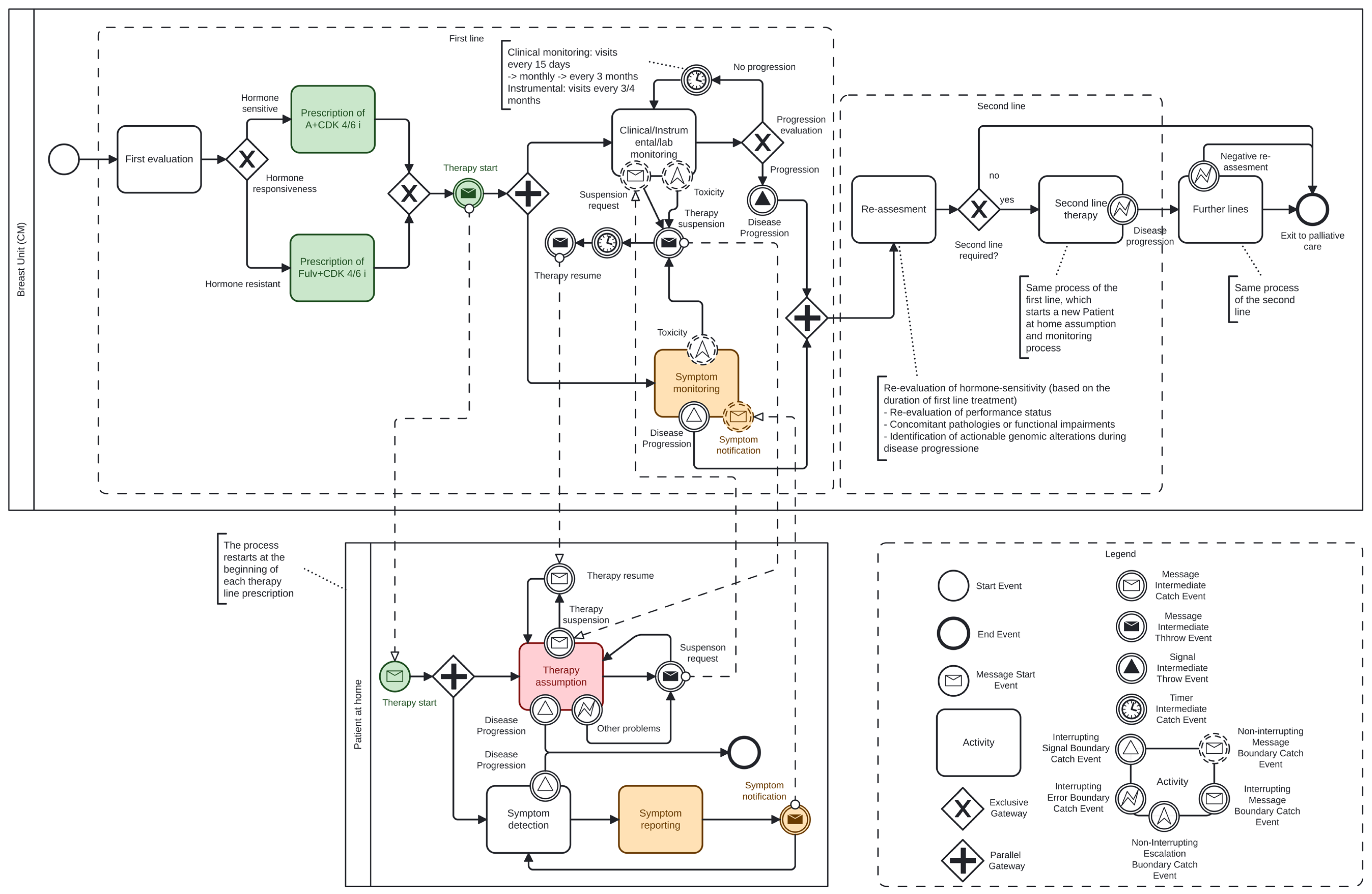
3.2.1. Analysis of the Clinical Process in Hospital Setting Pool
- Clinical, instrumental, and laboratory monitoring. In this activity, the oncologist team continuously controls the treatment course, which includes visits every 15 days initially, and then monthly, with monitoring of blood count, hepatic, renal function through regular blood tests, and psychological distress;
- At the same time, symptom monitoring relies on the patient’s self-reporting to the care team of any symptoms that may arise following home therapy administration (reception of the message Symptoms notification from the Patient at home pool). Currently, the communication occurs by phone or by visiting the ER.
