Characteristics of Primary Cutaneous Lymphoma in Italy: A Tertiary Care, Single-Center Study

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
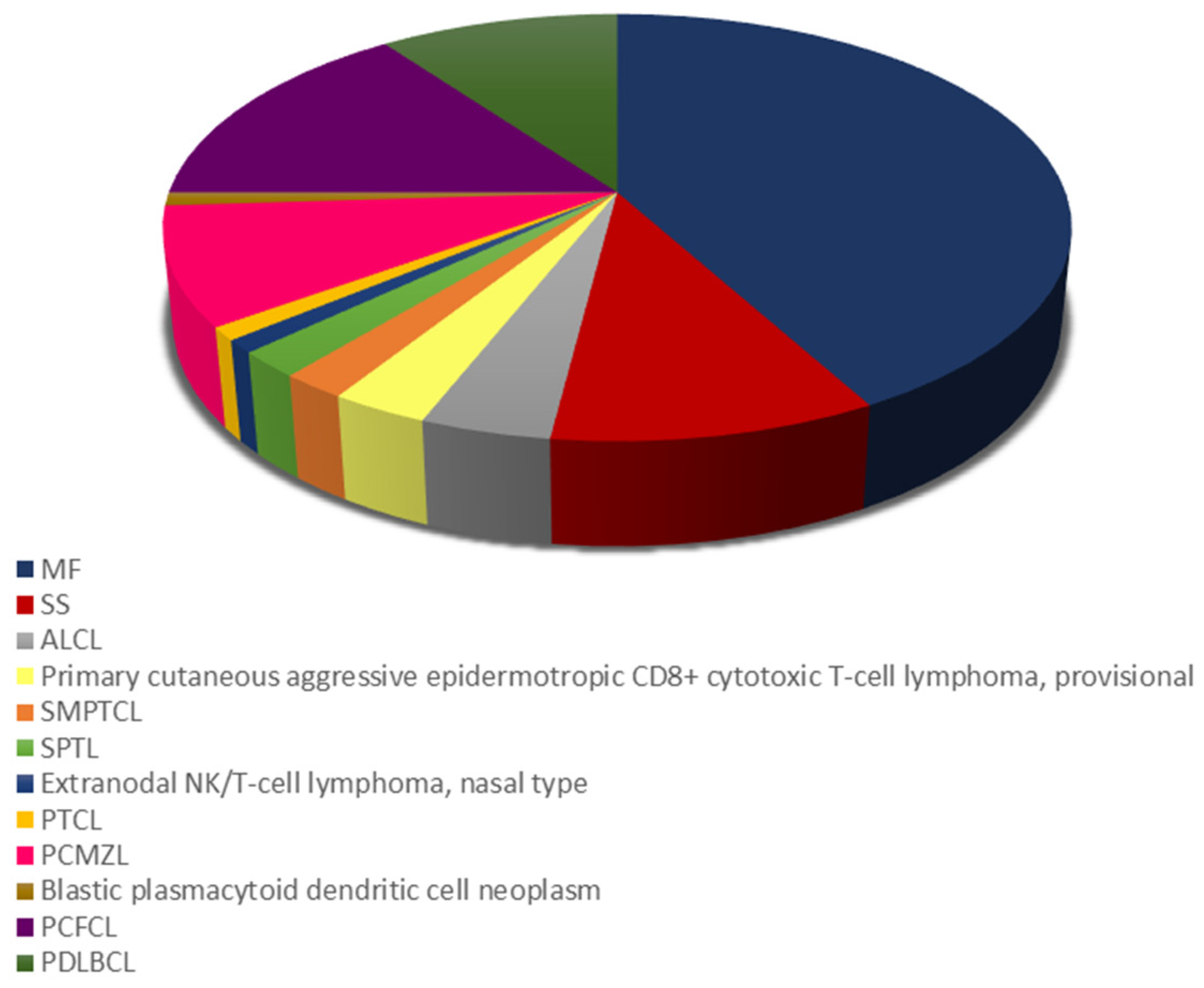
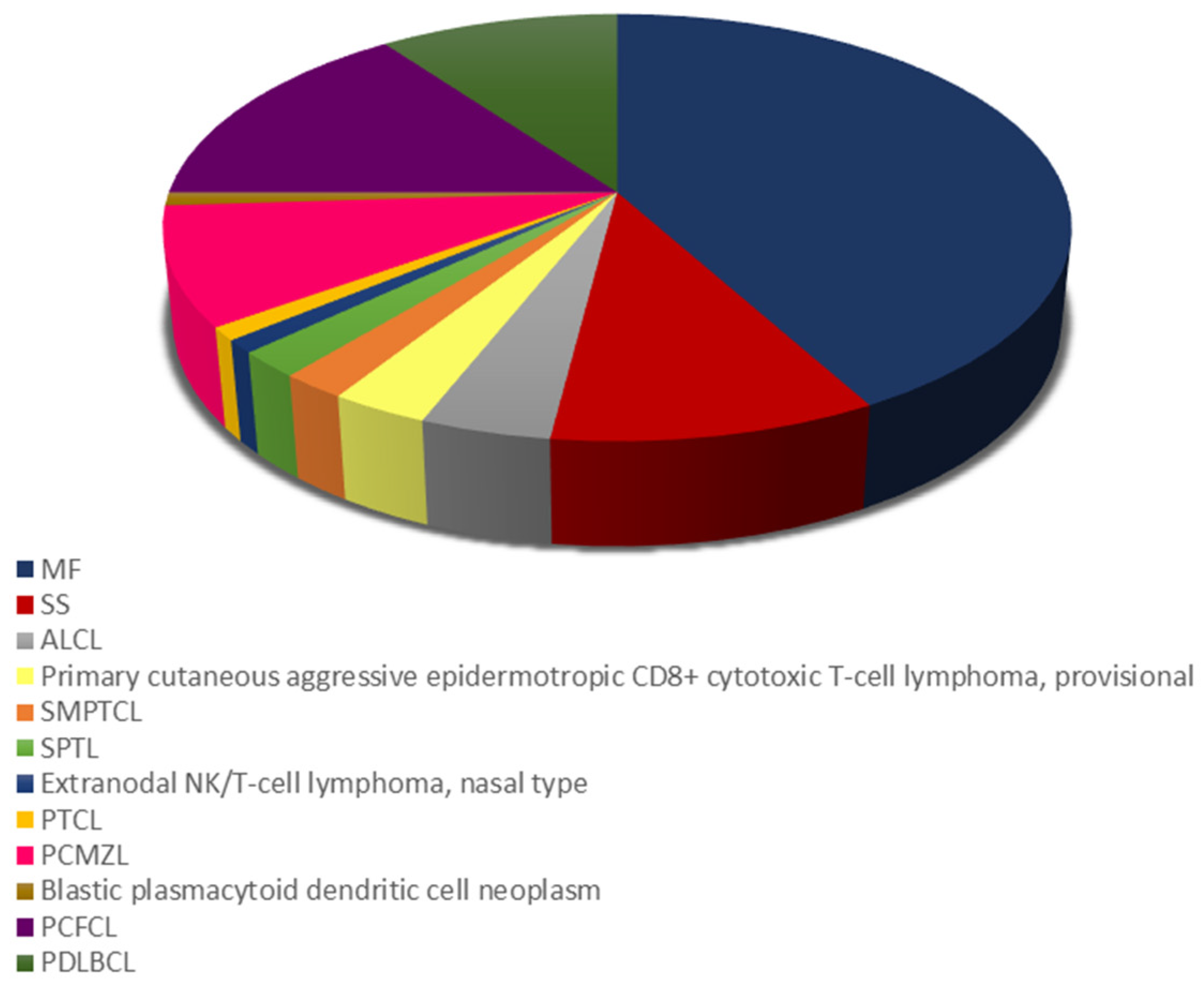
3.1. Demographics and PCL Subtype Subsection
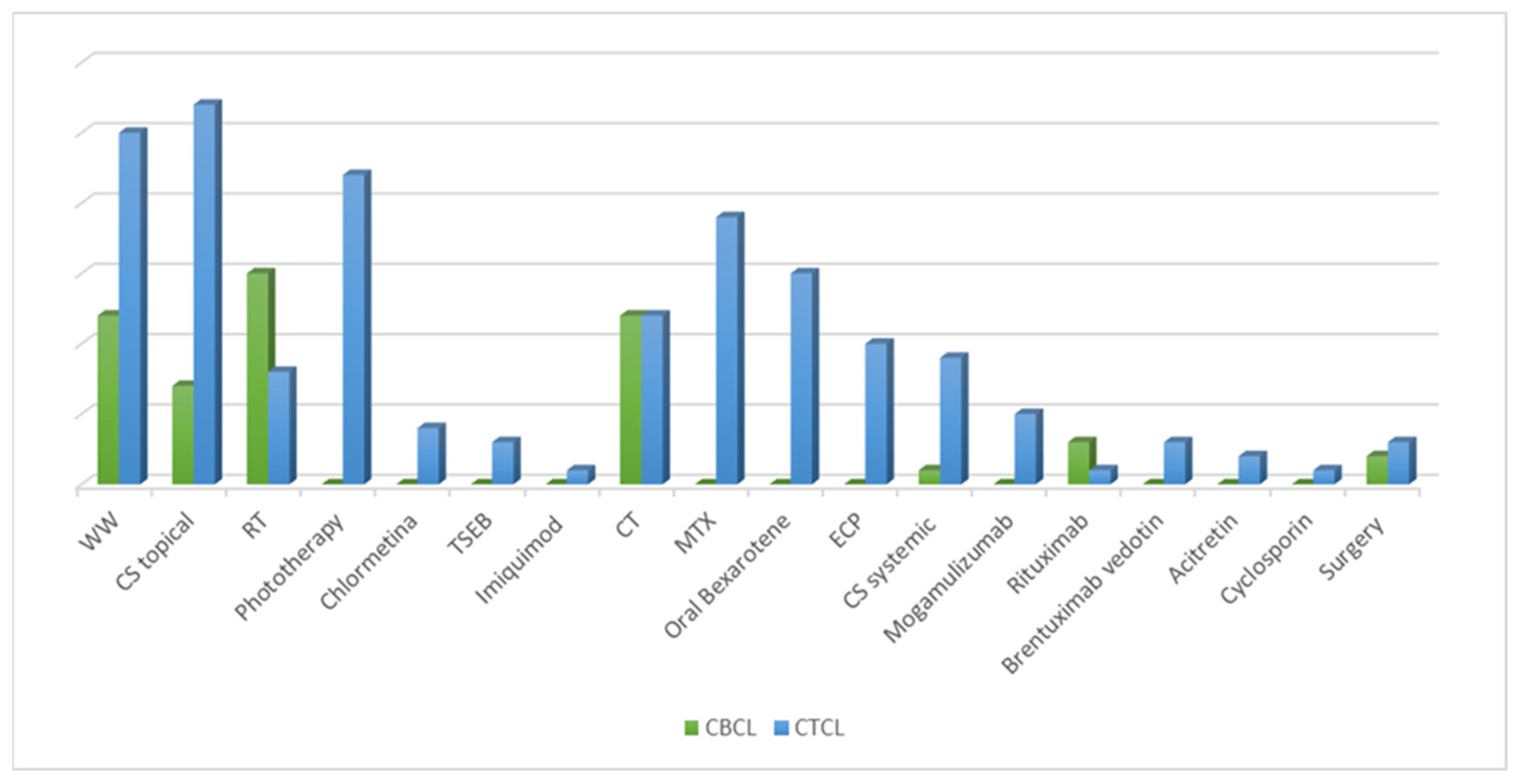
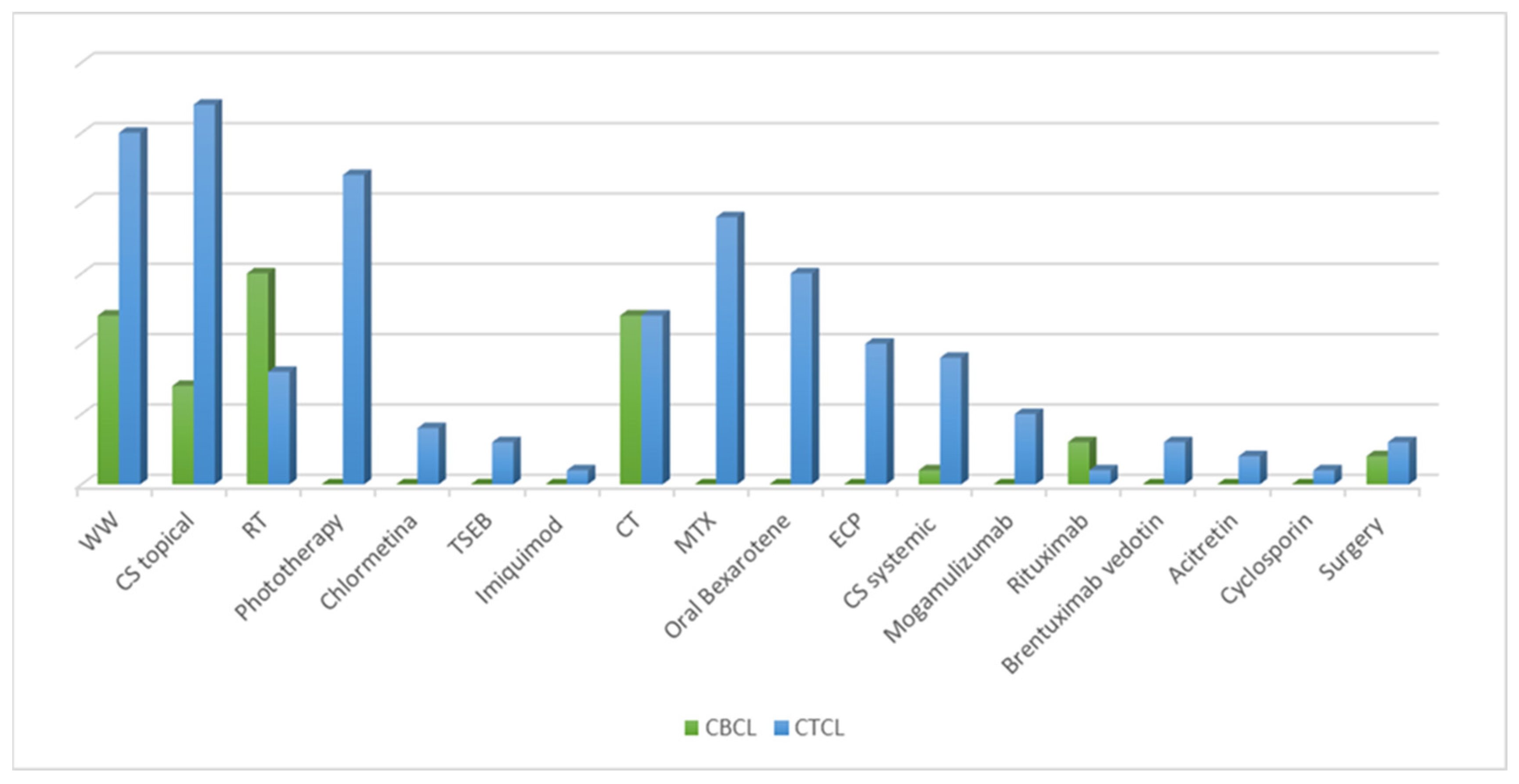
3.2. Treatment Modalities
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Willemze, R.; Cerron, L.; Kempf, W.; Berti, E.; Facchetti, F.; Swerdlow, S.H.; Jaffe, E.S. The 2018 update of the WHO-EORTC classification for primary cutaneous lymphomas. Blood 2019, 133, 1703–1714. [Google Scholar] [CrossRef] [PubMed]
- Dobos, G.; Miladi, M.; Michel, L.; Ram-Wolff, C.; Battistella, M.; Bagot, M.; de Masson, A. Recent advances on cutaneous lymphoma epidemiology. Presse Med. 2022, 51, 104108. [Google Scholar] [CrossRef] [PubMed]
- Dobos, G.; de Masson, A.; Ram-Wolff, C.; Beylot-Barry, M.; Pham-Ledard, A.; Ortonne, N.; Ingen-Housz-Oro, S.; Battistella, M.; d’Incan, M.; Rouanet, J.; et al. Epidemiological changes in cutaneous lymphomas: An analysis of 8593 patients from the French Cutaneous Lymphoma Registry. Br. J. Dermatol. 2021, 184, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Maurelli, M.; Tessari, G.; Colato, C.; Schena, D.; Girolomoni, G. Incidence and ten-year follow-up of primary cutaneous lymphomas: A single-centre cohort study. Eur. J. Dermatol. 2018, 28, 44–49. [Google Scholar] [CrossRef]
- Rubio-Gonzalez, B.; Zain, J.; Rosen, S.T.; Querfeld, C. Clinical manifestations and pathogenesis of cutaneous lymphomas: Current status and future directions. Br. J. Haematol. 2017, 176, 16–36. [Google Scholar] [CrossRef]
- Stadler, R.; Stranzenbach, R. Molecular pathogenesis of cutaneous lymphomas. Exp. Dermatol. 2018, 27, 1078–1083. [Google Scholar] [CrossRef]
