Impact of a Multidisciplinary Head and Neck Tumor Board on Treatment and Survival in Laryngeal Carcinoma


Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Analysis of Epidemiological Data
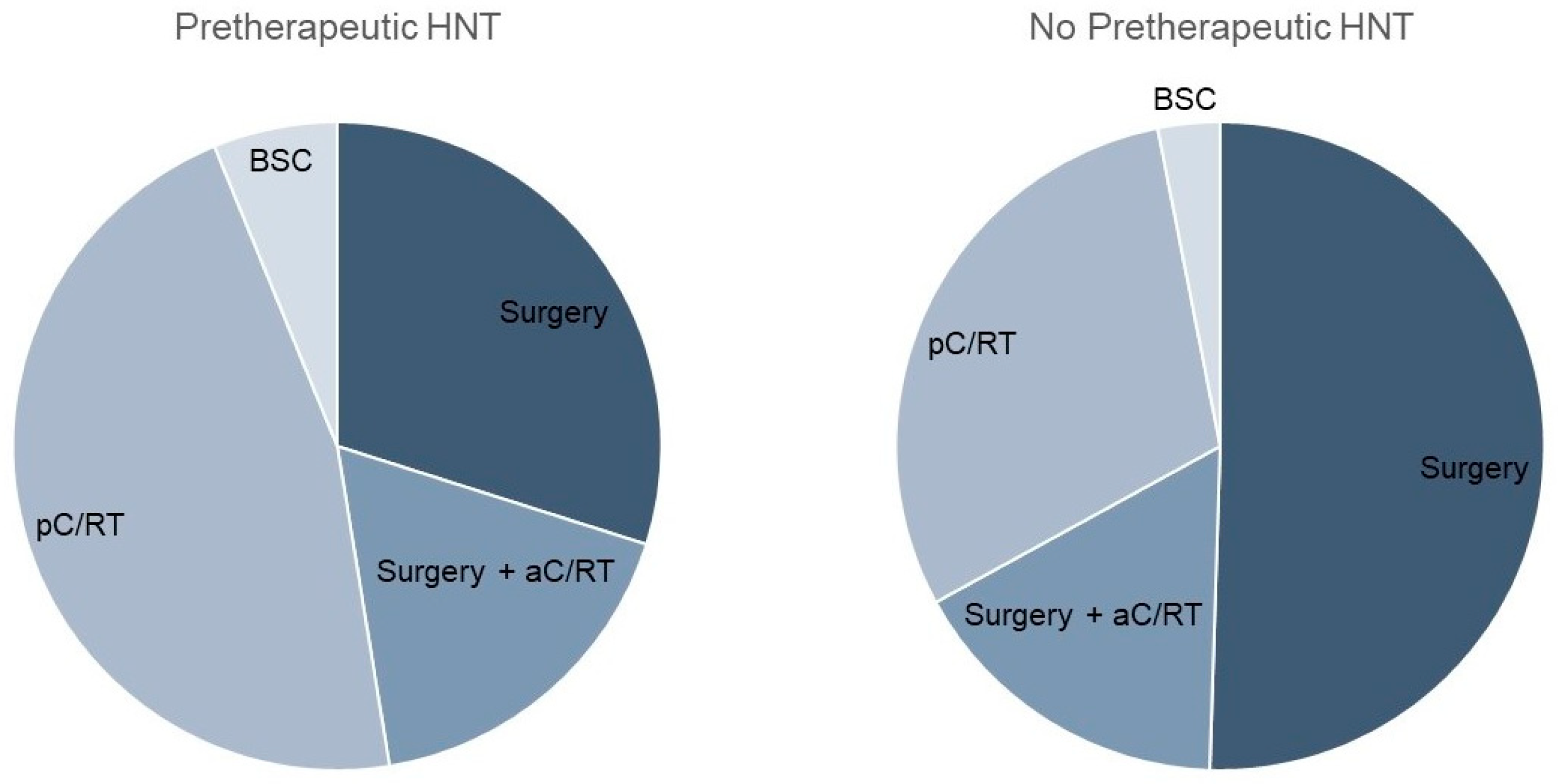
3.2. Treatment Regimen
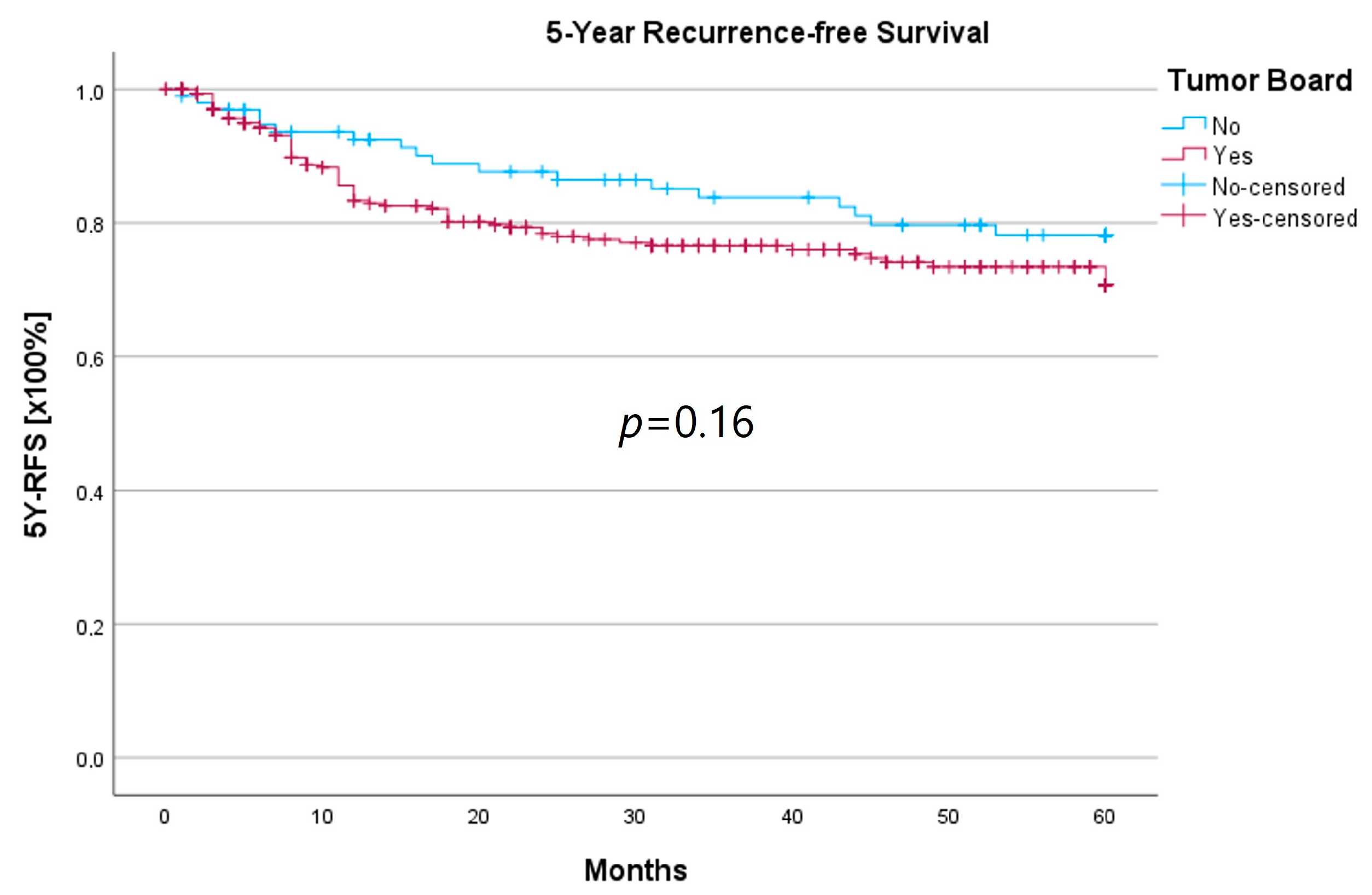
