Comparative Study of Short-Term Efficacy and Safety of Mitomycin versus Lobaplatin for Hyperthermic Intraperitoneal Chemotherapy after Radical Surgery in Colorectal Cancer with High-Risk Factors for Peritoneal Carcinomatosis: A Propensity Score Matching Analysis

 ,
,
Abstract
1. Introduction
2. Patients and Methods
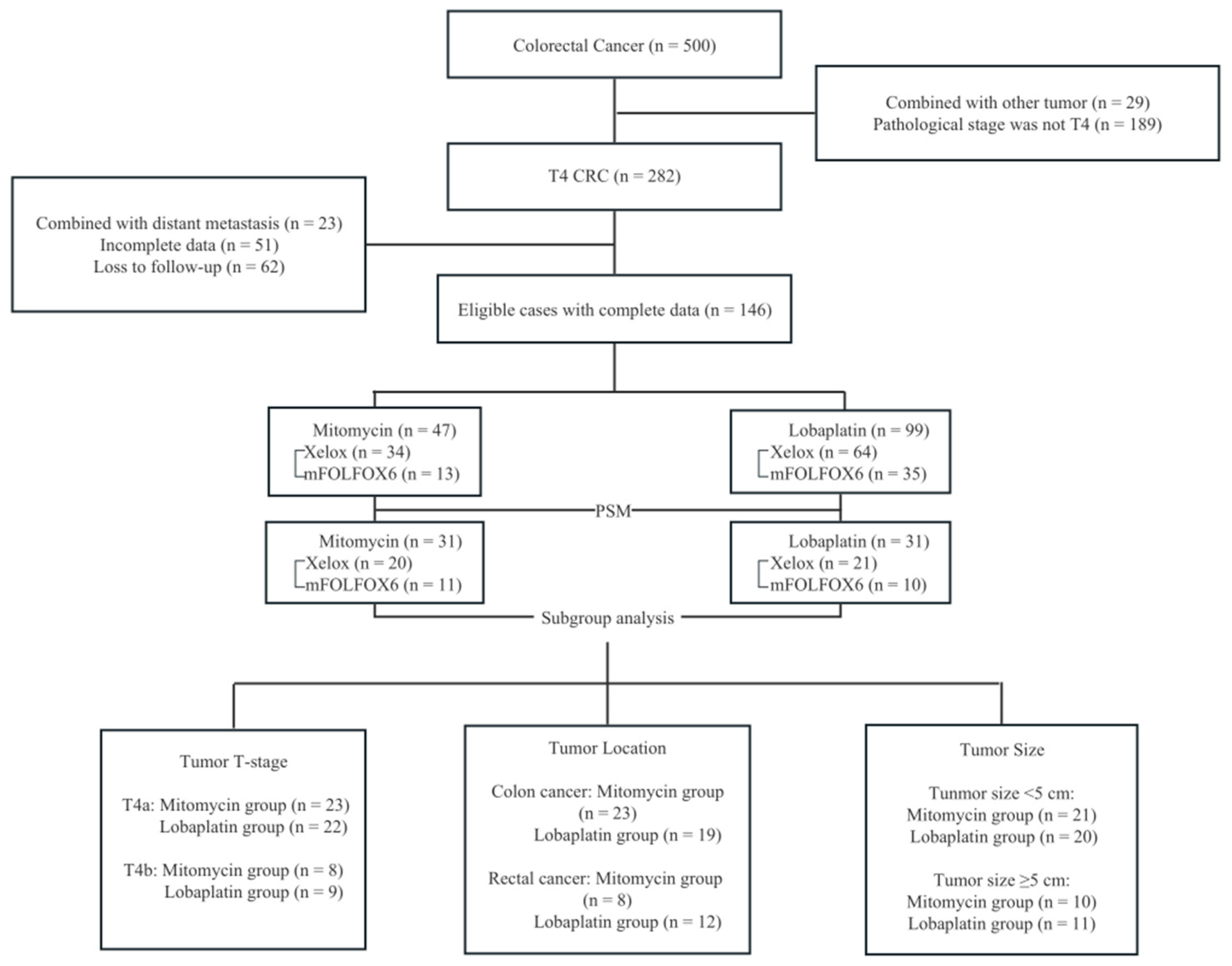
2.1. Study Cohort
2.2. Data Collection
2.3. Follow-Up
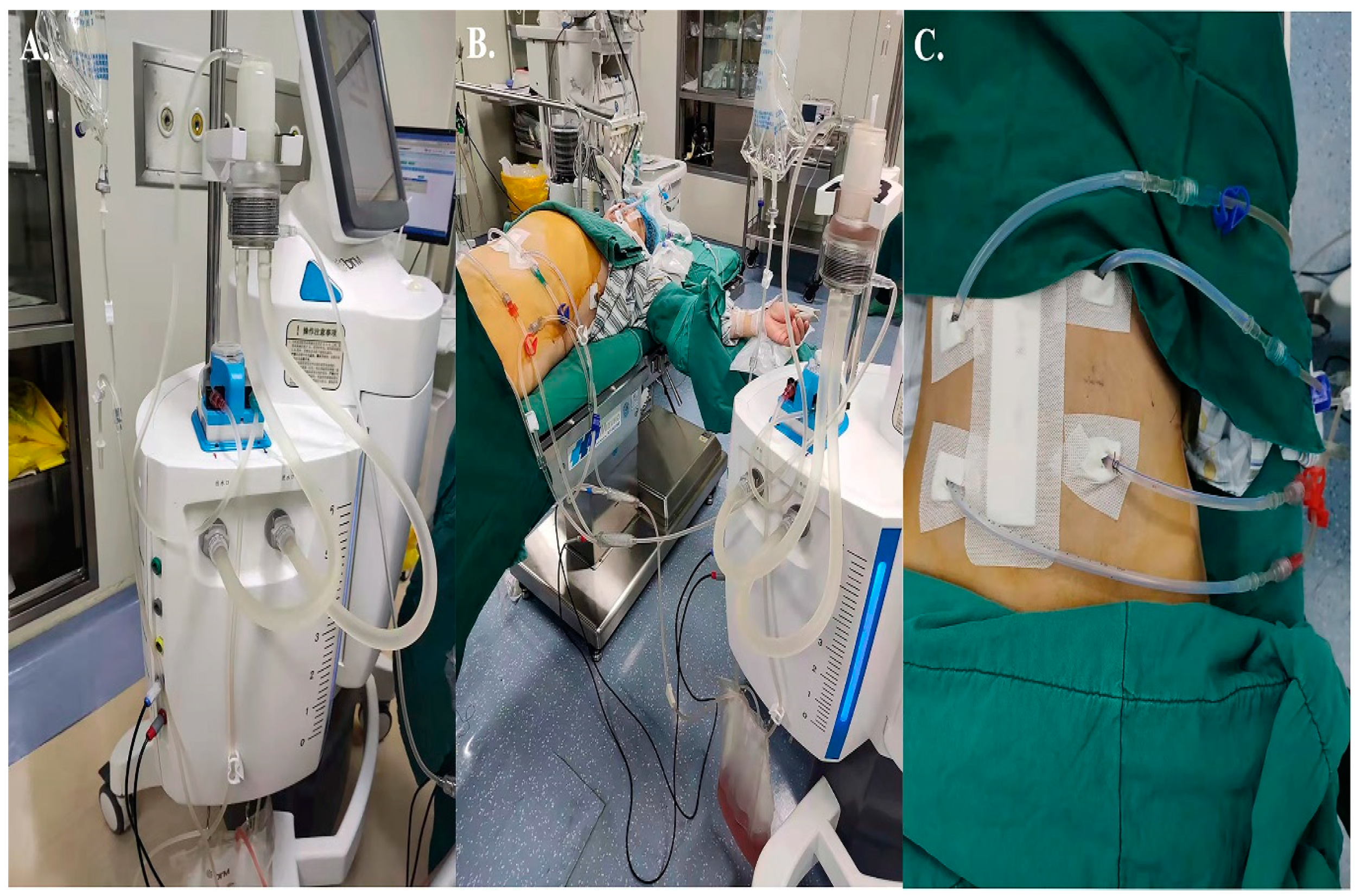
2.4. Treatment
2.5. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. Adverse Events
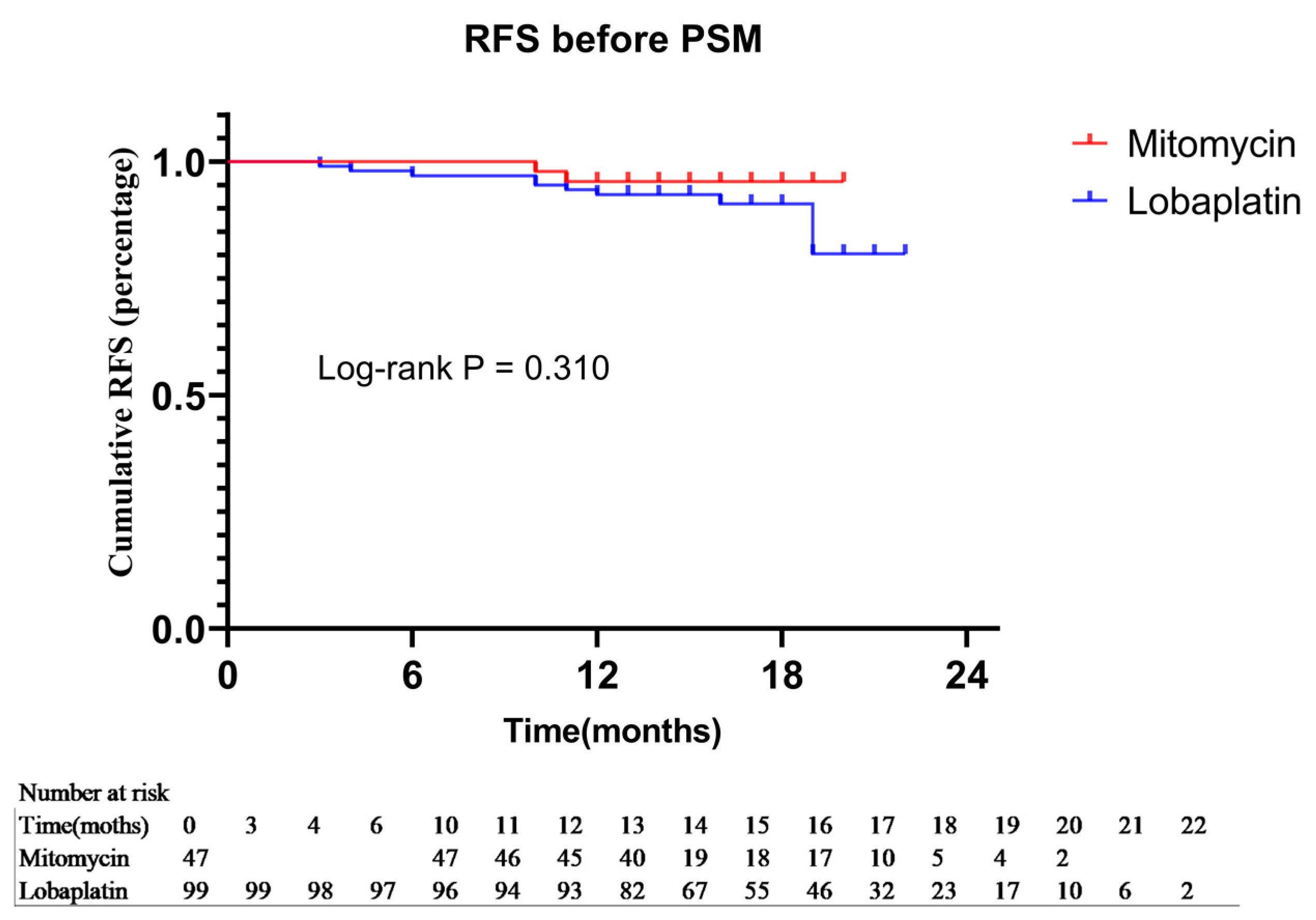
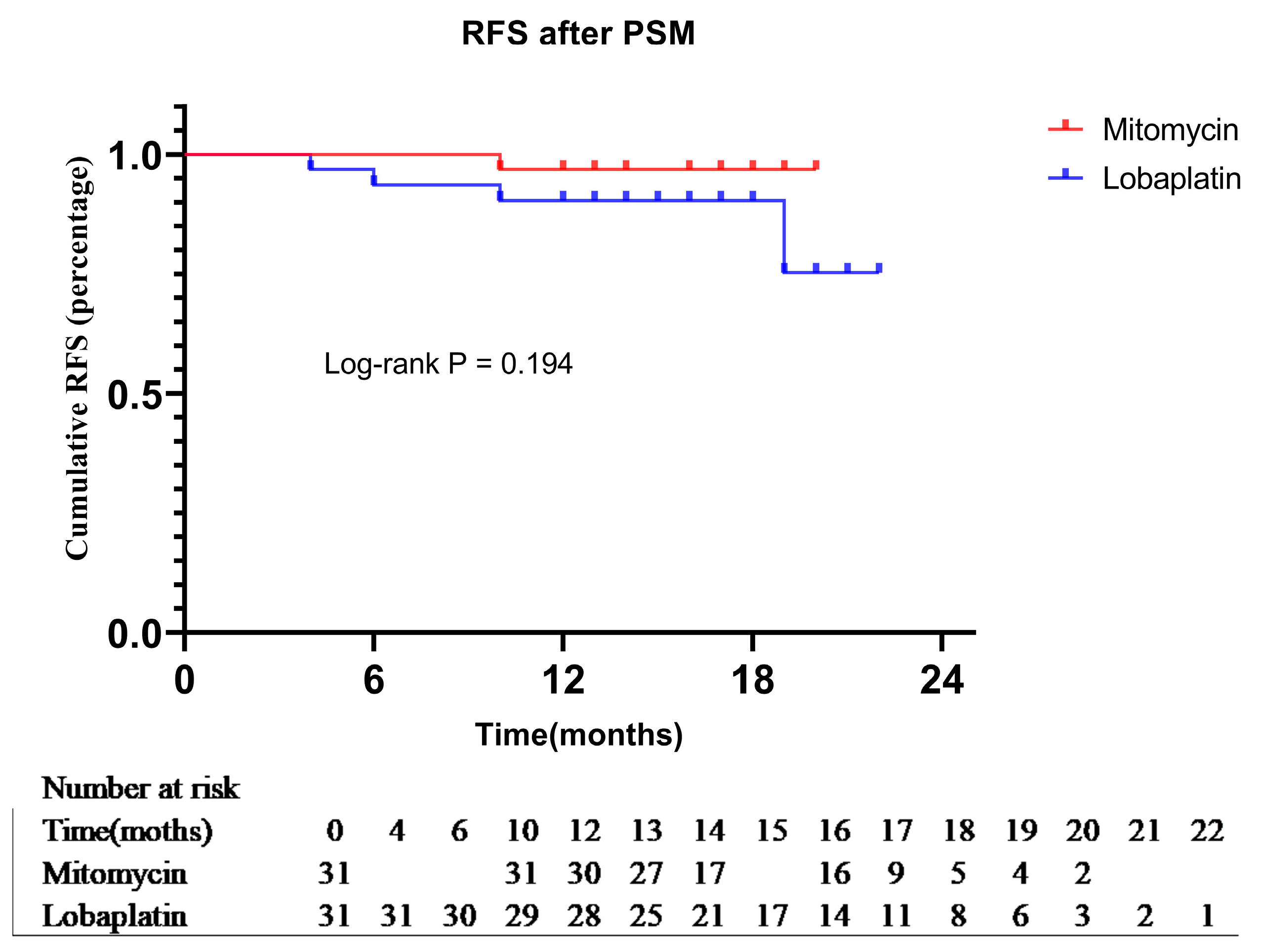
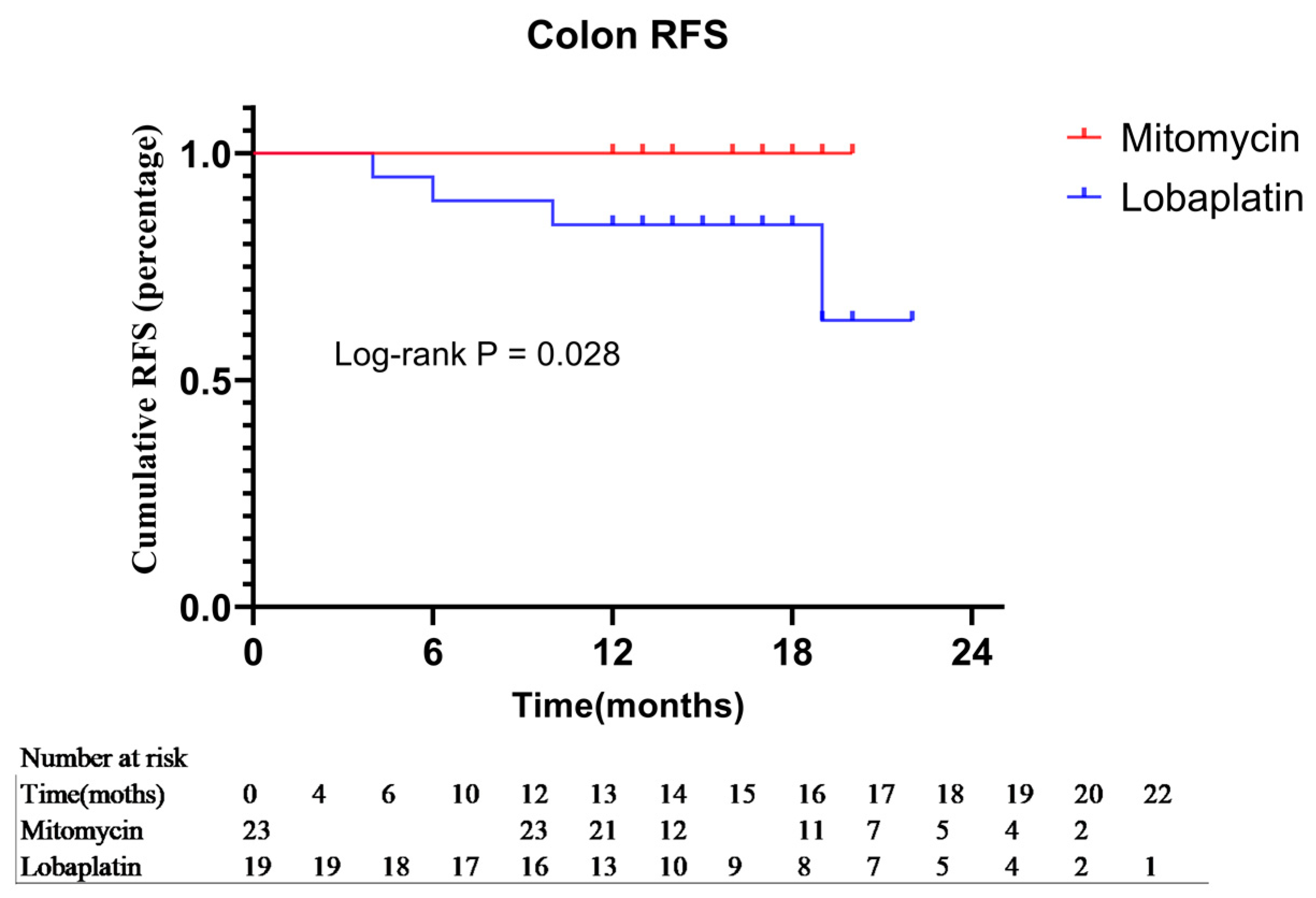
3.3. Comparison of Short-Term Prognosis
3.4. Stratified Analysis of Prognosis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hospital Authority of National Health Commission of the People’s Repuhlic of China; Chinese Society of Oncology CMA. Chinese protocol of diagnosis and treatment of colorectal cancer (2020 edition). Chin. J. Pract. Surg. 2020, 6, 601–625. [Google Scholar]
- Kerscher, A.G.; Chua, T.C.; Gasser, M.; Maeder, U.; Kunzmann, V.; Isbert, C.; Germer, C.T.; Pelz, J.O.W. Impact of peritoneal carcinomatosis in the disease history of colorectal cancer management: A longitudinal experience of 2406 patients over two decades. Br. J. Cancer 2013, 108, 1432–1439. [Google Scholar] [CrossRef] [PubMed]
- Klaver, C.E.L.; Musters, G.D.; Bemelman, W.A.; Punt, C.J.A.; Verwaal, V.J.; Dijkgraaf, M.G.W.; Aalbers, A.G.J.; van der Bilt, J.D.W.; Boerma, D.; Bremers, A.J.A.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy (HIPEC) in patients with colon cancer at high risk of peritoneal carcinomatosis; the COLOPEC randomized multicentre trial. BMC Cancer 2015, 15, 428. [Google Scholar] [CrossRef]
- Baratti, D.; Kusamura, S.; Iusco, D.; Gimondi, S.; Pietrantonio, F.; Milione, M.; Guaglio, M.; Bonomi, S.; Grassi, A.; Virzì, S.; et al. Hyperthermic Intraperitoneal Chemotherapy (HIPEC) at the Time of Primary Curative Surgery in Patients with Colorectal Cancer at High Risk for Metachronous Peritoneal Metastases. Ann. Surg. Oncol. 2016, 24, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Narasimhan, V.; Britto, M.; Pham, T.; Warrier, S.; Naik, A.; Lynch, A.C.; Michael, M.; Tie, J.; Ramsay, R.; Heriot, A. Evolution of Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Colorectal Peritoneal Metastases: 8-Year Single-Institutional Experience. Dis. Colon Rectum 2019, 62, 1195–1203. [Google Scholar] [CrossRef] [PubMed]