- Second-line ET (with or without other targeted agents), if appropriate;
- Cross to chemotherapy (or Antibody drug conjugates) regimen;
- Transition to exclusive palliative care if further treatment is not viable.
- Targeting of an altered endocrine pathway, encompassing fulvestrant, novel oral SERDs and an array of other novel endocrine agents, including SERMs, SERCAs, CERANs and PROTACs among patients who had longer prior exposure to CDK4/6is (at least 12 months), especially ESR1-mutant (median PFS 8 months in this specific subset). Inhibiting alternative estrogen receptor-independent signaling pathways (such as the PI3K/AKT/PTEN pathway) by alpelisib [50] and capivasertib, achieving, respectively, a median PFS of 11 and 7 months [51];
- Toxicity related to the treatment, as detected through the two monitoring activities mentioned above;
- Patient requests for personal or medical reasons;
- Other clinical or logistical issues that may arise during therapy administration (e.g., occurrence of other morbid conditions related or unrelated to the underlying oncological pathology).
3.2.2. Analysis of the Clinical Process in ‘Patient at Home’ Pool
- Taking the prescribed therapy as instructed by the care team;
- Monitoring and reporting symptoms to the care team that may indicate toxicity caused by the medication.
3.3. Technological Tools
3.4. Application Structure and Functionalities
3.4.1. Healthcare Professional Dashboard
3.4.2. Patient’s App
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ADCs | Antibody–Drug Conjugates |
| BC | Breast Cancer |
| BPMN | Business Process Model and Notation |
| ET | Endocrine Therapies |
| GDPR | General Data Protection Regulation |
| HR | Hormonal Receptor |
| mBC | Metastatic Breast Cancer |
| mTOR | Mechanistic Target of Rapamycin |
| OMG | Object Management Group |
| PARP | Poly ADP Ribose Polymerase |
| PFS | Progression Free Survival |
| OS | Overall Survival |
| PGHD | Patient-Generated Health Data |
| PREMS | Patient-Reported Experience |
| PROMS | Patient-Reported Outcomes |
| QoL | Quality Of Life |
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Liu, Y.-R.; Ji, P.; Hu, X.; Shao, Z.-M. Impact of Molecular Subtypes on Metastatic Breast Cancer Patients: A SEER Population-Based Study. Sci. Rep. 2017, 7, 45411. [Google Scholar] [CrossRef]
- Kast, K.; Link, T.; Friedrich, K.; Petzold, A.; Niedostatek, A.; Schoffer, O.; Werner, C.; Klug, S.J.; Werner, A.; Gatzweiler, A.; et al. Impact of Breast Cancer Subtypes and Patterns of Metastasis on Outcome. Breast Cancer Res. Treat. 2015, 150, 621–629. [Google Scholar] [CrossRef]
- Sant, M.; Allemani, C.; Berrino, F.; Coleman, M.P.; Aareleid, T.; Chaplain, G.; Coebergh, J.W.; Colonna, M.; Crosignani, P.; Danzon, A.; et al. Breast Carcinoma Survival in Europe and the United States: A Population-based Study. Cancer 2004, 100, 715–722. [Google Scholar] [CrossRef]
- Gobbini, E.; Ezzalfani, M.; Dieras, V.; Bachelot, T.; Brain, E.; Debled, M.; Jacot, W.; Mouret-Reynier, M.A.; Goncalves, A.; Dalenc, F.; et al. Time Trends of Overall Survival among Metastatic Breast Cancer Patients in the Real-Life ESME Cohort. Eur. J. Cancer 2018, 96, 17–24. [Google Scholar] [CrossRef]
- Miglietta, F.; Bottosso, M.; Griguolo, G.; Dieci, M.V.; Guarneri, V. Major Advancements in Metastatic Breast Cancer Treatment: When Expanding Options Means Prolonging Survival. ESMO Open 2022, 7, 100409. [Google Scholar] [CrossRef]
