Total Iliocaval Reconstruction in a Complex Palliative Patient with Malignant Inferior Vena Cava Syndrome

 ,
, {kind=link}
{kind=link}
Abstract
1. Introduction
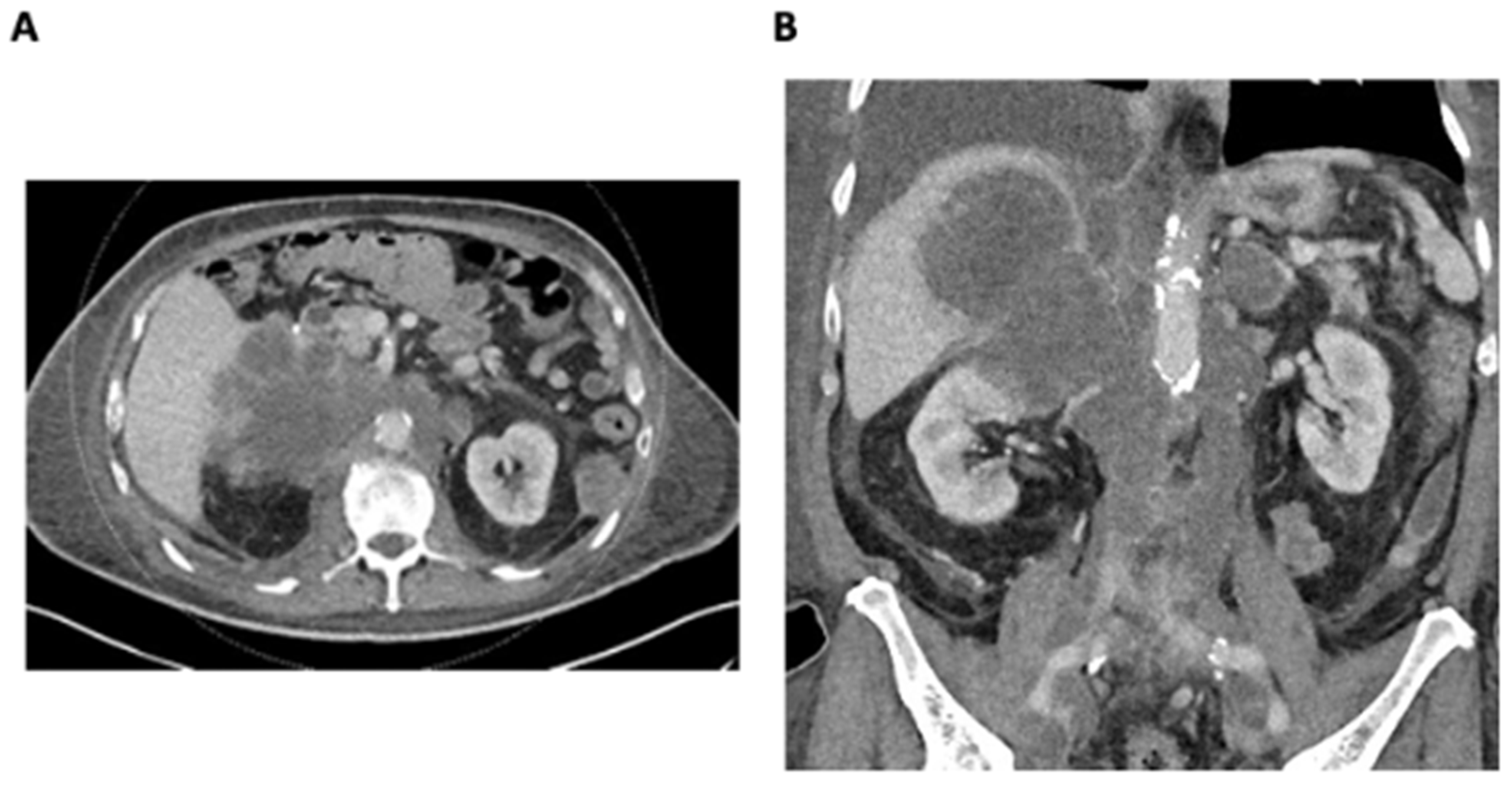
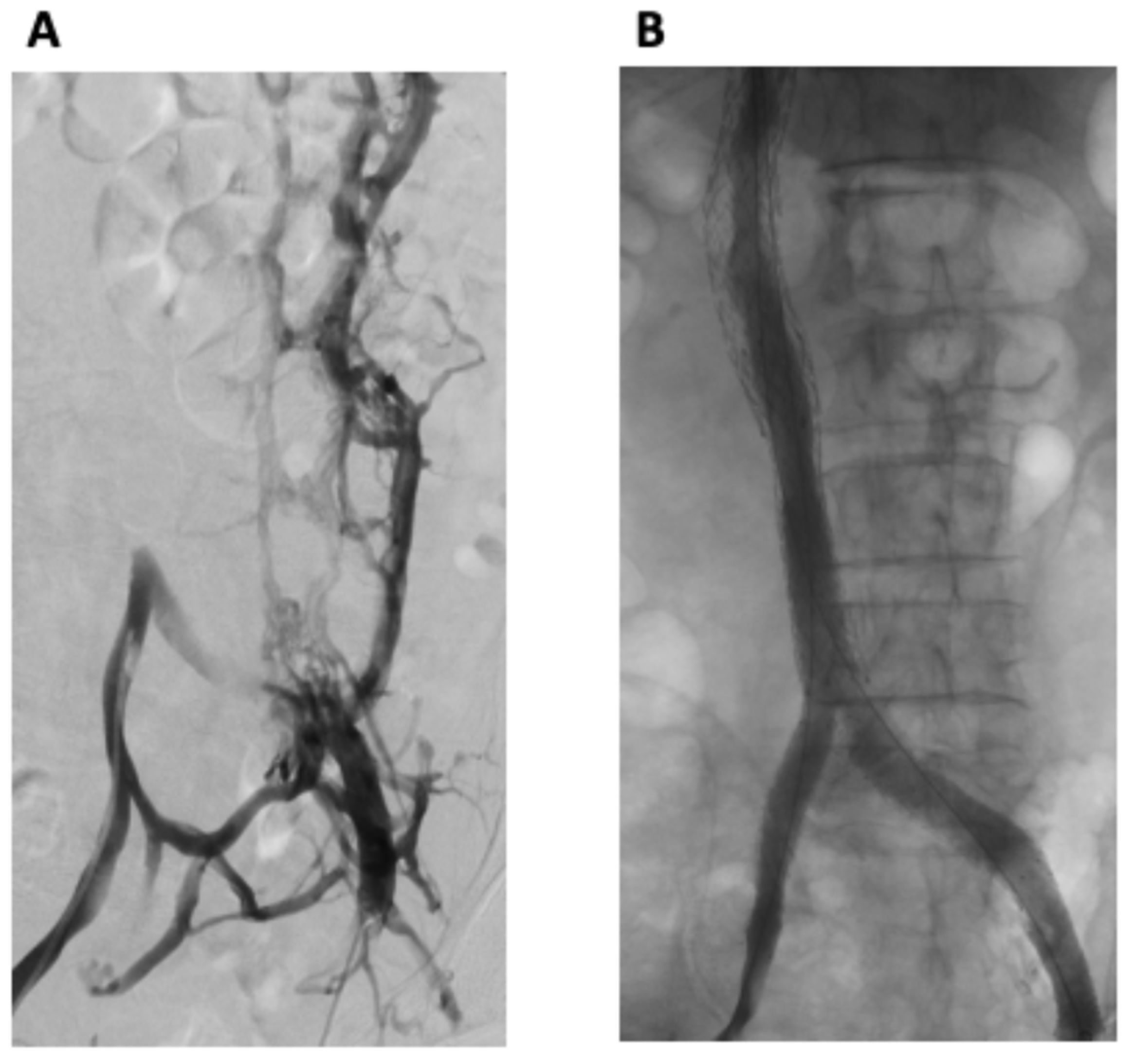
2. Detailed Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Klein-Weigel, P.F.; Elitok, S.; Ruttloff, A.; Reinhold, S.; Nielitz, J.; Steindl, J.; Lutfi, P.; Rehmenklau-Bremer, L.; Hillner, B.; Fuchs, H.; et al. Inferior vena cava-syndrome. Vasa 2021, 50, 250–264. [Google Scholar] [CrossRef] [PubMed]
- Alkhouli, M.; Morad, M.; Narins, C.R.; Raza, F.; Bashir, R. Inferior Vena Cava Thrombosis. JACC Cardiovasc. Interv. 2016, 9, 629–643. [Google Scholar] [CrossRef] [PubMed]
- Kuetting, D.; Thomas, D.; Wilhelm, K.; Pieper, C.C.; Schild, H.H.; Meyer, C. Endovascular Management of Malignant Inferior Vena Cava Syndromes. Cardiovasc. Intervent Radiol. 2017, 40, 1873–1881. [Google Scholar] [CrossRef]
- Delaney, C.L.; Puckridge, P.J. Reconstruction of the iliocaval venous confluence using arterial stent technology. J. Vasc. Surg. Cases Innov. Tech. 2020, 6, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Huang, Q.; Shen, B.; Sun, J.; Wang, X.; Liu, H. Efficacy and safety of endovascular intervention for the management of primary entire-inferior vena cava occlusion. Cardiovasc. Intervent Radiol. 2015, 38, 665–671. [Google Scholar] [CrossRef]
- Maleux, G.; Vertenten, B.; Laenen, A.; De Wever, L.; Heye, S.; Clement, P.; Oyen, R. Palliative endovascular treatment of cancer-related iliocaval obstructive disease: Technical and clinical outcomes. Acta Radiol. 2016, 57, 451–456. [Google Scholar] [CrossRef]
- Augustin, A.M.; Lucius, L.J.; Thurner, A.; Kickuth, R. Malignant obstruction of the inferior vena cava: Clinical experience with the self-expanding Sinus-XL stent system. Abdom. Radiol. 2022, 47, 3604–3614. [Google Scholar] [CrossRef] [PubMed]