- Lei, Z.; Guan, T.; Luo, J.; Tang, H.; Shuzhong, C. Rationality of performing hyperthermic intraperitoneal chemotherapy 5–8 weeks after primary tumor resection for patients with locally advanced colorectal cancer—Based on COLOPEC. Chin. J. Gastrointest. Surg. 2019, 22, 1115–1117. [Google Scholar]
- Birgisson, H.; Enblad, M.; Artursson, S.; Ghanipour, L.; Cashin, P.; Graf, W. Patients with colorectal peritoneal metastases and high peritoneal cancer index may benefit from cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Eur. J. Surg. Oncol. 2020, 46, 2283–2291. [Google Scholar] [CrossRef]
- Yonemura, Y.; Canbay, E.; Ishibashi, H. Prognostic Factors of Peritoneal Metastases from Colorectal Cancer following Cytoreductive Surgery and Perioperative Chemotherapy. Sci. World J. 2013, 2013, 7. [Google Scholar] [CrossRef]
- Chen, C.; Wang, J.; Zhao, Y.; Ge, X.; Wang, Z.; Yu, S.; Song, Y.; Ding, K.; Zhang, S.; Zheng, S.; et al. Factors Prognostic for Peritoneal Metastases from Colorectal Cancer Treated with Surgery. Cancer Manag. Res. 2020, 12, 10587–10602. [Google Scholar] [CrossRef]
- Segelman, J.; Granath, F.; Holm, T.; Machado, M.; Mahteme, H.; Martling, A. Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer. Br. J. Surg. 2012, 99, 699–705. [Google Scholar] [CrossRef]
- van Gestel, Y.R.B.M.; TThomassen, I.; Lemmens, V.E.P.P.; Pruijt, J.F.M.; van Herk-Sukel, M.P.P.; Rutten, H.J.T.; Creemers, G.-J.; de Hingh, I.H.J.T. Metachronous peritoneal carcinomatosis after curative treatment of colorectal cancer. Eur. J. Surg. Oncol. 2014, 40, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Klaver, C.E.L.; van Huijgevoort, N.C.M.; de Buck van Overstraeten, A.; Wolthuis, A.M.; Tanis, P.J.; van der Bilt, J.D.W.; Sagaert, X.; D’Hoore, A. Locally Advanced Colorectal Cancer: True Peritoneal Tumor Penetration is Associated with Peritoneal Metastases. Ann. Surg. Oncol. 2017, 25, 212–220. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. Colon Cancer Survival Rates With the New American Joint Committee on Cancer Sixth Edition Staging. JNCI J. Natl. Cancer Inst. 2004, 96, 1420–1425. [Google Scholar] [CrossRef] [PubMed]
- Hompes, D.; Tiek, J.; Wolthuis, A.; Fieuws, S.; Penninckx, F.; Van Cutsem, E.; D’Hoore, A. HIPEC in T4a colon cancer: A defendable treatment to improve oncologic outcome? Ann. Oncol. 2012, 23, 3123–3129. [Google Scholar] [CrossRef]