- Penberthy, J.K.; Stewart, A.L.; Centeno, C.F.; Penberthy, D.R. Psychological Aspects of Breast Cancer. Psychiatr. Clin. N. Am. 2023, 46, 551–570. [Google Scholar] [CrossRef]
- Krigel, S.; Myers, J.; Befort, C.; Krebill, H.; Klemp, J. ‘Cancer Changes Everything!’ Exploring the Lived Experiences of Women with Metastatic Breast Cancer. Int. J. Palliat. Nurs. 2014, 20, 334–342. [Google Scholar] [CrossRef]
- Reed, E.; Simmonds, P.; Haviland, J.; Corner, J. Quality of Life and Experience of Care in Women with Metastatic Breast Cancer: A Cross-Sectional Survey. J. Pain Symptom Manag. 2012, 43, 747–758. [Google Scholar] [CrossRef]
- Irvin, W.; Muss, H.B.; Mayer, D.K. Symptom Management in Metastatic Breast Cancer. Oncologist 2011, 16, 1203–1214. [Google Scholar] [CrossRef]
- Kenne Sarenmalm, E.; Thorén-Jönsson, A.-L.; Gaston-Johansson, F.; Öhlén, J. Making Sense of Living Under the Shadow of Death: Adjusting to a Recurrent Breast Cancer Illness. Qual. Health Res. 2009, 19, 1116–1130. [Google Scholar] [CrossRef] [PubMed]
- Willis, K.; Lewis, S.; Ng, F.; Wilson, L. The Experience of Living with Metastatic Breast Cancer—A Review of the Literature. Health Care Women Int. 2015, 36, 514–542. [Google Scholar] [CrossRef] [PubMed]
- Vilhauer, R.P. A Qualitative Study of the Experiences of Women with Metastatic Breast Cancer. Pall. Supp. Care 2008, 6, 249–258. [Google Scholar] [CrossRef]
- Warren, M. Uncertainty, Lack of Control and Emotional Functioning in Women with Metastatic Breast Cancer: A Review and Secondary Analysis of the Literature Using the Critical Appraisal Technique: Secondary Breast Cancer Literature Review. Eur. J. Cancer Care 2010, 19, 564–574. [Google Scholar] [CrossRef]
- Badr, H.; Shen, M.J. Pain Catastrophizing, Pain Intensity, and Dyadic Adjustment Influence Patient and Partner Depression in Metastatic Breast Cancer. Clin. J. Pain 2014, 30, 923–933. [Google Scholar] [CrossRef]
- White, C.B.; Smith, M.L.; Abidoye, O.O.; Lalla, D. Impacts of Toxicity on Patient Treatment Choices for Metastatic Breast Cancer. J. Clin. Oncol. 2012, 30, 18. [Google Scholar] [CrossRef]
- Ghislain, I.; Zikos, E.; Coens, C.; Quinten, C.; Balta, V.; Tryfonidis, K.; Piccart, M.; Zardavas, D.; Nagele, E.; Bjelic-Radisic, V.; et al. Health-Related Quality of Life in Locally Advanced and Metastatic Breast Cancer: Methodological and Clinical Issues in Randomised Controlled Trials. Lancet Oncol. 2016, 17, e294–e304. [Google Scholar] [CrossRef]
- Gaynor, S.; O’Meara, Y.; Mulvaney, E.; Keogh, R.J.; Weadick, C.S.; Duane, F.J.; Mc Brien, A.; Greally, H.; O’Leary, M.J.; Teiserskyte, I.; et al. A Patient-Led Survey on Information and Communication Needs of Patients with Metastatic Breast Cancer in Ireland and Northern Ireland (CTRIAL-IE 23–05). Breast 2025, 79, 103837. [Google Scholar] [CrossRef]
- Clarijs, M.E.; Thurell, J.; Kühn, F.; Uyl-de Groot, C.A.; Hedayati, E.; Karsten, M.M.; Jager, A.; Koppert, L.B. Measuring Quality of Life Using Patient-Reported Outcomes in Real-World Metastatic Breast Cancer Patients: The Need for a Standardized Approach. Cancers 2021, 13, 2308. [Google Scholar] [CrossRef]
- Basch, E.; Schrag, D.; Henson, S.; Jansen, J.; Ginos, B.; Stover, A.M.; Carr, P.; Spears, P.A.; Jonsson, M.; Deal, A.M.; et al. Effect of Electronic Symptom Monitoring on Patient-Reported Outcomes Among Patients with Metastatic Cancer: A Randomized Clinical Trial. JAMA 2022, 327, 2413. [Google Scholar] [CrossRef]
