Photon Absorption Remote Sensing Imaging of Breast Needle Core Biopsies Is Diagnostically Equivalent to Gold Standard H&E Histologic Assessment

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Materials
2.2. Sample Preparation Prior to PARS Imaging and Gold Standard H&E Staining
2.3. PARS Microscope Imaging
2.4. Gold Standard H&E Staining and Digital Image Acquisition
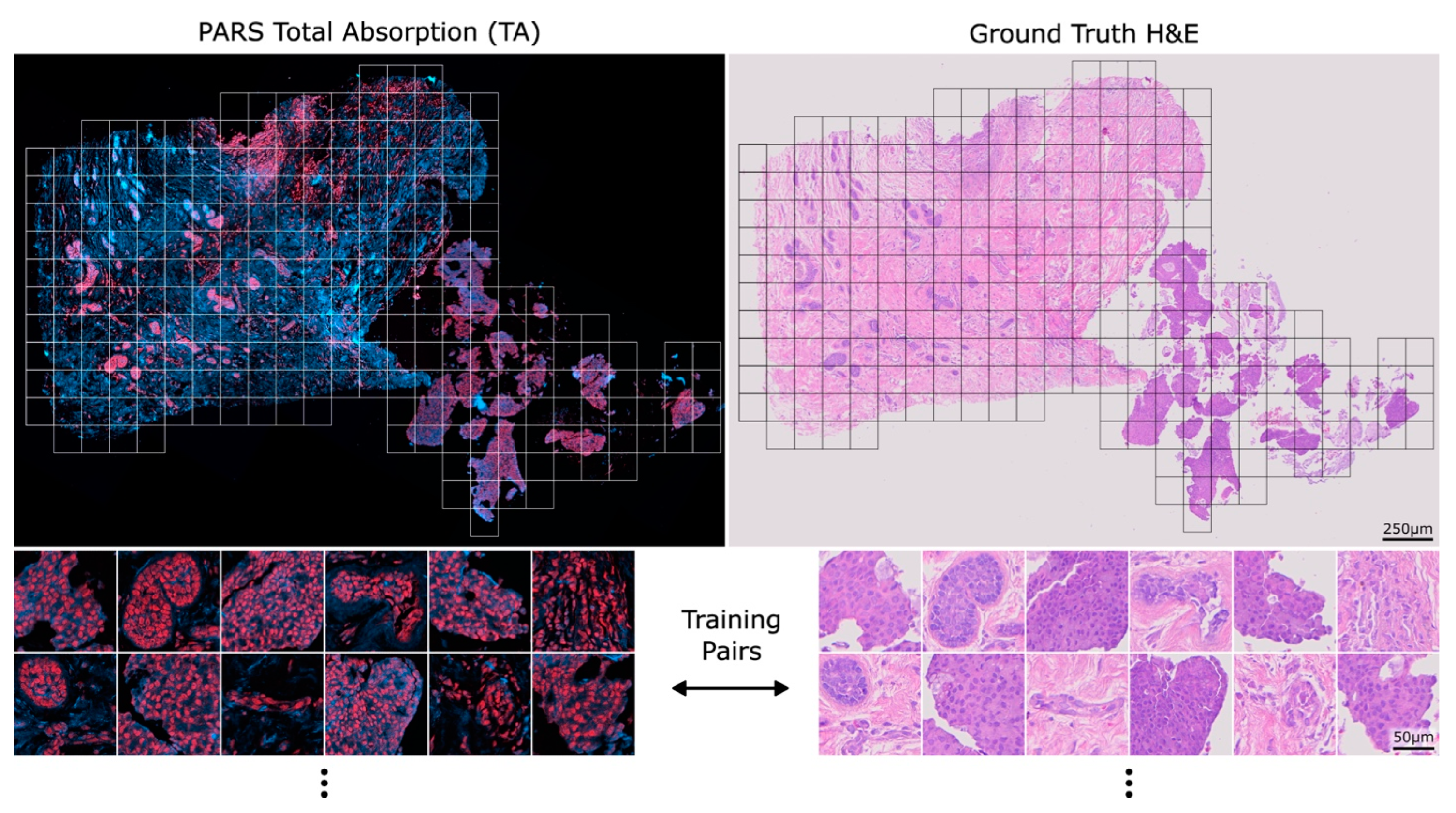
2.5. PARS Virtual H&E Colourization
2.6. Evaluation by Expert Pathologists
2.7. Statistical Analysis
3. Results
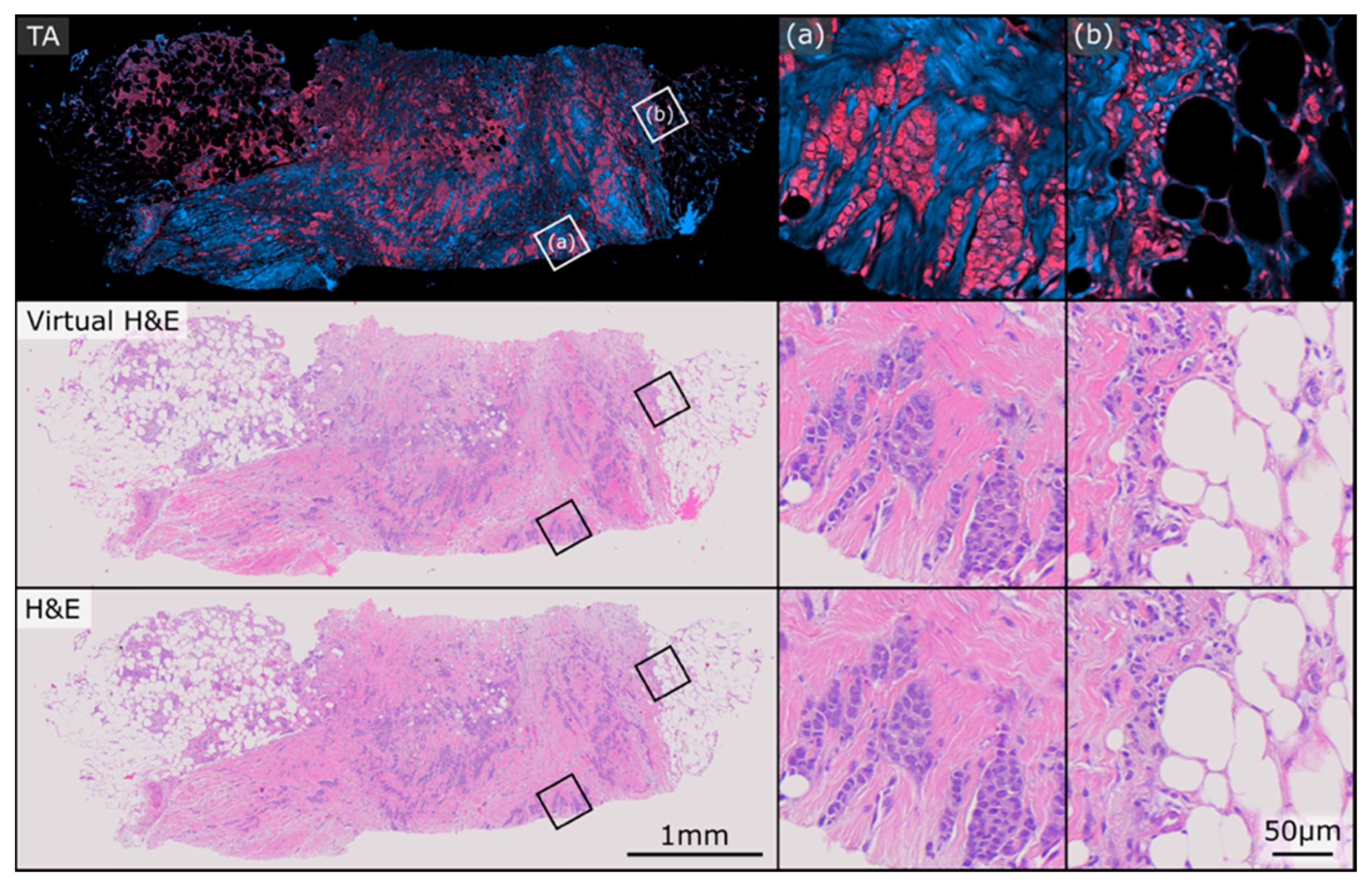
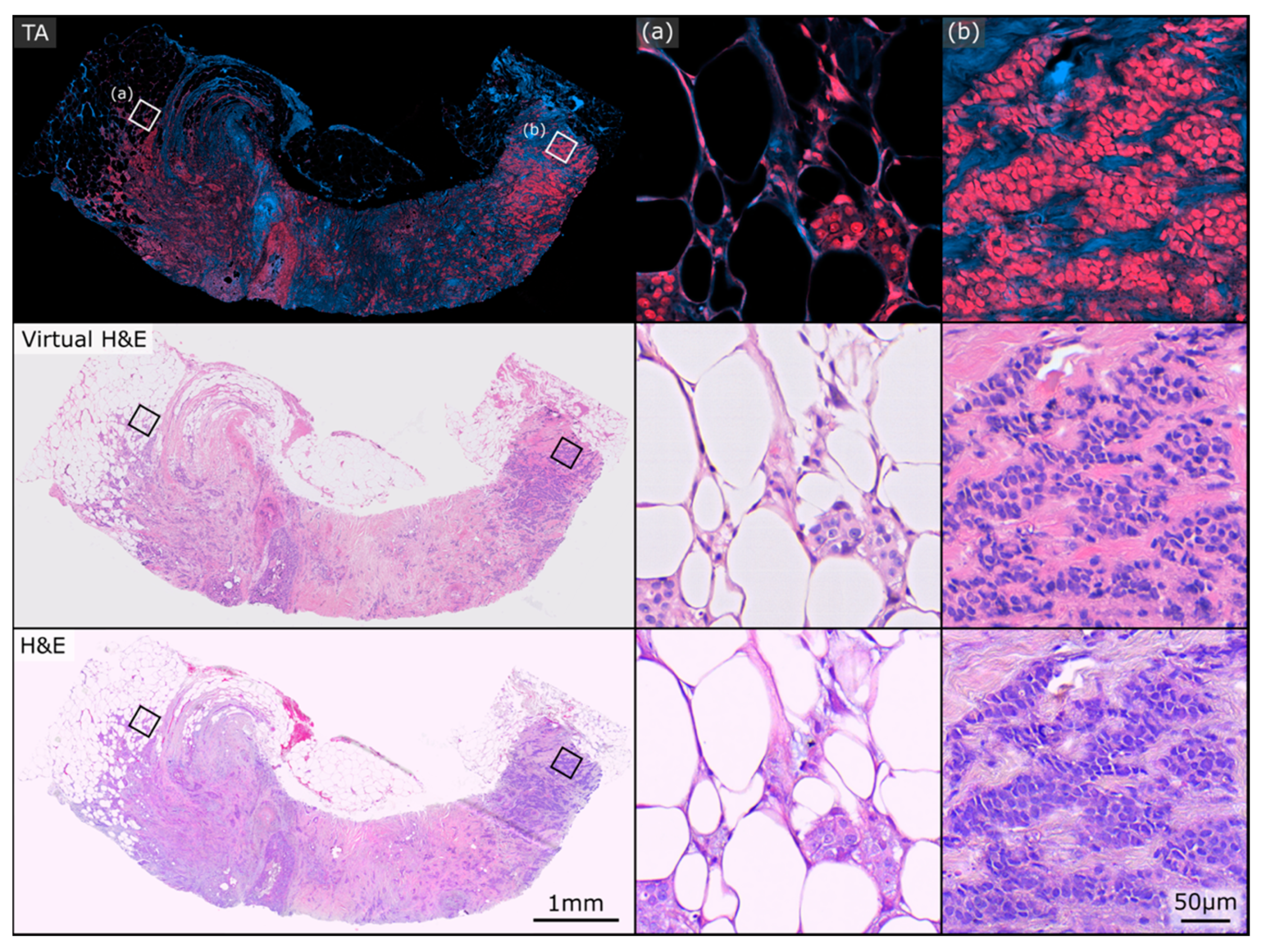
3.1. Example Whole-Slide Image Pairs
3.2. Image Origin
3.3. Primary Diagnosis
3.4. Evaluation of Tissue Gradings
4. Discussion
4.1. Study Summary and Key Findings
4.2. Interpretation of Findings in Context
4.3. Strengths, Limitations, and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bick, U.; Trimboli, R.M.; Athanasiou, A.; Balleyguier, C.; Baltzer, P.A.T.; Bernathova, M.; Borbély, K.; Brkljacic, B.; Carbonaro, L.A.; Clauser, P.; et al. Image-guided breast biopsy and localisation: Recommendations for information to women and referring physicians by the European Society of Breast Imaging. Insights Imaging 2020, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Verkooijen, H.M.; Peeters, P.H.; Buskens, E.; Koot, V.C.; Borel Rinkes, I.H.; Mali, W.P.; van Vroonhoven, T.J. Diagnostic accuracy of large-core needle biopsy for nonpalpable breast disease: A meta-analysis. Br. J. Cancer 2000, 82, 1017–1021. [Google Scholar] [CrossRef] [PubMed]
