Anti-Tumor Effect and Neurotoxicity of Ethanol Adjuvant Therapy after Surgery of a Soft Tissue Sarcoma

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. In Vitro Anti-Tumor Effect of Ethanol Adjuvant Therapy
2.1.1. Cell Line, Cell Culture, and Reagent
2.1.2. In Vitro Measurement of Cell Viability
2.1.3. Wound Healing Assay
2.1.4. Invasion Assay
2.2. In Vivo Anti-Tumor Effect of Ethanol Adjuvant Therapy
2.3. Neurotoxicity of Ethanol Adjuvant Therapy
2.3.1. Evaluation of Electrophysiological Activity of the Sciatic Nerve
2.3.2. Histological Evaluation and Histomorphometry of the Sciatic Nerve
2.4. Statistical Analysis
3. Results
3.1. In Vitro Anti-Tumor Effect of Ethanol Adjuvant Therapy
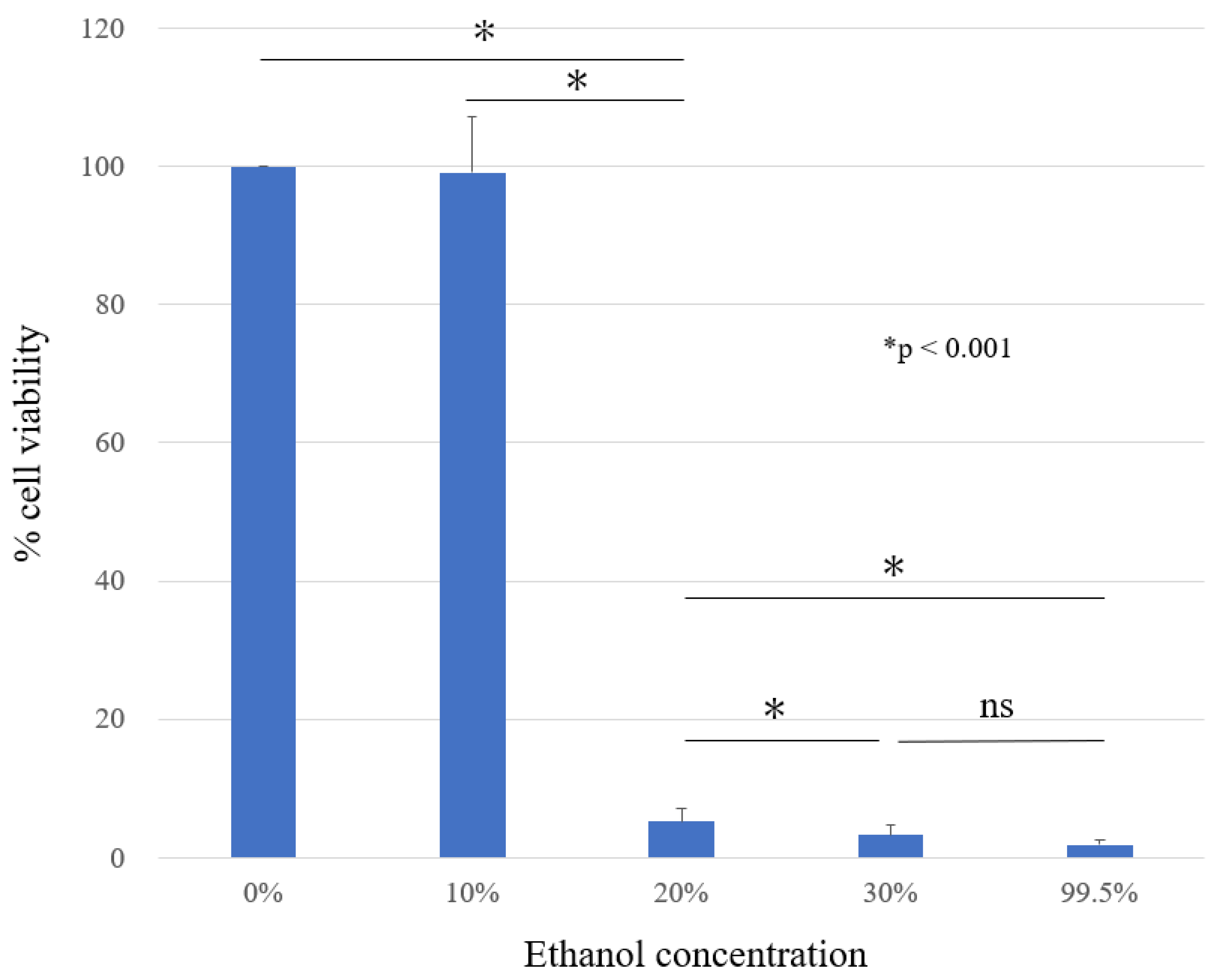
3.1.1. In Vitro Measurement of Cell Viability (MTT Assay)
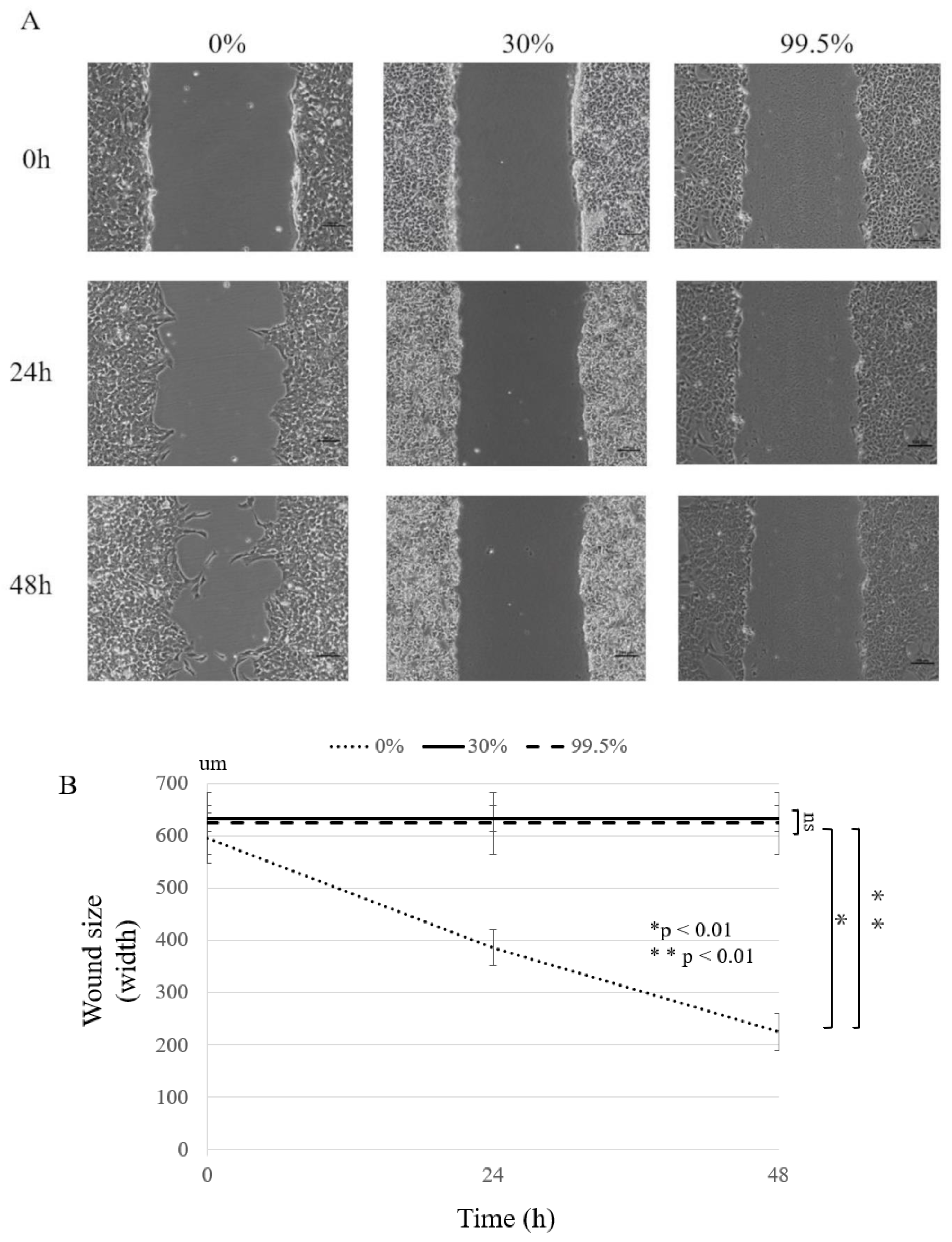
3.1.2. Wound Healing Assay
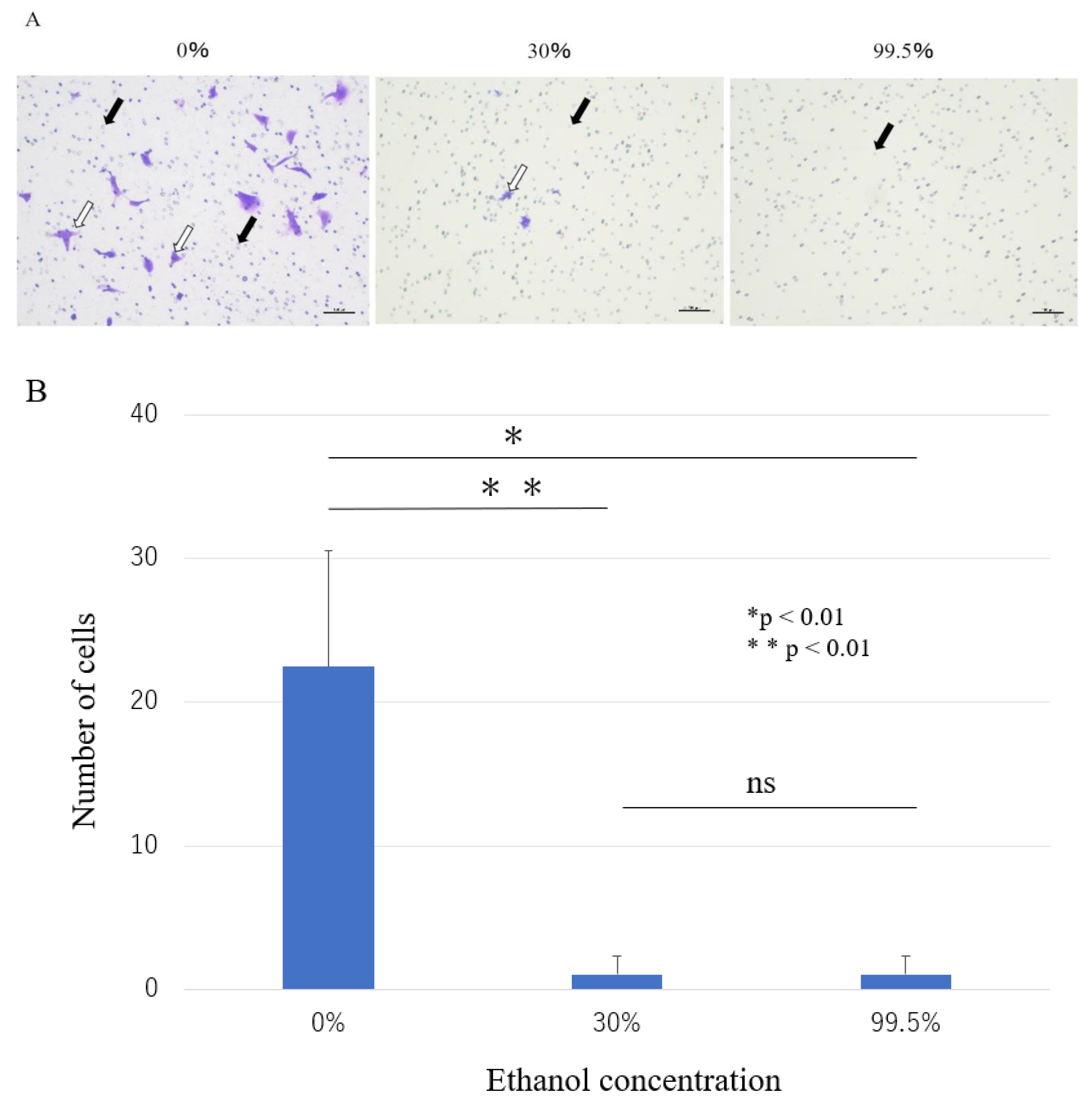
3.1.3. Invasion Assay
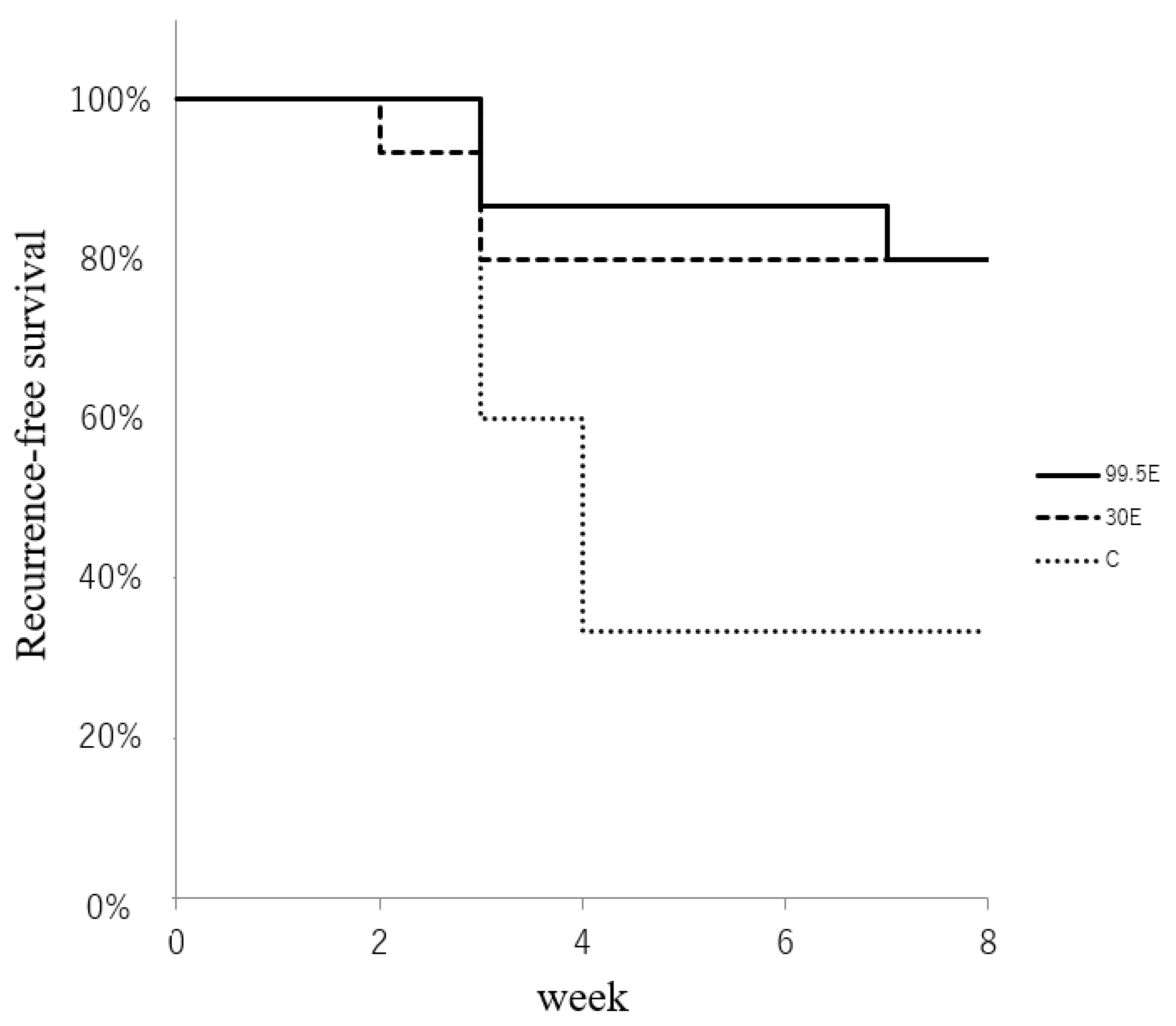
3.2. In Vivo Anti-Tumor Effect of Ethanol Adjuvant Therapy
3.3. Neurotoxicity of Ethanol Adjuvant Therapy In Vivo
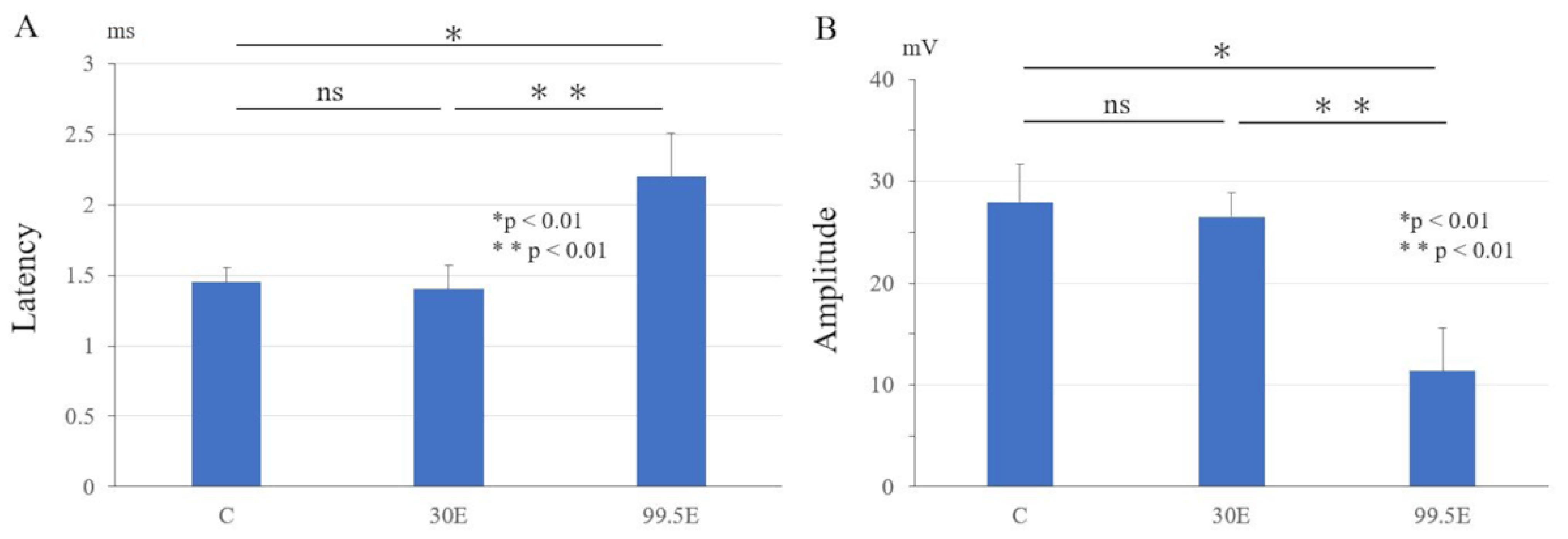
3.3.1. Electrophysiological Examinations of Sciatic Nerve
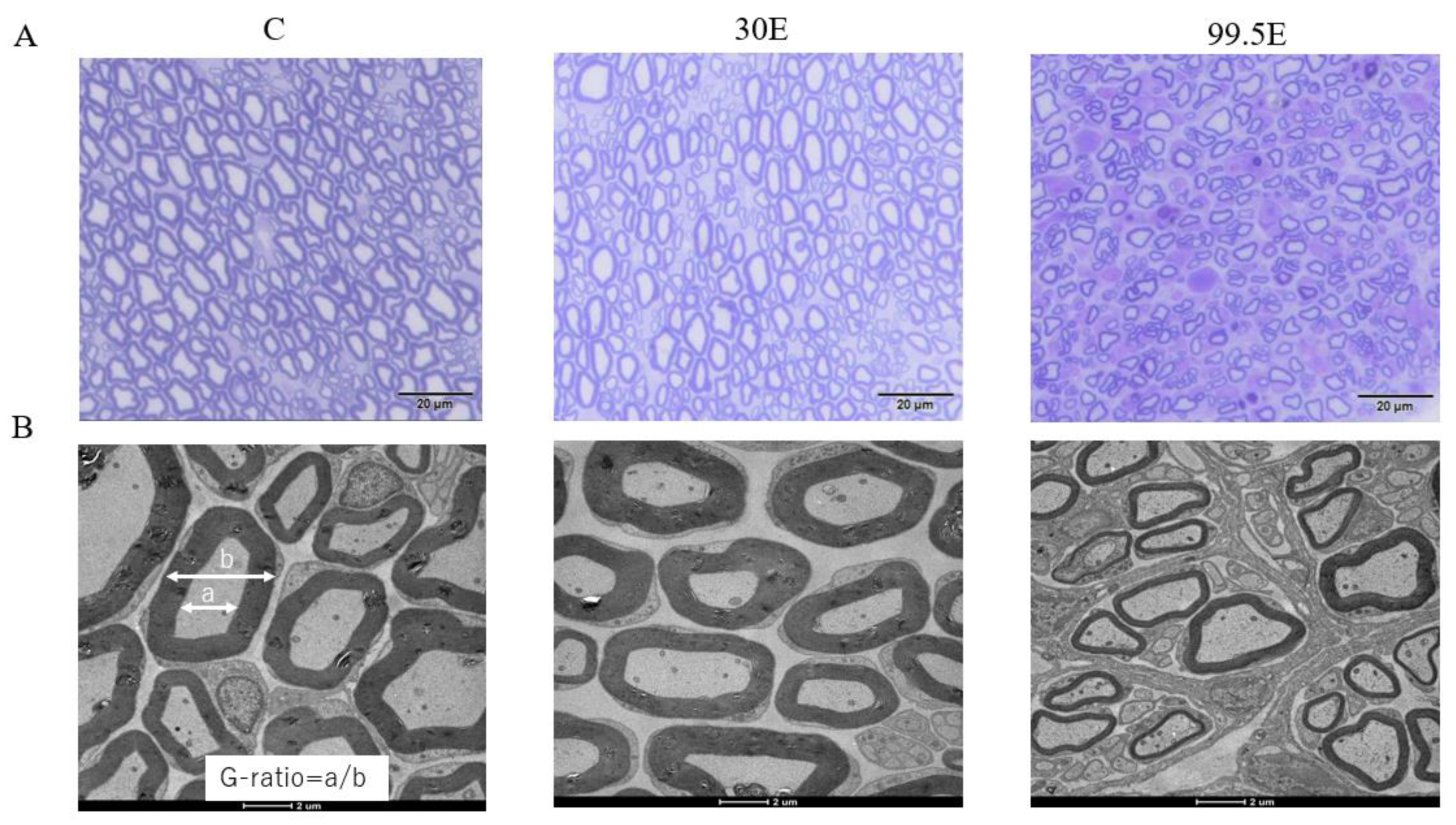
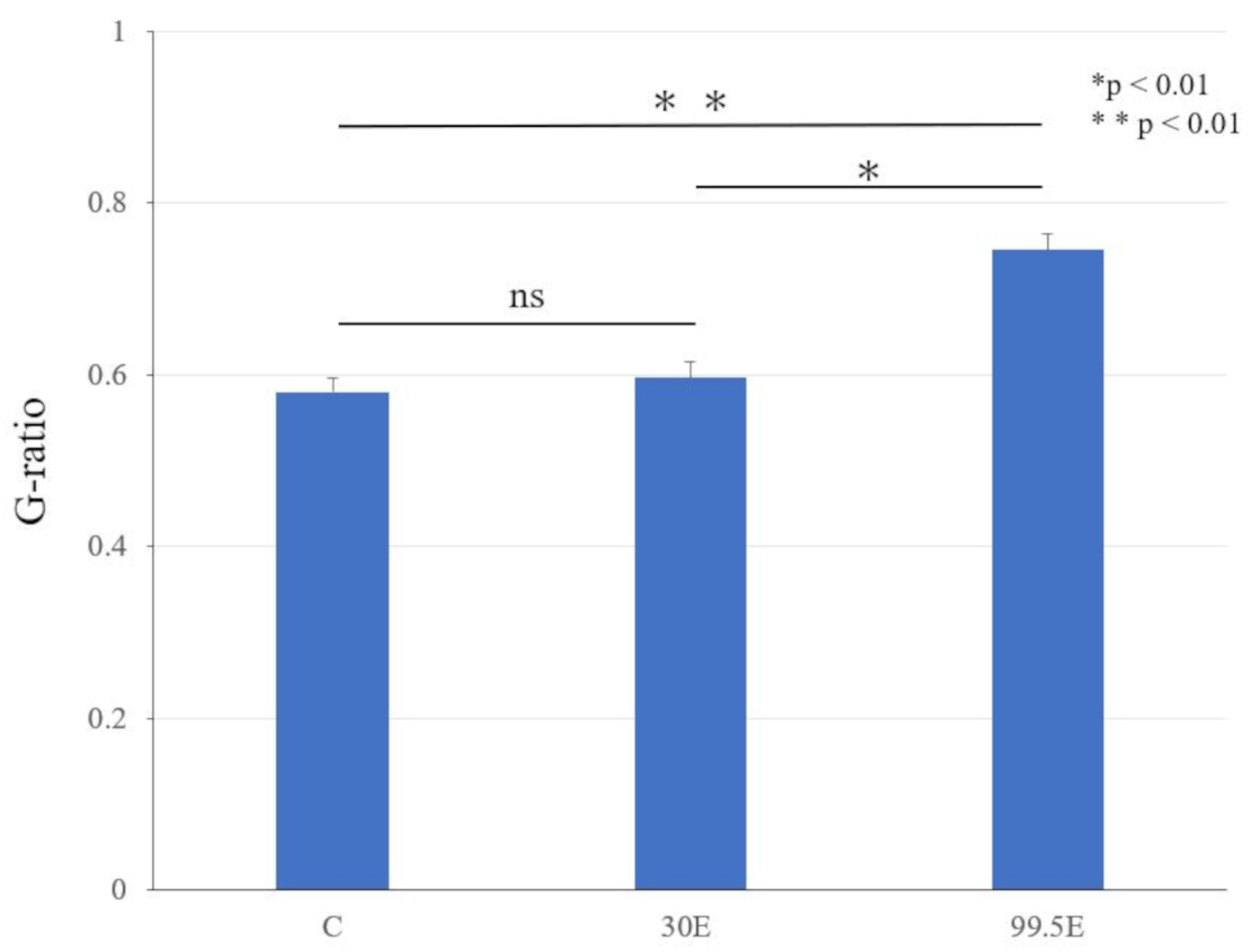
3.3.2. Histological Evaluation and Histomorphometry for Sciatic Nerve
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kawaguchi, N.; Ahmed, A.R.; Matsumoto, S.; Manabe, J.; Matsushita, Y. The concept of curative margin in surgery for bone and soft tissue sarcoma. Clin. Orthop. Relat. Res. 2004, 419, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Guenette, J.P.; Monchik, J.M.; Dupuy, D.E. Image-guided ablation of postsurgical locoregional recurrence of biopsy-proven well-differentiated thyroid carcinoma. J. Vasc. Interv. Radiol. 2013, 24, 672–679. [Google Scholar] [CrossRef] [PubMed]