- Hodak, E.; Amitay-Laish, I. Mycosis fungoides: A great imitator. Clin. Dermatol. 2019, 37, 255–267. [Google Scholar] [CrossRef]
- Scarisbrick, J.J.; Prince, H.M.; Vermeer, M.H.; Quaglino, P.; Horwitz, S.; Porcu, P.; Stadler, R.; Wood, G.S.; Beylot-Barry, M.; Pham-Ledard, A.; et al. Cutaneous Lymphoma International Consortium Study of Outcome in Advanced Stages of Mycosis Fungoides and Sezary Syndrome: Effect of Specific Prognostic Markers on Survival and Development of a Prognostic Model. J. Clin. Oncol. 2015, 33, 3766–3773. [Google Scholar] [CrossRef]
- Mehta-Shah, N.; Horwitz, S.M.; Ansell, S.; Ai, W.Z.; Barnes, J.; Barta, S.K.; Clemens, M.W.; Dogan, A.; Fisher, K.; Goodman, A.M.; et al. NCCN Guidelines Insights: Primary Cutaneous Lymphomas, Version 2. J. Natl. Compr. Canc. Netw. 2020, 18, 522–536. [Google Scholar] [CrossRef]
- Gilson, D.; Whittaker, S.J.; Child, F.J.; Scarisbrick, J.J.; Illidge, T.M.; Parry, E.J.; Mohd Mustapa, M.F.; Exton, L.S.; Kanfer, E.; Rezvani, K.; et al. British Association of Dermatologists and U.K. Cutaneous Lymphoma Group guidelines for the management of primary cutaneous lymphomas 2018. Br J Dermatol. 2019, 180, 496–526. [Google Scholar] [CrossRef]
- Willemze, R.; Hodak, E.; Zinzani, P.L.; Specht, L.; Ladetto, M. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv30–iv40. [Google Scholar] [CrossRef] [PubMed]
- Olsen, E.A.; Whittaker, S.; Willemze, R.; Pinter-Brown, L.; Foss, F.; Geskin, L.; Schwartz, L.; Horwitz, S.; Guitart, J.; Zic, J.; et al. Primary cutaneous lymphoma: Recommendations for clinical trial design and staging update from the ISCL, USCLC, and EORTC. Blood 2022, 140, 419–437. [Google Scholar] [CrossRef] [PubMed]
- Senff, N.J.; Noordijk, E.M.; Kim, Y.H.; Bagot, M.; Berti, E.; Cerroni, L.; Dummer, R.; Duvic, M.; Hoppe, R.T.; Pimpinelli, N.; et al. European Organization for Research and Treatment of Cancer and International Society for Cutaneous Lymphoma consensus recommendations for the management of cutaneous B-cell lymphomas. Blood 2008, 112, 1600–1609. [Google Scholar] [CrossRef] [PubMed]
