Salvage Ultrasound-Guided Robot-Assisted Video-Endoscopic Inguinal Lymphadenectomy (RAVEIL) as a Metastasis-Directed Therapy (MDT) in Oligoprogressive Metastatic Castration-Resistant Prostate Cancer (mCRPC): A Case Report and Review of the Literature



Abstract
1. Introduction
2. Case Presentation
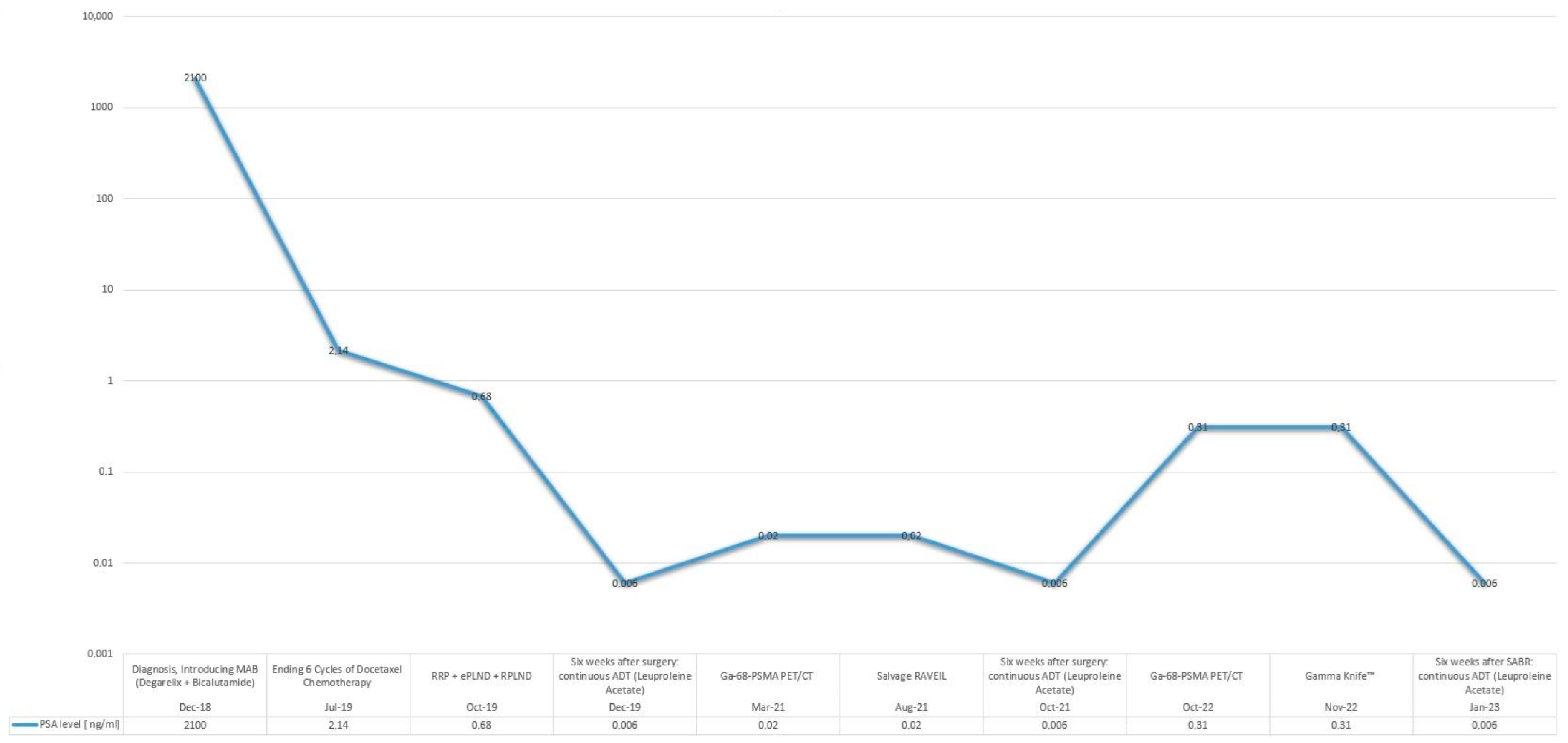
2.1. Initial Management
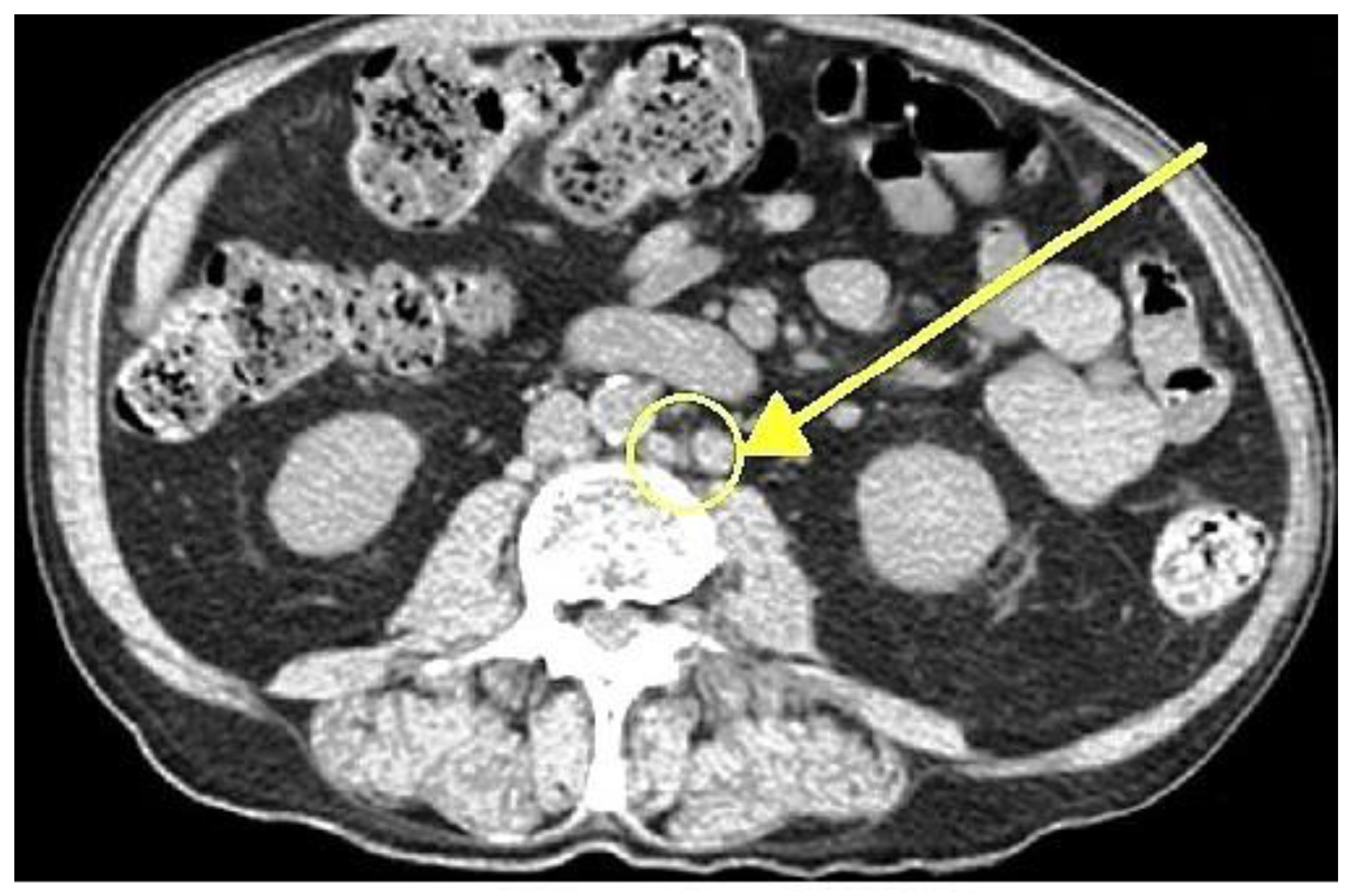
2.2. Detection of Disease Progression
2.3. Preoperative Evaluation and Targeting
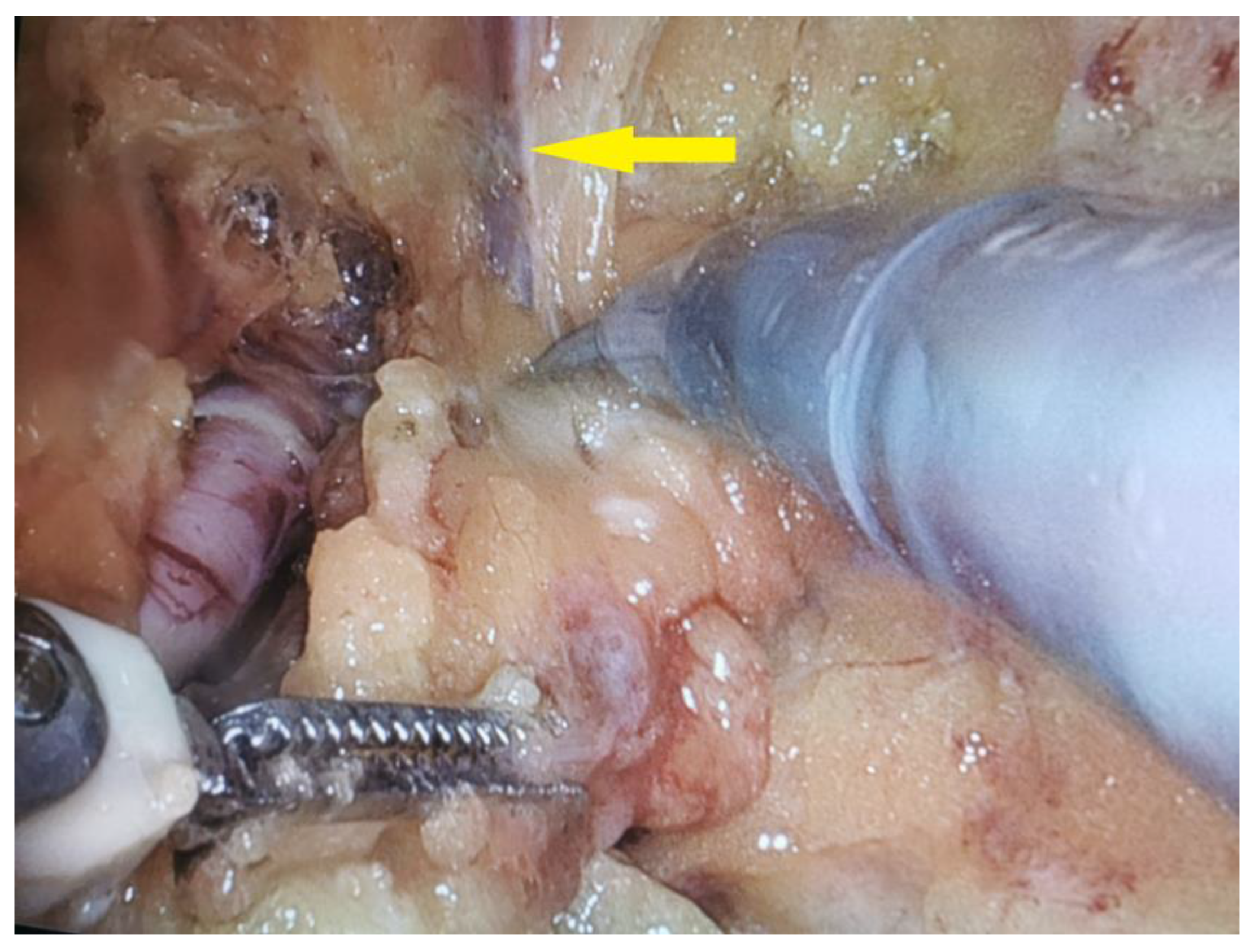
2.4. Salvage Surgical Intervention
2.5. Postoperative Course and Complications
2.6. Follow-Up
3. Discussion
3.1. Clinical and Economic Justification of Using RAVEIL in Oligoprogressive mCRPC
3.1.1. Rationale Behind Selection of Robot-Assisted Surgery
3.1.2. Expected Benefits Compared to Conventional Surgery
3.1.3. Balancing Clinical Advantages and Economic Burden of Robotic Surgery in Highly Selected Cases of Oligoprogressive mCRPC
3.2. Evidence Supporting Surgical Interventions and Their Clinical Impact in CRPC
3.3. The Role of Multidisciplinary Teams in Managing Oligoprogressive mCRPC
3.4. Limitations and Future Directions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Steuber, T.; Jilg, C.; Tennstedt, P.; De Bruycker, A.; Tilki, D.; Decaestecker, K.; Zilli, T.; Jereczek-Fossa, B.A.; Wetterauer, U.; Grosu, A.L.; et al. Standard of Care Versus Metastases-Directed Therapy for PET-Detected Nodal Oligorecurrent Prostate Cancer Following Multimodality Treatment: A Multi-Institutional Case-Control Study. Eur. Urol. Focus 2019, 5, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- De Bleser, E.; Jereczek-Fossa, B.A.; Pasquier, D.; Zilli, T.; Van As, N.; Siva, S.; Fodor, A.; Dirix, P.; Gomez-Iturriaga, A.; Trippa, F.; et al. Metastasis-Directed Therapy in Treating Nodal Oligorecurrent Prostate Cancer: A Multi-Institutional Analysis Comparing the Outcome and Toxicity of Stereotactic Body Radiotherapy and Elective Nodal Radiotherapy. Eur. Urol. 2019, 76, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Ost, P.; Reynders, D.; Decaestecker, K.; Fonteyne, V.; Lumen, N.; De Bruycker, A.; Lambert, B.; Delrue, L.; Bultijnck, R.; Claeys, T.; et al. Surveillance or Metastasis-Directed Therapy for Oligometastatic Prostate Cancer Recurrence: A Prospective, Randomized, Multicenter Phase II Trial. J. Clin. Oncol. 