- Sun, B.; Zhang, W.; Chen, L.; Sun, T.; Ren, Y.; Zhu, L.; Qian, K.; Zheng, C. The safety and efficacy of percutaneous ethanol injection in the treatment of tumor thrombus in advanced hepatocellular carcinoma with portal vein tumor thrombus. Abdom. Radiol. 2022, 47, 858–868. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, S.; Kawaguchi, N.; Manabe, J.; Matsushita, Y. ‘In situ preparation’: New surgical procedure indicated for soft-tissue sarcoma of a lower limb in close proximity to major neurovascular structures. Int. J. Clin. Oncol. 2002, 7, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Aiba, H.; Hayashi, K.; Yamada, S.; Okamoto, H.; Kimura, H.; Miwa, S.; Inatani, H.; Otsuka, T.; Murakami, H. Treatment of a malignant soft tissue tumor arising in the vicinity of the sciatic nerve with an in-situ preparation technique and intensive multidisciplinary therapy. Cancers 2019, 11, 506. [Google Scholar] [CrossRef] [PubMed]
- Sonobe, H.; Manabe, Y.; Furihata, M.; Iwata, J.; Oka, T.; Ohtsuki, Y.; Mizobuchi, H.; Yamamoto, H.; Kumano, O.; Abe, S. Establishment and characterization of a new human synovial sarcoma cell line, HS-SY-II. Lab. Investig. 1992, 67, 498–505. [Google Scholar]
- Justus, C.R.; Leffler, N.; Ruiz-Echevarria, M.; Yang, L.V. In vitro cell migration and invasion assays. J. Vis. Exp. 2014, 88, e51046. [Google Scholar] [CrossRef]
- Habibi, H.; Suzuki, A.; Hayashi, K.; Salimi, H.; Terai, H.; Hori, Y.; Tamai, K.; Orita, K.; Ohyama, S.; Yabu, A.; et al. Expression and function of FGF9 in the hypertrophied ligamentum flavum of lumbar spinal stenosis patients. Spine J. 2021, 21, 1010–1020. [Google Scholar] [CrossRef]