- Willemze, R.; Jaffe, E.S.; Burg, G.; Cerroni, L.; Berti, E.; Swerdlow, S.H.; Ralfkiaer, E.; Chimenti, S.; Diaz-Perez, J.L.; Duncan, L.M.; et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005, 105, 3768–3785. [Google Scholar] [CrossRef]
- Kim, Y.H.; Willemze, R.; Pimpinelli, N.; Whittaker, S.; Olsen, E.A.; Ranki, A.; Dummer, R.; Hoppe, R.T.; ISCL and the EORTC. TNM classification system for primary cutaneous lymphomas other than mycosis fungoides and Sezary syndrome: A proposal of the International Society for Cutaneous Lymphomas (ISCL) and the Cutaneous Lymphoma Task Force of the European Organization of Research and Treatment of Cancer (EORTC). Blood 2007, 110, 479–484. [Google Scholar]
- Olsen, E.; Vonderheid, E.; Pimpinelli, N.; Willemze, R.; Kim, Y.; Knobler, R.; Zackheim, H.; Duvic, M.; Estrach, T.; Lamberg, S.; et al. Revisions to the staging and classification of mycosis fungoides and Sezary syndrome: A proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood 2007, 110, 1713–1722. [Google Scholar]
- Fink-Puches, R.; Zenahlik, P.; Bäck, B.; Smolle, J.; Kerl, H.; Cerroni, L. Primary cutaneous lymphomas: Applicability of current classification schemes (European Organization for Research and Treatment of Cancer, World Health Organization) based on clinicopathologic features observed in a large group of patients. Blood 2002, 99, 800–805. [Google Scholar] [CrossRef]
- Assaf, C.; Gellrich, S.; Steinhoff, M.; Nashan, D.; Weisse, F.; Dippel, E.; Coors, E.; Stein, A.; Gollin, P.; Henke, U.; et al. Cutaneous lymphomas in Germany: An analysis of the Central Cutaneous Lymphoma Registry of the German Society of Dermatology (DDG). J. Dtsch. Derm. Ges. 2007, 5, 662–668. [Google Scholar] [CrossRef]