2018, 36, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Phillips, R.; Shi, W.Y.; Deek, M.; Radwan, N.; Lim, S.J.; Antonarakis, E.S.; Rowe, S.P.; Ross, A.E.; Gorin, M.A.; Deville, C.; et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol. 2020, 6, 650–659. [Google Scholar] [CrossRef]
- ClinicalTrials.gov. START-MET: Stereotactic Body Radiotherapy and Androgen Deprivation Therapy for Oligometastatic Prostate Cancer (NCT05209243). Available online: https://clinicaltrials.gov/study/NCT05209243 (accessed on 9 February 2025).
- ClinicalTrials.gov. PRESTO: Prostate-Specific Antigen (PSA) Response Evaluation for Streamlining Trial Optimization (NCT04115007). Available online: https://clinicaltrials.gov/study/NCT04115007 (accessed on 9 February 2025).
- de Barros, H.A.; van Oosterom, M.N.; Donswijk, M.L.; Hendrikx, J.J.; Vis, A.N.; Maurer, T.; van Leeuwen, F.W.; van der Poel, H.G.; van Leeuwen, P.J. Robot-assisted PSMA-radioguided salvage surgery in recurrent prostate cancer using a DROP-IN gamma probe: The first prospective feasibility study. Eur. Urol. 2022, 82, 97–105. [Google Scholar] [CrossRef]
- Kwan, E.M.; Spain, L.; Anton, A.; Gan, C.L.; Garrett, L.; Chang, D.; Liow, E.; Bennett, C.; Zheng, T.; Yu, J.; et al. Avelumab Combined with Stereotactic Ablative Body Radiotherapy in Metastatic Castration-Resistant Prostate Cancer: The Phase 2 ICE-PAC Clinical Trial. Eur. Urol. 2022, 81, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Orme, J.J.; Abraha, F.; Stish, B.J.; Lowe, V.J.; Lucien, F.; Tryggestad, E.J.; Bold, M.S.; Pagliaro, L.C.; Choo, C.R.; et al. Phase II Evaluation of 8Stereotactic Ablative Radiotherapy (SABR) and Immunity in 11C-Choline-PET/CT–Identified Oligometastatic Castration-Resistant Prostate Cancer. Clin. Cancer Res. 2021, 27, 6376–6383. [Google Scholar] [CrossRef] [PubMed]
- Onal, C.; Ozyigit, G.; Oymak, E.; Guler, O.C.; Tilki, B.; Hurmuz, P.; Akyol, F. Stereotactic radiotherapy to oligoprogressive lesions detected with 68Ga-PSMA-PET/CT in castration-resistant prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3612–3621. [Google Scholar] [CrossRef] [PubMed]