- Parker, S.H.; Burbank, F.; Jackman, R.J.; Aucreman, C.J.; Cardenosa, G.; Cink, T.M.; Coscia, J.L.; Eklund, G.W.; Evans, W.P.; Garver, P.R. Percutaneous large-core breast biopsy: A multi-institutional study. Radiology 1994, 193, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Crowe, J.P.; Rim, A.; Patrick, R.J.; Rybicki, L.A.; Grundfest-Broniatowski, S.F.; Kim, J.A.; Lee, K.B. Does core needle breast biopsy accurately reflect breast pathology? Surgery 2003, 134, 523–526; discussion 526–528. [Google Scholar] [CrossRef] [PubMed]
- Verkooijen, H.M. Diagnostic accuracy of stereotactic large-core needle biopsy for nonpalpable breast disease: Results of a multicenter prospective study with 95% surgical confirmation. Int. J. Cancer 2002, 99, 853–859. [Google Scholar] [CrossRef]
- Jackman, R.J.; Nowels, K.W.; Rodriguez-Soto, J.; Marzoni, F.A.; Finkelstein, S.I.; Shepard, M.J. Stereotactic, automated, large-core needle biopsy of nonpalpable breast lesions: False-negative and histologic underestimation rates after long-term follow-up. Radiology 1999, 210, 799–805. [Google Scholar] [CrossRef]
- Youk, J.H.; Kim, E.-K.; Kim, M.J.; Oh, K.K. Sonographically Guided 14-Gauge Core Needle Biopsy of Breast Masses: A Review of 2,420 Cases with Long-Term Follow-Up. Am. J. Roentgenol. 2008, 190, 202–207. [Google Scholar] [CrossRef]
- Hatmaker, A.R.; Donahue, R.M.J.; Tarpley, J.L.; Pearson, A.S. Cost-effective use of breast biopsy techniques in a veterans health care system. Am. J. Surg. 2006, 192, e37–e41. [Google Scholar] [CrossRef]
- Bruening, W.; Fontanarosa, J.; Tipton, K.; Treadwell, J.R.; Launders, J.; Schoelles, K. Systematic Review: Comparative Effectiveness of Core-Needle and Open Surgical Biopsy to Diagnose Breast Lesions. Ann. Intern. Med. 2010, 152, 238–246. [Google Scholar] [CrossRef]
