Durvalumab Treatment Patterns for Patients with Unresectable Stage III Non-Small Cell Lung Cancer in the Veterans Health Administration (VHA): A Nationwide, Real-World Study


 , ,
, , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design
2.3. Study Population
2.4. Data and Statistical Analysis
3. Results
3.1. Patient Characteristics
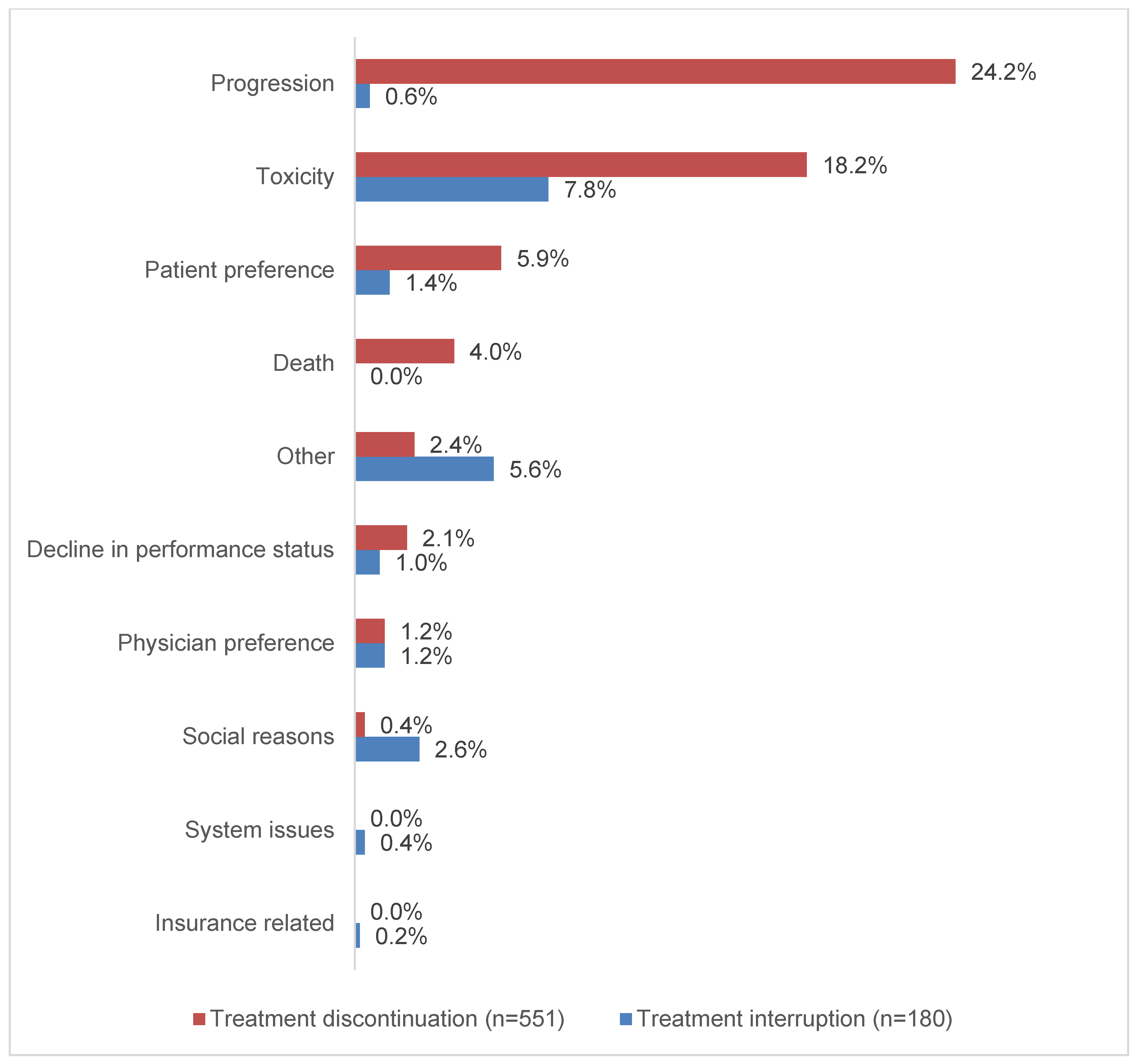
3.2. Durvalumab Treatment Patterns
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The eighth edition AJCC cancer staging manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Auperin, A.; Le Pechoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.M.; Shaikh, T.; Hallman, M. Therapeutic management options for stage III non-small cell lung cancer. World J. Clin. Oncol. 2017, 8, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-term results of NRG Oncology RTOG 0617: Standard- versus high-dose chemoradiotherapy with or without cetuximab for unresectable stage III non-small-cell lung cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.; Reckamp, K.L.; Baas, P.; Crino, L.; Eberhardt, W.E.; Poddubskaya, E.; Antonia, S.; Pluzanski, A.; Vokes, E.E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 123–135. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus docetaxel in advanced nonsquamous non-small-cell lung cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef]
- Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Perez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; Ahn, M.J.; et al. Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Lancet 2016, 387, 1540–1550. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [PubMed]
- AztraZeneca Pharmaceuticals LP. Imfinzi [Package Insert]; AztraZeneca Pharmaceuticals LP: Wilmington, DE, USA, 2020. [Google Scholar]
- Girard, N.; Bar, J.; Garrido, P.; Garassino, M.C.; McDonald, F.; Mornex, F.; Filippi, A.R.; Smit, H.J.M.; Peters, S.; Field, J.K.; et al. Treatment characteristics and real-world progression-free survival in patients with unresectable stage III NSCLC who received durvalumab after chemoradiotherapy: Findings from the PACIFIC-R study. J. Thorac. Oncol. 2023, 18, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.R.; Faivre-Finn, C.; Gray, J.E.; Vicente, D.; Planchard, D.; Paz-Ares, L.; Vansteenkiste, J.F.; Garassino, M.C.; Hui, R.; Quantin, X.; et al. Five-year survival outcomes from the PACIFIC Trial: Durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J. Clin. Oncol. 2022, 40, 1301. [Google Scholar] [CrossRef]
