Predictors of Prostate Cancer at Fusion Biopsy: The Role of Positive Family History, Hypertension, Diabetes, and Body Mass Index

 ,
,
Abstract
1. Introduction
2. Materials and Methods
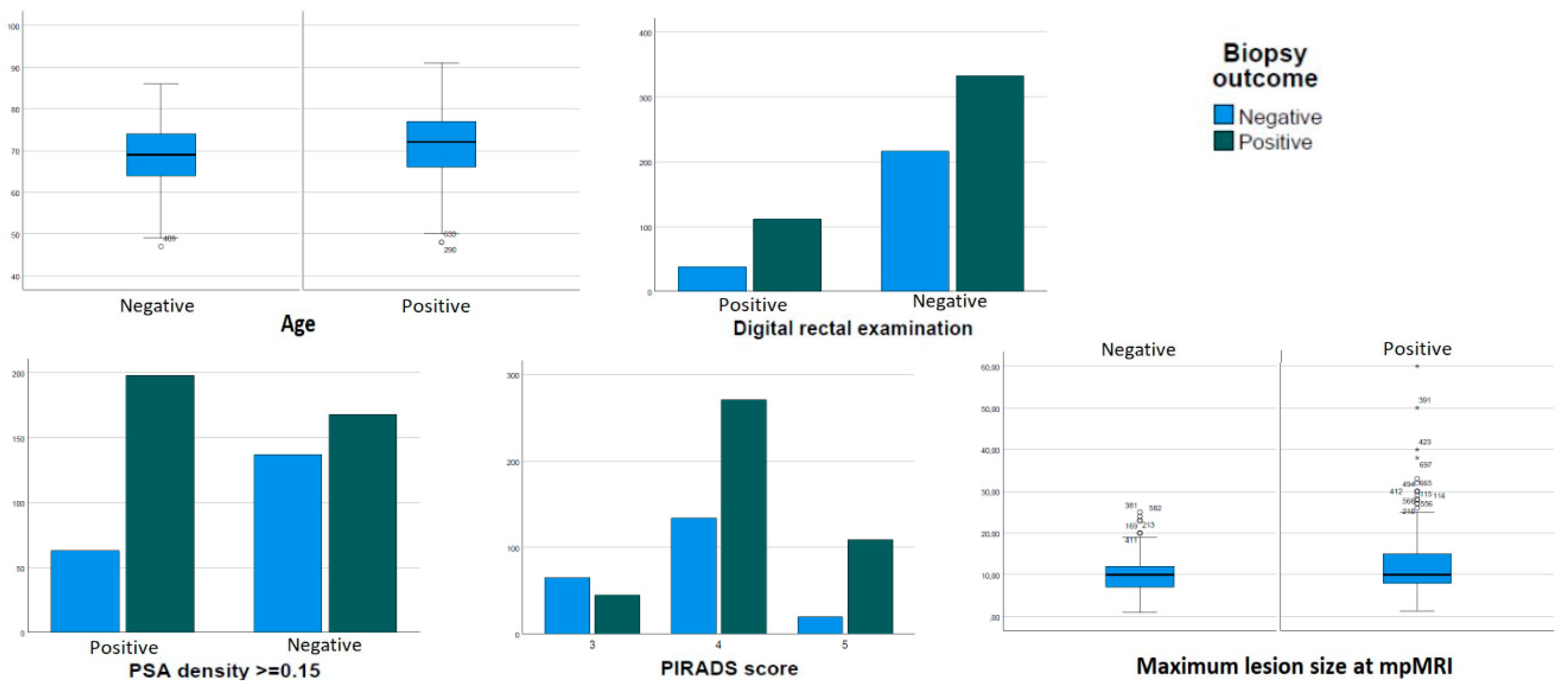
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Culp, M.B.; Soerjomataram, I.; Efstathiou, J.A.; Bray, F.; Jemal, A. Recent Global Patterns in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2020, 77, 38–52. [Google Scholar] [CrossRef] [PubMed]
- IARC; WHO. Data Visualization Tools for Exploring the Global Cancer Burden in 2020. Available online: https://gco.iarc.fr/today/home (accessed on 25 March 2023).
