Current Limitations of Sentinel Node Biopsy in Vulvar Cancer



Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Current Indications and Evidence for Sentinel Node Biopsy
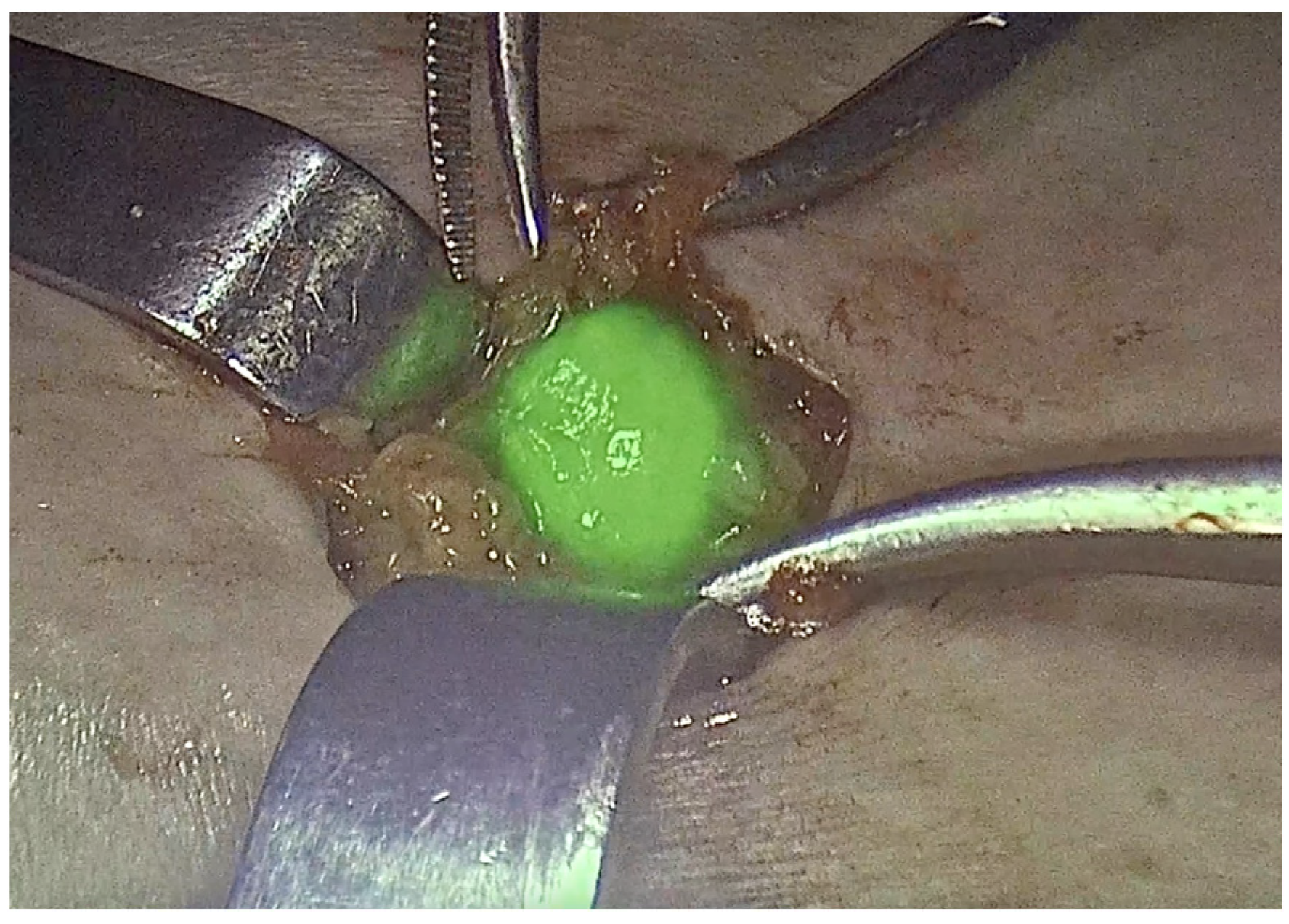
3.2. Surgical Technique of Sentinel Node Biopsy and Available Methods of Detection
3.3. Management of Metastatic Groin Nodes
3.3.1. Volume of Lymph Node Disease
3.3.2. Management of Contralateral Groin
3.4. Extended Indications for Sentinel Node Biopsy
3.4.1. Sentinel Node Biopsy in Recurrent Vulvar Cancer
3.4.2. Sentinel Node Biopsy in >4 cm or Multifocal Tumors
3.5. Potential Barriers and Limitations for Sentinel Node Biopsy
3.6. Future Directions
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Judson, P.L.; Habermann, E.B.; Baxter, N.N.; Durham, S.B.; Virnig, B.A. Trends in the Incidence of Invasive and In Situ Vulvar Carcinoma. Obstet. Gynecol. 2006, 107, 1018–1022. [Google Scholar] [CrossRef] [PubMed]
- Olawaiye, A.B.; Cotler, J.; Cuello, M.A.; Bhatla, N.; Okamoto, A.; Wilailak, S.; Purandare, C.N.; Lindeque, G.; Berek, J.S.; Kehoe, S. FIGO Staging for Carcinoma of the Vulva: 2021 Revision. Int. J. Gynaecol. Obstet. 2021, 155, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Miljanović-Špika, I.; Madunić, M.D.; Topolovec, Z.; Kujadin Kenjereš, D.; Vidosavljević, D. Prognostic Factors for Vulvar Cancer. Acta Clin. Croat. 2021, 60, 25–32. [Google Scholar] [CrossRef]
- Klapdor, R.; Wölber, L.; Hanker, L.; Schmalfeldt, B.; Canzler, U.; Fehm, T.; Luyten, A.; Hellriegel, M.; Kosse, J.; Heiss, C.; et al. Predictive Factors for Lymph Node Metastases in Vulvar Cancer: An Analysis of the AGO-CaRE-1 Multicenter Study. Gynecol. Oncol. 2019, 154, 565–570. [Google Scholar] [CrossRef]
- Cheraghlou, S.; Doudican, N.A.; Criscito, M.C.; Stevenson, M.L.; Carucci, J.A. Defining and Quantifying Histopathologic Risk Factors for Regional and Distant Metastases in a Large Cohort of Vulvar Squamous Cell Carcinomas. J. Am. Acad. Dermatol. 2023, 89, 1022–1030. [Google Scholar] [CrossRef]
- Gaarenstroom, K.N.; Kenter, G.G.; Trimbos, J.B.; Agous, I.; Amant, F.; Peters, A.A.; Vergote, I. Postoperative Complications after Vulvectomy and Inguinofemoral Lymphadenectomy Using Separate Groin Incisions. Int. J. Gynecol. Cancer 2003, 13, 522–527. [Google Scholar] [CrossRef]
- Barlow, E.L.; Donoghoe, M.W.; Hacker, N.F. Morbidity Related to the Groin Lymph Node Dissection for Vulvar Cancer. Int. J. Gynecol. Clin. Pract. 2019, 6, 149. [Google Scholar] [CrossRef]
