Does Pre-Emptive Availability of PREDICT 2.1 Results Change Ordering Practices for Oncotype DX? A Multi-Center Prospective Cohort Study

 , , ,
, , ,
Abstract
1. Introduction
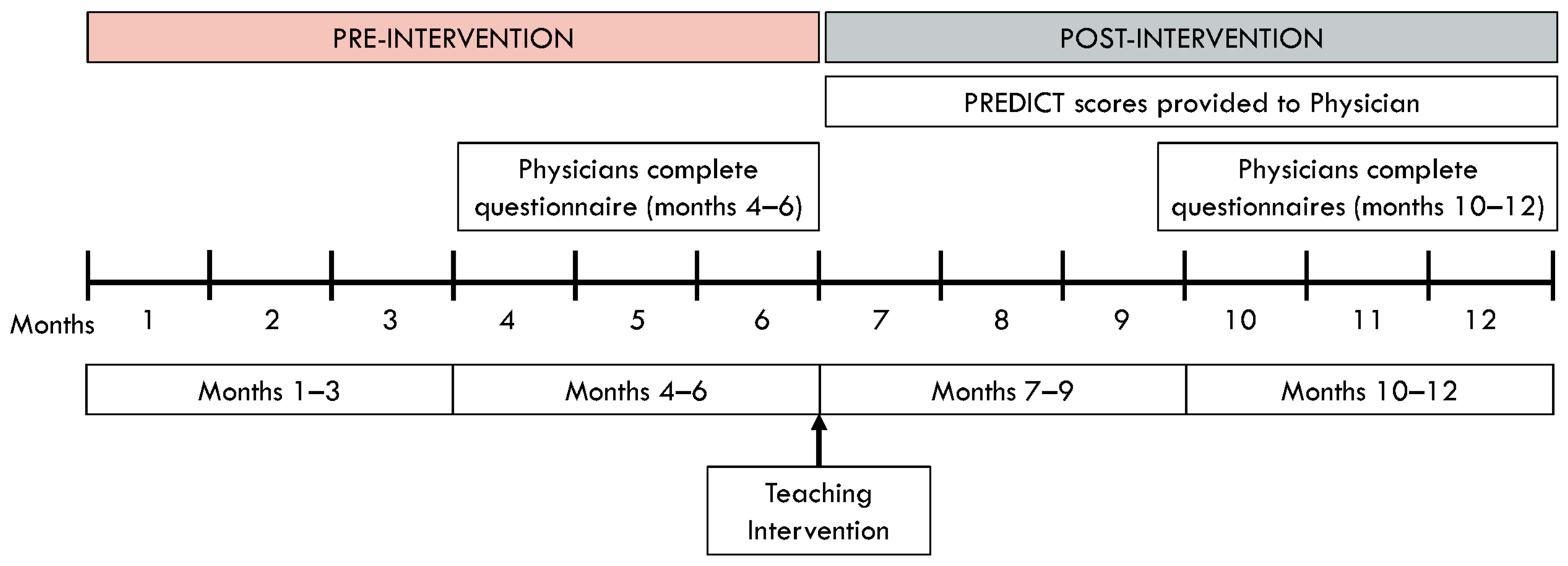
2. Materials and Methods
3. Results
3.1. Sites and Patients
3.2. Patient Characteristics
3.3. PREDICT 2.1 Results
3.4. Effect of Educational Intervention on Oncotype DX Requests
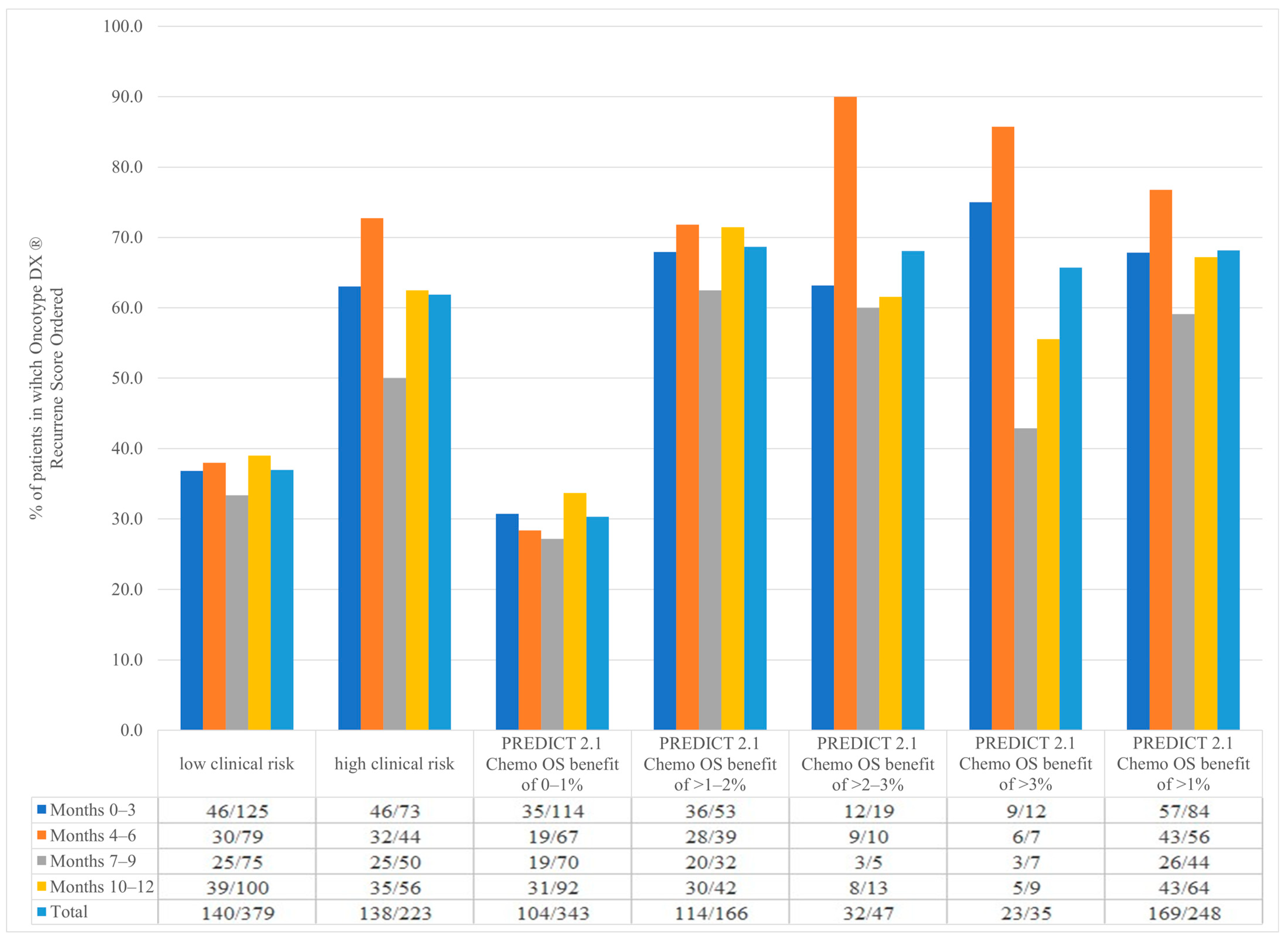
3.5. Oncotype DX Ordering and Oncotype DX Recurrence Score of ≥26 Depending on Clinical Risk
3.6. Oncotype DX Ordering and Oncotype DX Recurrence Score of ≥26 Depending on PREDICT 2.1 Results
3.7. Comparison of RSClin Scores with Clinical Risk and PREDICT 2.1 Results for Benefit from 2nd Generation Chemotherapy
3.8. Physician Questionnaires
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pinder, S.E.; Ellis, I.O.; Elston, C.W. Prognostic factors in primary breast carcinoma. J. Clin. Pathol. 1995, 48, 981–983. [Google Scholar] [CrossRef]
- Davies, C.; Godwin, J.; Gray, R.; Clarke, M.; Cutter, D.; Darby, S.; McGale, P.; Pan, H.C.; Taylor, C.; Wang, Y.C.; et al. Relevance of breast cancer hormone receptors and other factors to the efficacy of adjuvant tamoxifen: Patient-level meta-analysis of randomised trials. Lancet 2011, 378, 771–784. [Google Scholar]