- Liu, M.; Qi, Y.; Zhao, L.; Chen, D.; Zhou, Y.; Zhou, H.; Lv, Y.; Zhang, L.; Jin, S.; Li, S.; et al. Matrix metalloproteinase-14 induces epithelial-to-mesenchymal transition in synovial sarcoma. Hum. Pathol. 2018, 80, 201–209. [Google Scholar] [CrossRef]
- Onode, E.; Uemura, T.; Takamatsu, K.; Yokoi, T.; Shintani, K.; Hhama, S.; Miyashima, Y.; Okada, M.; Nakamura, H. Bioabsorbable nerve conduits three-dimensionally coated with human induced pluripotent stem cell-derived neural stem/progenitor cells promote peripheral nerve regeneration in rats. Sci. Rep. 2021, 11, 4204. [Google Scholar] [CrossRef]
- Gupta, R.; Nassiri, N.; Hazel, A.; Bathen, M.; Mozaffar, T. Chronic nerve compression alters Schwann cell myelin architecture in a murine model. Muscle Nerve 2012, 45, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Hama, S.; Yokoi, T.; Okada, M.; Uemura, T.; Takamatsu, K.; Nakamura, H. Microvascular neural blood flow assessment for a chronic nerve compression neuropathy mouse model by fluorescein angiography. Neurol. Res. 2022, 44, 937–945. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, S.; Zbinden, R.; Mandic, S.; Rüst, C.A.; Aguirre, J.; Borgeat, A. Influence of skin disinfection prior removal of perineural catheter on bacterial colonization, contamination and local inflammation: A prospective randomized study. Minerva Anestesiol. 2018, 84, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Dockery, D.M.; Allu, S.; Vishwanath, N.; Li, T.; Berns, E.; Glasser, J.; Spake, C.S.L.; Antoci, V.; Born, C.T.; Garcia, D.R. Review of pre-operative skin preparation options based on Surgical Site in orthopedic surgery. Surg. Infect. 2021, 22, 1004–1013. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Chen, J.; Wang, H.; Yu, H.; Wang, C.; You, J.; Wang, P.; Feng, C.; Xu, G.; Wu, X.; et al. Memantine can reduce ethanol-induced caspase-3 activity and apoptosis in H4 cells by decreasing intracellular calcium. J. Mol. Neurosci. 2017, 62, 402–411. [Google Scholar] [CrossRef]