- Bradford, P.T.; Devesa, S.S.; Anderson, W.F.; Toro, J.R. Cutaneous lymphoma incidence patterns in the United States: A population-based study of 3884 cases. Blood 2009, 113, 5064–5073. [Google Scholar] [CrossRef]
- Lee, H.S.; Suh, K.S.; Lee, D.Y.; Cho, K.H.; Oh, S.H.; Kim, S.C.; Lee, S.J.; Shin, D.H.; Yoon, T.Y.; Won, Y.H.; et al. Cutaneous Lymphoma in Korea: A Nationwide Retrospective Study. Acta Derm. Venereol. 2016, 96, 535–539. [Google Scholar] [CrossRef]
- Macagno, N.; Mastorino, L.; Rubatto, M.; Avallone, G.; Merli, M.; Agostini, A.; Fava, P.; Ribero, S.; Quaglino, P. Primary cutaneous lymphoma patients seen at a referral dermatological centre in 1 year: A single-centre observational retrospective cohort study of the diagnoses and staging, comorbidities and associated symptoms, treatment performed and clinical course. J. Eur. Acad. Derm. Venereol. 2022, 36, 2388–2392. [Google Scholar] [CrossRef] [PubMed]
- Pileri, A.; Morsia, E.; Zengarini, C.; Torre, E.; Goteri, G.; Quaglino, P.; Pimpinelli, N.; Paulli, M.; Pileri, S.A.; Zinzani, P.L.; et al. Epidemiology of cutaneous T-cell lymphomas: State of the art and a focus on the Italian Marche region. Eur. J. Dermatol. 2023, 33, 360–367. [Google Scholar] [CrossRef]
- Hristov, A.C.; Tejasvi, T.; Wilcox, R.A. Cutaneous B-cell lymphomas: 2023 update on diagnosis, risk-stratification, and management. Am. J. Hematol. 2023, 98, 1326–1332. [Google Scholar] [CrossRef] [PubMed]
- Rowe, B.; Yosipovitch, G. Malignancy-associated pruritus. Eur. J. Pain. 2016, 20, 19–23. [Google Scholar] [CrossRef]
- Claps, G.; Faouzi, S.; Quidville, V.; Chehade, F.; Shen, S.; Vagner, S.; Robert, C. The multiple roles of LDH in cancer. Nat. Rev. Clin. Oncol. 2022, 19, 749−762. [Google Scholar] [CrossRef] [PubMed]
