Histological and Genetic Diversity in Ovarian Mucinous Carcinomas: A Pilot Study

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Tumor Samples
2.2. Microdissection and Deoxyribonucleic Acid Extraction
2.3. Direct Sequence Analysis
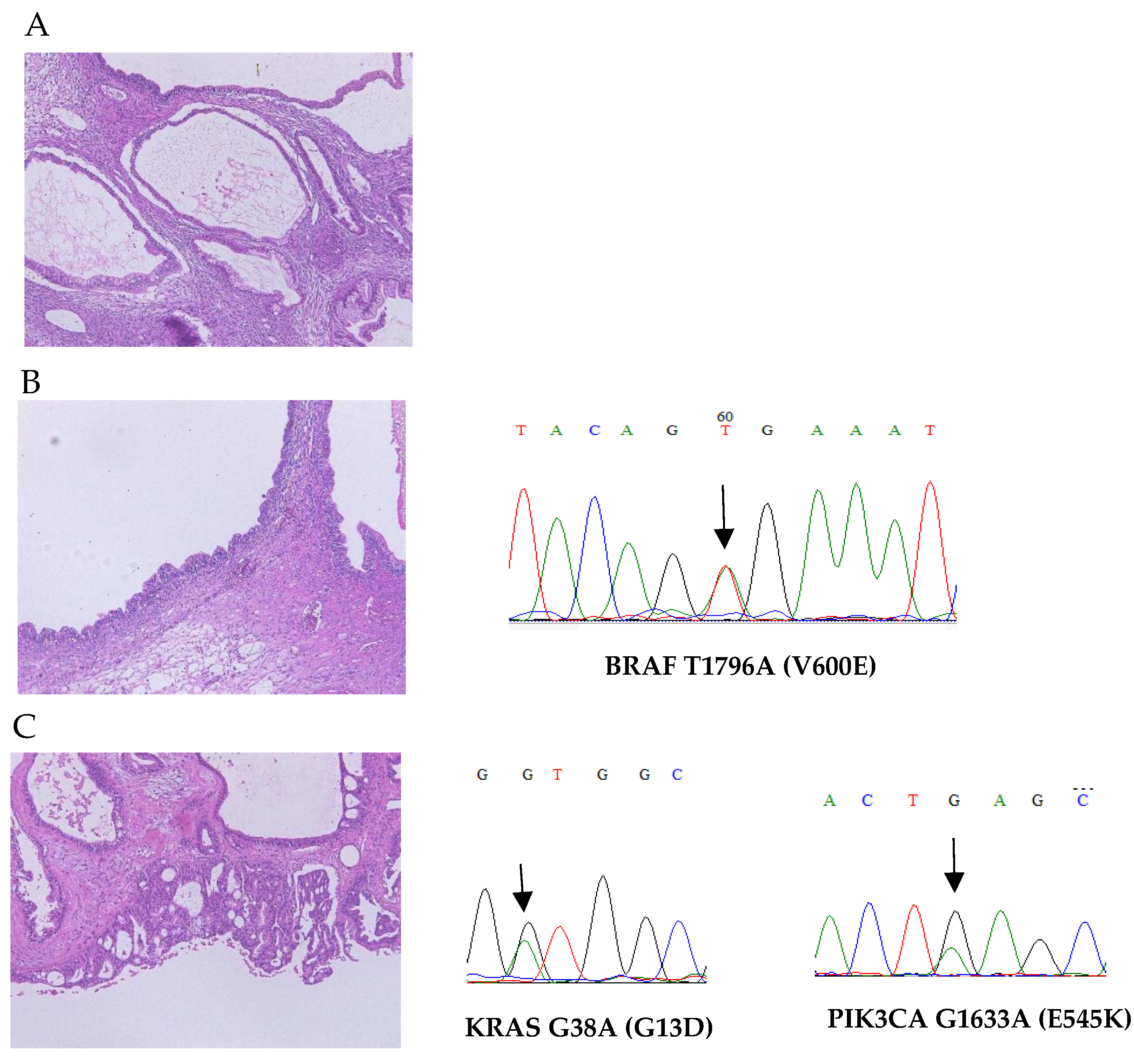
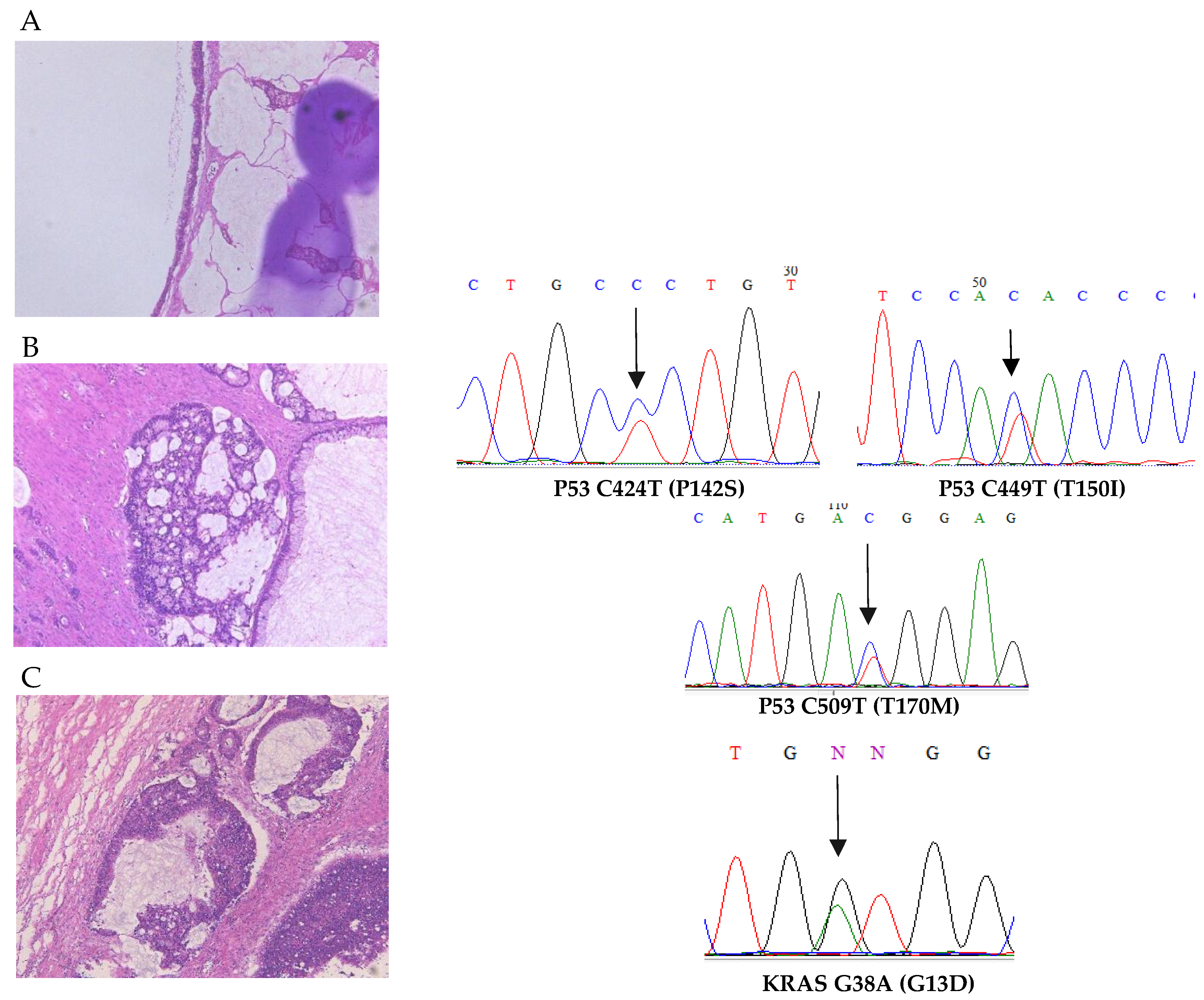
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D. Cancer statistics. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, 359–386. [Google Scholar] [CrossRef] [PubMed]
- Harrison, M.L.; Jameson, C.; Gore, M.E. Mucinous ovarian cancer. Int. J. Gynecol. Cancer 2008, 18, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Bond, V.K.; Eno, M.L.; Im, D.D.; Rosenshein, N.B. Low drug resistance to both platinum and taxane chemotherapy on an in vitro drug resistance assay predicts improved survival in patients with advanced epithelial ovarian, fallopian and peritoneal cancer. Int. J. Cancer 2009, 125, 2721–2727. [Google Scholar] [CrossRef] [PubMed]
- Tabrizi, A.D.; Kalloger, S.E.; Kobel, M.; Cipollone, J.; Roskelley, C.D.; Mehl, E.; Gilks, C.B. Primary ovarian mucinous carcinoma of intestinal type: Significance of pattern of invasion and immunohistochemical expression profile in a series of 31 cases. Int. J. Gynecol. Pathol. 2010, 29, 99–107. [Google Scholar] [CrossRef] [PubMed]
- Alexandre, J.; Ray-Coquard, I.; Selle, F.; Floquet, A.; Cottu, P.; Weber, B.; Falandry, C.; Lebrun, D.; Pujade-Lauraine, E.; GINECO. Mucinous advanced epithelial ovarian carcinoma: Clinical presentation and sensitivity to platinum-paclitaxel-based chemotherapy, the GINECO experience. Ann. Oncol. 2010, 21, 2377–2381. [Google Scholar] [CrossRef]
- Mackay, H.J.; Brady, M.F.; Oza, A.M.; Reuss, A.; Pujade-Lauraine, E.; Swart, A.M.; Siddiqui, N.; Colombo, N.; Bookman, M.A.; Pfisterer, J.; et al. Prognostic relevance of uncommon ovarian histology in women with stage III/IV epithelial ovarian cancer. Int. J. Gynecol. Cancer 2010, 20, 945–952. [Google Scholar] [CrossRef]
- Lim, D.; Oliva, E. Precursors and pathogenesis of ovarian carcinoma. Pathology 2013, 45, 229–242. [Google Scholar] [CrossRef]