- Mir, O.; Ferrua, M.; Fourcade, A.; Mathivon, D.; Duflot-Boukobza, A.; Dumont, S.; Baudin, E.; Delaloge, S.; Malka, D.; Albiges, L.; et al. Digital Remote Monitoring plus Usual Care versus Usual Care in Patients Treated with Oral Anticancer Agents: The Randomized Phase 3 CAPRI Trial. Nat. Med. 2022, 28, 1224–1231. [Google Scholar] [CrossRef] [PubMed]
- Absolom, K.; Warrington, L.; Hudson, E.; Hewison, J.; Morris, C.; Holch, P.; Carter, R.; Gibson, A.; Holmes, M.; Clayton, B.; et al. Phase III Randomized Controlled Trial of eRAPID: eHealth Intervention During Chemotherapy. J. Clin. Oncol. 2021, 39, 734–747. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Iasonos, A.; McDonough, T.; Barz, A.; Culkin, A.; Kris, M.G.; Scher, H.I.; Schrag, D. Patient versus Clinician Symptom Reporting Using the National Cancer Institute Common Terminology Criteria for Adverse Events: Results of a Questionnaire-Based Study. Lancet Oncol. 2006, 7, 903–909. [Google Scholar] [CrossRef]
- Di Maio, M.; Gallo, C.; Leighl, N.B.; Piccirillo, M.C.; Daniele, G.; Nuzzo, F.; Gridelli, C.; Gebbia, V.; Ciardiello, F.; De Placido, S.; et al. Symptomatic Toxicities Experienced During Anticancer Treatment: Agreement Between Patient and Physician Reporting in Three Randomized Trials. J. Clin. Oncol. 2015, 33, 910–915. [Google Scholar] [CrossRef]
- Di Maio, M.; Basch, E.; Bryce, J.; Perrone, F. Patient-Reported Outcomes in the Evaluation of Toxicity of Anticancer Treatments. Nat. Rev. Clin. Oncol. 2016, 13, 319–325. [Google Scholar] [CrossRef]
- Lazare, A. The Customer Approach to Patienthood: Attending to Patient Requests in a Walk-In Clinic. Arch. Gen. Psychiatry 1975, 32, 553. [Google Scholar] [CrossRef]
- Slack, W. Points of View. Lancet 1977, 310, 240. [Google Scholar] [CrossRef]
- Fiore, N. Fighting Cancer—One Patient’s Perspective. N. Engl. J. Med. 1979, 300, 284–289. [Google Scholar] [CrossRef]
- Kirsch, E.P.; Kunte, S.A.; Wu, K.A.; Kaplan, S.; Hwang, E.S.; Plichta, J.K.; Lad, S.P. Digital Health Platforms for Breast Cancer Care: A Scoping Review. J. Clin. Med. 2024, 13, 1937. [Google Scholar] [CrossRef]
- Kim, S.M.; Kim, D.S.; Jang, Y.; Kim, M.K.; Yu, E.-S.; Han, D.H.; Kim, H.J. Evaluating the Effectiveness of a Mobile App for Breast Cancer Self-Management on Self-Efficacy: Nonrandomized Intervention Trial. JMIR mHealth uHealth 2025, 13, e63989. [Google Scholar] [CrossRef]
- Handa, S.; Okuyama, H.; Yamamoto, H.; Nakamura, S.; Kato, Y. Effectiveness of a Smartphone Application as a Support Tool for Patients Undergoing Breast Cancer Chemotherapy: A Randomized Controlled Trial. Clin. Breast Cancer 2020, 20, 201–208. [Google Scholar] [CrossRef] [PubMed]
- Grašič Kuhar, C.; Gortnar Cepeda, T.; Kovač, T.; Kukar, M.; Ružić Gorenjec, N. Mobile App for Symptom Management and Associated Quality of Life During Systemic Treatment in Early Stage Breast Cancer: Nonrandomized Controlled Prospective Cohort Study. JMIR mHealth uHealth 2020, 8, e17408. [Google Scholar] [CrossRef]
- Zhu, J.; Ebert, L.; Liu, X.; Wei, D.; Chan, S.W.-C. Mobile Breast Cancer E-Support Program for Chinese Women With Breast Cancer Undergoing Chemotherapy (Part 2): Multicenter Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e104. [Google Scholar] [CrossRef]
- Mohammadzadeh, Z.; Eghtedar, S.; Ayatollahi, H.; Jebraeily, M. Effectiveness of a Self-Management Mobile App on the Quality of Life of Women with Breast Cancer: A Study in a Developing Country. BMC Women’s Health 2022, 22, 446. [Google Scholar] [CrossRef]
- Buscemi, J.; Buitrago, D.; Iacobelli, F.; Penedo, F.; Maciel, C.; Guitleman, J.; Balakrishnan, A.; Corden, M.; Adler, R.F.; Bouchard, L.C.; et al. Feasibility of a Smartphone-Based Pilot Intervention for Hispanic Breast Cancer Survivors: A Brief Report. Transl. Behav. Med. 2019, 9, 638–645. [Google Scholar] [CrossRef]