- Serrano, L.; Martinez-Escala, M.E.; Zhou, X.A.; Guitart, J. Pruritus in Cutaneous T-Cell Lymphoma and Its Management. Derm. Clin. 2018, 36, 245–258. [Google Scholar] [CrossRef]
- Farabi, B.; Seminario-Vidal, L.; Jamgochian, M.; Akay, B.N.; Atak, M.F.; Rao, B.K.; Karagaiah, P.; Grabbe, S.; Goldust, M. Updated review on prognostic factors in mycosis fungoides and new skin lymphoma trials. J. Cosmet. Dermatol. 2022, 21, 2742–2748. [Google Scholar] [CrossRef]
- Gülseren, D.; Bostan, E.; Doğan, S.; Yalıcı-Armağan, B.; Akdoğan, N.; Ersoy-Evans, S.; Elçin, G.; Karaduman, A.; Atakan, N. Lactate dehydrogenase, Beta-2 Microglobulin Levels and CD4/CD8 Lymphocyte Ratio in Patients with Mycosis Fungoides in Stage 1A. ActaMed. 2020, 51, 16–21. [Google Scholar] [CrossRef]
- Quaglino, P.; Maule, M.; Prince, H.M.; Porcu, P.; Horwitz, S.; Duvic, M.; Talpur, R.; Vermeer, M.; Bagot, M.; Guitart, J. Global patterns of care in advanced stage mycosis fungoides/Sezary syndrome: A multicenter retrospective follow-up study from the Cutaneous Lymphoma International Consortium. Ann. Oncol. 2017, 28, 2517–2525. [Google Scholar] [CrossRef]
- Willemze, R.; Hodak, E.; Zinzani, P.L.; Specht, L.; Ladetto, M. Primary cutaneous lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24 (Suppl. 6), vi149–vi154. [Google Scholar] [CrossRef]
- Horwitz, S.M.; Olsen, E.A.; Duvic, M.; Porcu, P.; Kim, Y.H. Review of the treatment of mycosis fungoides and sezary syndrome: A stage-based approach. J. Natl. Compr. Cancer Netw. 2008, 6, 436–442. [Google Scholar] [CrossRef] [PubMed]
- Specht, L.; Skov, L. Cutaneous Lymphomas. Clin. Oncol. (R. Coll. Radiol.) 2019, 31, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Olszewska-Szopa, M.; Sobas, M.; Laribi, K.; Bao Perez, L.; Drozd-Sokołowska, J.; Subocz, E.; Joks, M.; Zduniak, K.; Gajewska, M.; de Nalecz, A.K.; et al. Primary cutaneous indolent B-cell lymphomas—A retrospective multicenter analysis and a review of literature. Acta Oncol. 