- Morton, D.L.; Wen, D.R.; Wong, J.H.; Economou, J.S.; Cagle, L.A.; Storm, F.K.; Foshag, L.J.; Cochran, A.J. Technical Details of Intraoperative Lymphatic Mapping for Early-Stage Melanoma. Arch. Surg. 1992, 127, 392–399. [Google Scholar] [CrossRef]
- Cody, H.S., III; Hill, A.D.; Tran, K.N.; Brennan, M.F.; Borgen, P.I. Credentialing for Breast Lymphatic Mapping: How Many Cases Are Enough? Ann. Surg. 1999, 229, 723–728. [Google Scholar] [CrossRef]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP Guidelines for the Management of Patients with Endometrial Carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Decesare, S.L.; Fiorica, J.V.; Roberts, W.S.; Reintgen, D.; Arango, H.; Hoffman, M.S.; Puleo, C.; Cavanagh, D. A Pilot Study Utilizing Intraoperative Lymphoscintigraphy for Identification of the Sentinel Lymph Nodes in Vulvar Cancer. Gynecol. Oncol. 1997, 66, 425–428. [Google Scholar] [CrossRef]
- Van der Zee, A.G.J.; Oonk, M.H.; De Hullu, J.A.; Ansink, A.C.; Vergote, I.; Verheijen, R.H.; Maggioni, A.; Gaarenstroom, K.N.; Baldwin, P.J.; Van Dorst, E.B.; et al. Sentinel Node Dissection Is Safe in the Treatment of Early-Stage Vulvar Cancer. J. Clin. Oncol. 2008, 26, 884–889. [Google Scholar]
- Levenback, C.F.; Ali, S.; Coleman, R.L.; Gold, M.A.; Fowler, J.M.; Judson, P.L.; Bell, M.C.; De Geest, K.; Spirtos, N.M.; Potkul, R.K.; et al. Lymphatic Mapping and Sentinel Lymph Node Biopsy in Women with Squamous Cell Carcinoma of the Vulva: A Gynecologic Oncology Group Study. J. Clin. Oncol. 2012, 30, 3786–3791. [Google Scholar] [CrossRef] [PubMed]
- Meads, C.; Sutton, A.; Małysiak, S.; Kowalska, M.; Zapalska, A.; Rogozinska, E.; Baldwin, P.; Rosenthal, A.; Ganesan, R.; Borowiack, E.; et al. Sentinel Lymph Node Status in Vulval Cancer: Systematic Reviews of Test Accuracy and Decision-Analytic Model-Based Economic Evaluation. Health Technol. Assess. 2013, 17, 1–216. [Google Scholar] [CrossRef]
- Hassanzade, M.; Attaran, M.; Treglia, G.; Yousefi, Z.; Sadeghi, R. Lymphatic mapping and sentinel node biopsy in squamous cell carcinoma of the vulva: Systematic review and meta-analysis of the literature. Gynecol. Oncol. 2013, 130, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Oonk, M.H.M.; Planchamp, F.; Baldwin, P.; Mahner, S.; Mirza, M.R.; Fischerová, D.; Creutzberg, C.L.; Guillot, E.; Garganese, G.; Lax, S.; et al. European Society of Gynaecological Oncology Guidelines for the Management of Patients with Vulvar Cancer—Update 2023. Int. J. Gynecol. Cancer 2023, 33, 1023–1043. [Google Scholar] [CrossRef]