- Baik, S.H.; Oswald, L.B.; Buscemi, J.; Buitrago, D.; Iacobelli, F.; Perez-Tamayo, A.; Guitelman, J.; Penedo, F.J.; Yanez, B. Patterns of Use of Smartphone-Based Interventions Among Latina Breast Cancer Survivors: Secondary Analysis of a Pilot Randomized Controlled Trial. JMIR Cancer 2020, 6, e17538. [Google Scholar] [CrossRef]
- Lin, P.-J.; Fang, S.-Y.; Kuo, Y.-L. Development and Usability Testing of a Decision Support App for Women Considering Breast Reconstruction Surgery. J. Canc. Educ. 2021, 36, 160–167. [Google Scholar] [CrossRef]
- Ponder, M.; Venkatraman, V.; Charalambous, L.; Ansah-Yeboah, A.A.; Adil, S.M.; Antezana, L.A.; Dharmapurikar, R.; Gellad, Z.F.; Lad, S.P.; Hwang, E.S.; et al. Mobile Health Application for Patients Undergoing Breast Cancer Surgery: Feasibility Study. JCO Oncol. Pract. 2021, 17, e1344–e1353. [Google Scholar] [CrossRef]
- Yu, J.; Wu, J.; Huang, O.; Chen, X.; Shen, K. A Smartphone-Based App to Improve Adjuvant Treatment Adherence to Multidisciplinary Decisions in Patients with Early-Stage Breast Cancer: Observational Study. J. Med. Internet Res. 2021, 23, e27576. [Google Scholar] [CrossRef]
- Voorberg, W.H.; Bekkers, V.J.J.M.; Tummers, L.G. A Systematic Review of Co-Creation and Co-Production: Embarking on the Social Innovation Journey. Public Manag. Rev. 2015, 17, 1333–1357. [Google Scholar] [CrossRef]
- Eyles, H.; Jull, A.; Dobson, R.; Firestone, R.; Whittaker, R.; Te Morenga, L.; Goodwin, D.; Mhurchu, C.N. Co-Design of mHealth Delivered Interventions: A Systematic Review to Assess Key Methods and Processes. Curr. Nutr. Rep. 2016, 5, 160–167. [Google Scholar] [CrossRef]
- Eccher, C.; Gios, L.; Zanutto, A.; Bizzarri, G.; Conforti, D.; Forti, S. TreC Platform. An Integrated and Evolving Care Model for Patients’ Empowerment and Data Repository. J. Biomed. Inform. 2020, 102, 103359. [Google Scholar] [CrossRef] [PubMed]
- Ferro, A.; Preti, L.M.; Eccher, C.; Maimone, R. Sviluppo Ed Applicazione Di Strumenti Di Telemedicina All’interno Del Percorso Delle Pazienti Con Tumore Mammario in Fase Precoce: Dalla Diagnosi al Follow-Up. Mecosan Manag. Ed Econ. Sanit. 2023, 127, 43–66. [Google Scholar] [CrossRef]
- Bjelic-Radisic, V.; Cardoso, F.; Cameron, D.; Brain, E.; Kuljanic, K.; Da Costa, R.A.; Conroy, T.; Inwald, E.C.; Serpentini, S.; Pinto, M.; et al. An International Update of the EORTC Questionnaire for Assessing Quality of Life in Breast Cancer Patients: EORTC QLQ-BR45. Ann. Oncol. 2020, 31, 283–288. [Google Scholar] [CrossRef]
- Balestroni, G.; Bertolotti, G. EuroQol-5D (EQ-5D): An Instrument for Measuring Quality of Life. Monaldi Arch. Chest Dis. 2015, 78, 155–159. [Google Scholar] [CrossRef]
- Wheelwright, S.; Darlington, A.-S.; Fitzsimmons, D.; Fayers, P.; Arraras, J.I.; Bonnetain, F.; Brain, E.; Bredart, A.; Chie, W.-C.; On behalf of the EORTC Quality of Life Group; et al. International Validation of the EORTC QLQ-ELD14 Questionnaire for Assessment of Health-Related Quality of Life Elderly Patients with Cancer. Br. J. Cancer 2013, 109, 852–858. [Google Scholar] [CrossRef]
- Ferro, A.; Campora, M.; Caldara, A.; De Lisi, D.; Lorenzi, M.; Monteverdi, S.; Mihai, R.; Bisio, A.; Dipasquale, M.; Caffo, O.; et al. Novel Treatment Strategies for Hormone Receptor (HR)-Positive, HER2-Negative Metastatic Breast Cancer. J. Clin. Med. 2024, 13, 3611. [Google Scholar] [CrossRef]