- Mandai, M.; Konishi, I.; Kuroda, H.; Komatsu, T.; Yamamoto, S.; Nanbu, K.; Matsushita, K.; Fukumoto, M.; Yamabe, H.; Mori, T. Heterogeneous distribution of K-RAS-mutated epithelia in mucinous ovarian tumors with special reference to histopathology. Hum. Pathol. 1998, 29, 34–40. [Google Scholar] [CrossRef]
- Takeshima, Y.; Amatya, V.J.; Daimaru, Y.; Nakayori, F.; Nakano, T.; Inai, K. Heterogeneous genetic alterations in ovarian mucinous tumors: Application and usefulness of laser capture microdissection. Hum. Pathol. 2001, 32, 1203–1208. [Google Scholar] [CrossRef]
- Mok, S.C.; Bell, D.A.; Knapp, R.C.; Fishbaugh, P.M.; Welch, W.R.; Muto, M.G.; Berkowitz, R.S.; Tsao, S.W. Mutation of K-ras protooncogene in human ovarian epithelial tumors of borderline malignancy. Cancer Res. 1993, 53, 1489–1492. [Google Scholar]
- Ricci, F.; Affatato, R.; Carrassa, L.; Damia, G. Recent insights into mucinous ovarian carcinoma. Int. J. Mol. Sci. 2018, 19, 6. [Google Scholar] [CrossRef] [PubMed]
- Mackenzie, R.; Kommoss, S.; Winterhoff, B.J.; Kipp, B.R.; Garcia, J.J.; Voss, J.; Halling, K.; Karnezis, A.; Senz, J.; Yang, W.; et al. Targeted deep sequencing of mucinous ovarian tumors reveals multiple overlapping RAS-pathway activating mutations in borderline and cancerous neoplasms. BMC Cancer 2015, 15, 415. [Google Scholar] [CrossRef]
- Ohnishi, K.; Nakayama, K.; Ishikawa, M.; Ishibashi, T.; Yamashita, H.; Nakamura, K.; Minamoto, T.; Iida, K.; Razia, S.; Ishikawa, N.; et al. Mucinous borderline ovarian tumors with BRAF V600E mutation may have low risk for progression to invasive carcinomas. Arch. Gynecol. Obstet. 2020, 302, 487–495. [Google Scholar] [CrossRef]
- Nakayama, K.; Nakayama, N.; Kurman, R.J.; Cope, L.; Pohl, G.; Samuels, Y.; Velculescu, V.E.; Wang, T.L.; Shih, I.M. Sequence mutations and amplification of PIK3CA and AKT2 genes in purified ovarian serous neoplasms. Cancer Biol. Ther. 2006, 5, 779–785. [Google Scholar] [CrossRef]
- Forbes, S.A.; Beare, D.; Boutselakis, H.; Bamford, S.; Bindal, N.; Tate, J.; Cole, C.G.; Ward, S.; Dawson, E.; Ponting, L.; et al. COSMIC: Somatic cancer genetics at high-resolution. Nucleic Acids Res. 2017, 45, D777–D783. [Google Scholar] [CrossRef] [PubMed]