- Quintana, M.; Saavedra, E.; Del Rosario, H.; González, I.; Hernández, I.; Estévez, F.; Quintana, J. Ethanol enhances hyperthermia-induced cell death in human leukemia cells. Int. J. Mol. Sci. 2021, 22, 4948. [Google Scholar] [CrossRef]
- Huang, H.; Li, Y.; Wu, M.; Luo, J.; Nie, J.; Hou, B.; He, Q.; Diao, Y.; Qi, L.; Zhao, Y.; et al. Effects of ethanol on the anti-cancer function of doxorubicin in JJ012 cells. Future Oncol. 2018, 14, 1285–1297. [Google Scholar] [CrossRef]
- Liu, J.; Guo, M.; Fan, X. Ethanol induces necroptosis in gastric epithelial cells in vitro. J. Food Biochem. 2021, 45, e13692. [Google Scholar] [CrossRef]
- Kawai, A.; Araki, N.; Ae, K.; Akiyama, T.; Ozaki, T.; Kawano, H.; Kunisada, T.; Sumi, M.; Takahashi, S.; Tanaka, K.; et al. Japanese Orthopaedic Association (JOA) clinical practice guidelines on the management of soft tissue tumors 2020—Secondary publication. J. Orthop. Sci. 2022, 27, 533–550. [Google Scholar] [CrossRef]
- Hashimoto, K.; Nishimura, S.; Oka, N.; Akagi, M. Surgical management of sarcoma in adolescent and young adult patients. BMC Res. Notes 2020, 13, 257. [Google Scholar] [CrossRef]
- Fujiwara, T.; Stevenson, J.; Parry, M.; Tsuda, Y.; Kaneuchi, Y.; Jeys, L. The adequacy of resection margin for non-infiltrative soft-tissue sarcomas. Eur. J. Surg. Oncol. 2021, 47, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Gundle, K.R.; Kafchinski, L.; Gupta, S.; Griffin, A.M.; Dickson, B.C.; Chung, P.W.; Catton, C.N.; O’Sullivan, B.; Wunder, J.S.; Ferguson, P.C. Analysis of margin classification systems for assessing the risk of local recurrence after soft tissue sarcoma resection. J. Clin. Oncol. 2018, 36, 704–709. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.H.; Lan, T.Y.; Chen, C.Y.; Wu, K.; Yang, R.S. Similar local control between phenol- and ethanol-treated giant cell tumors of bone. Clin. Orthop. Relat. Res. 2011, 469, 3200–3208. [Google Scholar] [CrossRef]
