Real-World Clinical Outcomes for Patients with EGFR and HER2 Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer


 , , , and
, , , and
Abstract
1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Target | Patient Population | Results | |
|---|---|---|---|
| Amivantamab | EGFR | Previously treated advanced NSCLC patients with EGFR ex20ins (N = 81) | ORR 40%, median PFS 8.3 months, median DoR 11.1 months (CHRYSALIS) [11] |
| Mobocertinib | EGFR | Previously treated advanced NSCLC patients with EGFR ex20ins (N = 114) | ORR 28%, median PFS 7.3 months, median DoR 17.5 months, median OS 24 months (EXCLAIM) [12] |
| Poziotinib | EGFR and HER2 | EGFR ex20ins—previously treated advanced NSCLC patients (N = 115) | ORR 14.8%, median PFS 4.2 months, median DoR 7.4 months (ZENITH20-1) [13] |
| EGFR ex20ins—previously untreated advanced NSCLC patients (N = 79) | ORR 27.8%, median PFS 7.2 months, median DoR 6.5 months (ZENITH20-3) [14] | ||
| HER2 ex20ins—previously treated advanced NSCLC patients (N = 90) | ORR 27.8%, median PFS 5.5 months, median DoR 5.1 months (ZENITH20-2) [19] | ||
| HER2 ex20ins—previously untreated advanced NSCLC patients (N = 70) | ORR 41%, median PFS 5.6 months, median DoR 5.7 months (ZENITH20-4) [22] | ||
| Sunvozertinib | EGFR | Previously untreated advanced NSCLC patients with EGFR ex20ins (N = 26 evaluable patients) | ORR 73.1%, median PFS, and DoR not reached (WU-KONG) [15] |
| T-Dxd | HER2 | Previously treated advanced NSCLC patients with HER2 mutations (N = 91 with 78 ex20ins) | ORR 55%, median PFS 8.2 months, median DoR 9.3 months, median OS 17.8 months [21] |
2. Materials and Methods
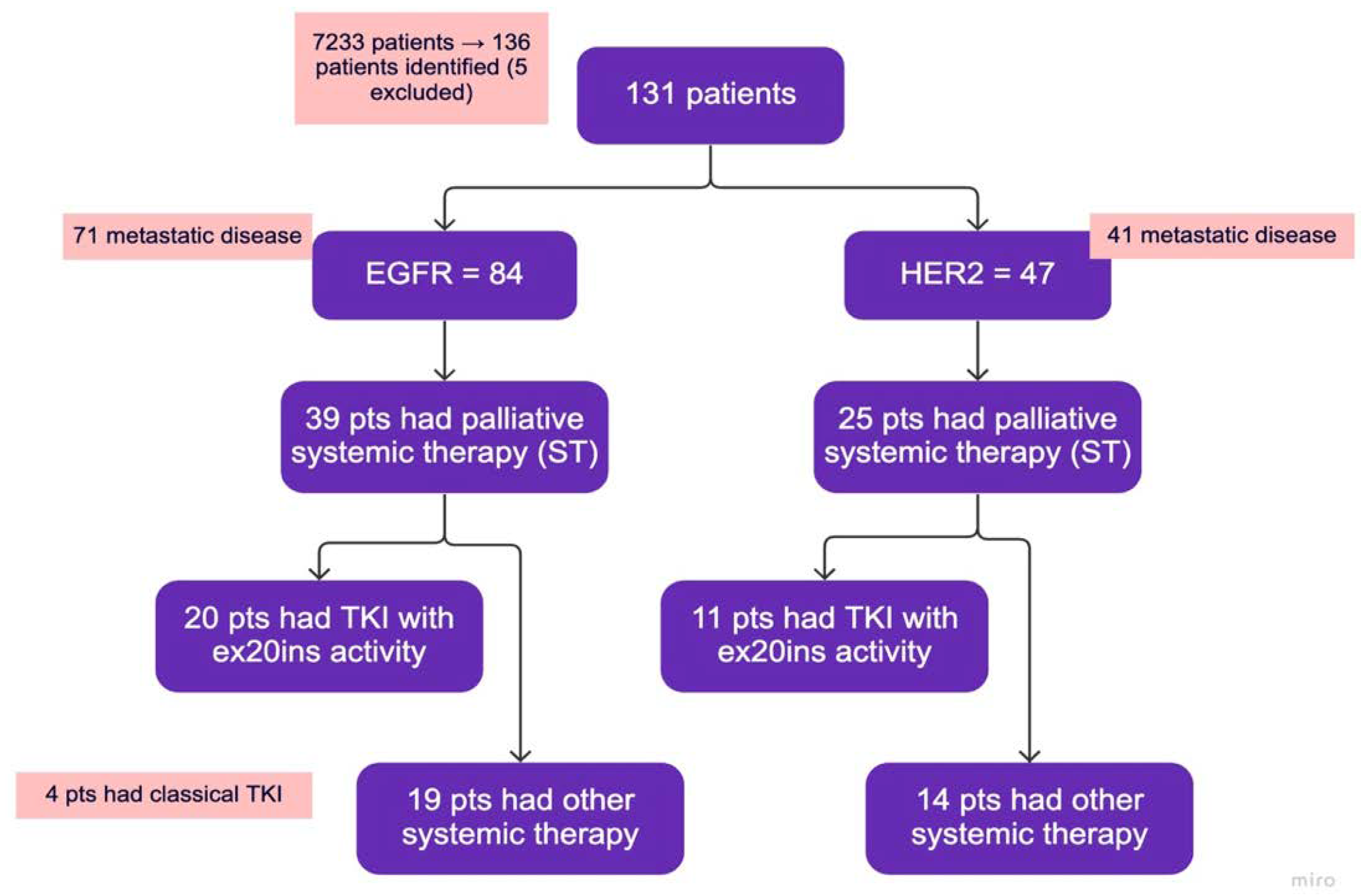
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analyses
3. Results
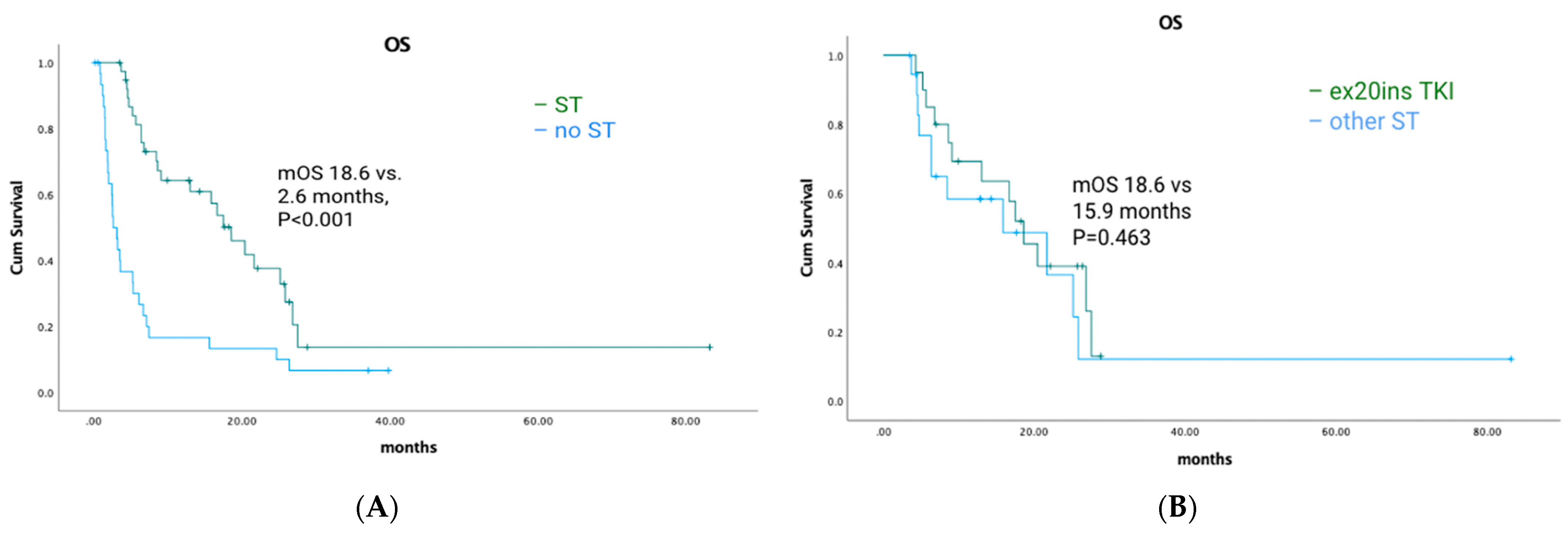
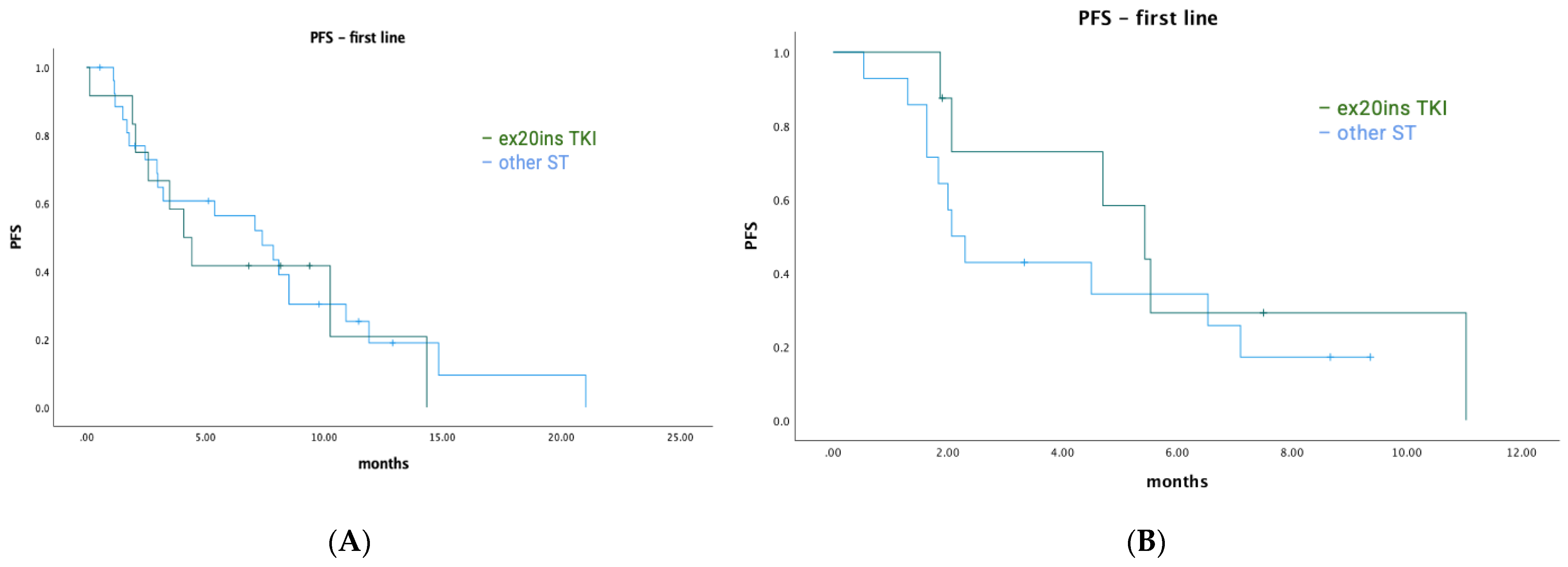
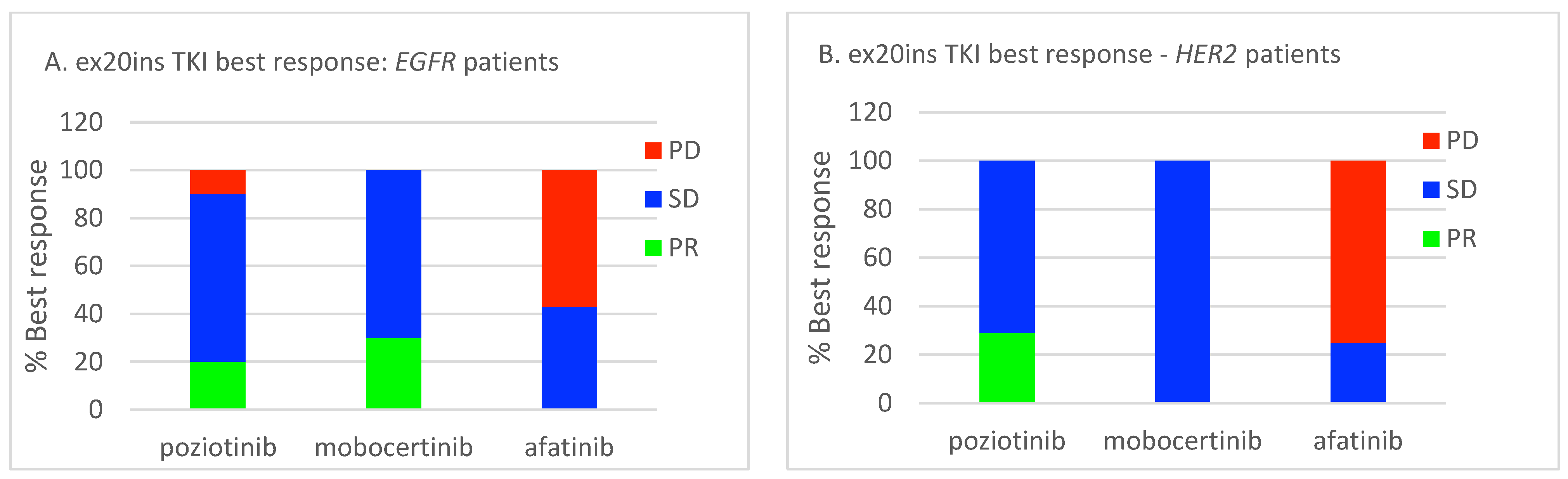
3.1. Treatment Outcomes for Metastatic EGFR ex20ins Patients
3.2. Treatment Outcomes for Metastatic HER2 ex20ins Patients