- Kalinsky, K.; Accordino, M.K.; Chiuzan, C.; Mundi, P.S.; Sakach, E.; Sathe, C.; Ahn, H.; Trivedi, M.S.; Novik, Y.; Tiersten, A.; et al. Randomized Phase II Trial of Endocrine Therapy With or Without Ribociclib After Progression on Cyclin-Dependent Kinase 4/6 Inhibition in Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative Metastatic Breast Cancer: MAINTAIN Trial. J. Clin. Oncol. 2023, 41, 4004–4013. [Google Scholar] [CrossRef]
- Kalinsky, K.; Bianchini, G.; Hamilton, E.P.; Graff, S.L.; Park, K.H.; Jeselsohn, R.; Demirci, U.; Martin, M.; Layman, R.M.; Hurvitz, S.A.; et al. Abemaciclib plus Fulvestrant vs. Fulvestrant Alone for HR+, HER2- Advanced Breast Cancer Following Progression on a Prior CDK4/6 Inhibitor plus Endocrine Therapy: Primary Outcome of the Phase 3 postMONARCH Trial. J. Clin. Oncol. 2024, 42, 1101–1112. [Google Scholar] [CrossRef]
- André, F.; Ciruelos, E.M.; Juric, D.; Loibl, S.; Campone, M.; Mayer, I.A.; Rubovszky, G.; Yamashita, T.; Kaufman, B.; Lu, Y.-S.; et al. Alpelisib plus Fulvestrant for PIK3CA-Mutated, Hormone Receptor-Positive, Human Epidermal Growth Factor Receptor-2–Negative Advanced Breast Cancer: Final Overall Survival Results from SOLAR-1. Ann. Oncol. 2021, 32, 208–217. [Google Scholar] [CrossRef]
- Turner, N.C.; Oliveira, M.; Howell, S.J.; Dalenc, F.; Cortes, J.; Gomez Moreno, H.L.; Hu, X.; Jhaveri, K.; Krivorotko, P.; Loibl, S.; et al. Capivasertib in Hormone Receptor–Positive Advanced Breast Cancer. N. Engl. J. Med. 2023, 388, 2058–2070. [Google Scholar] [CrossRef] [PubMed]
- Robson, M.; Im, S.-A.; Senkus, E.; Xu, B.; Domchek, S.M.; Masuda, N.; Delaloge, S.; Li, W.; Tung, N.; Armstrong, A.; et al. Olaparib for Metastatic Breast Cancer in Patients with a Germline BRCA Mutation. N. Engl. J. Med. 2017, 377, 523–533. [Google Scholar] [CrossRef]
- Litton, J.K.; Hurvitz, S.A.; Mina, L.A.; Rugo, H.S.; Lee, K.-H.; Gonçalves, A.; Diab, S.; Woodward, N.; Goodwin, A.; Yerushalmi, R.; et al. Talazoparib versus Chemotherapy in Patients with Germline BRCA1/2-Mutated HER2-Negative Advanced Breast Cancer: Final Overall Survival Results from the EMBRACA Trial. Ann. Oncol. 2020, 31, 1526–1535. [Google Scholar] [CrossRef]
- Litton, J.K.; Rugo, H.S.; Ettl, J.; Hurvitz, S.A.; Gonçalves, A.; Lee, K.-H.; Fehrenbacher, L.; Yerushalmi, R.; Mina, L.A.; Martin, M.; et al. Talazoparib in Patients with Advanced Breast Cancer and a Germline BRCA Mutation. N. Engl. J. Med. 2018, 379, 753–763. [Google Scholar] [CrossRef]
- Passardi, A.; Foca, F.; Caffo, O.; Tondini, C.A.; Zambelli, A.; Vespignani, R.; Bartolini, G.; Sullo, F.G.; Andreis, D.; Dianti, M.; et al. A Remote Monitoring System to Optimize the Home Management of Oral Anticancer Therapies (ONCO-TreC): Prospective Training–Validation Trial. J. Med. Internet Res. 2022, 24, e27349. [Google Scholar] [CrossRef]
- Dragoni, M.; Eccher, C.; Ferro, A.; Bailoni, T.; Maimone, R.; Zorzi, A.; Bacchiega, A.; Stulzer, G.; Ghidini, C. Supporting Patients and Clinicians during the Breast Cancer Care Path with AI: The Arianna Solution. Artif. Intell. Med. 2023, 138, 102514. [Google Scholar] [CrossRef]
- Moreno, P.I.; Horner, F.S.; Torzewski, J.B.; Thomas, J.L.; Gradishar, W.; Victorson, D.; Penedo, F.J. Study Design and Protocol for Tailored Acceptance and Commitment Therapy (ACT) to Optimize Quality of Life in Women Living with Metastatic Breast Cancer. Contemp. Clin. Trials Commun. 2022, 25, 100870. [Google Scholar] [CrossRef]