- Deek, M.P.; Taparra, K.; Phillips, R.; Velho, P.I.; Gao, R.W.; Deville, C.; Song, D.Y.; Greco, S.; Carducci, M.; Eisenberger, M.; et al. Metastasis-directed therapy prolongs efficacy of systemic therapy and improves clinical outcomes in oligoprogressive castration-resistant prostate cancer. Eur. Urol. Oncol. 2021, 4, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Wei, Y.; Zhang, T.; Liu, C.; Hu, X.; Zhao, J.; Gan, H.; Liu, W.; Zhu, B.; Wu, J.; et al. Stereotactic radiotherapy for lesions detected via 68Ga-prostate-specific membrane antigen and 18F-fluorodeoxyglucose PET/CT in patients with nonmetastatic prostate cancer with early PSA progression on androgen deprivation therapy: A prospective single-center study. Eur. Urol. Oncol. 2022, 5, 420–427. [Google Scholar] [CrossRef] [PubMed]
- Rans, K.; Joniau, S.; Berghen, C.; Goffin, K.; Dumez, H.; Haustermans, K.; De Meerleer, G. Progression-directed therapy in oligoprogressive castration-resistant prostate cancer: Final results from the prospective, single-arm, phase 2 MEDCARE trial. Eur. Urol. Oncol. 2024, 7, 1441–1450. [Google Scholar] [CrossRef] [PubMed]
- Francolini, G.; Garlatti, P.; Di Cataldo, V.; Triggiani, L.; Simoni, N.; Detti, B.; Lorenzetti, V.; Colombo, F.; Morelli, V.; Ganovelli, M.; et al. Pattern of recurrence after stereotactic body radiotherapy for para-aortic oligo-recurrent prostate cancer: A multicentric analysis. Radiother. Oncol. 2023, 128, 1423–1428. [Google Scholar] [CrossRef] [PubMed]
- Francolini, G.; Di Cataldo, V.; Garlatti, P.; Detti, B.; Caini, S.; Bruni, A.; Ingrosso, G.; D’Angelillo, R.M.; Alitto, A.R.; Augugliaro, M.; et al. ARTO trial: Overall survival analysis from a randomized phase II trial testing the benefit of adding stereotactic body radiotherapy to abiraterone acetate in patients with oligometastatic castrate-resistant prostate cancer. J. Clin. Oncol. 2024, 42 (Suppl. S6), 132. [Google Scholar] [CrossRef]