- Auer, R.C.; Sivajohanathan, D.; Biagi, J.; Conner, J.; Kennedy, E.; May, T. Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: A systematic review. Eur. J. Cancer 2020, 127, 76–95. [Google Scholar] [CrossRef]
- Verwaal, V.J.; van Ruth, S.; de Bree, E.; van Slooten, G.W.; van Tinteren, H.; Boot, H.; Zoetmulder, F.A.N. Randomized Trial of Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy Versus Systemic Chemotherapy and Palliative Surgery in Patients With Peritoneal Carcinomatosis of Colorectal Cancer. J. Clin. Oncol. 2003, 21, 3737–3743. [Google Scholar] [CrossRef]
- Klaver, C.E.L.; Wisselink, D.D.; Punt, C.J.A.; Snaebjornsson, P.; Crezee, J.; Aalbers, A.G.J.; Brandt, A.; Bremers, A.J.A.; Burger, J.W.A.; Fabry, H.F.J.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy in patients with locally advanced colon cancer (COLOPEC): A multicentre, open-label, randomised trial. Lancet Gastroenterol. Hepatol. 2019, 4, 761–770. [Google Scholar] [CrossRef]
- Turaga, K.; Levine, E.; Barone, R.; Sticca, R.; Petrelli, N.; Lambert, L.; Nash, G.; Morse, M.; Adbel-Misih, R.; Alexander, H.R.; et al. Consensus Guidelines from The American Society of Peritoneal Surface Malignancies on Standardizing the Delivery of Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Colorectal Cancer Patients in the United States. Ann. Surg. Oncol. 2013, 21, 1501–1505. [Google Scholar] [CrossRef]
- Peritoneal Surface Oncology Committee of China Anti-Cancer Association. Chinese Expert Cnsensus on the Clinical Application of China Hyperthermic Intraperitoneal Chemotherapy. Natl. Med. J. China 2020, 100, 89–96. [Google Scholar]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.-J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN Guidelines Insights: Colon Cancer, Version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef]
- Arjona-Sanchez, A.; Cano-Osuna, M.T.; Gutierrez, A.; Segura, J.J.; Perez, V.C.E.; Sanchez, S.; Garcia, A.; Prieto, I.; Barrios Sanchez, P.; Torres, J.; et al. Adjuvant hyperthermic intraperitoneal chemotherapy in locally advanced colon cancer (HIPECT4): A randomized phase III study. Ann. Oncol. 2022, 33, S680. [Google Scholar] [CrossRef]