2021, 60, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Nicolay, J.P.; Wobser, M. Cutaneous B-cell lymphomas - pathogenesis, diagnostic workup, and therapy. J. Dtsch. Derm. Ges. 2016, 14, 1207–1224. [Google Scholar] [CrossRef] [PubMed]
- Krenitsky, A.; Klager, S.; Hatch, L.; Sarriera-Lazaro, C.; Chen, P.L.; Seminario-Vidal, L. Update in Diagnosis and Management of Primary Cutaneous B-Cell Lymphomas. Am. J. Clin. Dermatol. 2022, 23, 689–706. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Overall (n = 100) | |
|---|---|
| Male, n (%) | 57 (57) |
| Age at diagnosis, mean (SD) | 70.33 (14.14) |
| PCL subtypes | |
| Cutaneous T-cell and NK-cell lymphomas | |
| Mycosis fungoides, n (%) | 42 (42) |
| Sezary syndrome, n (%) | 10 (10) |
| Primary cutaneous anaplastic large cell lymphoma, n (%) | 4 (4) |
| Primary cutaneous aggressive epidermotropic CD8+ cytotoxic T-cell lymphoma (provisional), n (%) | 3 (3) |
| Primary cutaneous CD4+ small/medium pleomorphic T-cell lymphoma, n (%) | 2 (2) |
| Subcutaneous panniculitis-like T-cell lymphoma, n (%) | 2 (2) |
| Extranodal NK/T-cell lymphoma, nasal type, n (%) | 1 (1) |
| Primary cutaneous peripheral T-cell lymphoma, unspecified n (%) | 1 (1) |
| Cutaneous B-cell lymphomas, n (%) | |
| Primary cutaneous follicle center lymphoma, n (%) | 15 (15) |
| Primary cutaneous diffuse large B-cell lymphoma, leg type, n (%) | 10 (10) |
| Primary cutaneous marginal zone lymphoma, n (%) | 9 (9) |
| Precursor hematological neoplasm, n (%) | |
| Blastic plasmacytoid dendritic cell neoplasm, n (%) | 1 (1) |
| TNMB stage at time of diagnosis for CTCL and CBCL * | |
| T1, n (%) | 33 (47.8) |
| T2, n (%) | 21 (30.4) |
| T3, n (%) | 4 (5.8) |
| T4, n (%) | 11 (15.9) |
| Clinical stage at time of diagnosis for MF and SS, n (%) ** | |
| IA, n (%) | 34 (73.9) |
| IB, n (%) | 5 (10.8) |