- Le Guevelou, J.; Cuccia, F.; Flippot, R.; Ferrera, G.; Terlizzi, M.; Zilli, T.; De Crevoisier, R.; Hannoun-Levi, J.M.; Supiot, S.; Sargos, P.; et al. The Current Landscape of Stereotactic Body Radiation Therapy for Metastatic Castration-Resistant Prostate Cancer. Prostate Cancer Prostatic Dis. 2024; in press. [Google Scholar] [CrossRef] [PubMed]
- Eule, C.J.; Candelario, N.; Nath, S.K.; Robin, T.P. Time to Next Systemic Therapy After Stereotactic Body Radiation Therapy for Oligoprogressive Metastatic Castrate-Resistant Prostate Cancer. Adv. Radiat. Oncol. 2024, 9, 101655. [Google Scholar] [CrossRef] [PubMed]
- Ge, S.; Zheng, L.; Li, Y.; Gan, L.; Wang, Z.; Zeng, Z.; Meng, C.; Li, K.; Ma, J.; Wang, D.; et al. Comparing the Safety and Effectiveness of Minimally Invasive Surgery and Open Inguinal Lymph Node Dissection in Penile Cancer: A Systematic Review and Meta-Analysis. Eur. J. Surg. Oncol. 2024, 50, 108553. [Google Scholar] [CrossRef]
- Patel, K.N.; Salunke, A.; Bakshi, G.; Jayaprakash, D.; Pandya, S.J. Robotic-Assisted Video-Endoscopic Inguinal Lymphadenectomy (RAVEIL) and Video-Endoscopic Inguinal Lymphadenectomy (VEIL) versus Open Inguinal Lymph-Node Dissection (OILND) in Carcinoma of Penis: Comparison of Perioperative Outcomes, Complications and Oncological Outcomes. A Systematic Review and Meta-Analysis. Urol. Oncol. 2022, 40, 112.e11–112.e22. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Jaipuria, J.; Goel, A.; Shah, S.; Bhardwaj, R.; Baidya, S.; Jain, J.; Jain, C.; Rawal, S. Comparing Outcomes of Robotic and Open Inguinal Lymph Node Dissection in Patients with Carcinoma of the Penis. J. Urol. 2018, 199, 1518–1525. [Google Scholar] [CrossRef]
- Zahid, A.; Ayyan, M.; Farooq, M.; Cheema, H.A.; Shahid, A.; Naeem, F.; Ilyas, M.A.; Sohail, S. Robotic Surgery in Comparison to the Open and Laparoscopic Approaches in the Field of Urology: A Systematic Review. J. Robot. Surg. 2023, 17, 11–29. [Google Scholar] [CrossRef] [PubMed]
- Goudarzi, Z.; Lotfi, F.; Najafpour, Z.; Hafezi, A.A.; Alizadeh Zakaria, M.; Keshavarz, K. Cost-Effectiveness and Budget Impact Analysis of Enzalutamide in Comparison to Abiraterone in Treatment of Metastatic Prostate Cancer Resistant to Castration in Iran. BMC Urol. 2024, 24, 45. [Google Scholar] [CrossRef] [PubMed]