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Kane, G.M.; Bradbury, P.A.; Feld, R.; Leighl, N.B.; Liu, G.; Pisters, K.M.; Kamel-Reid, S.; Tsao, M.S.; Shepherd, F.A. Uncommon EGFR mutations in advanced non-small cell lung cancer. Lung Cancer 2017, 109, 137–144. [Google Scholar] [CrossRef]
- Friedlaender, A.; Subbiah, V.; Russo, A.; Banna, G.L.; Malapelle, U.; Rolfo, C.; Addeo, A. EGFR and HER2 exon 20 insertions in solid tumours: From biology to treatment. Nat. Rev. Clin. Oncol. 2022, 19, 51–69. [Google Scholar] [CrossRef]
- Bai, R.; Chen, X.; Song, W.; Tian, H.; Cui, J. Therapeutic exploration of uncommon EGFR exon 20 insertion mutations in advanced non-small cell lung cancer: Breaking through brambles and thorns. J. Cancer Res. Clin. Oncol. 2022, 148, 163–176. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, H.; Ichihara, E.; Sakakibara-Konishi, J.; Zenke, Y.; Takeuchi, S.; Morise, M.; Hotta, K.; Sato, M.; Matsumoto, S.; Tanimoto, Z.; et al. A phase I/II study of osimertinib in EGFR exon 20 insertion mutation-positive non-small cell lung cancer. Lung Cancer 2021, 162, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.H.; Lim, S.H.; An, H.J.; Kim, K.H.; Park, K.U.; Kang, E.J.; Choi, Y.H.; Ahn, M.S.; Lee, M.H.; Sun, J.; et al. Osimertinib for patients with non-small-cell lung cancer harboring uncommon EGFR mutations: A multicenter, open-label, phase II trial. J. Clin. Oncol. 2020, 38, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Remon, J.; Hendriks, L.E.L.; Cardona, A.F.; Besse, B. EGFR exon 20 insertions in advanced non-small cell lung cancer: A new history begins. Cancer Treat. Rev. 2020, 90, 102105. [Google Scholar] [CrossRef]
- Patil, T.; Mushtaq, R.; Marsh, S.; Azelby, C.; Pujara, M.; Davies, K.D.; Aisner, D.L.; Purcell, W.T.; Schenk, E.L.; Pacheco, J.M.; et al. Clinicopathologic characteristics, treatment outcomes, and acquired resistance patterns of atypical EGFR mutations and HER2 alterations in stage IV non-small-cell lung cancer. Clin. Lung Cancer 2020, 21, e191–e204. [Google Scholar] [CrossRef]