- Goldhirsch, A.; Wood, W.C.; Gelber, R.D.; Coates, A.S.; Thurlimann, B.; Senn, H.J. Progress and promise: Highlights of the inter-national expert consensus on the primary therapy of early breast cancer 2007. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2007, 18, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Galea, M.H.; Blamey, R.W.; Elston, C.E.; Ellis, I.O. The Nottingham Prognostic Index in primary breast cancer. Breast Cancer Res. Treat. 1992, 22, 207–219. [Google Scholar] [CrossRef] [PubMed]
- Mokbel, K.; Wazir, U.; El Hage Chehade, H.; Manson, A.; Choy, C.; Moye, V.; Mokbel, K. A Comparison of the Performance of EndoPredict Clinical and NHS PREDICT in 120 Patients Treated for ER-positive Breast Cancer. Anticancer Res. 2017, 37, 6863–6869. [Google Scholar]
- Flanagan, M.B.; Dabbs, D.J.; Brufsky, A.M.; Beriwal, S.; Bhargava, R. Histopathologic variables predict Oncotype DX recurrence score. Mod. Pathol. 2008, 21, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- Magee Equations™ for Estimating Oncotype DX® Recurrence Score. 2017. Available online: http://path.upmc.edu/onlineTools/MageeEuations.html (accessed on 3 July 2018).