- Ramaswamy, K.; Lechpammer, S.; Mardekian, J.; Huang, A.; Schultz, N.M.; Sandin, R.; Wang, L.; Baser, O.; George, D.J. Economic Outcomes in Patients with Chemotherapy-Naïve Metastatic Castration-Resistant Prostate Cancer Treated with Enzalutamide or Abiraterone Acetate Plus Prednisone. Adv. Ther. 2020, 37, 2083–2097. [Google Scholar] [CrossRef]
- Xu, C.; Cai, J.; Zhuang, J.; Zheng, B.; Chen, L.; Sun, H.; Zheng, G.; Wei, X.; Liu, M. Cost-Effectiveness of Olaparib, a PARP Inhibitor, for Patients with Metastatic Castration-Resistant Prostate Cancer in China and United States. Ann. Transl. Med. 2022, 10, 830. [Google Scholar] [CrossRef] [PubMed]
- Yanev, I.; Gatete, J., Jr.; Aprikian, A.G.; Guertin, J.R.; Dragomir, A. The Health Economics of Metastatic Hormone-Sensitive and Non-Metastatic Castration-Resistant Prostate Cancer—A Systematic Literature Review with Application to the Canadian Context. Curr. Oncol. 2022, 29, 3393–3424. [Google Scholar] [CrossRef]
- Soma, T.; Yoshida, S.; Wakejima, R.; Taguchi, T.; Fukuda, S.; Tanaka, H.; Yokoyama, M.; Ohashi, K.; Okubo, K.; Fujii, Y. A case of repeat oligoprogressive castration-resistant prostate cancer treated with pulmonary metastasectomy. IJU Case Rep. 2023, 6, 216–218. [Google Scholar] [CrossRef] [PubMed]
- Nozaki, K.; Kawai, T.; Fujimura, T.; Matsui, H.; Teshima, T.; Oshina, T.; Takahashi, A.; Sato, Y.; Yamada , D.; Azuma, T.; et al. Carbon 11-Choline Positron Emission Tomography/Computed Tomography and Palliative Local Therapy for Castration-Resistant Prostate Cancer. Int. Urol. Nephrol. 2019, 51, 1763–1769. [Google Scholar] [CrossRef]
- Kato, R.; Goffin, K.; Joniau, S.; Daugaard, G.; den Hartog, J.; Van Wynsberge, L.; De Meerleer, G. The impact of progression-directed therapy on survival in metastatic castration-refractory prostate cancer: MEDCARE phase 3 trial. BJU Int. 2025, 135, 63–70. [Google Scholar] [CrossRef]
- Heidenreich, A.; Bludau, M.; Bruns, C.; Nestler, T.; Porres, D.; Pfister, D.J.K.P. Pelvic exenteration surgery in patients with locally advanced castration-naïve and castration-resistant symptomatic prostate cancer. BJU Int. 2020, 126, 651–659. [Google Scholar] [CrossRef]