- Ou, S.; Lin, H.M.; Hong, J.; Yin, Y.; Jin, S.; Lin, J.; Mehta, M.; Nguyen, D.; Neal, J.W. Real-world response and outcomes in NSCLC patients with EGFR exon 20 insertion mutations. J. Clin. Oncol. 2021, 39, 9098. [Google Scholar] [CrossRef]
- Yang, J.C.; Schuler, M.; Popat, S.; Miura, S.; Heeke, S.; Park, K.; Marten, A.; Kim, E.S. Afatinib for the treatment of NSCLC harboring uncommon EGFR mutations: A database of 693 cases. J. Thorac. Oncol. 2020, 15, 803–815. [Google Scholar] [CrossRef]
- Yang, J.C.; Sequist, L.V.; Geater, S.L.; Tsai, C.; Mok, T.S.K.; Schuler, M.; Yamamoto, N.; Yu, C.; Ou, S.I.; Zhou, C.; et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: A combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef]
- Park, K.; Haura, E.B.; Leighl, N.B.; Mitchell, P.; Shu, C.A.; Girard, N.; Viteri, S.; Han, J.; Kim, S.; Lee, C.K.; et al. Amivantamab in EGFR Exon 20 insertion-mutated non-small-cell lung cancer progressing on platinum chemotherapy: Initial results from the CHRYSALIS Phase I study. J. Clin. Oncol. 2021, 39, 3391–3402. [Google Scholar] [CrossRef]
- Zhou, C.; Ramalingam, S.S.; Kim, T.M.; Kim, S.; Yang, J.C.; Riely, G.J.; Mekhail, T.; Nguyen, D.; Campelo, M.R.G.; Felip, E.; et al. Treatment outcomes and safety of mobocertinib in platinum-pretreated patients with EGFR exon 20 insertion-positive metastatic non-small cell lung cancer: A phase ½ open-label nonrandomized clinical trial. JAMA Oncol. 2021, 7, e214761. [Google Scholar] [CrossRef] [PubMed]
- Le, X.; Goldman, J.W.; Clarke, J.M.; Tchekmedyian, N.; Piotrowska, Z.; Chu, D.; Bhat, G.; Lebel, F.M.; Socinski, M.A. Poziotinib shows activity and durability of responses in subgroups of previously treated EGFR exon 20 NSCLC patient. J. Clin. Oncol. 2020, 38, 9514. [Google Scholar] [CrossRef]
- Sacher, A.; Le, X.; Cornelissen, R.; Shum, E.; Suga, J.; Socinski, M.; Molina, J.R.; Haura, E.; Clarke, J.; Bhat, G.; et al. 36MO Safety, tolerability and preliminary efficacy of poziotinib with twice daily strategy in EGFR/HER2 exon 20 mutant non-small cell lung cancer. Ann. Oncol. 2021, 32, S15. [Google Scholar] [CrossRef]
