Dual-Tracer PET-MRI-Derived Imaging Biomarkers for Prediction of Clinically Significant Prostate Cancer



 , ,
, ,
Abstract
1. Introduction
2. Material and Methods
2.1. Patients
2.2. Imaging Protocol and Analyses
2.3. Follow-Up
2.4. Statistical Analyses
3. Results
3.1. Patients
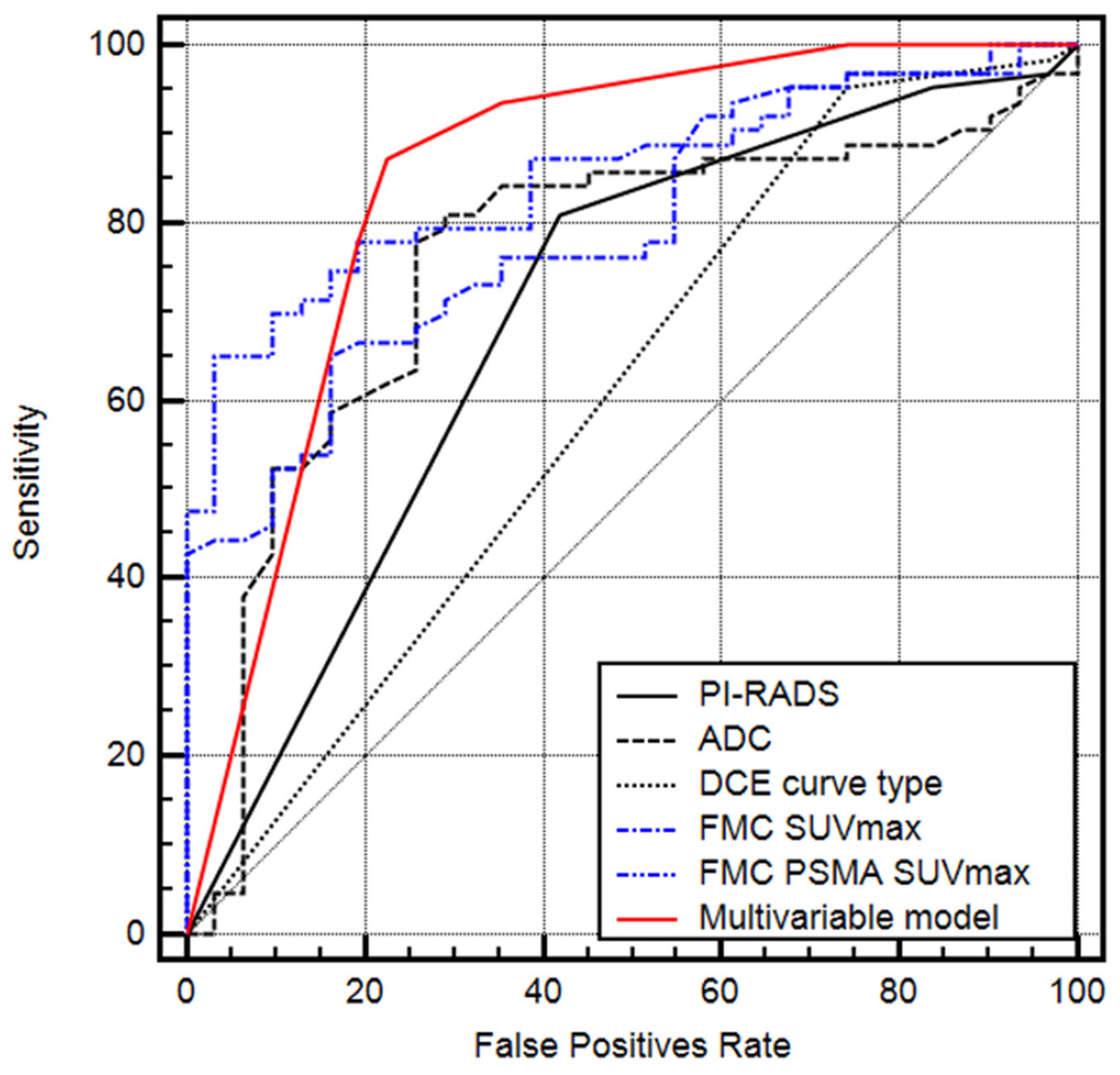
3.2. Prediction of Clinically Significant Prostate Cancer
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Matoso, A.; Epstein, J.I. Defining clinically significant prostate cancer on the basis of pathological findings. Histopathology 2019, 74, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; van den Bergh, R.C.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer—2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2020, 79, 243–262. [Google Scholar] [CrossRef]
- Hayes, J.H.; Ollendorf, D.A.; Pearson, S.D.; Barry, M.J.; Kantoff, P.; Lee, P.A.; McMahon, P.M. Observation Versus Initial Treatment for Men With Localized, Low-Risk Prostate Cancer: A Cost-Effectiveness Analysis. Ann. Intern. Med. 2013, 158, 853. [Google Scholar] [CrossRef]
- Lu-Yao, G.L.; Albertsen, P.C.; Moore, D.F.; Shih, W.; Lin, Y.; DiPaola, R.S.; Barry, M.J.; Zietman, A.; O’Leary, M.; Walker-Corkery, E.; et al. Outcomes of Localized Prostate Cancer Following Conservative Management. JAMA 2009, 302, 1202–1209. [Google Scholar] [CrossRef]
- Ali, A.; Hoyle, A.; Baena, E.; Clarke, N.W. Identification and evaluation of clinically significant prostate cancer. Curr. Opin. Urol. 2017, 27, 217–224. [Google Scholar] [CrossRef]
- Johnson, D.C.; Raman, S.S.; Mirak, S.A.; Kwan, L.; Bajgiran, A.M.; Hsu, W.; Maehara, C.K.; Ahuja, P.; Faiena, I.; Pooli, A.; et al. Detection of Individual Prostate Cancer Foci via Multiparametric Magnetic Resonance Imaging. Eur. Urol. 2019, 75, 712–720. [Google Scholar] [CrossRef]
- Drost, F.H.; Osses, D.F.; Nieboer, D.; Steyerberg, E.W.; Bangma, C.H.; Roobol, M.J.; Schoots, I.G. Prostate MRI, with or without MRI-targeted biopsy, and systematic biopsy for detecting prostate cancer. Cochrane Database Syst. Rev. 2019, 4, CD012663. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Barkovich, E.J.; Shankar, P.R.; Westphalen, A.C. A Systematic Review of the Existing Prostate Imaging Reporting and Data System Version 2 (PI-RADSv2) Literature and Subset Meta-Analysis of PI-RADSv2 Categories Stratified by Gleason Scores. Am. J. Roentgenol. 2019, 212, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Mehralivand, S.; Shih, J.H.; Rais-Bahrami, S.; Oto, A.; Bednarova, S.; Nix, J.W.; Thomas, J.V.; Gordetsky, J.B.; Gaur, S.; Harmon, S.A.; et al. A Magnetic Resonance Imaging–Based Prediction Model for Prostate Biopsy Risk Stratification. JAMA Oncol. 2018, 4, 678. [Google Scholar] [CrossRef] [PubMed]