- Gage, M.M.; Rosman, M.; Mylander, W.C.; Giblin, E.; Kim, H.S.; Cope, L.; Umbricht, C.; Wolff, A.C.; Tafra, L. A Validated Model for Identifying Patients Unlikely to Benefit from the 21-Gene Recurrence Score Assay. Clin. Breast Cancer 2015, 15, 467–472. [Google Scholar] [CrossRef]
- Orucevic, A.; Bell, J.L.; McNabb, A.P.; Heidel, R.E. Oncotype DX breast cancer recurrence score can be predicted with a novel nomogram using clinicopathologic data. Breast Cancer Res. Treat. 2017, 163, 51–61. [Google Scholar] [CrossRef]
- Cuzick, J.; Dowsett, M.; Pineda, S.; Wale, C.; Salter, J.; Quinn, E.; Zabaglo, L.; Mallon, E.; Green, A.R.; Ellis, I.O.; et al. Prognostic value of a combined estrogen receptor, progesterone receptor, Ki-67, and human epidermal growth factor receptor 2 immunohistochemical score and comparison with the Genomic Health recurrence score in early breast cancer. J. Clin. Oncol. 2011, 29, 4273–4278. [Google Scholar] [CrossRef] [PubMed]
- Filipits, M.; Rudas, M.; Jakesz, R.; Dubsky, P.; Fitzal, F.; Singer, C.F.; Dietze, O.; Greil, R.; Jelen, A.; Sevelda, P.; et al. A new molecular predictor of distant recurrence in ER-positive, HER2-negative breast cancer adds independent information to conventional clinical risk factors. Clin. Cancer Res. 2011, 17, 6012–6020. [Google Scholar] [CrossRef]
- Nielsen, T.O.; Parker, J.S.; Leung, S.; Voduc, D.; Ebbert, M.; Vickery, T.; Davies, S.R.; Snider, J.; Stijleman, I.J.; Reed, J.; et al. A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor-positive breast cancer. Clin. Cancer Res. 2010, 16, 5222–5232. [Google Scholar] [CrossRef]
- Paik, S.; Shak, S.; Tang, G.; Kim, C.; Baker, J.; Cronin, M.; Baehner, F.L.; Walker, M.G.; Watson, D.; Park, T.; et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N. Engl. J. Med. 2004, 351, 2817–2826. [Google Scholar] [CrossRef]
- Sgroi, D.C.; Carney, E.; Zarrella, E.; Steffel, L.; Binns, S.N.; Finkelstein, D.M.; Szymonifka, J.; Bhan, A.K.; Shepherd, L.E.; Zhang, Y.; et al. Prediction of late disease recurrence and extended adjuvant letrozole benefit by the HOXB13/IL17BR biomarker. J. Natl. Cancer Inst. 2013, 105, 1036–1042. [Google Scholar] [CrossRef]
- van’t Veer, L.J.; Dai, H.; van de Vijver, M.J.; He, Y.D.; Hart, A.A.; Mao, M.; Peterse, H.L.; Van Der Kooy, K.; Marton, M.J.; Witteveen, A.T.; et al. Gene expression profiling predicts clinical outcome of breast cancer. Nature 2002, 415, 530–536. [Google Scholar] [CrossRef]
- Candido Dos Reis, F.J.; Wishart, G.C.; Dicks, E.M.; Greenberg, D.; Rashbass, J.; Schmidt, M.K.; van den Broek, A.J.; Ellis, I.O.; Green, A.; Rakha, E.; et al. An updated PREDICT breast cancer prognostication and treatment benefit prediction model with independent validation. Breast Cancer Res. 2017, 19, 58. [Google Scholar] [CrossRef] [PubMed]