- Wang, Y.; Tian, Q.; Wu, C.; Li, H.; Li, J.; Feng, Y. Management of the cavity after removal of giant cell tumor of the bone. Front. Surg. 2021, 8, 626272. [Google Scholar] [CrossRef]
- Gazendam, A.M.; Popovic, S.; Munir, S.; Parasu, N.; Wilson, D.; Ghert, M. Synovial sarcoma: A clinical review. Curr. Oncol. 2021, 28, 1909–1920. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.J.; Kim, H.; Jin, U.S.; Minn, K.W.; Chang, H. Wide local excision for dermatofibrosarcoma protuberans: A single-center series of 90 patients. BioMed Res. Int. 2015, 2015, 642549. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, H.; Nishida, Y.; Nakashima, H.; Yamada, Y.; Tsukushi, S.; Yamada, K. Surgical procedures and prognostic factors for local recurrence of soft tissue sarcomas. J. Orthop. Sci. 2014, 19, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Mastrangelo, G.; Coindre, J.M.; Ducimetière, F.; Dei Tos, A.P.D.; Fadda, E.; Blay, J.Y.; Buja, A.; Fedeli, U.; Cegolon, L.; Frasson, A.; et al. Incidence of soft tissue sarcoma and beyond: A population-based prospective study in 3 European regions. Cancer 2012, 118, 5339–5348. [Google Scholar] [CrossRef] [PubMed]
- Stacchiotti, S.; Van, T.B.A. Synovial sarcoma: Current concepts and future perspectives. J. Clin. Oncol. 2018, 36, 180–187. [Google Scholar] [CrossRef]
- Feng, X.; Huang, Y.L.; Zhang, Z.; Wang, N.; Yao, Q.; Pang, L.J.; Li, F.; Qi, Y. The role of SYT-SSX fusion gene in tumorigenesis of synovial sarcoma. Pathol. Res. Pract. 2021, 222, 153416. [Google Scholar] [CrossRef]