- Gorringe, K.L.; Cheasley, D.; Wakefield, M.; Ryland, G.L.; Allan, P.E.; Alsop, K.; Amarasinghe, K.C.; Ananda, S.; Bowtell, D.D.; Christie, M.; et al. Therapeutic options for mucinous ovarian carcinoma. Gynecol. Oncol. 2020, 156, 552–560. [Google Scholar] [CrossRef]
- Anglesio, M.S.; Kommoss, S.; Tolcher, M.C.; Clarke, B.; Galletta, L.; Porter, H.; Damaraju, S.; Fereday, S.; Winterhoff, B.J.; Kalloger, S.E.; et al. Molecular characterization of mucinous ovarian tumours supports a stratified treatment approach with HER2 targeting in 19% of carcinomas. J. Pathol. 2013, 229, 111–120. [Google Scholar] [CrossRef] [PubMed]
- Rechsteiner, M.; Zimmermann, A.K.; Wild, P.J.; Caduff, R.; Von, T.A.; Fink, D.; Moch, H.; Noske, A. TP53 mutations are common in all subtypes of epithelial ovarian cancer and occur concomitantly with KRAS mutations in the mucinous type. Exp. Mol. Pathol. 2013, 95, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.; Ali, S.; Wang, K.; Palmer, G.; Yelensky, R.; Lipson, D.; Miller, V.; Zajchowski, D.; Shawver, L.; Stephens, P. Comprehensive genomic profiling of epithelial ovarian cancer by next generation sequencing-based diagnostic assay reveals new routes to targeted therapies. Gynecol. Oncol. 2013, 130, 554–559. [Google Scholar] [CrossRef]
- Teer, J.K.; Yoder, S.; Gjyshi, A.; Nicosia, S.V.; Zhang, C.; Monteiro, A.N.A. Mutational heterogeneity in non-serous ovarian cancers. Sci. Rep. 2017, 7, 9728. [Google Scholar] [CrossRef] [PubMed]
- Cheasley, D.; Wakefield, M.J.; Ryland, G.L.; Allan, P.E.; Alsop, K.; Amarasinghe, K.C.; Ananda, S.; Anglesio, M.S.; Au-Yeung, G.; Böhm, M.; et al. The molecular origin and taxonomy of mucinous ovarian carcinoma. Nat. Commun. 2019, 10, 3935. [Google Scholar] [CrossRef] [PubMed]
- Bagué, S.; Rodríguez, I.M.; Prat, J. Sarcoma-like mural nodules in mucinous cystic tumors of the ovary revisited: A clinicopathologic analysis of 10 additional cases. Am. J. Surg. Pathol. 2002, 26, 1467–1476. [Google Scholar] [CrossRef]
- Mesbah, A.N.; Giardina, T.; Amanuel, B.; Stewart, C.J. Molecular profiling reveals a clonal relationship between ovarian mucinous tumors and corresponding mural carcinomatous nodules. Am. J. Surg. Pathol. 2017, 41, 1261–1266. [Google Scholar] [CrossRef]