- Paik, S.; Tang, G.; Shak, S.; Kim, C.; Baker, J.; Kim, W.; Cronin, M.; Baehner, F.L.; Watson, D.; Wolmark, N.; et al. Gene expression and benefit of chemotherapy in women with node-negative, estrogen receptor-positive breast cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2006, 24, 3726–3734. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; Olson, J.A., Jr.; et al. Adjuvant Chemotherapy Guided by a 21-Gene Expression Assay in Breast Cancer. N. Engl. J. Med. 2018, 379, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Cuzick, J.; Costantino, J.P.; Dowsett, M.; Forbes, J.F.; Crager, M.; Mamounas, E.P.; Shak, S.; Wolmark, N. Risk of recurrence and chemotherapy benefit for patients with node-negative, estrogen receptor-positive breast cancer: Recurrence score alone and integrated with pathologic and clinical factors. J. Clin. Oncol. 2011, 29, 4365–4372. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Crager, M.R.; Tang, G.; Gray, R.J.; Stemmer, S.M.; Shak, S. Development and Validation of a Tool Integrating the 21-Gene Recurrence Score and Clinical-Pathological Features to Individualize Prognosis and Prediction of Chemotherapy Benefit in Early Breast Cancer. J. Clin. Oncol. 2021, 39, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Sparano, J.A.; Gray, R.J.; Ravdin, P.M.; Makower, D.F.; Pritchard, K.I.; Albain, K.S.; Hayes, D.F.; Geyer, C.E., Jr.; Dees, E.C.; Goetz, M.P.; et al. Clinical and Genomic Risk to Guide the Use of Adjuvant Therapy for Breast Cancer. N. Engl. J. Med. 2019, 380, 2395–2405. [Google Scholar] [CrossRef]
- Cardoso, F.; van’t Veer, L.J.; Bogaerts, J.; Slaets, L.; Viale, G.; Delaloge, S.; Pierga, J.Y.; Brain, E.; Causeret, S.; DeLorenzi, M.; et al. 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. Engl. J. Med. 2016, 375, 717–729. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, T.O.; Leung, S.C.Y.; Rimm, D.L.; Dodson, A.; Acs, B.; Badve, S.; Denkert, C.; Ellis, M.J.; Fineberg, S.; Flowers, M.; et al. Assessment of Ki67 in BreastCancer: Updated Recommendations From the International Ki67 in Breast Cancer Working Group. J. Natl. Cancer Inst. 2021, 113, 808–819. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Pts | Months 0–3 | Months 4–6 | Months 7–9 | Months 10–12 | ||
|---|---|---|---|---|---|---|
| N | All | 602 | 198 | 123 | 125 | 156 |
| Age (years) | Mean (sd) | 63.2 (11.8) | 62.3 (12.6) | 64.5 (11.7) | 64.6 (11.2) | 62.3 (11.2) |
| Median (IQR) | 64 (55–71) | 64 (53–71) | 65 (57–72) | 65 (57–72) | 63 (54–70) | |
| Tumor Size (mm) | Median (range) | 16.5 (6–109) | 17 (6–109) | 17 (6–96) | 15 (6–76) | 17 (6–46) |
| Diagnosis to Resection months | Median (range) | 1.2 (0, 4.7) | 1.2 (0.2, 3.7) | 1.0 (0.1, 4.7) | 1.1 (0, 3.4) | 1.3 (0.1, 4.5) |