- Belda-Ferre, M.; Garcia-Segui, A.; Pacheco-Bru, J.J.; Valencia-Guadalajara, V.J.; Verdú-Verdú, L.P.; Sánchez-Cano, E.; Chillón-Sempere, F.S.; Vázquez-Mazón, F. Multicenter study on multidisciplinary committees in advanced prostate cancer. Actas Urol. Esp. 2022, 46, 106–113. [Google Scholar] [CrossRef]
- Zhu, S.; Chen, J.; Ni, Y.; Zhang, H.; Liu, Z.; Shen, P.; Sun, G.; Liang, J.; Zhang, X.; Wang, Z.; et al. Dynamic multidisciplinary team discussions can improve the prognosis of metastatic castration-resistant prostate cancer patients. Prostate 2021, 81, 721–727. [Google Scholar] [CrossRef] [PubMed]
- Hahn, A.W.; Aparicio, A.; Jadvar, H.; Poon, D.M.C. MDT Perspective: Innovative Applications of Stereotactic Body Radiation Therapy in Metastatic Castration-Resistant Prostate Cancer. Prostate Cancer Prostatic Dis. 2024; ahead of print. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subscale | Maximum Score | Preoperative Score | Postoperative Score |
|---|---|---|---|
| Physical Well-Being (PWB) | 28 | 22 | 22 |
| Social/Family Well-Being (SWB) | 28 | 26 | 27 |
| Emotional Well-Being (EWB) | 24 | 20 | 21 |
| Functional Well-Being (FWB) | 28 | 24 | 25 |
| Prostate Cancer Subscale (PCS) | 48 | 38 | 37 |
| Trial | Intervention | Findings | Key Clinical Endpoints |
|---|---|---|---|
| Kwan et al. (2021) ICE-PAC [8] | Stereotactic Ablative Body Radiotherapy (SABR) + Immune Checkpoint Inhibitor (ICI) (avelumab) | 48% disease control rate; ORR 31%; systemic benefit noted; safety—90% Treatment-Related Adverse Events (TRAEs); 16% grade 3–4; 10% discontinued treatment | Radiographic progression-free survival (rPFS)—8.4 months; overall survival (OS)—14.1 months. |
| Zhang et al. (2021) [9] | SABR; SABR + Poly (ADP-ribose) Polymerase (PARP) inhibitors | 39.5% progression-free at 1 year; 20.8% at 2 years; delayed systemic progression; sustained local control; patients with BRCA1/2 mutations had improved progression-free survival (PFS) with SABR + PARP inhibitors | Prostate-Specific Antigen (PSA) PFS—9.2 months; local PFS—84.4% at 1 year, 75.3% at 2 years; Distant Metastasis-Free Survival (DMFS)—17.6% at 1 year, 5.0% at 2 years; BRCA1/2 PFS—13.2 months (vs. 6.8 for PARP inhibitors alone); time to systemic progression—16.4 months (vs. 9.1 for systemic therapy (ST), p < 0.01). |