- Wang, C.C.; Chiu, L.C.; Ju, J.S.; Lin, Y.C.; Fang, Y.F.; Yang, C.T.; Hsu, P.C. Durvalumab as consolidation therapy in post-concurrent chemoradiation (CCRT) in unresectable stage III non-small cell lung cancer patients: A multicenter observational study. Vaccines 2021, 9, 1122. [Google Scholar] [CrossRef] [PubMed]
- Bruni, A.; Scotti, V.; Borghetti, P.; Vagge, S.; Cozzi, S.; D’Angelo, E.; Giaj Levra, N.; Fozza, A.; Taraborrelli, M.; Piperno, G.; et al. A real-world, multicenter, observational retrospective study of durvalumab after concomitant or sequential chemoradiation for unresectable stage III non-small cell lung cancer. Front. Oncol. 2021, 11, 744956. [Google Scholar] [CrossRef] [PubMed]
- Horinouchi, H.; Atagi, S.; Oizumi, S.; Ohashi, K.; Kato, T.; Kozuki, T.; Seike, M.; Sone, T.; Sobue, T.; Tokito, T.; et al. Real-world outcomes of chemoradiotherapy for unresectable Stage III non-small cell lung cancer: The SOLUTION study. Cancer Med. 2020, 9, 6597–6608. [Google Scholar] [CrossRef]
- Jung, H.A.; Noh, J.M.; Sun, J.M.; Lee, S.H.; Ahn, J.S.; Ahn, M.J.; Pyo, H.; Ahn, Y.C.; Park, K. Real world data of durvalumab consolidation after chemoradiotherapy in stage III non-small-cell lung cancer. Lung Cancer 2020, 146, 23–29. [Google Scholar] [CrossRef]
- McDonald, F.; Mornex, F.; Garassino, M.C.; Filippi, A.R.; Christoph, D.; Haakensen, V.D.; Agbarya, A.; Van den Heuvel, M.; Vercauter, P.; Chouaid, C. PACIFIC-R: Real-world characteristics of unresectable stage III NSCLC patients treated with durvalumab after chemoradiotherapy. J. Thorac. Oncol. 2021, 16, S737–S747. [Google Scholar] [CrossRef]
- Sankar, K.; Bryant, A.K.; Strohbehn, G.W.; Zhao, L.; Elliott, D.; Moghanaki, D.; Kelley, M.J.; Ramnath, N.; Green, M.D. Real world outcomes versus clinical trial results of durvalumab maintenance in veterans with stage III non-small cell lung cancer. Cancers 2022, 14, 614. [Google Scholar] [CrossRef]
- Frei, C.R.; Le, H.; McHugh, D.; Ryan, K.; Jones, X.; Galley, S.; Franklin, K.; Baus, C.J.; Tavera, J.; Janania-Martinez, M.; et al. Outcomes in chronic lymphocytic leukemia patients on novel agents in the US Veterans Health Administration System. Leuk. Lymphoma 2021, 62, 1664–1673. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Boersma, P.; Cohen, R.A.; Zelaya, C.E.; Moy, E. Multiple Chronic Conditions among Veterans and Nonveterans: United States, 2015–2018; National Health Statistics Reports; National Center for Health Statistics: Hyattsville, MD, USA, 2021; pp. 1–13.