| IIA, n (%) | 1 (2.1) |
| IIB, n (%) | 0 (0) |
| IIIA, n (%) | 2 (4.3) |
| IIIB, n (%) | 0 (0) |
| IVA, n (%) | 4 (8.6) |
| IVB, n (%) | 0 (0) |
| Itch, n (%) | 22 (22) |
| LDH, mean (SD) | 211.8 (79.21) |
| LDH > ULN, n (%) | 46 (46) |
| Beta2-M, mean (SD) | 2.53 (1.50) |
| Beta2-M > ULN, n (%) | 77 (77) |
| CBCL | CTCL | p Value | |
|---|---|---|---|
| Male, n (%) | 18 (51.4) | 39 (60.0) | 0.539 |
| Age at diagnosis, mean (SD) | 64.57 (13.56) | 73.43 (13.55) | 0.002 |
| Itch, n (%) | 2 (5.7) | 20 (30.8) | 0.008 |
| LDH, median (IQR) | 181.00 (156.00, 200.00) | 200.00 (173.50, 245.00) | 0.025 |
| Beta2-M, median (IQR) | 1.75 (1.50, 2.18) | 2.40 (2.00, 3.22) | <0.001 |
| Overall n | CBCL | CBCL, RP n (%) | CBCL, RC n (%) | CTCL | CTCL, RP n (%) | CTCL, RC n (%) | Overall Follow-Up Median (IQR) | |
|---|---|---|---|---|---|---|---|---|
| W&W | 37 | 12 | 3 (75) | 1 (25) | 25 | 2 (11.8) | 10 (58.8) | 7.23 (3.73, 12.73) |
| Skin Direct therapies | ||||||||
| Topical CS | 35 | 7 | 3 (71.4) | 2 (28.6) | 27 | 9 (60) | 6 (40) | 6.07 (3.12, 11.38) |
| RT | 23 | 15 | 4 | 9 | 8 | 3 (60) | 2 (40) | 0.97 (0.62, 7.35) |
| Phototherapy | 22 | 0 | Na | Na | 22 | 10 (66.7) | 5 (33.3) | 5.02 (3.10, 8.96) |
| Chlormethine | 4 | 0 | Na | Na | 4 | 2 (100) | 0 (0) | 5.78 (3.68, 7.95) |
| TSEB | 3 | 0 | Na | Na | 3 | 3 (100) | 0 (0) | 0.97 (0.82, 2.13) |
| Imiquimod | 1 | 0 | Na | Na | 1 | 0 (0) | 0 (0) | 0.93 (0.93, 0.93) |
| Systemic therapies | ||||||||
| CT | 24 | 12 | 4 (33.3) | 8 (66.7) | 12 | 10 (90.9) | 1(9.1) | 4.13 (3.22, 6.07) |
| MTX | 19 | 0 | Na | Na | 19 | 12 (85.7) | 2 (14.3) | 6.33 (2.55, 13.65) |
| Oral bexarotene | 15 | 0 | Na | Na | 15 | 12 (85.7) | 2 (14.3) | 10.27 (5.52, 23.53) |
| ECP | 10 | 0 | Na | Na | 10 | 7 (77.8) | 2 (22.2) | 18.42 (5.28, 35.62) |
| Systemic CS | 10 | 1 | 1 (100) | Na | 9 | 5 (71.4) | 3 (42.9) | 5.15 (2.68, 13.96) |