- Xu, Y.; Yang, J.C.; Chiu, C.; Hsu, P.; Mitchell, P.; Chang, C.I.; John, T.; Bazhenova, L.; Kim, T.M.; Yip, C.W.; et al. Efficacy and safety of sunvozertinib in treatment naïve NSCLC patients with EGFR exon20 insertion mutations. J. Clin. Oncol. 2023, 41, 9073. [Google Scholar] [CrossRef]
- Riudavets, M.; Sullivan, I.; Abdayem, P.; Planchard, D. Targeting HER2 in non-small-cell lung cancer (NSCLC): A glimpse of hope? An updated review on therapeutic strategies in NSCLC harbouring HER2 alterations. ESMO Open 2021, 6, 100260. [Google Scholar] [CrossRef] [PubMed]
- Hyman, D.M.; Piha-Paul, S.A.; Won, H.; Rodon, J.; Saura, C.; Shapiro, G.I.; Juric, D.; Quinn, D.I.; Moreno, V.; Doger, B.; et al. HER kinase inhibition in patients with HER2- and HER3-mutant cancers. Nature 2018, 554, 189–194. [Google Scholar] [CrossRef]
- Li, B.T.; Shen, R.; Buonocore, D.; Olah, Z.T.; Ni, A.; Ginsberg, M.S.; Ulaner, G.A.; Offin, M.; Feldman, D.; Hembrough, T.; et al. Ado-trastuzumab emtansine for patients with HER2-mutant lung cancers: Results from a phase II basket trial. J. Clin. Oncol. 2018, 36, 2532–2537. [Google Scholar] [CrossRef]
- Le, X.; Cornelissen, R.; Carassino, M.; Clarke, J.M.; Tchekmedyian, N.; Goldman, J.W.; Leu, S.; Bhat, G.; Lebel, F.; Heymach, J.V.; et al. Poziotinib in non-small-cell lung cancer habouring HER2 exon 20 insertion mutations after prior therapies: ZENITH20-2 Trial. J. Clin. Oncol. 2022, 40, 710–718. [Google Scholar] [CrossRef]
- Han, H.; Li, S.; Chen, T.; Fitzgerald, M.; Liu, S.; Peng, C.; Tang, K.H.; Cao, S.; Chouitar, J.; Wu, J.; et al. Targeting HER2 exon 20 insertion-mutant lung adenocarcinoma with a novel tyrosine kinase inhibitor mobocertinib. Cancer Res. 2021, 81, 5311–5324. [Google Scholar] [CrossRef]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H.; Mazieres, J.; Nagasaka, M.; Bazhenova, L.; Saltos, A.N.; Felip, E.; et al. Trastuzumab Deruxtecan in HER2-mutant non-small-cell lung cancer. N. Engl. J. Med. 2022, 386, 241–251. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Prelaj, A.; Baik, C.; Le, X.; Garassino, M.; Wollner, M.; Haura, E.; Piotrowska, Z.; Socinski, M.; Dreiling, L.; et al. 26MO Efficacy and safety of poziotinib in treatment-naïve HER2 exon 20 insertion (ex20ins) mutated non-small cell lung cancer (NSCLC): ZENITH20-4 [abstract]. Ann. Oncol. 2022, 33, S13. [Google Scholar] [CrossRef]
- Mountzios, G.; Planchard, D.; Metro, G.; Tsiouda, D.; Prelaj, A.; Lampaki, S.; Shalata, W.; Riudavets, M.; Christopoulos, P.; Girard, N.; et al. Molecular epidemiology and treatment patterns of patients with EGFR exon 20-mutant NSCLC in the precision oncology Era: The European EXOTIC registry. JTO Clin. Res. Rep. 2022, 4, 100433. [Google Scholar] [CrossRef]
- Ahn, B.; Han, Y.; Kim, H.R.; Hong, M.H.; Cho, B.C.; Lim, S.M. Real world characteristics and clinical outcomes of HER2-mutant non-small cell lung cancer patients detected by next-generation sequencing. Cancer Res. Treat. 2023, 55, 488–497. [Google Scholar] [CrossRef]
- Prelaj, A.; Bottiglieri, A.; Proto, C.; Russo, G.L.; Signorelli, D.; Ferrara, R.; Galli, G.; De Toma, A.; Viscardi, G.; Brambilla, M.; et al. Poziotinib for EGFR and HER2 exon 20 insertion mutation in advanced NSCLC: Results from the expanded access program. Eur. J. Cancer 2021, 149, 235–248. [Google Scholar] [CrossRef]
- O’Sullivan, D.E.; Jarada, T.N.; Yusuf, A.; Hu, L.; Gogna, P.; Brenner, D.R.; Abbie, E.; Rose, J.B.; Eaton, K.; Elia-Pacitti, J.; et al. Prevalence, treatment patterns, and outcomes of individuals with EGFR positive metastatic non-small cell lung cancer in a Canadian real-world setting: A comparison of exon 19 deletion, L858R, and exon 20 insertion EGFR mutation carriers. Curr. Oncol. 2022, 29, 7198–7208. [Google Scholar] [CrossRef]
- Elamin, Y.Y.; Robichaux, J.P.; Carter, B.W.; Altan, M.; Tran, H.; Gibbons, D.L.; Heeke, S.; Fossella, F.V.; Lam, V.K.; Le, X.; et al. Poziotinib for EGFR exon 20-mutant NSCLC: Clinical efficacy, resistance mechanisms, and impact of insertion location on drug sensitivity. Cancer Cell 2022, 40, 754–767. [Google Scholar] [CrossRef]