| Onal et al. (2021) [10] | SABR | 73.1% PSA response; 48.6% oligometastatic relapse; 35.1% diffuse progression; effective in most cases | OS (2-year)—86.9%; PFS—16.6 months; Time to Next Systemic Therapy (TTNST)—16.4 months. |
| Deek et al. (2021) [11] | SABR; SABR + Docetaxel | SABR significantly delayed PSA failure, Time to Next Intervention (TTNI), and DMFS; 2-year OS improved vs. systemic therapy (ST) alone; SABR + Docetaxel showed an OS benefit over Docetaxel monotherapy, particularly in low-volume metastatic disease | PSA Failure—9.7 months; TTNI—14.9 months; DMFS—12.7 months, 2-year OS—90.3%; SABR + Docetaxel OS—42.6 months (vs. 29.8 months for Docetaxel alone, Hazard Ratio (HR)—0.65, p = 0.008). |
| Pan et al. (2022) [12] | Stereotactic Body Radiotherapy (SBRT) guided by dual-tracer Positron Emission Tomography/Computed Tomography (PET/CT) | SBRT improved Metastasis-Free Survival (MFS) compared to androgen deprivation therapy (ADT) alone; PSA response > 90% was achieved by 86% of patients with SBRT; minimal toxicity—no grade ≥ 3 Adverse Events (AEs) | MFS—11.0 months (ADT) vs. not reached (SBRT); HR—4.69 (95% Confidence Interval (CI): 2.92–25.0, p < 0.001); PSA response > 90% in 86% of patients with SBRT. |
| Rans et al. (2024) MEDCARE [13] | SABR | Delayed systemic progression; significantly prolonged Next-Line Systemic Treatment-Free Survival (NEST-FS) (31 vs. 13 months in treated vs. untreated lesions); 2-year local control rate 95% | NEST-FS—17 months; Local Control—95%. |
| Francolini et al. (2024) ARTO [14,15] | SABR + Abiraterone | Enhanced efficacy vs. systemic therapy (ST) alone; improved disease control; OS benefit observed but not statistically significant (p = 0.07) | PFS—10 months; OS—114 months. |
| Le Guevelou et al. (2024) [16] | SABR + Androgen Receptor Inhibitors (ARIs); SABR + Lutetium-177 Prostate-Specific Membrane Antigen (177Lu-PSMA-617) | Extended PFS (HR: 0.35); low toxicity (grade 3 < 5%); prolonged systemic treatment-free survival; SABR + 177Lu-PSMA-617 improved biochemical PFS and reduced skeletal-related events | PFS extended (HR: 0.35); NEST-FS—2–3 years; SABR + 177Lu-PSMA-617: biochemical PFS—12.1 months (vs. 7.4 for 177Lu-PSMA-617 alone, p = 0.045); skeletal-related events—10% (vs. 22% for radiopharmaceutical-only group). |