- White, R.R.; Halperin, T.J.; Olson, J.A.; Soo, M.S.; Bentley, R.C.; Seigler, H.F. Impact of Core-Needle Breast Biopsy on the Surgical Management of Mammographic Abnormalities. Ann. Surg. 2001, 233, 769–777. [Google Scholar] [CrossRef]
- Smith, D.N.; Christian, R.; Meyer, J.E. Large-core needle biopsy of nonpalpable breast cancers. The impact on subsequent surgical excisions. Arch. Surg. 1997, 132, 256–259; discussion 260. [Google Scholar] [CrossRef] [PubMed]
- Day, C.E. (Ed.) Histopathology: Methods and Protocols; Methods in Molecular Biology; Springer: New York, NY, USA, 2014; Volume 1180, ISBN 978-1-4939-1049-6. [Google Scholar]
- Gurina, T.S.; Simms, L. Histology, Staining. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kwok, T.C.; Rakha, E.A.; Lee, A.H.S.; Grainge, M.; Green, A.R.; Ellis, I.O.; Powe, D.G. Histological grading of breast cancer on needle core biopsy: The role of immunohistochemical assessment of proliferation. Histopathology 2010, 57, 212. [Google Scholar] [CrossRef] [PubMed]
- Brown, L. Improving histopathology turnaround time: A process management approach. Curr. Diagn. Pathol. 2004, 10, 444–452. [Google Scholar] [CrossRef]
- Ecclestone, B.R.; Bell, K.; Sparkes, S.; Dinakaran, D.; Mackey, J.R.; Haji Reza, P. Label-free complete absorption microscopy using second generation photoacoustic remote sensing. Sci. Rep. 2022, 12, 8464. [Google Scholar] [CrossRef] [PubMed]
- Hosseinaee, Z.; Abbasi, N.; Pellegrino, N.; Khalili, L.; Mukhangaliyeva, L.; Haji Reza, P. Functional and structural ophthalmic imaging using noncontact multimodal photoacoustic remote sensing microscopy and optical coherence tomography. Sci. Rep. 2021, 11, 11466. [Google Scholar] [CrossRef]