- Aly, A.K.; Moussa, A.M.; Chevallier, O.; Kishore, S.; Petre, E.; Friedman, A.; Bryce, Y.; Gonzalez, A.; Camacho, J.; Santos, E.; et al. Iliocaval and iliofemoral venous stenting for obstruction secondary to tumor compression. CVIR Endovasc. 2024, 7, 33. [Google Scholar] [CrossRef]
- Oudkerk, M.; Heystraten, F.M.; Stoter, G. Stenting in malignant vena caval obstruction. Cancer 1993, 71, 142–146. [Google Scholar] [CrossRef]
- Charnsangavej, C.; Carrasco, C.H.; Wallace, S.; Wright, K.C.; Ogawa, K.; Richli, W.; Gianturco, C. Stenosis of the vena cava: Preliminary assessment of treatment with expandable metallic stents. Radiology 1986, 161, 295–298. [Google Scholar]
- Gagne, P.J.; Tahara, R.W.; Fastabend, C.P.; Dzieciuchowicz, L.; Marston, W.; Vedantham, S.; Ting, W.; Iafrati, M.D. Venography versus intravascular ultrasound for diagnosing and treating iliofemoral vein obstruction. J. Vasc. Surg. Venous Lymphat. Disord. 2017, 5, 678–687. [Google Scholar] [CrossRef]
- Secemsky, E.A.; Aronow, H.D.; Kwolek, C.J.; Meissner, M.; Muck, P.E.; Parikh, S.A.; Winokur, R.S.; George, J.C.; Salazar, G.; Murphy, E.H.; et al. Intravascular Ultrasound Use in Peripheral Arterial and Deep Venous Interventions: Multidisciplinary Expert Opinion From SCAI/AVF/AVLS/SIR/SVM/SVS. J. Vasc. Interv. Radiol. 2024, 35, 335–348. [Google Scholar] [CrossRef] [PubMed]
- Murphy, E.; Gibson, K.; Sapoval, M.; Dexter, D.J.; Kolluri, R.; Razavi, M.; Black, S. Pivotal Study Evaluating the Safety and Effectiveness of the Abre Venous Self-Expanding Stent System in Patients With Symptomatic Iliofemoral Venous Outflow Obstruction. Circ. Cardiovasc. Interv. 2022, 15, e010960. [Google Scholar] [CrossRef]
- Gwon, D.I.; Ko, G.Y.; Kim, J.H.; Shin, J.H.; Yoon, H.K.; Sung, K.B. Malignant superior vena cava syndrome: A comparative cohort study of treatment with covered stents versus uncovered stents. Radiology 2013, 266, 979–987. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.S.; Li, C.W.; Li, J.X.; Wu, W.J.; Li, Y.; Shi, J.G. Covered versus uncovered stent insertion for malignant superior vena cava obstruction. Minim. Invasive Ther. Allied Technol. 2020, 29, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Hage, A.N.; Srinivasa, R.N.; Abramowitz, S.D.; Cooper, K.J.; Khaja, M.S.; Barnes, G.D.; Chick, J.F.B. Endovascular iliocaval reconstruction for the treatment of iliocaval thrombosis: From imaging to intervention. Vasc. Med. 2018, 23, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Kinariwala, D.; Liles, A.; Williams, D.M.; Khaja, M.S. Iliocaval Reconstruction: Review of Technique, Challenges, and Outcomes. Semin. Intervent Radiol. 2022, 39, 464–474. [Google Scholar] [CrossRef]
- Marcy, P.Y.; Magne, N.; Bentolila, F.; Drouillard, J.; Bruneton, J.N.; Descamps, B. Superior vena cava obstruction: Is stenting necessary? Support. Care Cancer. 2001, 9, 103–107. [Google Scholar] [CrossRef]
- Apostolova, Y.; Mehier, P.; Qanadli, S.D.; Pruijm, M. Inferior vena cava thrombosis as a possible cause of nephrotic-range proteinuria: Two case reports. J. Med. Case Rep. 2021, 15, 569. [Google Scholar] [CrossRef]
- Liu, Z.; Gao, N.; Shen, L.; Yang, J.; Zhu, Y.; Li, Z.; Si, Y. Endovascular treatment for symptomatic iliac vein compression syndrome: A prospective consecutive series of 48 patients. Ann. Vasc. Surg. 2014, 28, 695–704. [Google Scholar] [CrossRef]
- Neglen, P.; Hollis, K.C.; Olivier, J.; Raju, S. Stenting of the venous outflow in chronic venous disease: Long-term stent-related outcome, clinical, and hemodynamic result. J. Vasc. Surg. 2007, 46, 979–990. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Haqq, R.; Novak, Z.; Pearce, B.J.; Matthews, T.C.; Patterson, M.A.; Jordan, W.D., Jr.; Passman, M.A. Routine extended follow-up surveillance of iliac vein stents for iliocaval venous obstruction may not be warranted. J. Vasc. Surg. Venous Lymphat. Disord. 