- Ann, W.H.; Hsing, A.W.; Chokkalingam, A.P. Prostate cancer epidemiology. Front. Biosci. 2006, 11, 1388–1413. [Google Scholar] [CrossRef]
- Hemminki, K. Familial risk and familial survival in prostate cancer. World J. Urol. 2012, 30, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Jansson, K.F.; Akre, O.; Garmo, H.; Bill-Axelson, A.; Adolfsson, J.; Stattin, P.; Bratt, O. Concordance of Tumor Differentiation Among Brothers with Prostate Cancer. Eur. Urol. 2012, 62, 656–661. [Google Scholar] [CrossRef]
- Haenszel, W.; Kurihara, M. Studies of Japanese migrants. I. Mortality from cancer and other diseases among Japanese in the United States. J. Natl. Cancer Inst. 2012, 30, 143–148. [Google Scholar] [CrossRef]
- Shimizu, H.; Ross, R.K.; Bernstein, L.; Yatani, R.; E Henderson, B.; Mack, T.M. Cancers of the prostate and breast among Japanese and white immigrants in Los Angeles County. Br. J. Cancer 1991, 63, 963–966. [Google Scholar] [CrossRef]
- Haas, G.P.; Delongchamps, N.; Brawley, O.W.; Wang, C.Y.; De La Roza, G. The worldwide epidemiology of prostate cancer: Perspectives from autopsy studies. Can. J. Urol. 2008, 15, 3866–3871. [Google Scholar]
- Fleshner, K.; Carlsson, S.; Roobol, M.J. The effect of the USPSTF PSA screening recommendation on prostate cancer incidence patterns in the USA. Nat. Rev. Urol. 2017, 14, 26–37. [Google Scholar] [CrossRef]
- Pernar, C.H.; Ebot, E.M.; Wilson, K.M.; Mucci, L.A. The Epidemiology of Prostate Cancer. Cold Spring Harb. Perspect. Med. 2018, 8, a030361. [Google Scholar] [CrossRef]
- Vidal, A.C.; Howard, L.E.; Moreira, D.M.; Castro-Santamaria, R.; Andriole, G.L., Jr.; Freedland, S.J. Obesity Increases the Risk for High-Grade Prostate Cancer: Results from the REDUCE Study. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2936–2942. [Google Scholar] [CrossRef]
- Esposito, K.; Chiodini, P.; Capuano, A.; Bellastella, G.; Maiorino, M.I.; Parretta, E.; Lenzi, A.; Giugliano, D. Effect of metabolic syndrome and its components on prostate cancer risk: Meta-analysis. J. Endocrinol. Investig. 2013, 36, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Eberli, D.; De Meerleer, G.; De Santis, M.; Gillessen, S.; Grummet, J.; Henry, A.M.; et al. EAU Guidelines. Edn. presented at the EAU Annual Congress Milan; EAU Guidelines Office: Arnhem, The Netherlands, 2023; ISBN 978-94-92671-19-6. Available online: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (accessed on 25 March 2023).
- Oderda, M.; Albisinni, S.; Benamran, D.; Calleris, G.; Ciccariello, M.; Dematteis, A.; Diamand, R.; Descotes, J.; Fiard, G.; Forte, V.; et al. Accuracy of elastic fusion biopsy: Comparing prostate cancer detection between targeted and systematic biopsy. Prostate 2023, 83, 162–168. [Google Scholar] [CrossRef] [PubMed]
- Barentsz, J.O.; Weinreb, J.C.; Verma, S.; Thoeny, H.C.; Tempany, C.M.; Shtern, F.; Padhani, A.R.; Margolis, D.; Macura, K.J.; Haider, M.A.; et al. Synopsis of the PI-RADS v2 Guidelines for Multiparametric Prostate Magnetic Resonance Imaging and Recommendations for Use. Eur. Urol. 2016, 69, 41–49. [Google Scholar] [CrossRef] [PubMed]
- Bossuyt, P.M.; Reitsma, J.B.; E Bruns, D.; A Gatsonis, C.; Glasziou, P.P.; Irwig, L.; Lijmer, J.G.; Moher, D.; Rennie, D.; de Vet, H.C.W.; et al. STARD 2015: An Updated List of Essential Items for Reporting Diagnostic Accuracy Studies. Clin. Chem. 2015, 61, 1446–1452. [Google Scholar] [CrossRef]
- Pourmand, G.; Salem, S.; Mehrsai, A.; Lotfi, M.; Amirzargar, M.; Mazdak, H.; Roshani, A.; Kheirollahi, A.R.; Kalantar, E.; Baradaran, N.; et al. The risk factors of prostate cancer: A multicentric case-control study in Iran. Asian Pac. J. Cancer Prev. 2007, 8, 422–428. [Google Scholar]
- American Cancer Society: Facts & Figures 2015; American Cancer Society: Atlanta, GA, USA, 2015.