- Zhang, P.; Su, D.M.; Liang, M.; Fu, J. Chemopreventive agents induce programmed death-1-ligand 1 (PD-L1) surface expression in breast cancer cells and promote PD-L1-mediated T cell apoptosis. Mol. Immunol. 2008, 45, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Deng, L.; Liang, H.; Burnette, B.; Beckett, M.; Darga, T.; Weichselbaum, R.R.; Fu, Y.X. Irradiation and anti-PD-L1 treatment synergistically promote antitumor immunity in mice. J. Clin. Investig. 2014, 124, 687–695. [Google Scholar] [CrossRef] [PubMed]
- Dovedi, S.J.; Adlard, A.L.; Lipowska-Bhalla, G.; McKenna, C.; Jones, S.; Cheadle, E.J.; Stratford, I.J.; Poon, E.; Morrow, M.; Stewart, R.; et al. Acquired resistance to fractionated radiotherapy can be overcome by concurrent PD-L1 blockade. Cancer Res. 2014, 74, 5458–5468. [Google Scholar] [CrossRef] [PubMed]
- Yoneda, K.; Kuwata, T.; Kanayama, M.; Mori, M.; Kawanami, T.; Yatera, K.; Ohguri, T.; Hisaoka, M.; Nakayama, T.; Tanaka, F. Alteration in tumoural PD-L1 expression and stromal CD8-positive tumour-infiltrating lymphocytes after concurrent chemo-radiotherapy for non-small cell lung cancer. Br. J. Cancer 2019, 121, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Faivre-Finn, C.; Spigel, D.R.; Senan, S.; Langer, C.; Perez, B.A.; Ozguroglu, M.; Daniel, D.; Villegas, A.; Vicente, D.; Hui, R.; et al. Impact of prior chemoradiotherapy-related variables on outcomes with durvalumab in unresectable Stage III NSCLC (PACIFIC). Lung Cancer 2021, 151, 30–38. [Google Scholar] [CrossRef]
- Desilets, A.; Blanc-Durand, F.; Lau, S.; Hakozaki, T.; Kitadai, R.; Malo, J.; Belkaid, W.; Richard, C.; Messaoudene, M.; Cvetkovic, L.; et al. Durvalumab therapy following chemoradiation compared with a historical cohort treated with chemoradiation alone in patients with stage III non-small cell lung cancer: A real-world multicentre study. Eur. J. Cancer 2021, 142, 83–91. [Google Scholar] [CrossRef]
- Bryant, A.K.; Sankar, K.; Strohbehn, G.W.; Zhao, L.; Elliott, D.; Daniel, V.; Ramnath, N.; Green, M.D. Timing of adjuvant durvalumab initiation is not associated with outcomes in stage III non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2022, 113, 60–65. [Google Scholar] [CrossRef]
- Waterhouse, D.M.; Young, C.; Robert, N.J.; Aguilar, K.M.; Ndukum, J.; Xie, Y.; Seal, B.S.; Cotarla, I. Durvalumab consolidation therapy following chemoradiotherapy among patients with unresectable stage III non-small cell lung cancer (NSCLC) treated in a U.S. community oncology network. J. Clin. Oncol. 2021, 39, 295. [Google Scholar] [CrossRef]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Kurata, T.; Chiappori, A.; Lee, K.H.; de Wit, M.; et al. Overall survival with durvalumab after chemoradiotherapy in stage III NSCLC. N. Engl. J. Med. 2018, 379, 2342–2350. [Google Scholar] [CrossRef]