2017, 5, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Kishore, S.; Khaja, M.S.; Thornburg, B.; Sharma, A.M.; Knuttinen, M.G.; Shamoun, F.; Mantha, S.; Desai, K.R.; Sista, A.K.; Black, S.A.; et al. Antithrombotic Therapy After Venous Interventions: AJR Expert Panel Narrative Review. AJR Am. J. Roentgenol. 2022, 219, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Xiao, N.; Genet, M.; Khaja, M.; Desai, K.R. Antithrombotic Therapy after Deep Venous Intervention. Semin. Intervent Radiol. 2022, 39, 357–363. [Google Scholar] [CrossRef]
- Takeuchi, Y.; Arai, Y.; Sone, M.; Sugawara, S.; Aramaki, T.; Sato, R.; Kichikawa, K.; Tanaka, T.; Morishita, H.; Ito, T.; et al. Evaluation of stent placement for vena cava syndrome: Phase II trial and phase III randomized controlled trial. Support. Care Cancer 2019, 27, 1081–1088. [Google Scholar] [CrossRef]
- Erben, Y.; Bjarnason, H.; Oladottir, G.L.; McBane, R.D.; Gloviczki, P. Endovascular recanalization for nonmalignant obstruction of the inferior vena cava. J. Vasc. Surg. Venous Lymphat. Disord. 2018, 6, 173–182. [Google Scholar] [CrossRef]
- Barrette, L.X.; McLaughlin, S.W.; Vance, A.Z.; Trerotola, S.O.; Soulen, M.C.; Sudheendra, D.; Dagli, M.; Redmond, J.W.; Clark, T.W.I. Inferior Vena Cava Reconstruction in Symptomatic Patients Using Palmaz Stents: A Retrospective Single-Center Experience. Ann. Vasc. Surg. 2020, 66, 370–377. [Google Scholar] [CrossRef]
- Morita, S.; Sugawara, S.; Suda, T.; Prasetyo, D.; Kobayashi, Y.; Hoshi, T.; Abe, S.; Yagi, K.; Terai, S. Stent Placement for Malignant Inferior Vena Cava Syndrome in a Patient with Recurrent Colon Cancer. Intern. Med. 2020, 59, 2885–2890. [Google Scholar] [CrossRef]
- Hartung, O.; Otero, A.; Boufi, M.; De Caridi, G.; Barthelemy, P.; Juhan, C.; Alimi, Y.S. Mid-term results of endovascular treatment for symptomatic chronic nonmalignant iliocaval venous occlusive disease. J. Vasc. Surg. 2005, 42, 1138–1144, discussion 1144. [Google Scholar] [CrossRef]