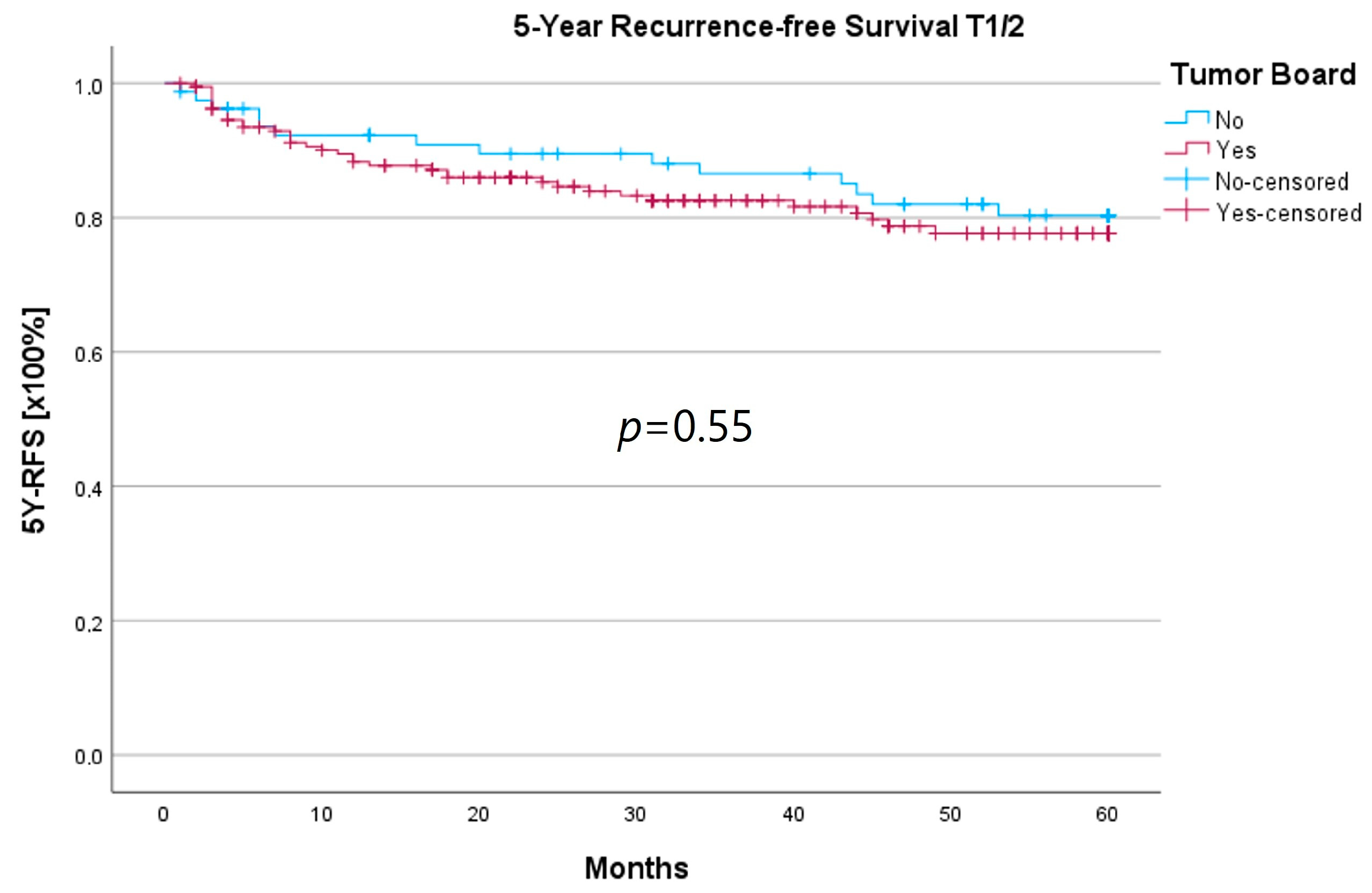
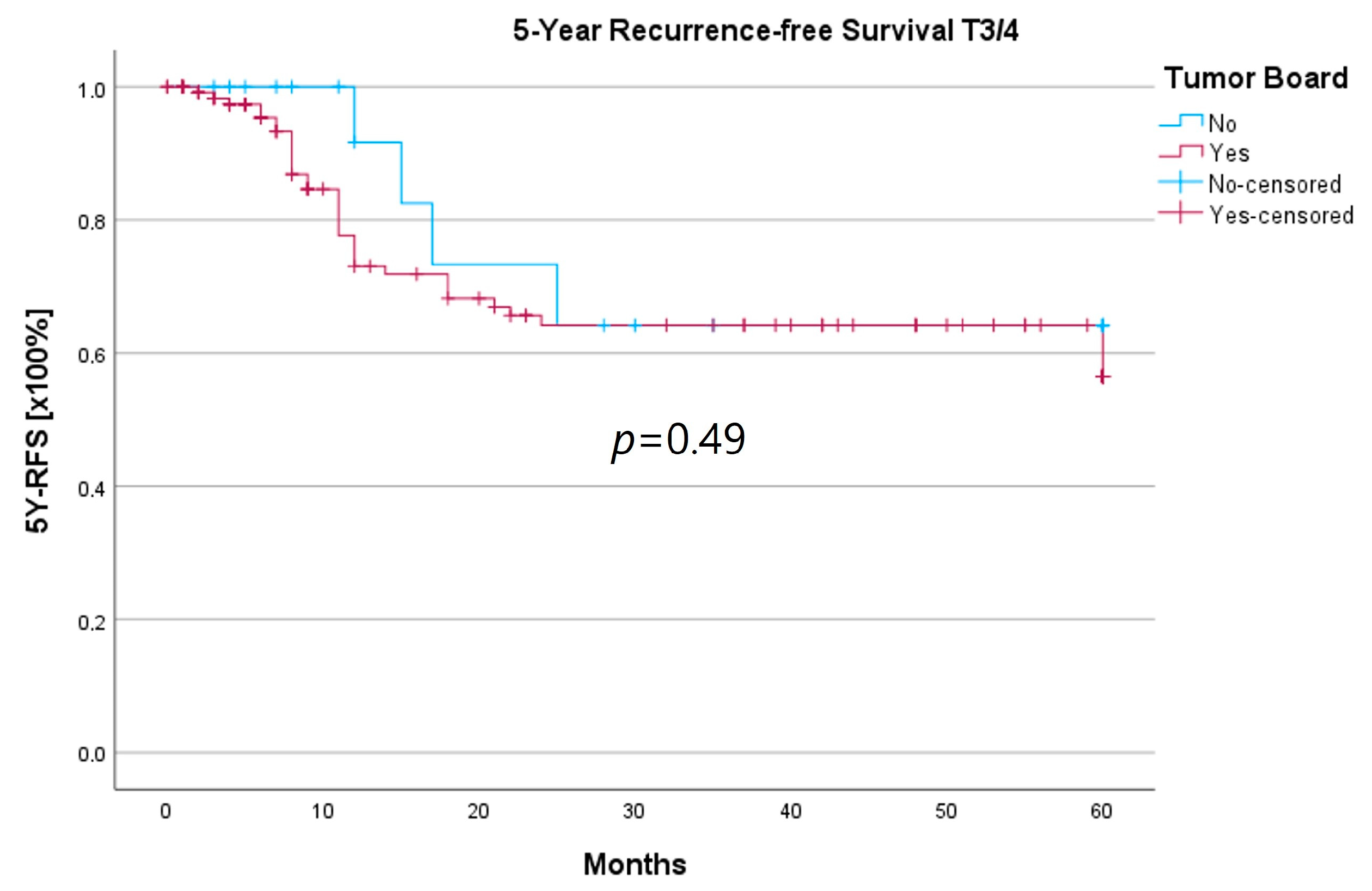
3.3. Survival Analysis
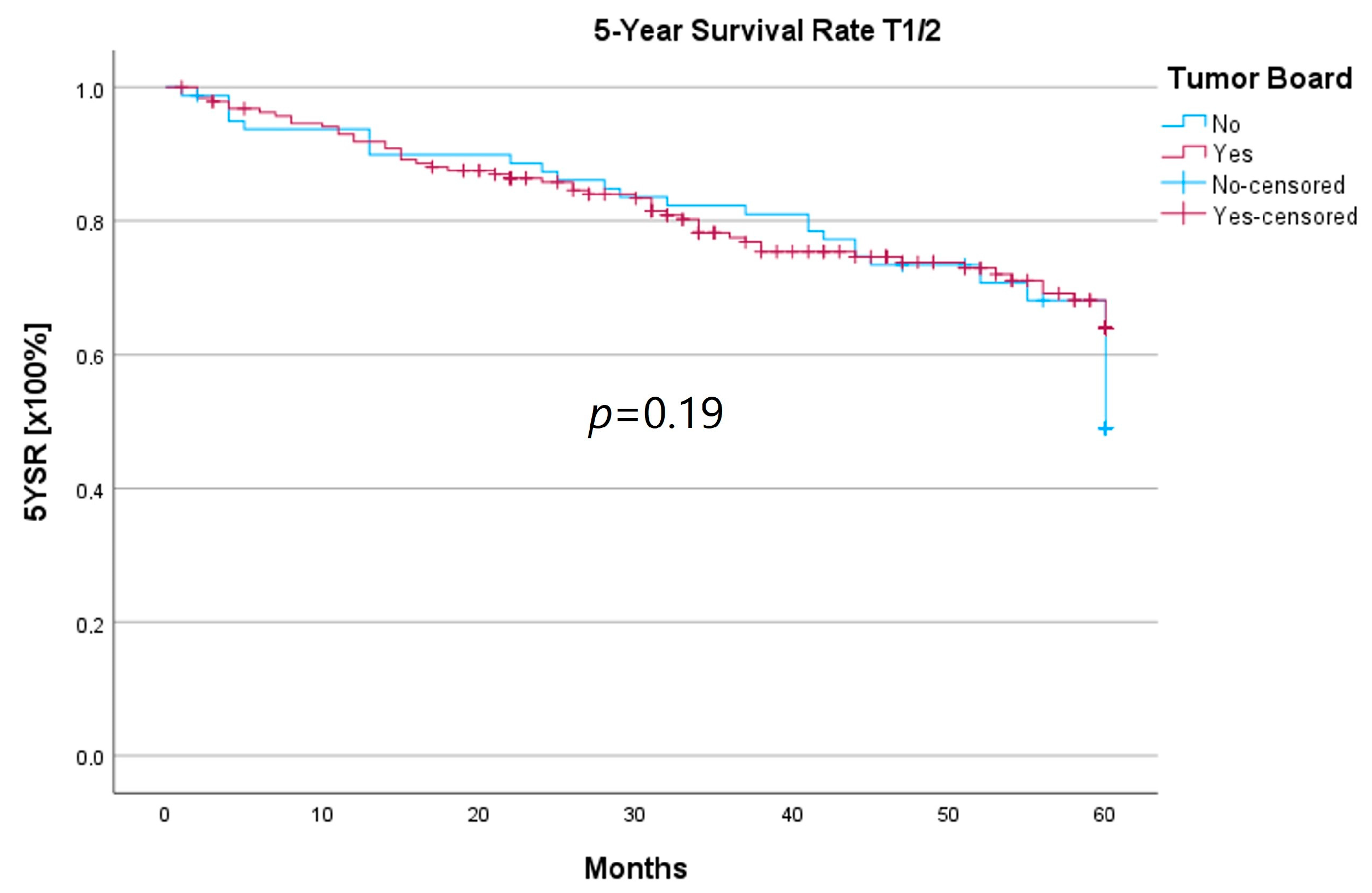
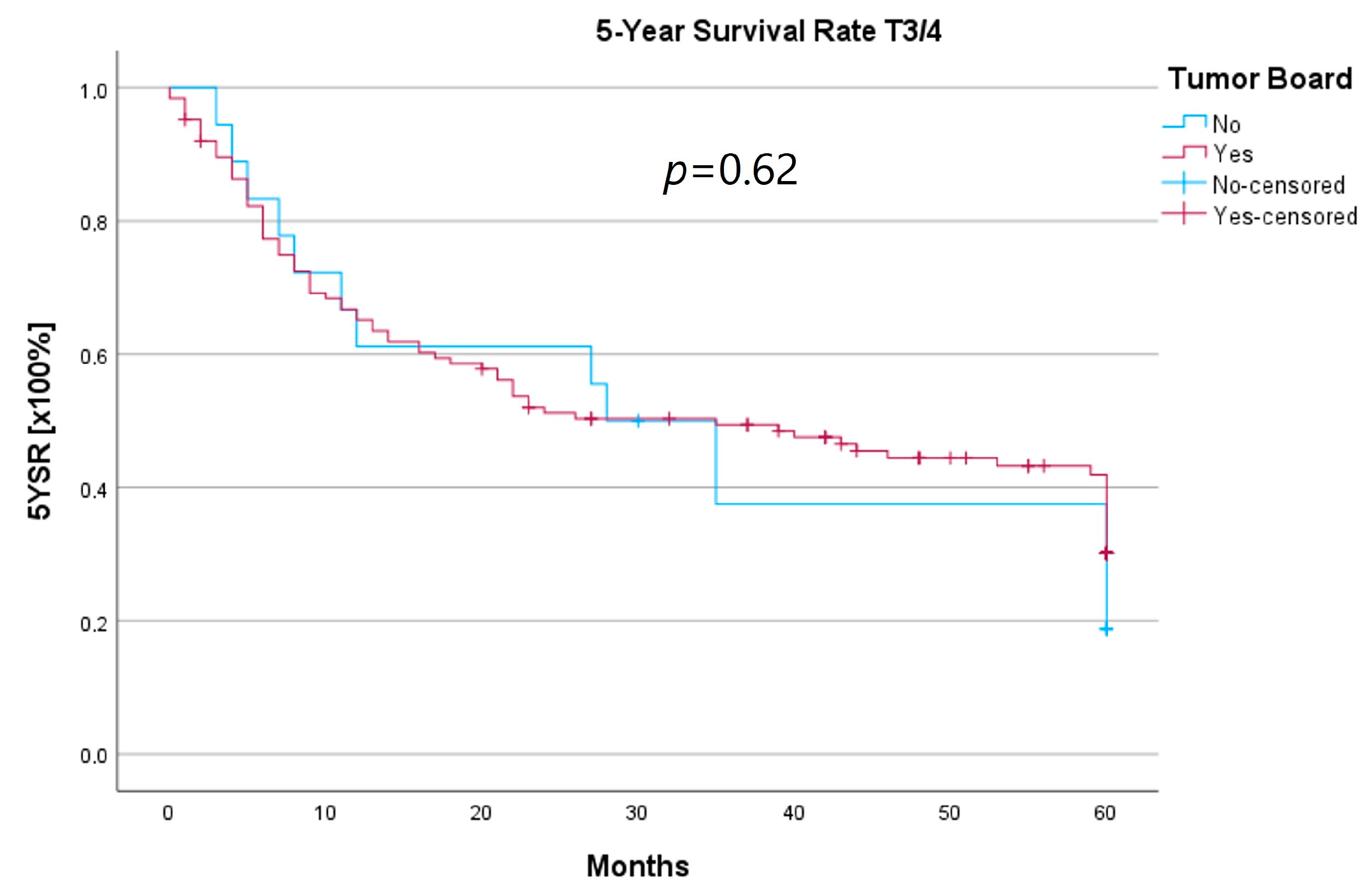
3.4. Subset Analysis of the T3/4 Cohort and Laryngectomy-Free Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, D.K., AWMF). Diagnostik, Therapie und Nachsorge des Larynxkarzinoms, Langversion 1.1. Available online: http://www.leitlinienprogramm-onkologie.de/leitlinien/larynxkarzinom/ (accessed on 11 September 2023).
- Westin, T.; Stalfors, J. Tumour boards/multidisciplinary head and neck cancer meetings: Are they of value to patients, treating staff or a political additional drain on healthcare resources? Curr. Opin. Otolaryngol. Head Neck Surg. 2008, 16, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Friedland, P.L.; Bozic, B.; Dewar, J.; Kuan, R.; Meyer, C.; Phillips, M. Impact of multidisciplinary team management in head and neck cancer patients. Br. J. Cancer 2011, 104, 1246–1248. [Google Scholar] [CrossRef]
- Iro, H.; Ehrenfeld, M. FAQ’ s zum Erhebungsbogen für Kopf-Hals-Tumor-Zentren Modul im Onkologischen Zentrum. Available online: https://www.onkozert.de/wordpress/wp-content/uploads/2021/09/eb_mkht-F_faq_210908.pdf?v=80906458 (accessed on 11 September 2023).