- Abu-Rustum, N.R.; Yashar, C.M.; Arend, R.; Barber, E.; Bradley, K.; Brooks, R.; Campos, S.M.; Chino, J.; Chon, H.S.; Crispens, M.A.; et al. Vulvar Cancer, Version 3.2024, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2024, 22, 117–135. [Google Scholar] [CrossRef]
- Deken, M.M.; van Doorn, H.C.; Verver, D.; Boogerd, L.S.; de Valk, K.S.; Rietbergen, D.D.; van Poelgeest, M.I.; de Kroon, C.D.; Beltman, J.J.; van Leeuwen, F.W.; et al. Near-Infrared Fluorescence Imaging Compared to Standard Sentinel Lymph Node Detection with Blue Dye in Patients with Vulvar Cancer—A Randomized Controlled Trial. Gynecol. Oncol. 2020, 159, 672–680. [Google Scholar] [CrossRef]
- Di Donna, M.C.; Quartuccio, N.; Giallombardo, V.; Sturiale, L.; Arnone, A.; Ricapito, R.; Sozzi, G.; Arnone, G.; Chiantera, V. Detection of sentinel lymph node in vulvar cancer using 99mTc-labeled Colloid lymphoscintigraphy, blue dye, and indocyanine-green fluorescence: A meta-analysis of studies published in 2010–2020. Arch. Gynecol. Obstet. 2023, 307, 1677–1686. [Google Scholar] [CrossRef]
- Van der Kolk, W.L.; Van der Zee, A.G.J.; Slomovitz, B.M.; Baldwin, P.; Van Doorn, H.; De Hullu, J.; Van der Velden, J.; Gaarenstroom, K.; Kjolhede, P.; Brännström, M.; et al. Unilateral Inguinofemoral Lymphadenectomy in Patients with Early-Stage Vulvar Squamous Cell Carcinoma and a Unilateral Metastatic Sentinel Lymph Node Is Safe. Gynecol. Oncol. 2022, 167, 3–10. [Google Scholar]
- De Cicco, C.; Sideri, M.; Bartolomei, M.; Grana, C.; Cremonesi, M.; Fiorenza, M.; Maggioni, A.; Bocciolone, L.; Mangioni, C.; Colombo, N.; et al. Sentinel node biopsy in early vulvar cancer. Br. J. Cancer 2000, 82, 295–299. [Google Scholar] [CrossRef]
- De Hullu, J.A.; Piers, D.A.; Hollema, H.; Aalders, J.G.; Van der Zee, A.G.J. Sentinel lymph node detection in locally recurrent carcinoma of the vulva. BJOG Int. J. Obstet. Gynaecol. 2001, 108, 766–768. [Google Scholar]
- Levenback, C.; Coleman, R.L.; Burke, T.W.; Bodurka-Bevers, D.; Wolf, J.K.; Gershenson, D.M. Intraoperative lymphatic mapping and sentinel node identification with blue dye in patients with vulvar cancer. Gynecol. Oncol. 2001, 83, 276–281. [Google Scholar] [CrossRef]
- Hauspy, J.; Beiner, M.; Harley, I.; Ehrlich, L.; Rasty, G.; Covens, A. Sentinel lymph node in vulvar cancer. Cancer 2007, 110, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Hampl, M.; Hantschmann, P.; Michels, W.; Hillemanns, P.; German Multicenter Study Group. Validation of the accuracy of the sentinel lymph node procedure in patients with vulvar cancer: Results of a multicenter study in Germany. Gynecol. Oncol. 2008, 111, 282–288. [Google Scholar] [CrossRef]