- Restall, B.S.; Haven, N.J.M.; Kedarisetti, P.; Zemp, R.J. In vivo combined virtual histology and vascular imaging with dual-wavelength photoacoustic remote sensing microscopy. OSA Contin. 2020, 3, 2680–2689. [Google Scholar] [CrossRef]
- Haven, N.J.M.; Bell, K.L.; Kedarisetti, P.; Lewis, J.D.; Zemp, R.J. Ultraviolet photoacoustic remote sensing microscopy. Opt. Lett. 2019, 44, 3586–3589. [Google Scholar] [CrossRef]
- Bell, K.; Mukhangaliyeva, L.; Khalili, L.; Reza, P.H. Hyperspectral Absorption Microscopy Using Photoacoustic Remote Sensing. Opt. Express 2021, 29, 24338. [Google Scholar] [CrossRef]
- Kedarisetti, P.; Haven, N.J.M.; Restall, B.S.; Martell, M.T.; Zemp, R.J. Label-free lipid contrast imaging using non-contact near-infrared photoacoustic remote sensing microscopy. Opt. Lett. 2020, 45, 4559–4562. [Google Scholar] [CrossRef]
- Tweel, J.E.D.; Ecclestone, B.R.; Boktor, M.; Simmons, J.A.T.; Fieguth, P.; Reza, P.H. Virtual Histology with Photon Absorption Remote Sensing using a Cycle-Consistent Generative Adversarial Network with Weakly Registered Pairs. arXiv 2023, arXiv:2306.08583. [Google Scholar]
- Martell, M.T.; Haven, N.J.; Cikaluk, B.D.; Restall, B.S.; McAlister, E.A.; Mittal, R.; Adam, B.A.; Giannakopoulos, N.; Peiris, L.; Silverman, S.; et al. Deep learning-enabled realistic virtual histology with ultraviolet photoacoustic remote sensing microscopy. Nat. Commun. 2023, 14, 5967. [Google Scholar] [CrossRef]
- Pecourt, J.-M.L.; Peon, J.; Kohler, B. DNA Excited-State Dynamics: Ultrafast Internal Conversion and Vibrational Cooling in a Series of Nucleosides. J. Am. Chem. Soc. 2001, 123, 10370–10378. [Google Scholar] [CrossRef] [PubMed]
- Bricker, W.P.; Shenai, P.M.; Ghosh, A.; Liu, Z.; Enriquez, M.G.M.; Lambrev, P.H.; Tan, H.-S.; Lo, C.S.; Tretiak, S.; Fernandez-Alberti, S.; et al. Non-radiative relaxation of photoexcited chlorophylls: Theoretical and experimental study. Sci. Rep. 2015, 5, 13625. [Google Scholar] [CrossRef] [PubMed]