- Winter, A.; Iro, H.; Wolff, K.D.; Wesselmann, S. Certification of head and neck tumor centers by the German Cancer Society: An overview. Hno 2013, 61, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Heil, J.; Gondos, A.; Rauch, G.; Marmé, F.; Rom, J.; Golatta, M.; Junkermann, H.; Sinn, P.; Aulmann, S.; Debus, J.J.T.B. Outcome analysis of patients with primary breast cancer initially treated at a certified academic breast unit. Breast 2012, 21, 303–308. [Google Scholar] [CrossRef]
- Kreienberg, R.; Wöckel, A.; Wischnewsky, M.J.T.b. Highly significant improvement in guideline adherence, relapse-free and overall survival in breast cancer patients when treated at certified breast cancer centres: An evaluation of 8323 patients. Breast 2018, 40, 54–59. [Google Scholar]
- von Wilmowsky, C.; Traxdorf, M.; Adler, W.; Neukam, F.W.; Iro, H.; Nkenke, E.; Kesting, M.; Wurm, M. Survival benefit for patients treated in a certified head and neck tumor center. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 2863–2869. [Google Scholar] [CrossRef]
- Yoo, J.; Lacchetti, C.; Hammond, J.A.; Gilbert, R.W.; Head and Neck Cancer Disease Site Group. Role of endolaryngeal surgery (with or without laser) versus radiotherapy in the management of early (T1) glottic cancer: A systematic review. Head Neck 2014, 36, 1807–1819. [Google Scholar] [CrossRef]
- Gabel, M.; Hilton, N.E.; Nathanson, S.D. Multidisciplinary breast cancer clinics: Do they work? Cancer Interdiscip. Int. J. Am. Cancer Soc. 1997, 79, 2380–2384. [Google Scholar] [CrossRef]
- Dyckhoff, G.; Warta, R.; Herold-Mende, C.; Plinkert, P.K.; Ramroth, H. Larynx preservation up to T4 laryngeal cancer? Hno 2022, 70, 595–600. [Google Scholar] [CrossRef]
- Alkasbi, J.; Mortuaire, G.; Rysman, B.; Nicot, R.; Chevalier, D.; Mouawad, F. Match between therapeutic proposal in multidisciplinary tumor board and actual treatment in head and neck cancer. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2021, 138, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Hollunder, S.; Herrlinger, U.; Zipfel, M.; Schmolders, J.; Janzen, V.; Thiesler, T.; Güresir, E.; Schröck, A.; Far, F.; Pietsch, T.; et al. Cross-sectional increase of adherence to multidisciplinary tumor board decisions. BMC Cancer 2018, 18, 936. [Google Scholar] [CrossRef] [PubMed]
- Graessle, R.; Stromberger, C.; Heiland, M.; Doll, C.; Hofmann, V.M.; Klinghammer, K.; Tinhofer, I.; Olze, H.; Beck, M.; Arens, P.J.C. Predictors for Adherence to Treatment Strategies in Elderly HNSCC Patients. Cancers 2022, 14, 423. [Google Scholar] [CrossRef] [PubMed]
- Megwalu, U.C.; Sikora, A.G. Survival outcomes in advanced laryngeal cancer. JAMA Otolaryngol. Head Neck Surg. 2014, 140, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Coca-Pelaz, A.; Takes, R.P.; Hutcheson, K.; Saba, N.F.; Haigentz, M.; Bradford, C.R.; de Bree, R.; Strojan, P.; Lund, V.J.; Mendenhall, W.M.; et al. Head and neck cancer: A review of the impact of treatment delay on outcome. Adv. Ther. 2018, 35, 153–160. [Google Scholar] [CrossRef]
- Primdahl, H.; Linnet Nielsen, A.; Larsen, S.; Andersen, E.; Ipsen, M.; Lajer, C.; Weber Vestermark, L.; Andersen, L.J.; Sand Hansen, H.; Overgaard, M.J. Changes from 1992 to 2002 in the pretreatment delay for patients with squamous cell carcinoma of larynx or pharynx: A Danish nationwide survey from DAHANCA. Acta Oncol. 2006, 45, 156–161. [Google Scholar] [CrossRef]
- Piccirillo, J.F. Importance of comorbidity in head and neck cancer. Laryngoscope 2000, 110, 593–602. [Google Scholar] [CrossRef]
- Kompelli, A.R.; Li, H.; Neskey, D.M. Impact of Delay in Treatment Initiation on Overall Survival in Laryngeal Cancers. Otolaryngol. Head Neck Surg. 2019, 160, 651–657. [Google Scholar] [CrossRef]
- Aydinguel, O.; Jussupow, E.; Spohrer, K.; Heinzl, A. Designing a Mobile Application for Ad-Hoc Tumor Board Scheduling. In Proceedings of the 26th European Conference on Information Systems: Beyond Digitization—Facets of Socio-Technical Change, ECIS, Portsmouth, UK, 23–28 June 2018; p. 70. [Google Scholar]