| Eule et al. (2024) [17] | SABR; SABR + Next-Generation ARIs | Delayed need for systemic therapy; 40.6% PSA response; treating all lesions further improved TTNST; extended treatment efficacy; SABR + ARIs prolonged Time to Progression (TTP) and enhanced PSA response | TTNST—10.1 months; OS—40.3 months; SABR + ARIs: TTP—14.5 months (vs. 8.3 months for ARIs alone, p = 0.03); PSA reduction ≥ 50% in 35% of cases within six months. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drobot, R.B.; Lipa, M.; Antoniewicz, A.A. Salvage Ultrasound-Guided Robot-Assisted Video-Endoscopic Inguinal Lymphadenectomy (RAVEIL) as a Metastasis-Directed Therapy (MDT) in Oligoprogressive Metastatic Castration-Resistant Prostate Cancer (mCRPC): A Case Report and Review of the Literature. Curr. Oncol. 2025, 32, 115. https://doi.org/10.3390/curroncol32020115
Drobot RB, Lipa M, Antoniewicz AA. Salvage Ultrasound-Guided Robot-Assisted Video-Endoscopic Inguinal Lymphadenectomy (RAVEIL) as a Metastasis-Directed Therapy (MDT) in Oligoprogressive Metastatic Castration-Resistant Prostate Cancer (mCRPC): A Case Report and Review of the Literature. Current Oncology. 2025; 32(2):115. https://doi.org/10.3390/curroncol32020115
Chicago/Turabian StyleDrobot, Rafał B., Marcin Lipa, and Artur A. Antoniewicz. 2025. "Salvage Ultrasound-Guided Robot-Assisted Video-Endoscopic Inguinal Lymphadenectomy (RAVEIL) as a Metastasis-Directed Therapy (MDT) in Oligoprogressive Metastatic Castration-Resistant Prostate Cancer (mCRPC): A Case Report and Review of the Literature" Current Oncology 32, no. 2: 115. https://doi.org/10.3390/curroncol32020115
APA StyleDrobot, R. B., Lipa, M., & Antoniewicz, A. A. (2025). Salvage Ultrasound-Guided Robot-Assisted Video-Endoscopic Inguinal Lymphadenectomy (RAVEIL) as a Metastasis-Directed Therapy (MDT) in Oligoprogressive Metastatic Castration-Resistant Prostate Cancer (mCRPC): A Case Report and Review of the Literature. Current Oncology, 32(2), 115. https://doi.org/10.3390/curroncol32020115