- Hartenbach, M.; Hartenbach, S.; Bechtloff, W.; Danz, B.; Kraft, K.; Klemenz, B.; Sparwasser, C.; Hacker, M. Combined PET/MRI improves diagnostic accuracy in patients with prostate cancer: A prospective diagnostic trial. Clin. Cancer Res. 2014, 20, 3244–3253. [Google Scholar] [CrossRef] [PubMed]
- Grubmüller, B.; Baltzer, P.; Hartenbach, S.; D’Andrea, D.; Helbich, T.H.; Haug, A.R.; Goldner, G.M.; Wadsak, W.; Pfaff, S.; Mitterhauser, M.; et al. PSMA Ligand PET/MRI for Primary Prostate Cancer: Staging Performance and Clinical Impact. Clin. Cancer Res. 2018, 24, 6300–6307. [Google Scholar] [CrossRef] [PubMed]
- EEiber, M.; Weirich, G.; Holzapfel, K.; Souvatzoglou, M.; Haller, B.; Rauscher, I.; Beer, A.J.; Wester, H.-J.; Gschwend, J.; Schwaiger, M.; et al. Simultaneous 68Ga-PSMA HBED-CC PET/MRI Improves the Localization of Primary Prostate Cancer. Eur. Urol. 2016, 70, 829–836. [Google Scholar] [CrossRef]
- Ahmed, H.U.; El-Shater Bosaily, A.; Brown, L.C.; Gabe, R.; Kaplan, R.; Parmar, M.K.; Collaco-Moraes, Y.; Ward, K.; Hindley, R.G.; Freeman, A.; et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017, 389, 815–822. [Google Scholar] [CrossRef]
- Polanec, S.H.; Helbich, T.H.; Bickel, H.; Wengert, G.J.; Pinker, K.; Spick, C.; Clauser, P.; Susani, M.; Shariat, S.; Baltzer, P.A. Quantitative Apparent Diffusion Coefficient Derived From Diffusion-Weighted Imaging Has the Potential to Avoid Unnecessary MRI-Guided Biopsies of mpMRI-Detected PI-RADS 4 and 5 Lesions. Investig. Radiol. 2018, 53, 736–741. [Google Scholar] [CrossRef]
- Chatterjee, A.; He, D.; Fan, X.; Antic, T.; Jiang, Y.; Eggener, S.; Karczmar, G.S.; Oto, A. Diagnosis of Prostate Cancer by Use of MRI-Derived Quantitative Risk Maps: A Feasibility Study. Am. J. Roentgenol. 2019, 213, W66–W75. [Google Scholar] [CrossRef]
- Wang, Y.; Tadimalla, S.; Rai, R.; Goodwin, J.; Foster, S.; Liney, G.; Holloway, L.; Haworth, A. Quantitative MRI: Defining repeatability, reproducibility and accuracy for prostate cancer imaging biomarker development. Magn. Reson. Imaging 2021, 77, 169–179. [Google Scholar] [CrossRef]