- Sood, T.; Supriya, M.; Thopil, J.; Surendra, V.; Patel, B.B. One stop neck lump clinic: A boon for quick diagnosis and early management. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 4951–4954. [Google Scholar] [CrossRef]
- Fesinmeyer, M.D.; Mehta, V.; Blough, D.; Tock, L.; Ramsey, S.D. Effect of radiotherapy interruptions on survival in medicare enrollees with local and regional head-and-neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 675–681. [Google Scholar] [CrossRef]
- Farquhar, D.R.; Masood, M.M.; Lenze, N.R.; Sheth, S.; Patel, S.N.; Lumley, C.; Zanation, A.M.; Weissler, M.C.; Olshan, A.F.; Hackman, T.G. Academic affiliation and surgical volume predict survival in head and neck cancer patients receiving surgery. Laryngoscope 2021, 131, E479–E488. [Google Scholar] [CrossRef] [PubMed]
- Benoit, C.; Orbach, D.; Cyrille, S.; Belhous, K.; Minard-Colin, V.; Kadlub, N.; Kolb, F.; Reguerre, Y.; Carton, M.; Bolle, S. Head and neck tumors in children and adolescents: Impact of a multidisciplinary tumor board. Oral Oncol. 2021, 114, 105145. [Google Scholar] [CrossRef] [PubMed]
- Kelly, S.L.; Jackson, J.E.; Hickey, B.E.; Szallasi, F.G.; Bond, C.A. Multidisciplinary clinic care improves adherence to best practice in head and neck cancer. Am. J. Otolaryngol. 2013, 34, 57–60. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pretherapeutic HNT | No Pretherapeutic HNT | p-Value | |
|---|---|---|---|
| N | 314 | 98 | |
| Age at initial diagnosis (years) | |||
| Mean ± SD (Median) | 65.8 ± 11 (66) | 64.2 ± 10.6 (64) | 0.21 |
| Gender, n (%) | |||
| Male:Female | 265 (84)/49 (16) | 88 (90)/10 (10) | 0.15 |
| Tumor localization, n (%) | 0.89 | ||
| Glottis | 174 (55) | 64 (65) | |
| Supraglottis | 74 (24) | 13 (13) | |
| Subglottis | 8 (3) | 1 (1) | |
| Laryngeal cartilage | 1 (0.3) | 1 (1) | |
| Overlapping sites of larynx | 56 (18) | 15 (15) | |
| Larynx, unspecified | 1 (0.3) | 4 (4) | |
| T status, n (%) | <0.001 | ||
| T1 | 143 (46) | 58 (59) | |
| T2 | 45 (14) | 22 (22) | |
| T3 | 57 (18) | 6 (6) | |
| T4 | 68 (22) | 12 (12) | |
| N status, n (%) | 0.15 | ||
| N0 | 211 (67) | 70 (71) | |
| N1 | 13 (4) | 5 (5) | |
| N2 | 81 (26) | 20 (20) | |
| N3 | 8 (3) | 1 (1) | |
| M status, n (%) | 0.23 | ||
| M0 | 295 (94) | 94 (96) | |
| M1 | 18 (6) | 3 (3) | |
| UICC classification, n (%) | 0.003 | ||
| I | 138 (44) | 55 (56) | |
| II | 25 (8) | 16 (15) | |
| III | 34 (11) | 5 (5) | |
| IVA | 59 (19) | 11 (11) | |
| IVB | 39 (12) | 9 (9) | |
| IVC | 18 (6) | 3 (3) | |
| R status, n (%) | 0.4 | ||
| R0 | 126 (87) | 53 (83) | |
| R1 | 19 (13) | 11 (17) | |
| Recurrence, n (%) | 0.41 | ||
| None | 244 (78) | 80 (82) | |
| Local | 41 (13) | 12 (12) | |
| Regional | 8 (3) | - | |
| Distant | 4 (1) | 3 (3) | |
| Locoregional | 12 (4) | 2 (2) | |
| Loco distant | 3 (1) | - | |
| Regional and distant | 1 (0.3) | 1 (1) | |
| Locoregional and distant | 1 (0.3) | - | |
| Secondary tumors, n (%) | 0.56 | ||
| 0 | 257 (82) | 71 (72) | |
| 1 | 51 (16) | 22 (22) | |
| 2 | 4 (1) | 4 (4) | |
| 3 | 2 (0.6) | - | |
| 5 | - | 1 (1) |
| Pretherapeutic HNT | No Pretherapeutic HNT | p-Value | |
|---|---|---|---|
| Therapy, n (%) Surgery pC/RT | <0.001 | ||
| 145 (46) | 64 (65) | ||
| 140 (45) | 28 (29) | ||
| Best supportive care | 18 (6) | 3 (3) | |
| Adjuvant therapy, n (%) | 25 (17) | 10 (16) | 0.77 |
| Delta diagnosis > HNT presentation (days) | |||
| Mean ± SD (Median) | 12.3 ± 22.9 (10) | - | |
| Delta diagnosis > therapy initiation (days) | 0.008 | ||
| Mean ± SD (Median) | 37.9 ± 62 (27) | 20.1 ± 19 (15) | |
| Delta diagnosis > surgery (days) Mean ± SD (Median) | 20.6 ± 12.6 (20) | 11.8 ± 9 (12) | <0.001 |
| Delta diagnosis > pC/RT (days) Mean ± SD (Median) | 54.7 ± 81.6 (41) | 40.7 ± 22 (38) | 0.4 |
| Non-tumor-board-adherent cases, n (%) | 18 (6) | - | |
| Patient’s wish | 11 (4) | - | |
| Intra-clinic decision | 4 (1) | - | |