- Addeo, A.; Passaro, A.; Malapelle, U.; Banna, G.L.; Subbiah, V.; Friedlaender, A. Immunotherapy in non-small cell lung cancer harbouring driver mutations. Cancer Treat. Rev. 2021, 96, 102179. [Google Scholar] [CrossRef]
- Mazieres, J.; Drilon, A.; Lusque, A.; Mhanna, L.; Cortot, A.B.; Mezquita, L.; Thai, A.A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: Results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- Choudhury, N.J.; Schoenfeld, A.J.; Flynn, J.; Falcon, C.J.; Rizvi, H.; Rudin, C.M.; Kris, M.G.; Arcila, M.E.; Heller, G.; Yu, H.A.; et al. Response to standard therapies and comprehensive genomic analysis for patients with lung adenocarcinoma with EGFR exon 20 insertions. Clin. Cancer Res. 2021, 27, 2920–2927. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.C.M.; Fares, A.F.; Le, L.W.; Mackay, K.M.; Soberano, S.; Chan, S.W.; Smith, E.; Ryan, M.; Tsao, M.S.; Bradbury, P.A.; et al. Subtypes of EGFR- and HER2-mutant metastatic NSCLC influence response to immune checkpoint inhibitors. Clin. Lung Cancer 2021, 22, 253–259. [Google Scholar] [CrossRef] [PubMed]





| EGFR (N = 84) | HER2 (N = 47) | |
|---|---|---|
| Age (y), median (range) | 66 (37–87) | 67 (27–97) |
| Sex | ||
| Male | 33 (39) | 20 (43) |
| Female | 51 (61) | 27 (57) |
| Ethnicity | ||
| Asian | 41 (49) | 19 (40) |
| Non-Asian | 43 (51) | 28 (60) |
| Smoking status (pack years) | ||
| Never | 47 (56) | 26 (55) |
| Light (</=10) | 16 (19) | 4 (9) |
| Heavy (>10) | 21 (25) | 15 (32) |
| Unknown | 0 (0) | 2 (4) |
| Stage at initial diagnosis | ||
| 1 | 6 (7) | 2 (4) |
| 2 | 12 (14) | 3 (6) |
| 3 | 8 (10) | 11 (23) |
| 4 | 58 (69) | 31 (67) |
| Performance status (ECOG) | ||
| 0 | 17 (20) | 7 (15) |
| 1 | 38 (45) | 26 (55) |
| 2 | 8 (10) | 6 (13) |
| 3 | 16 (19) | 7 (15) |
| 4 | 5 (6) | 1 (2) |
| Histology, N (%) | ||
| Adeno | 80 (95) | 46 (98) |