- Goere, D.; Glehen, O.; Quenet, F.; Ducreux, M.; Guilloit, J.M.; Texier, M.; Benhamou, E.; Elias, D. Results of a randomized phase 3 study evaluating the potential benefit of a secondlook surgery plus HIPEC in patients at high risk of developing colorectal peritoneal metastases (PROPHYLOCHIP-NTC01226394). J. Clin. Oncol. Conf. 2018, 36 (Suppl. 31), 3531. [Google Scholar] [CrossRef]
- Wisselink, D.D.; Braakhuis, L.L.F.; Gallo, G.; van Grevenstein, W.M.U.; van Dieren, S.; Kok, N.F.M.; de Reuver, P.R.; Tanis, P.J.; de Hingh, I.H.J.T. Systematic review of published literature on oxaliplatin and mitomycin C as chemotherapeutic agents for hyperthermic intraperitoneal chemotherapy in patients with peritoneal metastases from colorectal cancer. Crit. Rev. Oncol. Hematol. 2019, 142, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Torphy, R.J.; Stewart, C.; Sharma, P.; Halpern, A.L.; Oase, K.; Herter, W.; Bartsch, C.; Friedman, C.; Del Chiaro, M.; Schulick, R.D.; et al. Dextrose-Containing Carrier Solution for Hyperthermic Intraperitoneal Chemotherapy: Increased Intraoperative Hyperglycemia and Postoperative Complications. Ann. Surg. Oncol. 2020, 27, 4874–4882. [Google Scholar] [CrossRef]
- Zhou, H.T.; Jiang, J.; Guan, X.; Su, H.; Liang, J.-W.; Pei, W.; Wang, Z.; Liu, Z.; Jiang, Z.; Liu, Q.; et al. The short-term effect analysis of intraoperative intraperitoneal perfusion chemotherapy with Lobaplatin for colorectal cancer. Chin. J. Color. Dis. Electron. Ed. 2018, 7, 125–129. [Google Scholar]
- Wu, H.T.; Yang, X.J.; Huang, C.Q.; Sun, J.-H.; Ji, Z.-H.; Peng, K.-W.; Zhang, Q.; Li, Y. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy with lobaplatin and docetaxel improves survival for patients with peritoneal carcinomatosis from abdominal and pelvic malignancies. World J. Surg. Oncol. 2016, 14, 246. [Google Scholar] [CrossRef]
- Pei, W.; Zhou, S.; Zhang, J.; Zhou, H.; Chen, H.; Bi, J.; Zheng, Z.; Liu, Z.; Jiang, Z.; Wang, Z.; et al. Lobaplatin-Based Hyperthermic Intraperitoneal Chemotherapy for Patients with Peritoneal Metastasis from Appendiceal and Colorectal Cancer: Safety and Efficacy. Cancer Manag. Res. 2020, 12, 12099–12110. [Google Scholar] [CrossRef]
- Goéré, D.; Glehen, O.; Quenet, F.; Guilloit, J.-M.; Bereder, J.-M.; Lorimier, G.; Thibaudeau, E.; Ghouti, L.; Pinto, A.; Tuech, J.-J.; et al. Second-look surgery plus hyperthermic intraperitoneal chemotherapy versus surveillance in patients at high risk of developing colorectal peritoneal metastases (PROPHYLOCHIP–PRODIGE 15): A randomised, phase 3 study. Lancet Oncol. 2020, 21, 1147–1154. [Google Scholar] [CrossRef]