- Te Grootenhuis, N.C.; van der Zee, A.G.; van Doorn, H.C.; van der Velden, J.; Vergote, I.; Zanagnolo, V.; Baldwin, P.J.; Gaarenstroom, K.N.; van Dorst, E.B.; Trum, J.W.; et al. Sentinel nodes in vulvar cancer: Long-term follow-up of the GROningen INternational Study on Sentinel nodes in Vulvar cancer (GROINSS-V) I. Gynecol. Oncol. 2016, 140, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Covens, A.; Vella, E.T.; Kennedy, E.B.; Reade, C.J.; Jimenez, W.; Le, T. Sentinel lymph node biopsy in vulvar cancer: Systematic review, meta-analysis and guideline recommendations. Gynecol. Oncol. 2015, 137, 351–361. [Google Scholar] [CrossRef]
- Robison, K.; Roque, D.; McCourt, C.; Stuckey, A.; DiSilvestro, P.A.; Sung, C.J.; Steinhoff, M.; Granai, C.O.; Moore, R.G. Long-term follow-up of vulvar cancer patients evaluated with sentinel lymph node biopsy alone. Gynecol. Oncol. 2014, 133, 416–420. [Google Scholar] [CrossRef]
- Greer, B.E.; Koh, W. New NCCN Guidelines for Vulvar Cancer. J. Natl. Compr. Canc. Netw. 2016, 14, 656–658. [Google Scholar]
- Kanbergs, A.; Melamed, A.; Viveros-Carreño, D.; Wu, C.F.; Wilke, R.N.; Zamorano, A.; Paladuga, K.; Havrilesky, L.; Rauh-Hain, J.A.; Agusti, N. Surgical Deescalation Within Gynecologic Oncology. JAMA Netw. Open 2025, 8, e2453604. [Google Scholar] [CrossRef] [PubMed]
- Erickson, B.K.; Divine, L.M.; Leath, C.A.; Straughn, J.M. Cost-Effectiveness Analysis of Sentinel Lymph Node Biopsy in the Treatment of Early-Stage Vulvar Cancer. Int. J. Gynecol. Cancer 2014, 24, 1480–1485. [Google Scholar] [CrossRef] [PubMed]
- McCann, G.A.; Cohn, D.E.; Jewell, E.L.; Havrilesky, L.J. Lymphatic Mapping and Sentinel Lymph Node Dissection Compared to Complete Lymphadenectomy in the Management of Early-Stage Vulvar Cancer: A Cost-Utility Analysis. Gynecol. Oncol. 2015, 136, 300–304. [Google Scholar] [CrossRef]
- Ramirez, P.T.; Frumovitz, M.; Abu-Rustum, N.R. Principles of Gynecologic Oncology Surgery; Elsevier: Philadelphia, PA, USA, 2019. [Google Scholar]
- Collins, A.; Phillips, A. Sentinel Lymph Node Mapping in the Modern Management of Gynaecological Malignancy. Obstet. Gynaecol. 2023, 25, 210–219. [Google Scholar] [CrossRef]
- Penn, C.A.; Schneiter, M.K.; Watson, C.H. Advances in Ovarian Cancer Treatment: A Review of Current Therapeutic Approaches. Curr. Treat. Options Oncol. 2024, 25, 20–26. [Google Scholar] [CrossRef]