- Offin, M.; Shaverdian, N.; Rimner, A.; Lobaugh, S.; Shepherd, A.F.; Simone, C.B., 2nd; Gelblum, D.Y.; Wu, A.J.; Lee, N.; Kris, M.G.; et al. Clinical outcomes, local-regional control and the role for metastasis-directed therapies in stage III non-small cell lung cancers treated with chemoradiation and durvalumab. Radiother. Oncol. 2020, 149, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Shaverdian, N.; Offin, M.; Shepherd, A.F.; Hellmann, M.D.; Gomez, D.R.; Chaft, J.E.; Rimner, A. Association between the early discontinuation of durvalumab and poor survival in patients with stage III NSCLC. JTO Clin. Res. Rep. 2021, 2, 100197. [Google Scholar] [CrossRef] [PubMed]
- Taugner, J.; Kasmann, L.; Eze, C.; Tufman, A.; Reinmuth, N.; Duell, T.; Belka, C.; Manapov, F. Durvalumab after chemoradiotherapy for PD-L1 expressing inoperable stage III NSCLC leads to significant improvement of local-regional control and overall survival in the real-world setting. Cancers 2021, 13, 1613. [Google Scholar] [CrossRef] [PubMed]
- Taugner, J.; Kasmann, L.; Eze, C.; Ruhle, A.; Tufman, A.; Reinmuth, N.; Duell, T.; Belka, C.; Manapov, F. Real-world prospective analysis of treatment patterns in durvalumab maintenance after chemoradiotherapy in unresectable, locally advanced NSCLC patients. Investig. New Drugs 2021, 39, 1189–1196. [Google Scholar] [CrossRef]
- Faehling, M.; Schumann, C.; Christopoulos, P.; Hoffknecht, P.; Alt, J.; Horn, M.; Eisenmann, S.; Schlenska-Lange, A.; Schutt, P.; Steger, F.; et al. Durvalumab after definitive chemoradiotherapy in locally advanced unresectable non-small cell lung cancer (NSCLC): Real-world data on survival and safety from the German expanded-access program (EAP). Lung Cancer 2020, 150, 114–122. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | All (n = 935) |
|---|---|
| Age (years), median (IQR) | 69 (65–72) |
| Age groups, n (%) | -- |
| <65 years | 229 (24) |
| 65 to 74 years | 567 (61) |
| >74 years | 139 (15) |
| Male, n (%) | 891 (95) |
| Race, n (%) | -- |
| Missing/unknown | 1 (<1) |
| White | 726 (78) |
| Black | 198 (21) |
| Other | 10 (1) |
| Charlson score, median (IQR) | 3 (3–5) |
| Charlson Age score, median (IQR) | 6 (5–7) |
| Selected comorbidities, n (%) | -- |
| Congestive heart failure | 123 (13) |
| COPD | 659 (70) |
| Cerebrovascular disease | 131 (14) |
| Dementia | 15 (2) |
| Diabetes | 306 (33) |
| Hemi/paraplegia | 9 (1) |
| HIV/AIDS | 5 (1) |
| Liver disease | 107 (11) |
| Myocardial infarction | 65 (7) |
| Peptic ulcer disease | 17 (2) |
| Peripheral vascular disease | 219 (23) |
| Renal disease | 109 (12) |
| ECOG performance status score, n (%) | -- |
| Missing/unknown | 181 (20) |
| 0–1 | 602 (64) |
| 2–3 | 152 (16) |
| NSCLC histologic subtype, n (%) | -- |
| Missing/unknown | 56 (6) |
| Squamous cell | 469 (50) |
| Non-squamous cell | 400 (43) |
| Mixed | 10 (1) |
| PD-L1 tumor expression level, n (%) | -- |
| Missing/unknown | 595 (63) |
| Available PD-L1 test results | 340 (37) |
| PD-L1 expression level <1% among those with results | 118 (35) |
| PD-L1 expression level ≥1% among those with results | 222 (65) |
| Prior chemotherapy, n (%) | -- |
| Cisplatin-based chemotherapy | 106 (11) |
| Carboplatin-based chemotherapy | 817 (88) |
| Other | 12 (1) |
| Total chemotherapy weeks, median (IQR) | 6 (5–7) |
| Total radiation dose (Gy), n (%) | -- |
| Missing/unknown | 99 (10) |
| <54 | 27 (3) |
| 54–66 | 728 (78) |
| 67–74 | 74 (8) |
| >74 | 7 (1) |
| Radiation fractions, median (IQR) | 30 (30–33) |