- Thorne, S.; Oliffe, J.L.; Stajduhar, K.I. Communicating Shared Decision-Making: Cancer Patient Perspectives. Patient Educ. Couns. 2013, 90, 291–296. [Google Scholar] [CrossRef]
- Murray, E.; Lo, B.; Pollack, L.; Donelan, K.; Catania, J.; White, M.; Zapert, K.; Turner, R. The Impact of Health Information on the Internet on the Physician-Patient Relationship: Patient Perceptions. Arch. Intern. Med. 2003, 163, 1727. [Google Scholar] [CrossRef]
- Bombard, Y.; Baker, G.R.; Orlando, E.; Fancott, C.; Bhatia, P.; Casalino, S.; Onate, K.; Denis, J.-L.; Pomey, M.-P. Engaging Patients to Improve Quality of Care: A Systematic Review. Implement. Sci. 2018, 13, 98. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Kris, M.G.; Scher, H.I.; Hudis, C.A.; Sabbatini, P.; Rogak, L.; Bennett, A.V.; Dueck, A.C.; Atkinson, T.M.; et al. Symptom Monitoring With Patient-Reported Outcomes During Routine Cancer Treatment: A Randomized Controlled Trial. J. Clin. Oncol. 2016, 34, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197. [Google Scholar] [CrossRef] [PubMed]
- Denis, F.; Basch, E.; Septans, A.-L.; Bennouna, J.; Urban, T.; Dueck, A.C.; Letellier, C. Two-Year Survival Comparing Web-Based Symptom Monitoring vs Routine Surveillance Following Treatment for Lung Cancer. JAMA 2019, 321, 306. [Google Scholar] [CrossRef]
- Gussoni, G.; Ravot, E.; Zecchina, M.; Recchia, G.; Santoro, E.; Ascione, R.; Perrone, F. Digital therapeutics in oncology: Findings, barriers and prospects. A narrative review. Ann. Res. Oncol. 2022, 2, 55. [Google Scholar] [CrossRef]
- Nekhlyudov, L.; Duijts, S.; Hudson, S.V.; Jones, J.M.; Keogh, J.; Love, B.; Lustberg, M.; Smith, K.C.; Tevaarwerk, A.; Yu, X.; et al. Addressing the Needs of Cancer Survivors during the COVID-19 Pandemic. J. Cancer Surviv. 2020, 14, 601–606. [Google Scholar] [CrossRef]
- Lewis, J.; Ray, P.; Liaw, S.-T. Recent Worldwide Developments in eHealth and mHealth to More Effectively Manage Cancer and Other Chronic Diseases—A Systematic Review. Yearb. Med. Inf. 2016, 25, 93–108. [Google Scholar] [CrossRef]
- Jiang, Y.; West, B.T.; Barton, D.L.; Harris, M.R. Acceptance and Use of eHealth/mHealth Applications for Self-Management Among Cancer Survivors; Studies in Health Technology and Informatics; IOS Press: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Triberti, S.; Savioni, L.; Sebri, V.; Pravettoni, G. eHealth for Improving Quality of Life in Breast Cancer Patients: A Systematic Review. Cancer Treat. Rev. 2019, 74, 1–14. [Google Scholar] [CrossRef]
- Schuit, A.S.; Zwieten, V.; Holtmaat, K.; Cuijpers, P.; Eerenstein, S.E.J.; Leemans, C.R.; Vergeer, M.R.; Voortman, J.; Karagozoglu, H.; Weert, S.; et al. Symptom Monitoring in Cancer and Fully Automated Advice on Supportive Care: Patients’ Perspectives on Self-management Strategies and the eHealth Self-management Application Oncokompas. Eur. J. Cancer Care 2021, 30, e13497. [Google Scholar] [CrossRef]
- Singleton, A.C.; Raeside, R.; Hyun, K.K.; Partridge, S.R.; Di Tanna, G.L.; Hafiz, N.; Tu, Q.; Tat-Ko, J.; Sum, S.C.M.; Sherman, K.A.; et al. Electronic Health Interventions for Patients with Breast Cancer: Systematic Review and Meta-Analyses. J. Clin. Oncol. 2022, 40, 2257–2270. [Google Scholar] [CrossRef]

| Verbatim | Emerging Theme | |
|---|---|---|
| #1 | I need information about bureaucratic aspects too, like illness and work… | Digital tools for non-clinical informational needs |
| #2 | Having a clear list of direct contacts, I can reach out to… | Digital tools for healthcare contacts |
| #3 | I used a paper calendar where I wrote everything: appointments, exams, therapies… | Digital tools for self-management |