- Scheer, M.; Dantonello, T.; Hallmen, E.; Blank, B.; Sparber-Sauer, M.; Vokuhl, C.; Leuschner, I.; Münter, M.W.; von Kalle, T.V.; Bielack, S.S.; et al. Synovial sarcoma recurrence in children and young adults. Ann. Surg. Oncol. 2016, 23, 618–626. [Google Scholar] [CrossRef]
- Xu, G.; Aiba, H.; Yamamoto, N.; Hayashi, K.; Takeuchi, A.; Miwa, S.; Higuchi, T.; Abe, K.; Taniguchi, Y.; Araki, Y.; et al. Efficacy of perioperative chemotherapy for synovial sarcoma: A retrospective analysis of a Nationwide database in Japan. BMC Cancer 2021, 21, 773. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Zhong, N.; Zhao, C.; Xu, W.; He, S.; Zhao, J.; Yang, X.; Xiao, J. Surgical management and outcome of synovial sarcoma in the spine. World J. Surg. Oncol. 2018, 16, 175. [Google Scholar] [CrossRef] [PubMed]
- Sweiti, H.; Tamimi, N.; Bormann, F.; Divo, M.; Schulz-Ertner, D.; Ahrens, M.; Ronellenfitsch, U.; Schwarzbach, M. Limb-salvage surgery of soft tissue sarcoma with sciatic nerve involvement. Sarcoma 2018, 2018, 6483579. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; Athanasou, N.; Gibbons, C.L.M.H.; Cosker, T.D.A. The management and outcome of large volume liposarcomas encasing the sciatic nerve. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 1537–1542. [Google Scholar] [CrossRef]
- Yokoi, T.; Uemura, T.; Takamatsu, K.; Shintani, K.; Onode, E.; Okada, M.; Hidaka, N.; Nakamura, H. Bioabsorbable nerve conduits coated with induced pluripotent stem cell-derived neurospheres enhance axonal regeneration in sciatic nerve defects in aged mice. J. Biomed. Mater. Res. B Appl. Biomater. 2018, 106, 1752–1758. [Google Scholar] [CrossRef]