- Ravn, S.; Heide-Jørgensen, U.; Christiansen, C.F.; Verwaal, V.J.; Hagemann-Madsen, R.H.; Iversen, L.H. Overall risk and risk factors for metachronous peritoneal metastasis after colorectal cancer surgery: A nationwide cohort study. BJS Open 2020, 4, 284–292. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | No (%) | χ2/Z | p Value | ||
|---|---|---|---|---|---|
| Overall (n = 146) | Mitomycin (n = 47) | Lobaplatin (n = 99) | |||
| Age, years | |||||
| Mean ± SD | 57.79 ± 11.092 | 55.06 ± 9.841 | 59.08 ± 11.460 | −2.067 | 0.040 |
| ≤60 | 81 (55.5) | 30 (63.8) | 51 (51.5) | ||
| >60 | 65 (0.445) | 17 (36.2) | 48 (48.5) | ||
| Sex | 1.706 | 0.191 | |||
| Female | 61 (41.8) | 16 (34.0) | 45 (45.5) | ||
| Male | 85 (58.2) | 31 (66.0) | 54 (54.5) | ||
| BMI | |||||
| Mean ± SD | 23.50 ± 3.690 | 23.68 ± 4.296 | 23.42 ± 3.386 | 0.402 | 0.689 |
| Charlson Comorbidity Index | 0.282 | 0.963 | |||
| 0 | 108 (74.0) | 34 (72.3) | 74 (74.7) | ||
| 1 | 28 (19.2) | 10 (21.3) | 18 (18.2) | ||
| 2 | 6 (4.1) | 2 (4.3) | 4 (4.0) | ||
| ≥3 | 4 (2.7) | 1 (2.1) | 3 (3.0) | ||
| ASA Score | 6.974 | 0.031 | |||
| 1 | 31 (21.2) | 15 (31.9) | 16 (16.2) | ||
| 2 | 109 (74.7) | 32 (68.1) | 77 (77.8) | ||
| ≥3 | 6 (4.1) | 0 (0.0) | 6 (6.1) | ||
| Surgical Procedures | 0.002 | 0.966 | |||
| laparoscopy | 143 (97.9) | 46 (97.9) | 97 (98.0) | ||
| laparotomy | 3 (2.1) | 1 (2.1) | 2 (2.0) | ||
| Tumor Location | 6.372 | 0.041 | |||
| right semicolon | 43 (29.5) | 14 (29.8) | 29 (29.3) | ||
| left semicolon | 50 (34.2) | 22 (46.8) | 28 (28.3) | ||
| rectum | 53 (36.3) | 11 (23.4) | 42 (42.4) | ||
| Tumor Size, cm | |||||
| Mean ± SD | 4.848 ± 2.320 | 4.681 ± 1.944 | 4.927 ± 2.484 | −0.598 | 0.551 |
| ≤5 | 104 (71.2) | 38 (80.9) | 66 (66.7) | ||
| >5 | 42 (28.8) | 9 (19.1) | 33 (33.3) | ||
| Tumor differentiation | 1.900 | 0.168 | |||
| poor or undifferentiation | 12 (8.2) | 6 (12.8) | 6 (6.1) | ||
| Well or moderately | 134 (91.8) | 41 (87.2) | 93 (93.9) | ||
| pT status | 0.067 | 0.796 | |||
| pT4a | 91 (62.3) | 30 (63.8) | 61 (61.6) | ||
| pT4b | 55 (37.7) | 17 (36.2) | 38 (38.4) | ||
| No. of resected lymph nodes | 2.018 | 0.045 | |||
| Mean ± SD | 21.39 ± 7.599 | 23.21 ± 8.382 | 20.53 ± 7.079 | ||
| pN status | 8.920 | 0.063 | |||
| pN0 | 83 (56.8) | 29 (61.7) | 54 (54.5) | ||
| pN1a | 21 (14.4) | 11 (23.4) | 10 (10.1) | ||
| pN1b | 25 (17.1) | 4 (8.5) | 21 (21.2) | ||