| Unknown | 3 (1) | - |
| Pretherapeutic HNT | No Pretherapeutic HNT | p-Value | |
|---|---|---|---|
| Therapy, n (%) | 0.027 | ||
| Surgery | 122 (65) | 61 (76) | |
| pC/RT | 59 (31) | 15 (19) |
| Pretherapeutic HNT | No Pretherapeutic HNT | p-Value | |
|---|---|---|---|
| 5-Year Survival Rate (5YSR) (months) | 0.96 | ||
| Mean ± SD | 43.4 ± 1.3 | 47 ± 2 | |
| 5-Year Recurrence-Free Survival (5Y-RFS) (months) | 0.16 | ||
| Mean ± SD | 48.2 ± 1.3 | 51.9 ± 1.8 |
| Pretherapeutic HNT | No Pretherapeutic HNT | p-Value | |
|---|---|---|---|
| 5YSR for T1/2 (months) | 0.19 | ||
| Mean ± SD | 49.7 ± 1.4 | 50.2 ± 2 | |
| 5YSR for T3/4 (months) | 0.62 | ||
| Mean ± SD | 33.7 ± 2.3 | 32.7 ± 5.7 | |
| 5Y-RFS for T1/2 (months) | 0.55 | ||
| Mean ± SD | 50.8 ± 1.4 | 52.9 ± 1.9 | |
| 5Y-RFS for T3/4 (months) | 0.49 | ||
| Mean ± SD | 42.6 ± 2.5 | 44.7 ± 6.2 |
| Variable | Hazard Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Age at initial diagnosis | 1.051 | 1.034–1.069 | <0.001 |
| UICC classification UICC I–II vs. UICC III–IV | 2.954 | 2.125–4.107 | <0.001 |
| Secondary tumors | 1.241 | 1.009–1.525 | 0.04 |
| Pretherapeutic HNT | No Pretherapeutic HNT | p-Value | |
|---|---|---|---|
| N | 125 | 18 | |
| Age at initial diagnosis (years) | 0.82 | ||
| Mean ± SD | 65.7 ± 10.9 | 66.4 ± 7.6 | |
| Gender, n (%) | 0.6 | ||
| Male:Female | 109 (87)/16 (13) | 15 (83)/3 (17) | |
| Tumor localization, n (%) | 0.002 | ||
| Glottis | 32 (26) | 2 (11) | |
| Supraglottis | 40 (32) | 2 (11) | |
| Subglottis | 2 (2) | - | |
| Laryngeal cartilage | - | - | |
| Overlapping sites of larynx | 51 (41) | 11 (61) | |
| Larynx, unspecified | - | 3 (17) | |
| T status, n (%) | 0.48 | ||
| T3 | 55 (44) | 6 (33) | |
| T4a | 68 (54) | 12 (67) | |
| T4b | 2 (2) | - | |
| N status, n (%) | 0.64 | ||
| N0 | 48 (38) | 4 (22) | |
| N1 | 6 (5) | 3 (17) | |
| N2 | 66 (53) | 11 (61) | |
| N3 | 5 (4) | - | |
| M status, n (%) | <0.001 | ||
| M0 | 112 (90) | 18 (100) | |
| M1 | 13 (10) | - | |
| R status, n (%) | 0.22 | ||
| R0 | 20 (87) | 2 (67) | |
| R1 | 3 (13) | 1 (33) | |
| Recurrence, n (%) | 0.75 | ||
| None | 72 (67) | 7 (64) | |
| Local | 17 16) | 1 (9) | |
| Regional | 2 (2) | - | |
| Distant | 3 (3) | 2 (18) | |
| Locoregional | 8 (8) | 1 (9) | |
| Loco distant | 3 (3) | - | |
| Regional and distant | 1 (1) | - | |
| Locoregional and distant | 1 (1) | - | |
| Therapy, n (%) | 0.69 | ||
| Laryngectomy | 19 (15) | 2 (11) | |
| Partial laryngectomy | 4 (3) | 1 (6) | |
| pC/RT | 82 (66) | 13 (72) | |
| Best supportive care | 14 (11) | 1 (6) | |
| Unknown/no therapy | 6 (5) | 1 (6) | |
| Adjuvant therapy, n (%) | 17 (74) | 3 (100) | 0.97 |
| Neck Dissection, n (%) | 21 (91) | 3 (100) | 0.76 |
| Laryngectomy | pC/RT | p-Value | |
|---|---|---|---|
| N | 21 | 95 | |
| 5YSR (months) | 0.52 | ||
| Mean ± SD | 39.7 ± 5.5 | 36.1 ± 2.5 | |
| 5Y-RFS (months) | 0.17 | ||
| Mean ± SD | 50.4 ± 5 | 40.9 ± 2.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Shabrawi, K.; Burkhardt, V.; Becker, C. Impact of a Multidisciplinary Head and Neck Tumor Board on Treatment and Survival in Laryngeal Carcinoma. Curr. Oncol. 2023, 30, 10085-10099. https://doi.org/10.3390/curroncol30120733
El-Shabrawi K, Burkhardt V, Becker C. Impact of a Multidisciplinary Head and Neck Tumor Board on Treatment and Survival in Laryngeal Carcinoma. Current Oncology. 2023; 30(12):10085-10099. https://doi.org/10.3390/curroncol30120733
Chicago/Turabian StyleEl-Shabrawi, Katharina, Valentin Burkhardt, and Christoph Becker. 2023. "Impact of a Multidisciplinary Head and Neck Tumor Board on Treatment and Survival in Laryngeal Carcinoma" Current Oncology 30, no. 12: 10085-10099. https://doi.org/10.3390/curroncol30120733
APA StyleEl-Shabrawi, K., Burkhardt, V., & Becker, C. (2023). Impact of a Multidisciplinary Head and Neck Tumor Board on Treatment and Survival in Laryngeal Carcinoma. Current Oncology, 30(12), 10085-10099. https://doi.org/10.3390/curroncol30120733