| Mogamulizumab | 5 | 0 | Na | Na | 5 | 5 (100) | 0 (0) | 0.00 (0.00, 0.00) |
| Rituximab | 4 | 3 | 2 (66.7) | 1 (33.3) | 1 | 0 (0) | 1 (100) | 1.65 (0.00, 5.51) |
| Brentuximab-vedotin | 3 | 0 | Na | Na | 3 | 2 (66.7) | 1 (33.3) | 0.97 (3.90, 4.23,) |
| Acitretin | 2 | 0 | Na | Na | 2 | 2 (100) | 0 (0) | 13.58 (10.34, 16.82) |
| Cyclosporine | 1 | 0 | Na | Na | 1 | 1 (100) | 0 (0) | 12.13 (12.13, 12.13) |
| Surgery | 5 | 2 | 1 (50) | 1 (50) | 3 | 2 (100) | 0 (0) | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Onghia, M.; Cartocci, A.; Calabrese, L.; Maio, D.; Sirchio, A.; Erasti, M.; Tognetti, L.; Rubegni, P.; Bocchia, M.; Cencini, E.; et al. Characteristics of Primary Cutaneous Lymphoma in Italy: A Tertiary Care, Single-Center Study. Curr. Oncol. 2023, 30, 9813-9823. https://doi.org/10.3390/curroncol30110712
D’Onghia M, Cartocci A, Calabrese L, Maio D, Sirchio A, Erasti M, Tognetti L, Rubegni P, Bocchia M, Cencini E, et al. Characteristics of Primary Cutaneous Lymphoma in Italy: A Tertiary Care, Single-Center Study. Current Oncology. 2023; 30(11):9813-9823. https://doi.org/10.3390/curroncol30110712
Chicago/Turabian StyleD’Onghia, Martina, Alessandra Cartocci, Laura Calabrese, Daniele Maio, Azzurra Sirchio, Maria Erasti, Linda Tognetti, Pietro Rubegni, Monica Bocchia, Emanuele Cencini, and et al. 2023. "Characteristics of Primary Cutaneous Lymphoma in Italy: A Tertiary Care, Single-Center Study" Current Oncology 30, no. 11: 9813-9823. https://doi.org/10.3390/curroncol30110712
APA StyleD’Onghia, M., Cartocci, A., Calabrese, L., Maio, D., Sirchio, A., Erasti, M., Tognetti, L., Rubegni, P., Bocchia, M., Cencini, E., Fabbri, A., & Cinotti, E. (2023). Characteristics of Primary Cutaneous Lymphoma in Italy: A Tertiary Care, Single-Center Study. Current Oncology, 30(11), 9813-9823. https://doi.org/10.3390/curroncol30110712