- Soltani, S.; Ojaghi, A.; Robles, F.E. Deep UV dispersion and absorption spectroscopy of biomolecules. Biomed. Opt. Express 2019, 10, 487–499. [Google Scholar] [CrossRef] [PubMed]
- Focke, C.M.; Decker, T.; van Diest, P.J. The reliability of histological grade in breast cancer core needle biopsies depends on biopsy size: A comparative study with subsequent surgical excisions. Histopathology 2016, 69, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Tweel, J.E.D.; Ecclestone, B.R.; Boktor, M.; Dinakaran, D.; Mackey, J.R.; Reza, P.H. Automated Whole Slide Imaging for Label-Free Histology using Photon Absorption Remote Sensing Microscopy. arXiv 2023, arXiv:2304.13736. [Google Scholar]
- Zhu, J.-Y.; Park, T.; Isola, P.; Efros, A.A. Unpaired Image-to-Image Translation using Cycle-Consistent Adversarial Networks. arXiv 2020, arXiv:1703.10593. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Fleiss, J.L. Measuring nominal scale agreement among many raters. Psychol. Bull. 1971, 76, 378–382. [Google Scholar] [CrossRef]
- A Coefficient of Agreement for Nominal Scales—Jacob Cohen. 1960. Available online: https://journals.sagepub.com/doi/10.1177/001316446002000104 (accessed on 1 August 2023).
- Practical Statistics for Medical Research. Available online: https://www.routledge.com/Practical-Statistics-for-Medical-Research/Altman/p/book/9780412276309 (accessed on 1 August 2023).
- R: A Language and Environment for Statistical Computing. Available online: https://www.gbif.org/tool/81287/r-a-language-and-environment-for-statistical-computing (accessed on 1 August 2023).