| pN2a | 7 (4.8) | 1 (2.1) | 6 (6.1) | ||
| pN2b | 10 (6.8) | 2 (4.3) | 8 (8.1) | ||
| nerve invasion | 0.934 | 0.334 | |||
| No | 86 (58.9) | 25 (53.2) | 61 (61.6) | ||
| Yes | 60 (41.1) | 22 (46.8) | 38 (38.4) | ||
| vascular invasion | 0.126 | 0.723 | |||
| No | 90 (61.6) | 28 (59.6) | 62 (62.6) | ||
| Yes | 56 (38.4) | 19 (40.4) | 37 (37.4) | ||
| MMR positive | 0.109 | 0.741 | |||
| No | 138 (94.5) | 44 (93.6) | 94 (94.9) | ||
| Yes | 8 (5.5) | 3 (6.4) | 5 (5.1) | ||
| Adjuvant chemotherapy | 0.855 | 0.355 | |||
| XELOX | 98 (67.1) | 34 (72.3) | 64 (64.6) | ||
| mFOLFOX6 | 48 (32.9) | 13 (27.7) | 35 (35.3) | ||
| Follow-up time, months | −2.439 | 0.016 | |||
| Mean ± SD | 15.36 ± 2.713 | 14.57± 2.320 | 15.73± 2.817 | ||
| Median(range) | 15(12–22) | 13(12–20) | 15(12–22) | ||
| Characteristic | No (%) | χ2/Z | p Value | ||
|---|---|---|---|---|---|
| Overall (n = 62) | Mitomycin (n = 31) | Lobaplatin (n = 31) | |||
| Age, years | |||||
| Mean ± SD | 59.02 ± 11.810 | 56.29 ± 8.844 | 57.90 ± 11.825 | −0.608 | 0.545 |
| ≤60 | 36 (58.1) | 19 (61.3) | 17 (54.8) | ||
| >60 | 26 (41.9) | 12 (38.7) | 14 (45.2) | ||
| Sex | 0.076 | 0.783 | |||
| Female | 19 (30.6) | 9 (29.0) | 10 (32.3) | ||
| Male | 43 (69.4) | 22 (71.0) | 21 (67.7) | ||
| BMI | |||||
| Mean ± SD | 22.840 ± 3.369 | 23.899 ± 4.830 | 23.950 ± 3.561 | −0.047 | 0.962 |
| Charlson Comorbidity Index | 0.828 | 0.843 | |||
| 0 | 43 (69.4) | 20 (64.5) | 23 (74.2) | ||
| 1 | 14 (22.6) | 8 (25.8) | 6 (19.4) | ||
| 2 | 3 (4.8) | 2 (6.5) | 1 (3.2) | ||
| ≥3 | 2 (3.2) | 1 (3.2) | 1 (3.2) | ||
| ASA Score | 1.160 | 0.560 | |||
| 1 | 13 (21.0) | 6 (19.4) | 7 (22.6) | ||
| 2 | 48 (77.4) | 25 (80.6) | 23 (74.2) | ||
| 3 | 1 (1.6) | 0 (0.0) | 1 (3.2) | ||
| Surgical Procedures | <0.001 | 1.000 | |||
| laparoscopy | 60 (96.8) | 30 (96.8) | 30 (96.8) | ||
| laparotomy | 2 (3.2) | 1 (3.2) | 1 (3.2) | ||
| Tumor Location | 1.182 | 0.554 | |||
| right semicolon | 20 (32.3) | 11 (35.5) | 9 (29.0) | ||
| left semicolon | 22 (35.5) | 12 (38.7) | 10 (32.3) | ||
| rectum | 20 (32.3) | 8 (25.8) | 12 (38.7) | ||
| Tumor Size, cm | |||||
| Mean ± SD | 4.73 ± 2.127 | 4.58 ± 1.852 | 4.84 ± 3.081 | −0.405 | 0.687 |
| ≤5 | 47 (75.8) | 25 (80.6) | 22 (71.0) | ||
| >5 | 15 (24.2) | 6 (19.4) | 9 (29.0) | ||
| Tumor differentiation | 2.296 | 0.130 | |||
| poor or undifferentiation | 8 (12.9) | 2 (6.5) | 6 (19.4) | ||
| Well or moderately | 54 (87.1) | 29 (93.5) | 25 (80.6) | ||