- Ying, S.; Qin, L.; Haiyan, S.; Bingjian, L. Ovarian mucinous tumors with mural nodules: Immunohistochemical and molecular analysis of 3 cases. Case Reports, Diagn. Pathol. 2020, 15, 35. [Google Scholar] [CrossRef]
- Takeshima, Y.; Inai, K. Genetic alterations in ovarian mucinous tumors-with special reference to the histogenesis. Acta Histochem. Cytochem. 2000, 33, 123–129. [Google Scholar] [CrossRef]
- Ling, S.; Hu, Z.; Yang, Z.; Yang, F.; Li, Y.; Lin, P.; Chen, K.; Dong, L.; Cao, L.; Tao, Y.; et al. Extremely high genetic diversity in a single tumor points to prevalence of non-Darwinian cell evolution. Proc. Natl. Acad. Sci. USA 2015, 112, E6496–E6505. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.J.; Werner, B.; Barnes, C.P.; Graham, T.A.; Sottoriva, A. Identification of neutral tumor evolution across cancer types. Nat. Genet. 2016, 48, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Bozic, I.; Gerold, J.M.; Nowak, M.A. Quantifying clonal and subclonal passenger mutations in cancer evolution. PLoS Comput. Biol. 2016, 12, e1004731. [Google Scholar] [CrossRef]
- Loeb, L.A.; Bielas, J.H.; Beckman, R.A. Cancers exhibit a mutator phenotype: Clinical implications. Cancer Res. 2008, 68, 3551–3557. [Google Scholar] [CrossRef]
- Sottoriva, A.; Kang, H.; Ma, Z.; Graham, T.A.; Salomon, M.P.; Zhao, J.; Marjoram, P.; Siegmund, K.; Press, M.F.; Shibata, D.; et al. A Big Bang model of human colorectal tumor growth. Nat. Genet. 2015, 47, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Donghi, R.; Longoni, A.; Pilotti, S.; Michieli, P.; Della Porta, G.; Pierotti, M.A. Gene p53 mutations are restricted to poorly differentiated and undifferentiated carcinomas of the thyroid gland. J. Clin. Investig. 1993, 91, 1753–1760. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.S.; Lim, J.A.; Park, Y.J. Mutation profile of well-differentiated thyroid cancer in Asians. Endocrinol. Metab. 2015, 30, 252–262. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Case | Tumor Size | Age | Stage (FIGO) | Histologic Category | KRAS | BRAF | TP53 | PIK3CA |
|---|---|---|---|---|---|---|---|---|