- Broach, V.; Abu-Rustum, N.R.; Sonoda, Y.; Brown, C.L.; Jewell, E.; Gardner, G.; Chi, D.S.; Zivanovic, O.; Leitao, M.M., Jr. Fertility-sparing surgery for early-stage cervical cancer: Oncologic and obstetric outcomes. Int. J. Gynecol. Cancer 2020, 30, 383–386. [Google Scholar] [CrossRef]
- Crane, L.M.A.; Themelis, G.; Buddingh, K.T.; Harlaar, N.J.; Pleijhuis, R.G.; Sarantopoulos, A.; van der Zee, A.G.; Ntziachristos, V.; van Dam, G.M. Intraoperative near-infrared fluorescence imaging for sentinel lymph node detection in vulvar cancer: A pilot study. J. Vis. Exp. 2010, 44, e2225. [Google Scholar] [CrossRef]
- Crane, L.M.A.; Themelis, G.; Pleijhuis, R.G.; Harlaar, N.J.; Sarantopoulos, A.; Arts, H.J.; van der Zee, A.G.; Ntziachristos, V.; van Dam, G.M. Intraoperative near-infrared fluorescence imaging for sentinel lymph node detection in vulvar cancer: First clinical results. Gynecol. Oncol. 2011, 120, 291–295. [Google Scholar] [CrossRef]
- Soergel, P.; Hertel, H.; Nacke, A.K.; Klapdor, R.; Derlin, T.; Hillemanns, P. Sentinel Lymphadenectomy in Vulvar Cancer Using Near-Infrared Fluorescence From Indocyanine Green Compared With Technetium 99m Nanocolloid. Int. J. Gynecol. Cancer 2017, 27, 805–812. [Google Scholar] [CrossRef]
- Koual, M.; Benoit, L.; Nguyen-Xuan, H.T.; Bentivegna, E.; Azaïs, H.; Bats, A.S. Diagnostic Value of Indocyanine Green Fluorescence Guided Sentinel Lymph Node Biopsy in Vulvar Cancer: A Systematic Review. Gynecol. Oncol. 2021, 161, 436–441. [Google Scholar] [CrossRef]
- Prader, S.; du Bois, A.; Harter, P.; Breit, E.; Schneider, S.; Baert, T.; Heitz, F.; Traut, A.; Ehmann, S.; Pauly, N.; et al. Sentinel Lymph Node Mapping with Fluorescent and Radioactive Tracers in Vulvar Cancer Patients. Arch. Gynecol. Obstet. 2020, 301, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, F.P.; Tummers, Q.R.; Rietbergen, D.D.; Peters, A.A.; Schaafsma, B.E.; van de Velde, C.J.; Frangioni, J.V.; van Leeuwen, F.W.; Gaarenstroom, K.N.; Vahrmeijer, A.L. Sentinel Lymph Node Biopsy in Vulvar Cancer Using Combined Radioactive and Fluorescence Guidance. Int. J. Gynecol. Cancer 2015, 25, 1086–1093. [Google Scholar] [CrossRef]
- Jedryka, M.; Kryszpin, M.; Manowiec, M.; Rossochacka-Rostalska, B.; Kalus, M.; Klimczak, P. 100 A new technique of sentinel lymph nodes detection in vulvar cancer patients. The sarvu study. Int. J. Gynecol. Cancer 2019, 29, A1–A197. [Google Scholar]