| pT status | 0.081 | 0.776 | |||
| pT4a | 45 (72.6) | 23 (74.2) | 22 (71.0) | ||
| pT4b | 17 (27.4) | 8 (25.8) | 9 (29.0) | ||
| No. of resected lymph nodes | 1.557 | 0.125 | |||
| Mean ± SD | 21.15 ± 9.416 | 23.06 ± 8.342 | 20.23 ± 5.783 | ||
| pN status | 2.816 | 0.589 | |||
| pN0 | 40 (64.5) | 22 (71.0) | 18 (58.1) | ||
| pN1a | 7 (11.3) | 4 (12.9) | 3 (9.7) | ||
| pN1b | 11 (17.7) | 3 (9.7) | 8 (25.8) | ||
| pN2a | 2 (3.2) | 1 (3.2) | 1 (3.2) | ||
| pN2b | 2 (3.2) | 1 (3.2) | 1 (3.2) | ||
| nerve invasion | 0.265 | 0.607 | |||
| No | 36 (58.1) | 17 (54.8) | 19 (61.3) | ||
| Yes | 26 (41.9) | 14 (45.2) | 12 (38.7) | ||
| vascular invasion | <0.001 | 1.000 | |||
| No | 40 (64.5) | 20 (64.5) | 20 (64.5) | ||
| Yes | 22 (35.5) | 11 (35.5) | 11 (35.5) | ||
| MMR positive | 0.218 | 0.641 | |||
| No | 57 (91.9) | 28 (90.3) | 29(93.5) | ||
| Yes | 5 (8.1) | 3 (9.7) | 2 (6.5) | ||
| Adjuvant chemotherapy | 0.072 | 0.788 | |||
| XELOX | 41 (66.1) | 20 (64.5) | 21 (67.7) | ||
| mFOLFOX6 | 21 (33.9) | 11 (35.5) | 10 (32.3) | ||
| Follow-up time, months | −0.943 | 0.349 | |||
| Mean ±SD | 18.95 ± 3.857 | 15.1 3± 2.487 | 15.77 ± 2.883 | ||
| Median(range) | 15.5 (12–22) | 16 (12–20) | 15 (12–22) | ||
| Adverse Event | Before PSM | After PSM | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| No (%) | χ2 | p Value | No (%) | χ2 | p Value | |||||
| Overall (n = 146) | Mitomycin (n = 47) | Lobaplatin (n = 99) | Overall (n = 62) | Mitomycin (n = 31) | Lobaplatin (n = 31) | |||||
| Anemia | 25 (17.1) | 6 (12.8) | 19 (19.2) | 0.927 | 0.336 | 13 (21.0) | 5 (16.1) | 8 (25.8) | 0.876 | 0.349 |
| Hypoalbuminemia | 36 (24.7) | 11 (23.4) | 25 (25.3) | 0.059 | 0.809 | 17 (27.4) | 6 (19.4) | 11 (35.5) | 2.026 | 0.155 |
| Myelosuppression | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.000 | 1.000 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.000 | 1.000 |
| Wound complications | 6 (4.1) | 0 (0.0) | 6 (6.1) | 2.971 | 0.082 | 1 (1.6) | 0 (0.0) | 1 (3.2) | 1.016 | 0.313 |
| Abdomen infection | 1 (0.7) | 1 (2.1) | 0 (0.0) | 2.121 | 0.145 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.000 | 1.000 |
| Pulmonary infection | 4 (2.7) | 1 (2.1) | 3 (3.0) | 0.097 | 0.755 | 2 (3.2) | 1 (3.2) | 1 (3.2) | 0.000 | 1.000 |
| Postoperative bleeding | 2 (1.4) | 1 (2.1) | 1 (1.0) | 0.295 | 0.587 | 2 (3.2) | 1 (3.2) | 1 (3.2) | 0.000 | 1.000 |