| Sex | N (%) Female | 596 (99.0) | 197 (99.5) | 122 (99.2) | 124 (99.2) | 153 (98.1) |
| Menopausal Status (of females) | N (%) Pre | 80 (13.4) | 33 (16.8) | 15 (12.3) | 11 (8.9) | 21 (13.7) |
| Peri | 42 (7.0) | 20 (10.1) | 7 (5.7) | 5 (4.0) | 10 (6.4) | |
| Post- | 474 (79.5) | 144 (73.1) | 100 (82.0) | 108 (87.1) | 122 (79.7) | |
| Tumor Detection | N (%) Screening | 394 (65.4) | 125 (63.1) | 74 (60.2) | 93 (74.4) | 102 (65.4) |
| Symptomatic | 208 (34.6) | 73 (36.9) | 49 (39.8) | 32 (25.6) | 54 (34.6) | |
| ER Staining | N (%) None | 0 | 0 | 0 | 0 | 0 |
| Weak | 9 (1.5) | 5 (2.5) | 2 (1.6) | 0 | 2 (1.3) | |
| Moderate | 58 (9.6) | 16 (8.1) | 18 (14.6) | 11 (8.8) | 13 (8.3) | |
| Strong | 535 (88.9) | 177 (89.4) | 103 (83.7) | 114 (91.2) | 141 (90.4) | |
| PR Status | N (%) Positive | 532 (88.4) | 178 (89.9) | 110 (89.4) | 108 (86.4) | 136 (87.2) |
| Negative | 70 (11.6) | 20 (10.1) | 13 (10.6) | 17 (13.6) | 20 (12.8) | |
| PR Staining | N (%) None | 70 (11.6) | 20 (10.1) | 13 (10.6) | 17 (13.6) | 20 (12.8) |
| Weak | 10 (1.7) | 3 (1.5) | 1 (0.8) | 3 (2.4) | 3 (1.9) | |
| Moderate | 105 (17.4) | 38 (19.2) | 20 (16.3) | 17 (13.6) | 30 (19.2) | |
| Strong | 417 (69.3) | 137 (69.2) | 89 (72.4) | 88 (70.4) | 103 (66.0) | |
| Grade | N (%) 1 | 114 (18.9) | 49 (24.8) | 21 (17.1) | 19 (15.2) | 25 (16.0) |
| 2 | 370 (61.5) | 109 (55.1) | 76 (61.8) | 87 (69.6) | 98 (62.8) | |
| 3 | 118 (19.6) | 40 (20.2) | 26 (21.1) | 19 (15.2) | 33 (21.2) | |
| Histology | N (%) Ductal and NOS | 445 (73.9) | 143 (72.2) | 87 (70.7) | 92 (73.6) | 123 (78.9) |
| Classic lobular | 69 (11.5) | 19 (9.6) | 20 (16.3) | 15 (12.0) | 15 (9.6) | |
| Mixed ductal–lobular | 38 (6.3) | 21 (10.6) | 9 (7.3) | 4 (3.2) | 4 (2.6) | |
| Pleomorphic lobular | 2 (0.3) | 1 (0.5) | 0 | 0 | 1 (0.6) | |
| Tubular | 3 (0.5) | 1 (0.5) | 1 (0.8) | 1 (0.8) | 0 | |
| Papillary | 11 (1.8) | 3 (1.5) | 0 | 6 (4.8) | 2 (1.3) | |
| Other | 34 (5.7) | 10 (5.1) | 6 (4.9) | 7 (5.6) | 11 (7.1) | |
| Isolated Tumor Cells | N (%) Yes | 28 (4.7) | 9 (4.6) | 8 (6.5) | 6 (4.8) | 5 (3.2) |
| No | 494 (82.1) | 167 (84.3) | 97 (78.9) | 102 (81.6) | 128 (82.1) | |
| Unknown | 80 (13.3) | 22 (11.1) | 18 (14.6) | 17 (13.6) | 23 (14.7) | |
| Micrometastatic Disease | N (%) Yes | 25 (4.2) | 9 (4.6) | 2 (1.6) | 4 (3.2) | 10 (6.4) |
| No | 571 (94.9) | 185 (93.4) | 120 (97.6) | 120 (96.0) | 146 (93.6) | |
| Unknown | 6 (1.0) | 4 (2.0) | 1 (0.8) | 1 (0.8) | 0 | |
| Lymphovascular Invasion Present | N (%) Yes | 69 (11.5) | 23 (11.6) | 17 (13.8) | 14 (11.2) | 15 (9.6) |
| No | 495 (82.2) | 164 (82.8) | 101 (82.1) | 105 (84.0) | 125 (80.1) | |
| Unknown | 38 (6.3) | 11 (5.6) | 5 (4.1) | 6 (4.8) | 16 (10.3) |