- Berger, I.; Annabattula, C.; Lewis, J.; Shetty, D.V.; Kam, J.; MacLean, F.; Arianayagam, M.; Canagasingham, B.; Ferguson, R.; Khadra, M.; et al. 68Ga-PSMA PET/CT vs. mpMRI for locoregional prostate cancer staging: Correlation with final histopathology. Prostate Cancer Prostatic Dis. 2018, 21, 204–211. [Google Scholar] [CrossRef]
- Metser, U.; Ortega, C.; Perlis, N.; Lechtman, E.; Berlin, A.; Anconina, R.; Eshet, Y.; Chan, R.; Veit-Haibach, P.; van der Kwast, T.H.; et al. Detection of clinically significant prostate cancer with 18F-DCFPyL PET/multiparametric MR. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3702–3711. [Google Scholar] [CrossRef] [PubMed]
- Jairath, N.K.; Pra, A.D.; Vince, R.; Dess, R.T.; Jackson, W.C.; Tosoian, J.J.; McBride, S.M.; Zhao, S.G.; Berlin, A.; Mahal, B.A.; et al. A Systematic Review of the Evidence for the Decipher Genomic Classifier in Prostate Cancer. Eur. Urol. 2020, 79, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Sommariva, S.; Tarricone, R.; Lazzeri, M.; Ricciardi, W.; Montorsi, F. Prognostic Value of the Cell Cycle Progression Score in Patients with Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2016, 69, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Hectors, S.; Cherny, M.; Yadav, K.K.; Beksaç, A.T.; Thulasidass, H.; Lewis, S.; Davicioni, E.; Wang, P.; Tewari, A.K.; Taouli, B. Radiomics Features Measured with Multiparametric Magnetic Resonance Imaging Predict Prostate Cancer Aggressiveness. J. Urol. 2019, 202, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Jambor, I.; Falagario, U.; Ratnani, P.; Msc, I.M.P.; Demir, K.; Merisaari, H.; Sobotka, S.; Haines, G.K.; Martini, A.; Beksac, A.T.; et al. Prediction of biochemical recurrence in prostate cancer patients who underwent prostatectomy using routine clinical prostate multiparametric MRI and decipher genomic score. J. Magn. Reson. Imaging 2020, 51, 1075–1085. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D.; Ng, S.; et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomised, open-label, phase 2 trial. Lancet 2021, 397, 797–804. [Google Scholar] [CrossRef]
- Thang, S.P.; Violet, J.; Sandhu, S.; Iravani, A.; Akhurst, T.; Kong, G.; Kumar, A.R.; Murphy, D.G.; Williams, S.G.; Hicks, R.J.; et al. Poor Outcomes for Patients with Metastatic Castration-resistant Prostate Cancer with Low Prostate-specific Membrane Antigen (PSMA) Expression Deemed Ineligible for 177Lu-labelled PSMA Radioligand Therapy. Eur. Urol. Oncol. 2019, 2, 670–676. [Google Scholar] [CrossRef]