- Shintani, K.; Uemura, T.; Takamatsu, K.; Yokoi, T.; Onode, E.; Okada, M.; Tabata, Y.; Nakamura, H. Evaluation of dual release of stromal cell-derived factor-1 and basic fibroblast growth factor with nerve conduit for peripheral nerve regeneration: An experimental study in mice. Microsurgery 2020, 40, 377–386. [Google Scholar] [CrossRef]
- Kocabas, H.; Salli, A.; Demir, A.H.; Ozerbil, O.M. Comparison of phenol and alcohol neurolysis of tibial nerve motor branches to the gastrocnemius muscle for treatment of spastic foot after stroke: A randomized controlled pilot study. Eur. J. Phys. Rehabil. Med. 2010, 46, 5–10. [Google Scholar]
- Verdegaal, S.H.M.; Corver, W.E.; Hogendoorn, P.C.W.; Taminiau, A.H.M. The cytotoxic effect of phenol and ethanol on the chondrosarcoma-derived cell line OUMS-27: An in vitro experiment. J. Bone Jt. Surg. Br. 2008, 90, 1528–1532. [Google Scholar] [CrossRef]
- Tapani, E.; Taavitsainen, M.; Lindros, K.; Vehmas, T.; Lehtonen, E. Toxicity of ethanol in low concentrations: Experimental evaluation in cell culture. Acta Radiol. 1996, 37, 923–926. [Google Scholar] [CrossRef]
- Hu, W.; Wu, C.; Yuan, C.; Chen, M.; Jin, C.; Zheng, C. Ethanol extracted from radix of Actinidia chinensis inhibits human colon tumor through inhibiting notch-signaling pathway. J. Cancer 2021, 12, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Francis, P.; Namløs, H.M.; Müller, C.; Edén, P.; Fernebro, J.; Berner, J.M.; Bjerkehagen, B.; Åkerman, M.; Bendahl, P.O.; Isinger, A.; et al. Diagnostic and prognostic gene expression signatures in 177 soft tissue sarcomas: Hypoxia-induced transcription profile signifies metastatic potential. BMC Genom. 2007, 8, 73. [Google Scholar] [CrossRef] [PubMed]
- Cederbaum, A.I. Alcohol metabolism. Clin. Liver Dis. 2012, 16, 667–685. [Google Scholar] [CrossRef] [PubMed]
- Rice, J.; Gu, C. Function and mechanism of myelin regulation in alcohol abuse and alcoholism. BioEssays 2019, 41, e1800255. [Google Scholar] [CrossRef]