| CRT type, n (%) | -- |
| Sequential | 15 (2) |
| Concurrent | 920 (98) |
| Time from end of CRT to first scan (days), median (IQR) | 30 (20–43) |
| Time from end of CRT to first scan, n (%) | -- |
| Missing/unknown | 128 (14) |
| <42 days | 590 (63) |
| ≥42 days | 217 (23) |
| CRT response a, n (%) | -- |
| Missing/unknown | 144 (15) |
| Complete response | 31 (3) |
| Partial response | 623 (67) |
| Stable disease | 98 (11) |
| Progressive disease | 27 (3) |
| Non-evaluable | 12 (1) |
| Characteristic | All (n = 935) |
|---|---|
| Time to durvalumab initiation (days), median (IQR) | 39 (28–54) |
| Patients with durvalumab initiation delays a, n (%) | 367 (39) |
| Duration of treatment initiation delay (days), median (IQR) | 61 (49–80) |
| Durvalumab duration of therapy (months), median (IQR) | 9.0 (2.9–11.8) |
| Durvalumab total doses/infusions, median (IQR) | 16 (7–24) |
| Patients with durvalumab interruptions b, n (%) | 180 (19) |
| Number of durvalumab interruptions, median (IQR) | 1 (1–1) |
| Duration of durvalumab interruptions (days), median (IQR) | 53 (39–90) |
| Durvalumab corrected duration of therapy (months) c, median (IQR) | 8.4 (2.8–11.7) |
| Durvalumab treatment discontinuations, n (%) | 551 (59) |
| Completed planned treatment, n (%) | 384 (41) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moore, A.M.; Nooruddin, Z.; Reveles, K.R.; Datta, P.; Whitehead, J.M.; Franklin, K.; Alkadimi, M.; Williams, M.H.; Williams, R.A.; Smith, S.; et al. Durvalumab Treatment Patterns for Patients with Unresectable Stage III Non-Small Cell Lung Cancer in the Veterans Health Administration (VHA): A Nationwide, Real-World Study. Curr. Oncol. 2023, 30, 8411-8423. https://doi.org/10.3390/curroncol30090611
Moore AM, Nooruddin Z, Reveles KR, Datta P, Whitehead JM, Franklin K, Alkadimi M, Williams MH, Williams RA, Smith S, et al. Durvalumab Treatment Patterns for Patients with Unresectable Stage III Non-Small Cell Lung Cancer in the Veterans Health Administration (VHA): A Nationwide, Real-World Study. Current Oncology. 2023; 30(9):8411-8423. https://doi.org/10.3390/curroncol30090611
Chicago/Turabian StyleMoore, Amanda M., Zohra Nooruddin, Kelly R. Reveles, Paromita Datta, Jennifer M. Whitehead, Kathleen Franklin, Munaf Alkadimi, Madison H. Williams, Ryan A. Williams, Sarah Smith, and et al. 2023. "Durvalumab Treatment Patterns for Patients with Unresectable Stage III Non-Small Cell Lung Cancer in the Veterans Health Administration (VHA): A Nationwide, Real-World Study" Current Oncology 30, no. 9: 8411-8423. https://doi.org/10.3390/curroncol30090611
APA StyleMoore, A. M., Nooruddin, Z., Reveles, K. R., Datta, P., Whitehead, J. M., Franklin, K., Alkadimi, M., Williams, M. H., Williams, R. A., Smith, S., Reichelderfer, R., Cotarla, I., Brannman, L., Frankart, A., Mulrooney, T., Hsieh, K., Simmons, D. J., Jones, X., & Frei, C. R. (2023). Durvalumab Treatment Patterns for Patients with Unresectable Stage III Non-Small Cell Lung Cancer in the Veterans Health Administration (VHA): A Nationwide, Real-World Study. Current Oncology, 30(9), 8411-8423. https://doi.org/10.3390/curroncol30090611