- Cote, R.J.; Fpeterson, H.; Chaiwun, B.; Gelber, R.D.; Goldhirsch, A.; Castiglione-Gertsch, M.; Gusterson, B.; Neville, A.M. Role of immunohistochemical detection of lymph-node metastases in management of breast cancer. Lancet 1999, 354, 896–900. [Google Scholar] [CrossRef]
- Bézu, C.; Coutant, C.; Ballester, M.; Feron, J.G.; Rouzier, R.; Uzan, S.; Daraï, E. Ultrastaging of lymph node in uterine cancers. J. Exp. Clin. Cancer Res. 2010, 29, 5. [Google Scholar] [CrossRef]
- Rychlik, A.; Bidzinski, M.; Rzepka, J.; Piatek, S. Sentinel lymph node biopsy in cervical cancer: Current clinical evidence and future perspectives. Chin. Clin. Oncol. 2021, 10, 19. [Google Scholar] [CrossRef]
- Mahner, S.; Jueckstock, J.; Hilpert, F.; Neuser, P.; Harter, P.; de Gregorio, N.; Hasenburg, A.; Sehouli, J.; Habermann, A.; Hillemanns, P.; et al. Adjuvant Therapy in Lymph Node-Positive Vulvar Cancer: The AGO-CaRE-1 Study. J. Natl. Cancer Inst. 2015, 107, dju426. [Google Scholar] [CrossRef] [PubMed]
- Oonk, M.H.; van Hemel, B.M.; Hollema, H.; de Hullu, J.A.; Ansink, A.C.; Vergote, I.; Verheijen, R.H.; Maggioni, A.; Gaarenstroom, K.N.; Baldwin, P.J.; et al. Sentinel node biopsy versus complete lymphadenectomy in early-stage vulvar cancer: A randomized trial. Lancet Oncol. 2010, 11, 646–652. [Google Scholar] [CrossRef]
- Oonk, M.H.M.; Slomovitz, B.; Baldwin, P.J.W.; van Doorn, H.C.; van der Velden, J.; de Hullu, J.A.; Gaarenstroom, K.N.; Slangen, B.F.M.; Vergote, I.; Brännström, M.; et al. Radiotherapy Versus Inguinofemoral Lymphadenectomy as Treatment for Vulvar Cancer Patients with Micrometastases in the Sentinel Node: Results of GROINSS-V II. J. Clin. Oncol. 2021, 39, 3623–3632. [Google Scholar] [CrossRef]
- Gien, L.T.; Slomovitz, B.; Van der Zee, A.; Oonk, M. Phase II Activity Trial of High-Dose Radiation and Chemosensitization in Patients with Macrometastatic Lymph Node Spread after Sentinel Node Biopsy in Vulvar Cancer: GROningen INternational Study on Sentinel Nodes in Vulvar Cancer III (GROINSS-V III/NRG-GY024). Int. J. Gynecol. Cancer 2023, 33, 619–622. [Google Scholar] [CrossRef]
- Woelber, L.; Eulenburg, C.; Grimm, D.; Trillsch, F.; Bohlmann, I.; Burandt, E.; Dieckmann, J.; Klutmann, S.; Schmalfeldt, B.; Mahner, S.; et al. The Risk of Contralateral Non-Sentinel Metastasis in Patients with Primary Vulvar Cancer and Unilaterally Positive Sentinel Node. Ann. Surg. Oncol. 2016, 23, 2508–2514. [Google Scholar] [PubMed]