- Hartung, O.; Loundou, A.D.; Barthelemy, P.; Arnoux, D.; Boufi, M.; Alimi, Y.S. Endovascular management of chronic disabling ilio-caval obstructive lesions: Long-term results. Eur. J. Vasc. Endovasc. Surg. 2009, 38, 118–124. [Google Scholar] [CrossRef]
- Morris, R.I.; Jackson, N.; Smith, A.; Black, S.A. A Systematic Review of the Safety and Efficacy of Inferior Vena Cava Stenting. Eur. J. Vasc. Endovasc. Surg. 2023, 65, 298–308. [Google Scholar] [CrossRef] [PubMed]
- Chick, J.; Bundy, J.; Srinivasa, R.; Hage, A.; Gemmete, J. Iliocaval Reconstruction Value Analysis Using a Time-Driven Activity-Based Costing Approach. 2018. Available online: https://www.jvascsurg.org/article/S0741-5214(18)30781-X/fulltext (accessed on 3 July 2024).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lofroth, J.; Pourghadiri, A.; Hadjivassiliou, A.; Heran, M.; Legiehn, G.; Ho, S.; Dhatt, R. Total Iliocaval Reconstruction in a Complex Palliative Patient with Malignant Inferior Vena Cava Syndrome. Curr. Oncol. 2024, 31, 3978-3984. https://doi.org/10.3390/curroncol31070294
Lofroth J, Pourghadiri A, Hadjivassiliou A, Heran M, Legiehn G, Ho S, Dhatt R. Total Iliocaval Reconstruction in a Complex Palliative Patient with Malignant Inferior Vena Cava Syndrome. Current Oncology. 2024; 31(7):3978-3984. https://doi.org/10.3390/curroncol31070294
Chicago/Turabian StyleLofroth, Jack, Amir Pourghadiri, Anastasia Hadjivassiliou, Manraj Heran, Gerald Legiehn, Stephen Ho, and Ravjot Dhatt. 2024. "Total Iliocaval Reconstruction in a Complex Palliative Patient with Malignant Inferior Vena Cava Syndrome" Current Oncology 31, no. 7: 3978-3984. https://doi.org/10.3390/curroncol31070294
APA StyleLofroth, J., Pourghadiri, A., Hadjivassiliou, A., Heran, M., Legiehn, G., Ho, S., & Dhatt, R. (2024). Total Iliocaval Reconstruction in a Complex Palliative Patient with Malignant Inferior Vena Cava Syndrome. Current Oncology, 31(7), 3978-3984. https://doi.org/10.3390/curroncol31070294