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Haiman, C.A.; Chen, G.K.; Blot, W.J.; Strom, S.S.; Berndt, S.I.; Kittles, R.A.; Rybicki, B.A.; Isaacs, W.B.; Ingles, S.A.; Stanford, J.L.; et al. Characterizing Genetic Risk at Known Prostate Cancer Susceptibility Loci in African Americans. PLOS Genet. 2011, 7, e1001387. [Google Scholar] [CrossRef]
- Center, M.M.; Jemal, A.; Lortet-Tieulent, J.; Ward, E.; Ferlay, J.; Brawley, O.; Bray, F. International Variation in Prostate Cancer Incidence and Mortality Rates. Eur. Urol. 2012, 61, 1079–1092. [Google Scholar] [CrossRef]
- Hemminki, K.; Czene, K. Attributable risks of familial cancer from the Family-Cancer Database. Cancer Epidemiol. Biomark. Prev. 2002, 11, 1638–1644. [Google Scholar]
- Mucci, L.A.; Hjelmborg, J.B.; Harris, J.R.; Czene, K.; Havelick, D.J.; Scheike, T.; Graff, R.E.; Holst, K.; Möller, S.; Nordic Twin Study of Cancer (NorTwinCan) Collaboration. Familial Risk and Heritability of Cancer Among Twins in Nordic Countries. JAMA 2016, 315, 68–76. [Google Scholar] [CrossRef]
- Lange, E.M.; Salinas, C.A.; Zuhlke, K.A.; Ray, A.M.; Wang, Y.; Lu, Y.; Ho, L.A.; Luo, J.; Cooney, K. Early onset prostate cancer has a significant genetic component. Prostate 2012, 72, 147–156. [Google Scholar] [CrossRef] [PubMed]
- Jahn, J.L.; Giovannucci, E.L.; Stampfer, M.J. The high prevalence of undiagnosed prostate cancer at autopsy: Implications for epidemiology and treatment of prostate cancer in the Prostate-specific Antigen-era. Int. J. Cancer 2015, 137, 2795–2802. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Ma, J. Body Mass Index, Prostate Cancer–Specific Mortality, and Biochemical Recurrence: A Systematic Review and Meta-analysis. Cancer Prev. Res. 2011, 4, 486–501. [Google Scholar] [CrossRef]
- Bashir, M.N.; Ahmad, M.R.; Malik, A. Risk Factors of Prostate Cancer: A Case-control Study in Faisalabad, Pakistan. Asian Pac. J. Cancer Prev. 2014, 15, 10237–10240. [Google Scholar] [CrossRef]
- Rivera-Izquierdo, M.; de Rojas, J.P.; Martínez-Ruiz, V.; Pérez-Gómez, B.; Sánchez, M.-J.; Khan, K.S.; Jiménez-Moleón, J.J. Obesity as a Risk Factor for Prostate Cancer Mortality: A Systematic Review and Dose-Response Meta-Analysis of 280,199 Patients. Cancers 2021, 13, 4169. [Google Scholar] [CrossRef]
- Bandini, M.; Gandaglia, G.; Briganti, A. Obesity and prostate cancer. Curr. Opin. Urol. 2017, 27, 415–421. [Google Scholar] [CrossRef]
- Wallner, L.P.; Morgenstern, H.; McGree, M.E.; Jacobson, D.J.; Sauver, J.L.S.; Jacobsen, S.J.; Sarma, A.V. The effects of metabolic conditions on prostate cancer incidence over 15 years of follow-up: Results from the Olmsted County Study. BJU Int. 2011, 107, 929–935. [Google Scholar] [CrossRef] [PubMed]
- Blanc-Lapierre, A.; Spence, A.R.; Karakiewicz, P.I.; Aprikian, A.G.; Saad, F.; Parent, M.É. Metabolic syndrome and prostate cancer risk in a population-based case–control study in Montreal, Canada. BMC Public Health 2015, 15, 913. [Google Scholar] [CrossRef]
- Bhindi, B.; Locke, J.; Alibhai, S.M.; Kulkarni, G.S.; Margel, D.S.; Hamilton, R.J.; Finelli, A.; Trachtenberg, J.; Zlotta, A.R.; Toi, A.; et al. Dissecting the Association Between Metabolic Syndrome and Prostate Cancer Risk: Analysis of a Large Clinical Cohort. Eur. Urol. 2015, 67, 64–70. [Google Scholar] [CrossRef]