- Nica, A.; Covens, A.; Vicus, D.; Kupets, R.; Osborne, R.; Cesari, M.; Gien, L.T. Sentinel Lymph Nodes in Vulvar Cancer: Management Dilemmas in Patients with Positive Nodes and Larger Tumors. Gynecol. Oncol. 2019, 152, 94–100. [Google Scholar] [PubMed]
- Ignatov, T.; Gaßner, J.; Bozukova, M.; Ivros, S.; Mészáros, J.; Ortmann, O.; Eggemann, H.; Ignatov, A. Contralateral Lymph Node Metastases in Patients with Vulvar Cancer and Unilateral Sentinel Lymph Node Metastases. Acta Obstet. Gynecol. Scand. 2021, 100, 1520–1525. [Google Scholar]
- Winarno, A.S.; Mondal, A.; Martignoni, F.C.; Fehm, T.N.; Hampl, M. The Potential Risk of Contralateral Non-Sentinel Groin Node Metastasis in Women with Early Primary Vulvar Cancer Following Unilateral Sentinel Node Metastasis: A Single Center Evaluation in University Hospital of Düsseldorf. BMC Womens Health 2021, 21, 23. [Google Scholar] [CrossRef] [PubMed]
- van Doorn, H.C.; van Beekhuizen, H.J.; Gaarenstroom, K.N.; van der Velden, J.; van der Zee, A.G.; Oonk, M.H.; de Hullu, J.A. Repeat sentinel lymph node procedure in patients with recurrent vulvar squamous cell carcinoma is feasible. Gynecol. Oncol. 2016, 140, 415–419. [Google Scholar]
- Landkroon, A.P.; de Hullu, J.A.; Ansink, A.C. Repeat Sentinel Lymph Node Procedure in Vulval Carcinoma. BJOG 2006, 113, 1333–1336. [Google Scholar] [CrossRef]
- van Doorn, H.C.; Oonk, M.H.M.; Fons, G.; Gaarenstroom, K.N.; de Hullu, J.; van Rosmalen, J.; van Beekhuizen, H.J. Sentinel Lymph Node Procedure in Patients with Recurrent Vulvar Squamous Cell Carcinoma: A Proposed Protocol for a Multicentre Observational Study. BMC Cancer 2022, 22, 445. [Google Scholar] [CrossRef]
- Garganese, G.; Collarino, A.; Fragomeni, S.M.; Rufini, V.; Perotti, G.; Gentileschi, S.; Evangelista, M.T.; Ieria, F.P.; Zagaria, L.; Bove, S.; et al. Groin sentinel node biopsy and 18F-FDG PET/CT-supported preoperative lymph node assessment in cN0 patients with vulvar cancer currently unfit for minimally invasive inguinal surgery: The GroSNaPET study. Eur. J. Surg. Oncol. 2017, 43, 1776–1783. [Google Scholar] [CrossRef] [PubMed]
- Zach, D.; Stenström Bohlin, K.; Kannisto, P.; Moberg, L.; Kjölhede, P. Time to Extend the Indication for Sentinel Node Biopsy in Vulvar Cancer? Results from a Prospective Nationwide Swedish Study. Int. J. Gynecol. Cancer 2023, 33, 1845–1852. [Google Scholar]
- Swift, B.E.; Tigert, M.; Nica, A.; Covens, A.; Vicus, D.; Parra-Herran, C.; Kupets, R.; Osborne, R.; Gien, L.T. The accuracy of intraoperative frozen section examination of sentinel lymph nodes in squamous cell cancer of the vulva. Gynecol. Oncol. 2022, 164, 393–397. [Google Scholar] [CrossRef]