| Anastomotic leakage | 2 (1.4) | 0 (0.0) | 2 (2.0) | 0.963 | 0.327 | 1 (1.6) | 0 (0.0) | 1 (3.2) | 1.016 | 0.313 |
| Ileus | 1 (0.7) | 1 (2.1) | 0 (0.0) | 2.121 | 0.145 | 1 (1.6) | 1 (3.2) | 0 (0.0) | 1.016 | 0.313 |
| Liver dysfunction | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.000 | 1.000 | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0.000 | 1.000 |
| Electrolyte disturbance | 4 (2.7) | 2 (4.3) | 2 (2.0) | 0.598 | 0.440 | 2 (3.2) | 1 (3.2) | 1 (3.2) | 0.000 | 1.000 |
| Digestive symptoms | 4 (2.7) | 0 (0.0) | 4 (4.0) | 1.952 | 0.162 | 1 (1.6) | 0 (0.0) | 1 (3.2) | 1.016 | 0.313 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, X.; Lin, Y.; Shen, C.; Li, Y.; Xiang, F.; Ruan, T.; Zeng, X.; Lv, J.; Tao, K.; Wu, C. Comparative Study of Short-Term Efficacy and Safety of Mitomycin versus Lobaplatin for Hyperthermic Intraperitoneal Chemotherapy after Radical Surgery in Colorectal Cancer with High-Risk Factors for Peritoneal Carcinomatosis: A Propensity Score Matching Analysis. Curr. Oncol. 2023, 30, 1488-1501. https://doi.org/10.3390/curroncol30020114
Guo X, Lin Y, Shen C, Li Y, Xiang F, Ruan T, Zeng X, Lv J, Tao K, Wu C. Comparative Study of Short-Term Efficacy and Safety of Mitomycin versus Lobaplatin for Hyperthermic Intraperitoneal Chemotherapy after Radical Surgery in Colorectal Cancer with High-Risk Factors for Peritoneal Carcinomatosis: A Propensity Score Matching Analysis. Current Oncology. 2023; 30(2):1488-1501. https://doi.org/10.3390/curroncol30020114
Chicago/Turabian StyleGuo, Xikai, Yao Lin, Chu Shen, Yuan Li, Fan Xiang, Tuo Ruan, Xinyu Zeng, Jianbo Lv, Kaixiong Tao, and Chuanqing Wu. 2023. "Comparative Study of Short-Term Efficacy and Safety of Mitomycin versus Lobaplatin for Hyperthermic Intraperitoneal Chemotherapy after Radical Surgery in Colorectal Cancer with High-Risk Factors for Peritoneal Carcinomatosis: A Propensity Score Matching Analysis" Current Oncology 30, no. 2: 1488-1501. https://doi.org/10.3390/curroncol30020114
APA StyleGuo, X., Lin, Y., Shen, C., Li, Y., Xiang, F., Ruan, T., Zeng, X., Lv, J., Tao, K., & Wu, C. (2023). Comparative Study of Short-Term Efficacy and Safety of Mitomycin versus Lobaplatin for Hyperthermic Intraperitoneal Chemotherapy after Radical Surgery in Colorectal Cancer with High-Risk Factors for Peritoneal Carcinomatosis: A Propensity Score Matching Analysis. Current Oncology, 30(2), 1488-1501. https://doi.org/10.3390/curroncol30020114