| 1 | cystadenoma | WT | WT | WT | WT | |||
| 17 | 56 | IV A | borderline tumor | WT | V600E | WT | WT | |
| carcinoma | G13D | WT | WT | E545K | ||||
| 2 | cystadenoma | WT | WT | WT | WT | |||
| 17 | 77 | I A | borderline tumor | WT | WT | T118I | NA | |
| carcinoma | G12D | WT | WT | WT | ||||
| 3 | cystadenoma | WT | WT | WT | WT | |||
| 18 | 63 | II C | borderline tumor | WT | WT | P142S, T150I, T170M | WT | |
| carcinoma | G13D | WT | WT | WT | ||||
| 4 | cystadenoma | WT | WT | WT | WT | |||
| 16 | 67 | IV A | borderline tumor | WT | WT | E62K, E68K | WT | |
| carcinoma | WT | WT | WT | WT | ||||
| 5 | cystadenoma | WT | WT | WT | WT | |||
| 22 | 81 | I A | borderline tumor | WT | WT | D57N | WT | |
| carcinoma | WT | WT | WT | WT | ||||
| 6 | cystadenoma | WT | WT | WT | WT | |||
| 17 | 78 | I C | borderline tumor | WT | WT | WT | WT | |
| carcinoma | G12D | WT | WT | WT | ||||
| 7 | cystadenoma | WT | WT | WT | WT | |||
| 33 | 47 | III A | borderline tumor | WT | WT | WT | WT | |
| carcinoma | G12D | WT | WT | WT |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razia, S.; Nakayama, K.; Yamashita, H.; Ishibashi, T.; Ishikawa, M.; Kanno, K.; Sato, S.; Kyo, S. Histological and Genetic Diversity in Ovarian Mucinous Carcinomas: A Pilot Study. Curr. Oncol. 2023, 30, 4052-4059. https://doi.org/10.3390/curroncol30040307
Razia S, Nakayama K, Yamashita H, Ishibashi T, Ishikawa M, Kanno K, Sato S, Kyo S. Histological and Genetic Diversity in Ovarian Mucinous Carcinomas: A Pilot Study. Current Oncology. 2023; 30(4):4052-4059. https://doi.org/10.3390/curroncol30040307
Chicago/Turabian StyleRazia, Sultana, Kentaro Nakayama, Hitomi Yamashita, Tomoka Ishibashi, Masako Ishikawa, Kosuke Kanno, Seiya Sato, and Satoru Kyo. 2023. "Histological and Genetic Diversity in Ovarian Mucinous Carcinomas: A Pilot Study" Current Oncology 30, no. 4: 4052-4059. https://doi.org/10.3390/curroncol30040307
APA StyleRazia, S., Nakayama, K., Yamashita, H., Ishibashi, T., Ishikawa, M., Kanno, K., Sato, S., & Kyo, S. (2023). Histological and Genetic Diversity in Ovarian Mucinous Carcinomas: A Pilot Study. Current Oncology, 30(4), 4052-4059. https://doi.org/10.3390/curroncol30040307