{kind=link}
| Age at RP (years), median (IQR) | 70 (65–76) |
| PSA at RP (ng/mL), median (IQR) | 8.1 (5.6–13.7) |
| Pathologic T staging after RP, n (%) | |
| 2 | 41 (53.2) |
| 3a | 19 (24.7) |
| 3b | 17 (22.1) |
| Positive surgical margins, n (%) | 24 (31.2) |
| ISUP grade on 77 RP specimen, n (%) | |
| 1 | 7 (9.1) |
| 2 | 15 (19.5) |
| 3 | 28 (36.3) |
| 4 | 11 (14.3) |
| 5 | 16 (20.8) |
| Number of cancer foci in all 77 prostates, n (%) | 104 (100) |
| Clinically insignificant cancer foci (ISUP 1) | 35 (33.7) |
| Clinically significant cancer foci (≥ISUP 2), | 69 (66.3) |
| Positive lymph nodes in histopathology, n (%) | 14 (18.2) |
| Overall PI-RADS, n (%) | |
| 3 | 2 (2.6) |
| 4 | 16 (20.8) |
| 5 | 59 (76.6) |
| FMC SUVmax of all cancer foci (MBq), median (IQR) | 5 (4–6.9) |
| FMC + PSMA SUVmax of all cancer foci (MBq), median (IQR) | 14.3 (11.1–20.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grubmüller, B.; Huebner, N.A.; Rasul, S.; Clauser, P.; Pötsch, N.; Grubmüller, K.H.; Hacker, M.; Hartenbach, S.; Shariat, S.F.; Hartenbach, M.; et al. Dual-Tracer PET-MRI-Derived Imaging Biomarkers for Prediction of Clinically Significant Prostate Cancer. Curr. Oncol. 2023, 30, 1683-1691. https://doi.org/10.3390/curroncol30020129
Grubmüller B, Huebner NA, Rasul S, Clauser P, Pötsch N, Grubmüller KH, Hacker M, Hartenbach S, Shariat SF, Hartenbach M, et al. Dual-Tracer PET-MRI-Derived Imaging Biomarkers for Prediction of Clinically Significant Prostate Cancer. Current Oncology. 2023; 30(2):1683-1691. https://doi.org/10.3390/curroncol30020129
Chicago/Turabian StyleGrubmüller, Bernhard, Nicolai A. Huebner, Sazan Rasul, Paola Clauser, Nina Pötsch, Karl Hermann Grubmüller, Marcus Hacker, Sabrina Hartenbach, Shahrokh F. Shariat, Markus Hartenbach, and et al. 2023. "Dual-Tracer PET-MRI-Derived Imaging Biomarkers for Prediction of Clinically Significant Prostate Cancer" Current Oncology 30, no. 2: 1683-1691. https://doi.org/10.3390/curroncol30020129
APA StyleGrubmüller, B., Huebner, N. A., Rasul, S., Clauser, P., Pötsch, N., Grubmüller, K. H., Hacker, M., Hartenbach, S., Shariat, S. F., Hartenbach, M., & Baltzer, P. (2023). Dual-Tracer PET-MRI-Derived Imaging Biomarkers for Prediction of Clinically Significant Prostate Cancer. Current Oncology, 30(2), 1683-1691. https://doi.org/10.3390/curroncol30020129