| Adenosquamous | 3 (4) | 1 (2) |
| Squamous | 1 (1) | 0 (0) |
| Palliative systemic therapy, N (%) | ||
| Total who received | 39 (46) | 25 (53) |
| Did not receive | 45 (54) | 22 (47) |
| # Lines, median (range) | 1 (0–5) | 1 (0–5) |
| N who received TKIs | 20 (24) | 11 (23) |
| N who received immunotherapy | 15 (19) | 17 (36) |
| Palliative radiation, N (%) | 51 (61) | 20 (43) |
| Prior curative intent treatment, N (%) | ||
| Surgery | 19 (23) | 6 (13) |
| Radiation | 3 (4) | 3 (6) |
| Combined modality | 4 (5) | 7 (15) |
| Sites of metastasis, N (%) | ||
| Pleura | 39 (46) | 27 (57) |
| Liver | 18 (21) | 9 (19) |
| Adrenal gland | 9 (11) | 8 (17) |
| Bone | 46 (55) | 23 (49) |
| Brain | 31 (37) | 12 (26) |
| A. EGFR Cohort. | ||
|---|---|---|
| Exon 20 mutation status | ||
| Insertion/duplication | 83 (99) | |
| Point mutation | 1 (1) | |
| Other concomitant EGFR mutations | ||
| Exon 18 point mutation | 2 | |
| Exon 21 L858R | 1 | |
| Other molecular alterations (N) | ||
| CDKN2A | 3 | |
| BRCA1 | 2 | |
| BRCA2 | 1 | |
| SDHA | 1 | |
| SDHB | 1 | |
| PIK3CA | 2 | |
| NF1 | 1 | |
| SMAD4 | 1 | |
| PTEN | 1 | |
| MSH2 | 1 | |
| Overall | 12 | |
| B. HER2 cohort | ||
| Exon 20 mutation status | ||
| Insertion/duplication | 47 (100) | |
| Other molecular alterations (N) | ||
| KRAS G12C | 1 (2) | |
| BRCA1 | 1 (2) | |
| SDHC | 1 (2) | |
| APC | 1 (2) | |
| PIK3CA | 1 (2) | |
| PTEN | 1 (2) | |
| Overall | 6 (13) | |
| C. PD-L1 status | ||
| PD-L1 | EGFR | HER2 |
| <1% | 30 (36) | 23 (49) |
| 1–49% | 25 (30) | 10 (21) |
| 50%+ | 21 (25) | 9 (19) |
| unknown | 8 (10) | 5 (11) |
| EGFR | HER2 | |
|---|---|---|
| All STs | 15.4% (6/39) | 16% (4/25) |
| ex20ins TKI | 20% (4/20) * | 9% (1/11) ** |
| A. EGFR Cohort | ||
|---|---|---|
| Type of Systemic Therapy | Best Response | Time to Progression (Months) (Median, Range) |
| Chemo-IO (N = 4) | PR (3/4, 75%) | 8.6 (3.0–10.5) |
| SD (0/4, 0%) | ||
| PD (1/4, 25%) | ||
| IO monotherapy (N = 11) | PR (3/11, 27%) | 3.0 (0.5–21.2) |
| SD (1/11, 9%) | ||