- Montano, D. Association Between Socioeconomic Determinants and the Metabolic Syndrome in the German Health Interview and Examination Survey for Adults (DEGS1)—A Mediation Analysis. Rev. Diabet. Stud. 2017, 14, 279–294. [Google Scholar] [CrossRef]
- Kaneko, M.; Sugano, D.; Lebastchi, A.H.; Duddalwar, V.; Nabhani, J.; Haiman, C.; Gill, I.S.; Cacciamani, G.E.; Abreu, A.L. Techniques and Outcomes of MRI-TRUS Fusion Prostate Biopsy. Curr. Urol. Rep. 2021, 22, 27. [Google Scholar] [CrossRef] [PubMed]
- Oderda, M.; Marra, G.; Albisinni, S.; Altobelli, E.; Baco, E.; Beatrici, V.; Cantiani, A.; Carbone, A.; Ciccariello, M.; Descotes, J.-L.; et al. Accuracy of elastic fusion biopsy in daily practice: Results of a multicenter study of 2115 patients. Int. J. Urol. 2018, 25, 990–997. [Google Scholar] [CrossRef]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budäus, L.; Hellawell, G.; Hindley, R.G.; et al. ECISION Study Group Collaborators. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef] [PubMed]
- Pagniez, M.A.; Kasivisvanathan, V.; Puech, P.; Drumez, E.; Villers, A.; Olivier, J. Predictive Factors of Missed Clinically Significant Prostate Cancers in Men with Negative Magnetic Resonance Imaging: A Systematic Review and Meta-Analysis. J. Urol. 2020, 204, 24–32. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | All Patients | Missing Data | Patients with Positive Biopsy | Patients with Negative Biopsy | p |
|---|---|---|---|---|---|
| Patients | 736 | - | 465 (63.2%) | 271 (36.8%) | |
| Age; years; median (IQR) | 71 (11) | 1 (0.1%) | 72 (11) | 69 (10) | <0.001 |
| BMI; mean (SD) | 25.8 (3.4) | 370 (50.2%) | 25.8 (3.4) | 25.9 (3.5) | 0.78 |
| Hypertension; n (%) | 399 (54.2%) | 13 (1.8%) | 253 (63.4%) | 146 (36.6%) | 1.00 |
| Diabetes; n (%) | 66 (9%) | 27 (3.7%) | 46 (69.7%) | 20 (30.3%) | 0.28 |
| Positive family history for PCa; n (%) | 55 (7.5%) | 97 (13.2%) | 36 (65.5%) | 19 (34.5%) | 0.77 |
| PSA; ng/mL; median (IQR) | 6.5 (4.3) | 7 (0.9%) | 6.8 (4.5) | 6.1 (3.8) | 0.13 |
| PSA density; ng/mL/mL; median (IQR) | 0.14 (0.12) | 170 (23.1%) | 0.16 (0.12) | 0.11 (0.10) | <0.001 |
| PSA density ≥0.15; n (%) | 261 (35.5) | 170 (23.1%) | 198 (75.9%) | 63 (24.1%) | <0.001 |
| Positive DRE; n (%) | 150 (20.4) | 37 (5.0%) | 112 (74.7%) | 38 (25.3%) | 0.002 |
| Prostate volume; cc; median (IQR) | 48 (35) | 168 (22.8%) | 42 (26) | 60 (40) | <0.001 |
| Previous negative biopsies; n (%) | 168 (22.8%) | 5 (0.7%) | 105 (62.5%) | 63 (37.5%) | 0.85 |
| Single mpMRI target; n (%) | 544 (73.9%) | 55 (7.5%) | 340 (62.5%) | 204 (37.5%) | 0.009 |
| Size of targets; mm; mean (SD) | 11.5 (6.2) | 106 (14.4%) | 12.3 (6.9) | 10.1 (4.4) | <0.001 |
| PIRADS of targets (maximum score if multiple); n (%) | |||||
| 110 (14.9%) | 92 (12.5%) | 45 (40.9%) | 65 (59.1%) | <0.001 |
| 405 (55.0%) | 271 (66.9%) | 134 (33.1%) | ||
| 129 (17.5%) | 109 (84.5%) | 20 (15.5%) | ||
| Cancer detection rate; n (%) | 465 (63.2%) | 0 (0%) | 465 (63.2%) | - | - |
| Clinically significant cancer detection rate; n (%) | 432 (58.7%) | 0 (0%) | 432 (58.7%) | - | - |
| PCa ISUP score; n (%) | |||||
| 33 (7.0%) | 33 (7.0%) | |||