| Months 0–3 | Months 4–6 | Months 7–9 | Months 10–12 | ||
|---|---|---|---|---|---|
| N | 198 | 123 | 125 | 156 | |
| Surgery Only | 10-year OS% | 74.7 (16.1) | 72.6 (17.0) | 73.9 (16.0) | 76.1 (15.0) |
| Chemotherapy (2nd Generation) | Additional OS Benefit | 1.24 (0.91) | 1.23 (0.83) | 1.20 (0.94) | 1.23 (0.85) |
| 10-year OS% | 78.5 (15.9) | 76.5 (16.9) | 77.3 (16.0) | 79.8 (14.7) | |
| Chemotherapy (3rd Generation) | Additional OS Benefit | 2.06 (1.52) | 2.03 (1.38) | 1.90 (1.27) | 2.02 (1.42) |
| 10-year OS% | 79.2 (15.9) | 77.2 (16.8) | 78.0 (16.0) | 80.6 (14.7) | |
| Hormone Therapy | Additional OS Benefit | 2.56 (1.79) | 2.53 (1.65) | 2.38 (1.51) | 2.53 (1.69) |
| 10-year OS% | 77.3 (15.9) | 75.2 (16.8) | 76.1 (16.0) | 78.6 (14.7) | |
| Bisphosphonates | Additional OS Benefit | 0.78 (0.57) | 0.77 (0.54) | 0.74 (0.52) | 0.72 (0.49) |
| 10-year OS% | 76.6 (16.1) | 75.3 (17.0) | 76.6 (16.1) | 79.0 (15.2) | |
| No Cancer | 10-year OS% | 83.1 (16.3) | 81.0 (17.3) | 81.5 (16.4) | 84.4 (14.9) |
| PREDICT 2.1 10-year Chemo 2nd gen OS Survival Benefit | 0–1% | 67 (54.5) | 70 (56.0) | 92 (59.0) | 343 (57.0) |
| >1 to 2% | 39 (31.7) | 32 (25.6) | 42 (26.9) | 166 (27.6) | |
| >2 to 3% | 10 (8.1) | 5 (4.0) | 13 (8.3) | 47 (7.8) | |
| >3% | 7 (5.7) | 7 (5.6) | 9 (5.8) | 35 (5.8) | |
| Clinical Risk | N (%) High | 44 (35.8) | 50 (40.0) | 56 (35.9) | 223 (37.0) |
| Low † | 79 (64.2) | 75 (60.0) | 100 (64.1) | 379 (63.0) |
| Months 0–3 | Months 4–6 | Months 7–9 | Months 10–12 | p Value * | ||
|---|---|---|---|---|---|---|
| N | 198 | 123 | 125 | 156 | ||
| N (%) of patients who had an Oncotype DX® Ordered | 92 (46.5) | 62 (50.4) | 50 (40.0) | 74 (47.4) | 0.37 | |
| Oncotype DX® Recurrence Score | Mean (sd) | 18.7 (12.4) | 15.6 (8.6) | 17.6 (9.1) | 19.2 (12.0) | 0.25 |
| Median (IQR) | 15 (11, 22) | 13.5 (9, 20) | 16 (12, 22) | 16 (12, 23) | ||
| Oncotype DX® Recurrence Score | N (%) high risk (≥26) | 19 (20.7) | 8 (12.9) | 10 (20.0) | 16 (21.6) | 0.54 # |
| Intermediate risk (21 to 25), and | 10 (10.9) | 5 (8.1) | 7 (14.0) | 8 (10.8) | ||
| Low risk (≤20) | 63 (68.5) | 49 (79.0) | 33 (66.0) | 50 (67.6) | ||
| Resection to Treatment | Median (RANGE) Months | 4.3 (0.1, 12.2) | 3.4 (0.5, 9.7) | 3.2 (0.5, 11.7) | 2.7 (0.4, 9.5) | 0.004 |
| Chemotherapy Planned | N (%) Yes | 25 (12.6) | 11 (8.9) | 13 (10.4) | 28 (17.9) | 0.22 # |
| No | 172 (86.9) | 105 (85.4) | 99 (79.2) | 112 (71.8) | ||
| Unknown | 1 (0.5) | 7 (5.7) | 13 (10.4) | 16 (10.3) | ||
| Recommended Chemotherapy and Frequency | 2nd Generation | 17 (68.0) | 10 (83.3) | 16 (94.1) | 20 (74.1) | 0.42 |
| 3rd Generation | 8 (32.0) | 2 (16.7) | 1 (5.9) | 7 (25.9) | ||
| Recommended Chemotherapy and Frequency | TC | 17 (68.0) | 10 (83.3) | 15 (88.2) | 20 (74.1) | 0.60 # |