| PD (7/11, 64%) | ||
| Chemotherapy (N = 19) | PR (3/19, 16%) | 4.73 (0.5–13.0) |
| SD (13/19, 68%) | ||
| PD (3/19, 16%) | ||
| PD-L1 50% or higher receiving IO monotherapy (N = 7) | PR (3/7, 43%) | 3.0 (1.2–21.2) |
| SD (1/7, 14%) | ||
| PD (3/7, 43%) | ||
| B. HER2 cohort | ||
| Type of Systemic Therapy | Best Response | Time to Progression (Months) (Median, Range) |
| Chemo-IO (N = 9) | PR (2/9, 22%) | 6.2 (0.5–15.7) |
| SD (4/9, 44%) | ||
| PD (3/9, 33%) | ||
| IO monotherapy (N = 7) | PR (0/7, 0%) | 2.3 (0.9–6.0) |
| SD (2/7, 29%) | ||
| PD (5/7, 71%) | ||
| Chemotherapy (N = 11) | PR (1/11, 9%) | 2.4 (0.9–8.6) |
| SD (5/11, 45%) | ||
| PD (5/11, 45%) | ||
| PD-L1 50% or higher receiving IO monotherapy (N = 3) | PR (0/3, 0%) | 2.3 (1.0–4.5) |
| SD (1/3, 33%) | ||
| PD (2/3, 67%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, K.; Bosdet, I.; Yip, S.; Ho, C.; Laskin, J.; Melosky, B.; Wang, Y.; Sun, S. Real-World Clinical Outcomes for Patients with EGFR and HER2 Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer. Curr. Oncol. 2023, 30, 7099-7111. https://doi.org/10.3390/curroncol30080515
Li K, Bosdet I, Yip S, Ho C, Laskin J, Melosky B, Wang Y, Sun S. Real-World Clinical Outcomes for Patients with EGFR and HER2 Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer. Current Oncology. 2023; 30(8):7099-7111. https://doi.org/10.3390/curroncol30080515
Chicago/Turabian StyleLi, Kelly, Ian Bosdet, Stephen Yip, Cheryl Ho, Janessa Laskin, Barbara Melosky, Ying Wang, and Sophie Sun. 2023. "Real-World Clinical Outcomes for Patients with EGFR and HER2 Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer" Current Oncology 30, no. 8: 7099-7111. https://doi.org/10.3390/curroncol30080515
APA StyleLi, K., Bosdet, I., Yip, S., Ho, C., Laskin, J., Melosky, B., Wang, Y., & Sun, S. (2023). Real-World Clinical Outcomes for Patients with EGFR and HER2 Exon 20 Insertion-Mutated Non-Small-Cell Lung Cancer. Current Oncology, 30(8), 7099-7111. https://doi.org/10.3390/curroncol30080515