| #4 | Getting info about my clinical pathway is fine, unless it changes and I’m not informed… it’s hard to have a clear plan from the start. | Digital tools for non-clinical informational needs and clinical updates |
| #5 | I used Google Calendar to remind myself to take home medications… | Digital tools for self-management |
| #6 | In the first days after diagnosis, there’s a need to know everything, so we look for information online… | Digital tools for clinical and non-clinical informational needs |
| #7 | A chat with case managers wouldn’t work because they’re already overloaded, and I don’t know how it would be managed… | Digital tools for direct communication |
| #8 | We need not only clinical information, but especially the kind doctors consider secondary… | Digital tools for clinical and non-clinical informational needs (Importance of practical/lifestyle information) |
| #9 | The app could be a tool where I find information that I know is true, consistent, and science-based, without getting mixed answers… | Digital tools for the reliability and consistency of information |
| #10 | If I enter data in a diary and receive feedback, that would be very useful… | Digital tools for recording personal narratives |
| #11 | Yes, I would use the diary as a reminder before the oncologist visit… | Digital tools for recording personal narratives |
| #12 | The informational content should be the top priority… | Digital tools for clinical and non-clinical informational needs |
| #13 | I didn’t use a personal diary, but I would use an app to note my emotions. I wouldn’t want a chatbot telling me how I should feel… | Digital tools for recording personal narratives |
| Level | Functionality | Description |
|---|---|---|
| Dashboard | Activation of credentials for the patient to access the application |
|
| Configuration of parameters that can be entered in the app |
| |
| Display of parameters (dashboard) |
| |
| Activation and use of a chat between doctor/healthcare personnel and patient |
| |
| Therapy reminder setting |
| |
| Configuration of routine reports |
| |
| App | Implementation of a video chat between doctor/healthcare personnel and patient |
|
| Personal observations diary (for patient) |
| |
| Activation of the drug diary |
| |
| Generation of reminders |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferro, A.; Pavesi, M.C.; Pederiva, L.; Eccher, C. TreC_Metha: A Digital Application to Enhance Patient Agency, Therapy Compliance and Quality of Life in Metastatic Breast Cancer Patients. Curr. Oncol. 2025, 32, 299. https://doi.org/10.3390/curroncol32060299
Ferro A, Pavesi MC, Pederiva L, Eccher C. TreC_Metha: A Digital Application to Enhance Patient Agency, Therapy Compliance and Quality of Life in Metastatic Breast Cancer Patients. Current Oncology. 2025; 32(6):299. https://doi.org/10.3390/curroncol32060299
Chicago/Turabian StyleFerro, Antonella, Maria Chiara Pavesi, Lucia Pederiva, and Claudio Eccher. 2025. "TreC_Metha: A Digital Application to Enhance Patient Agency, Therapy Compliance and Quality of Life in Metastatic Breast Cancer Patients" Current Oncology 32, no. 6: 299. https://doi.org/10.3390/curroncol32060299
APA StyleFerro, A., Pavesi, M. C., Pederiva, L., & Eccher, C. (2025). TreC_Metha: A Digital Application to Enhance Patient Agency, Therapy Compliance and Quality of Life in Metastatic Breast Cancer Patients. Current Oncology, 32(6), 299. https://doi.org/10.3390/curroncol32060299