- Di Donna, M.C.; Cucinella, G.; Giallombardo, V.; Balbo, G.L.; Capozzi, V.A.; Sozzi, G.; Buono, N.; Borsellino, L.; Giannini, A.; Laganà, A.S.; et al. Surgical outcomes and morbidity in open and videoendoscopic inguinal lymphadenectomy in vulvar cancer: A systematic review and metanalysis”. Eur. J. Surg. Oncol. 2024, 51, 108744. [Google Scholar] [CrossRef] [PubMed]
- Naldini, A.; Vizzielli, G.; Perrone, E.; Gallotta, V.; Scambia, G. Robotic video endoscopic inguinal lymphadenectomy (R-VEIL) for vulvar cancer with sentinel node mapping using indocyanine green and near-infrared fluorescence imaging technology. Gynecol. Oncol. 2018, 150, 203–204. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, A.; Hunter, M.I. Robot-assisted Sentinel Lymph Node Mapping and Inguinal Lymph Node Dissection Using Near-infrared Fluorescence in Vulvar Cancer. J. Minim. Invasive Gynecol. 2019, 26, 968–972. [Google Scholar] [CrossRef]

{kind=link}
| Author (Year) | Number of Patients | SLNB Technique | Identification Rate (%) | False Negatives (%) | Median Follow-Up (Months) | Groin Recurrences (%) | Outcome in SLN Negative Patients (%) |
|---|---|---|---|---|---|---|---|
| Van der Zee (2008) [13] | 403 | R + BD | 97 | 3.3 | 35 (2–87) | 2.3 (unifocal) 3 (including multifocal) | 97 3-year DSS |
| Levenback (2012) [14] | 452 | R + BD | 92.5 | 3.7 | NA | NA | NA |
| Robinson (2014) [29] | 69 | R + BD | 93 | NA | 58.3 | 4.7 | NA |
| Grootenhuis (2016) [27] | 377 | R + BD | 95 | 3.5 | 105 (0–179) | 2.5 (unifocal) | 93.5 5-year DSS 90.8 10-year DSS |
| Klapdor (2019) [5] | 772 | R or BD | 94.7 | 5.8 | 33 (0–156) | 4.5 | 82.7 3-year PFS 92.7 3-year OS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gracia, M.; Alonso-Espías, M.; Zapardiel, I. Current Limitations of Sentinel Node Biopsy in Vulvar Cancer. Curr. Oncol. 2025, 32, 215. https://doi.org/10.3390/curroncol32040215
Gracia M, Alonso-Espías M, Zapardiel I. Current Limitations of Sentinel Node Biopsy in Vulvar Cancer. Current Oncology. 2025; 32(4):215. https://doi.org/10.3390/curroncol32040215
Chicago/Turabian StyleGracia, Myriam, Maria Alonso-Espías, and Ignacio Zapardiel. 2025. "Current Limitations of Sentinel Node Biopsy in Vulvar Cancer" Current Oncology 32, no. 4: 215. https://doi.org/10.3390/curroncol32040215
APA StyleGracia, M., Alonso-Espías, M., & Zapardiel, I. (2025). Current Limitations of Sentinel Node Biopsy in Vulvar Cancer. Current Oncology, 32(4), 215. https://doi.org/10.3390/curroncol32040215