- Samantaray, S.; Knaryan, V.H.; Patel, K.S.; Mulholland, P.J.; Becker, H.C.; Banik, N.L. Chronic intermittent ethanol induced axon and myelin degeneration is attenuated by calpain inhibition. Brain Res. 2015, 1622, 7–21. [Google Scholar] [CrossRef]
- Jang, S.H.; Ahn, S.H.; Park, S.M.; Kim, S.H.; Lee, K.H.; Lee, Z.I. Alcohol neurolysis of tibial nerve motor branches to the gastrocnemius muscle to treat ankle spasticity in patients with hemiplegic stroke. Arch. Phys. Med. Rehabil. 2004, 85, 506–508. [Google Scholar] [CrossRef]
- Le Daré, B.; Gicquel, T. Therapeutic applications of ethanol: A review. J. Pharm. Pharm. Sci. 2019, 22, 525–535. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ban, Y.; Hoshi, M.; Oebisu, N.; Orita, K.; Iwai, T.; Yao, H.; Nakamura, H. Anti-Tumor Effect and Neurotoxicity of Ethanol Adjuvant Therapy after Surgery of a Soft Tissue Sarcoma. Curr. Oncol. 2023, 30, 5251-5265. https://doi.org/10.3390/curroncol30060399
Ban Y, Hoshi M, Oebisu N, Orita K, Iwai T, Yao H, Nakamura H. Anti-Tumor Effect and Neurotoxicity of Ethanol Adjuvant Therapy after Surgery of a Soft Tissue Sarcoma. Current Oncology. 2023; 30(6):5251-5265. https://doi.org/10.3390/curroncol30060399
Chicago/Turabian StyleBan, Yoshitaka, Manabu Hoshi, Naoto Oebisu, Kumi Orita, Tadashi Iwai, Hana Yao, and Hiroaki Nakamura. 2023. "Anti-Tumor Effect and Neurotoxicity of Ethanol Adjuvant Therapy after Surgery of a Soft Tissue Sarcoma" Current Oncology 30, no. 6: 5251-5265. https://doi.org/10.3390/curroncol30060399
APA StyleBan, Y., Hoshi, M., Oebisu, N., Orita, K., Iwai, T., Yao, H., & Nakamura, H. (2023). Anti-Tumor Effect and Neurotoxicity of Ethanol Adjuvant Therapy after Surgery of a Soft Tissue Sarcoma. Current Oncology, 30(6), 5251-5265. https://doi.org/10.3390/curroncol30060399