| AC | 0 | 0 | 1 (5.9) | 0 | ||
| Dd AC-paclitaxel | 3 (12.0) | 1 (8.3) | 0 | 4 (14.8) | ||
| Dd AC-weekly paclitaxel | 2 (8.0) | 1 (8.3) | 1 (5.9) | 1 (3.7) | ||
| AC-weekly paclitaxel | 0 | 0 | 0 | 1 (3.7) | ||
| AC-docetaxel | 2 (8.0) | 0 | 0 | 0 | ||
| FEC-D | 1 (4.0) | 0 | 0 | 1 (3.7) | ||
| Chemotherapy Received | N (%) Yes | 22 (11.1) | 10 (8.1) | 14 (11.2) | 23 (14.7) | 0.25 |
| Resection to Chemotherapy | Median (RANGE) Months | 1.9 (1.0, 3.0) | 1.8 (0.2, 2.5) | 1.8 (1.3, 2.4) | 1.9 (0.7, 3.2) | 0.86 |
| Radiation Received | N (%) Yes | 112 (56.6) | 88 (71.5) | 90 (72.0) | 110 (70.5) | 0.025 |
| Resection to Radiation | Median (RANGE) Months | 2.4 (1.0, 7.9) | 2.2 (1.0, 8.1) | 2.1 (1.0, 6.2) | 2.3 (0.9, 9.1) | 0.72 |
| Endocrine Therapy Received | N (%) Yes | 169 (85.4) | 104 (84.6) | 110 (88.0) | 130 (83.3) | 0.91 |
| Resection to Endocrine Therapy | Median (RANGE) Months | 1.8 (0.0, 8.2) | 1.9 (0.5, 7.1) | 2.3 (0.6, 7.6) | 2.2 (0.5, 9.8) | 0.04 |
| Clinical Risk | N (%) High | 46 (50.0) | 32 (51.6) | 25 (50.0) | 35 (47.3) | 0.72 |
| Low † | 46 (50.0) | 30 (48.4) | 25 (50.0) | 39 (52.7) | ||
| Predicted 10-Year Survival | N (%) ≥ 92% | 52/92 (56.5) | 29/62 (46.8) | 17/45 (37.8) | 38/74 (51.4) | 0.08 |
| PREDICT 2.1 10-year Chemo 2nd gen OS Survival Benefit | 0–1% | 35 (38.0) | 19 (30.7) | 19 (42.2) | 31 (41.9) | 0.26 # |
| >1 to 2% | 36 (39.1) | 28 (45.2) | 20 (44.4) | 30 (40.5) | ||
| >2 to 3% | 12 (13.0) | 9 (14.5) | 3 (6.7) | 8 (10.8) | ||
| >3 to 5% | 9 (9.8) | 6 (9.7) | 3 (6.7) | 5 (6.8) | ||
| >5% | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Months 0–3 | Months 4–6 | Months 7–9 | Months 10–12 | ||
|---|---|---|---|---|---|
| N | 198 | 123 | 125 | 156 | |
| N with Questionnaires | 0 | 123 | 0 | 156 | |
| Was Oncotype DX Recurrence Score Available When You Saw Patient? | N (%) Yes | NA | 7 (5.7) | NA | 6 (3.9) |
| Did you use PREDICT2.1 tool results? | N (%) Yes | NA | 64 (52.5) | NA | 135 (86.5) |
| Did you order Oncotype DX? | N (%) Yes | NA | 60 (49.6) | NA | 71 (45.8) |
| Did you recommend chemotherapy? | N (%) Yes | NA | 6 (4.9) | NA | 12 (7.7) |
| No | 68 (55.3) | 82 (52.6) | |||
| Pending Oncotype | 49 (39.8) | 62 (39.7) | |||
| Reason for No Chemotherapy | No benefit based on clin/path | NA | 53 (77.9) | NA | 48 (60.0) |
| No benefit based on PREDICT | 8 (11.8) | 14 (17.5) | |||
| Patient preference | 6 (8.8) | 10 (12.5) | |||
| Patient comorbidities | 1 (1.5) | 8 (10.0) | |||
| Unsure whether adjuvant chemotherapy would be best | Strongly Disagree | NA | 30 (24.6) | NA | 39 (25.3) |
| Disagree | 39 (32.0) | 35 (22.7) | |||
| Neither Agree nor Disagree | 11 (9.0) | 16 (10.4) | |||
| Agree | 37 (30.3) | 58 (37.7) | |||
| Strongly Agree | 5 (4.1) | 6 (3.9) | |||