| 199 (42.8%) | 199 (42.8%) | |||
| 144 (31.0%) | 144 (31.0%) | |||
| 61 (13.2%) | 61 (13.2%) | |||
| 28 (6.0%) | 28 (6.0%) |
| All PCa | CsPCa | |||
|---|---|---|---|---|
| Variable | Uni-Variable | Multi-Variable | Uni-Variable | Multi-Variable |
| Age | 1.04 (1.02–1.06) | 1.04 (1.02–1.07) | 1.05 (1.03–1.07) | 1.04 (1.01–1.07) |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | |
| Body mass index | 0.99 (0.93–1.05) | - | 0.97 (0.91–1.03) | - |
| p = 0.78 | p = 0.33 | |||
| Hypertension | 1.00 (0.74–1.36) | - | 0.98 (0.73–1.33) | - |
| p = 0.97 | p = 0.93 | |||
| Diabetes | 1.38 (0.80–2.40) | - | 1.36 (0.80–2.31) | - |
| p = 0.24 | p = 0.25 | |||
| Positive family history for PCa | 1.12 (0.63–2.01) | - | 1.20 (0.68–2.12) | - |
| p = 0.68 | p = 0.52 | |||
| PSA (ng/mL) | 1.02 (0.99–1.05) | - | 1.01 (0.99–1.04) | - |
| p = 0.15 | p = 0.22 | |||
| Positive DRE | 1.91 (1.27–2.86) | 1.47 (0.84–2.59) | 2.15 (1.45–3.20) | 1.75 (1.01–3.02) |
| p = 0.002 | p = 0.17 | p < 0.001 | p = 0.04 | |
| PSA density ≥0.15 | 2.56 (1.78–3.68) | 2.68 (1.73–4.15) | 2.41 (1.70–3.42) | 2.47 (1.62–3.76) |
| p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 | |
| Previous negative biopsy | 0.95 (0.66–1.36) | - | 0.91 (0.64–1.29) | - |
| p = 0.79 | p = 0.61 | |||
| PIRADS score | - | - | - | - |
| 3 | 2.92 (1.89–4.50) | 2.74 (1.61–4.68) | 3.31 (2.19–5.17) | 3.31 (1.91–5.73) |
| 4 | p < 0.001 | p < 0.001 | p < 0.001 | p < 0.001 |
| 7.87 (4.27–14.48) | 4.02 (1.62–9.96) | 7.81 (4.35–14.02) | 3.56 (1.50–8.45) | |
| 5 | p < 0.001 | p = 0.003 | p < 0.001 | p = 0.004 |
| Size of the lesion (mm) | 1.07 (1.03–1.10) | 1.03 (0.98–1.09) | 1.05 (1.02–1.08) | 1.04 (0.98–1.10) |
| p < 0.001 | p = 0.19 | p < 0.001 | p = 0.12 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oderda, M.; Dematteis, A.; Calleris, G.; Conti, A.; D’Agate, D.; Falcone, M.; Marquis, A.; Montefusco, G.; Marra, G.; Gontero, P. Predictors of Prostate Cancer at Fusion Biopsy: The Role of Positive Family History, Hypertension, Diabetes, and Body Mass Index. Curr. Oncol. 2023, 30, 4957-4965. https://doi.org/10.3390/curroncol30050374
Oderda M, Dematteis A, Calleris G, Conti A, D’Agate D, Falcone M, Marquis A, Montefusco G, Marra G, Gontero P. Predictors of Prostate Cancer at Fusion Biopsy: The Role of Positive Family History, Hypertension, Diabetes, and Body Mass Index. Current Oncology. 2023; 30(5):4957-4965. https://doi.org/10.3390/curroncol30050374
Chicago/Turabian StyleOderda, Marco, Alessandro Dematteis, Giorgio Calleris, Adriana Conti, Daniele D’Agate, Marco Falcone, Alessandro Marquis, Gabriele Montefusco, Giancarlo Marra, and Paolo Gontero. 2023. "Predictors of Prostate Cancer at Fusion Biopsy: The Role of Positive Family History, Hypertension, Diabetes, and Body Mass Index" Current Oncology 30, no. 5: 4957-4965. https://doi.org/10.3390/curroncol30050374
APA StyleOderda, M., Dematteis, A., Calleris, G., Conti, A., D’Agate, D., Falcone, M., Marquis, A., Montefusco, G., Marra, G., & Gontero, P. (2023). Predictors of Prostate Cancer at Fusion Biopsy: The Role of Positive Family History, Hypertension, Diabetes, and Body Mass Index. Current Oncology, 30(5), 4957-4965. https://doi.org/10.3390/curroncol30050374