| PREDICT results make me more confident in my recommendation | Strongly Disagree | NA | 1 (1.4) | NA | 3 (2.0) |
| Disagree | 8 (11.0) | 12 (7.8) | |||
| Neither Agree nor Disagree | 21 (28.8) | 36 (23.5) | |||
| Agree | 31 (42.5) | 71 (46.4) | |||
| Strongly Agree | 12 (16.4) | 31 (20.3) | |||
| PREDICT tool provided additional clinically relevant information | Strongly Disagree | NA | 0 | NA | 3 (2.0) |
| Disagree | 8 (11.0) | 8 (5.2) | |||
| Neither Agree nor Disagree | 10 (13.7) | 32 (20.9) | |||
| Agree | 45 (61.6) | 85 (55.6) | |||
| Strongly Agree | 10 (13.7) | 25 (16.3) | |||
| PREDICT influenced my treatment recommendation | Strongly Disagree | NA | 3 (4.2) | NA | 7 (4.6) |
| Disagree | 11 (15.3) | 21 (13.7) | |||
| Neither Agree nor Disagree | 17 (23.6) | 47 (30.7) | |||
| Agree | 32 (44.4) | 56 (36.6) | |||
| Strongly Agree | 9 (12.5) | 22 (14.4) | |||
| I would use PREDICT tool again | Strongly Disagree | NA | 1 (1.4) | NA | 1 (0.7) |
| Disagree | 1 (1.4) | 5 (3.3) | |||
| Neither Agree nor Disagree | 3 (4.1) | 19 (12.4) | |||
| Agree | 41 (56.2) | 68 (44.4) | |||
| Strongly Agree | 27 (37.0) | 60 (39.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Awan, A.A.; Saunders, D.; Pond, G.; Hamm, C.; Califaretti, N.; Mates, M.; Kumar, V.; Ibrahim, M.F.K.; Beltran-Bless, A.-A.; Vandermeer, L.; et al. Does Pre-Emptive Availability of PREDICT 2.1 Results Change Ordering Practices for Oncotype DX? A Multi-Center Prospective Cohort Study. Curr. Oncol. 2024, 31, 1278-1290. https://doi.org/10.3390/curroncol31030096
Awan AA, Saunders D, Pond G, Hamm C, Califaretti N, Mates M, Kumar V, Ibrahim MFK, Beltran-Bless A-A, Vandermeer L, et al. Does Pre-Emptive Availability of PREDICT 2.1 Results Change Ordering Practices for Oncotype DX? A Multi-Center Prospective Cohort Study. Current Oncology. 2024; 31(3):1278-1290. https://doi.org/10.3390/curroncol31030096
Chicago/Turabian StyleAwan, Arif Ali, Deanna Saunders, Gregory Pond, Caroline Hamm, Nadia Califaretti, Mihaela Mates, Vikaash Kumar, Mohammed F. K. Ibrahim, Ana-Alicia Beltran-Bless, Lisa Vandermeer, and et al. 2024. "Does Pre-Emptive Availability of PREDICT 2.1 Results Change Ordering Practices for Oncotype DX? A Multi-Center Prospective Cohort Study" Current Oncology 31, no. 3: 1278-1290. https://doi.org/10.3390/curroncol31030096
APA StyleAwan, A. A., Saunders, D., Pond, G., Hamm, C., Califaretti, N., Mates, M., Kumar, V., Ibrahim, M. F. K., Beltran-Bless, A.-A., Vandermeer, L., Hilton, J., & Clemons, M. (2024). Does Pre-Emptive Availability of PREDICT 2.1 Results Change Ordering Practices for Oncotype DX? A Multi-Center Prospective Cohort Study. Current Oncology, 31(3), 1278-1290. https://doi.org/10.3390/curroncol31030096