- Tosta, T.A.A.; de Faria, P.R.; Neves, L.A.; do Nascimento, M.Z. Color normalization of faded H&E-stained histological images using spectral matching. Comput. Biol. Med. 2019, 111, 103344. [Google Scholar] [CrossRef]
- Jackson, S.L.; Frederick, P.D.; Pepe, M.S.; Nelson, H.D.; Weaver, D.L.; Allison, K.H.; Carney, P.A.; Geller, B.M.; Tosteson, A.N.A.; Onega, T.; et al. Diagnostic Reproducibility: What Happens When the Same Pathologist Interprets the Same Breast Biopsy Specimen at Two Points in Time? Ann. Surg. Oncol. 2017, 24, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Calle, C.; Zhong, E.; Hanna, M.G.; Ventura, K.; Friedlander, M.A.; Morrow, M.; Cody, H.; Brogi, E. Changes in the Diagnoses of Breast Core Needle Biopsies on Second Review at a Tertiary Care Center: Implications for Surgical Management. Am. J. Surg. Pathol. 2023, 47, 172–182. [Google Scholar] [CrossRef] [PubMed]
- Polónia, A.; Campelos, S.; Ribeiro, A.; Aymore, I.; Pinto, D.; Biskup-Fruzynska, M.; Veiga, R.S.; Canas-Marques, R.; Aresta, G.; Araújo, T.; et al. Artificial Intelligence Improves the Accuracy in Histologic Classification of Breast Lesions. Am. J. Clin. Pathol. 2021, 155, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Han, D.; Parwani, A.V.; Li, Z. Applications of Artificial Intelligence in Breast Pathology. Arch. Pathol. Lab. Med. 2023, 147, 1003–1013. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| 1. The primary tissue diagnosis is: | |||||||
| Invasive ductal carcinoma | Invasive lobular carcinoma | DCIS | Normal glandular tissue | Image inadequate for diagnosis | |||
| ◯ | ◯ | ◯ | ◯ | ◯ | |||
| 2. DCIS necrotic score: | |||||||
| No in situ disease present | Grade 1 | Grade 2 | Grade 3 | Not assessable | |||
| ◯ | ◯ | ◯ | ◯ | ◯ | |||
| 3. DCIS nuclear grade: | |||||||
| No in situ disease present | Grade 1 | Grade 2 | Grade 3 | Not assessable | |||
| ◯ | ◯ | ◯ | ◯ | ◯ | |||
| 4. Evaluation for invasive disease: | |||||||
| No invasive disease | Score 1 | Score 2 | Score 3 | Not assessable | |||
| Tubule formation | ◯ | ◯ | ◯ | ◯ | ◯ | ||
| Nuclear pleomorphism | ◯ | ◯ | ◯ | ◯ | ◯ | ||
| Mitotic rate | ◯ | ◯ | ◯ | ◯ | ◯ | ||
| 5. Type of image: Is this image from FFPE H&E-stained tissue? | |||||||
| Yes, this is H&E | No, this is not H&E | Uncertain | |||||
| ◯ | ◯ | ◯ | |||||
| H&E Diagnosis | ||||||
|---|---|---|---|---|---|---|
| PARS Diagnosis | IDC | ILC | DCIS | Benign | Image Inadequate | Total |
| IDC | 36 | 0 | 1 | 1 | 0 | 38 |
| ILC | 1 | 1 | 0 | 0 | 0 | 2 |
| DCIS | 1 | 0 | 0 | 0 | 0 | 1 |
| Benign | 0 | 0 | 0 | 7 | 0 | 7 |
| Image Inadequate | 1 | 0 | 0 | 0 | 0 | 1 |
| Total | 39 | 1 | 1 | 8 | 0 | 49 |
| Evaluation Component | Comparison | Kappa Coefficient * |
|---|---|---|
| Invasive Tubule Formation Score | Within H&E | 0.553 |
| Within PARS | 0.300 | |
| H&E–PARS | 0.420 | |
| Invasive Nuclear Pleomorphism Score | Within H&E | 0.051 |
| Within PARS | 0.058 | |
| H&E–PARS | 0.188 | |
| Invasive Mitotic Rate Score | Within H&E | 0.125 |
| Within PARS | 0.148 | |
| H&E–PARS | 0.032 | |
| Nottingham Histological Grade | Within H&E | 0.161 |
| Within PARS | 0.126 | |
| H&E–PARS | 0.073 |
| DCIS Necrotic | DCIS Nuclear | Invasive Tubule Formation | Invasive Nuclear Pleomorphism | Invasive Mitotic Rate | Nottingham Histological Grade * | |
|---|---|---|---|---|---|---|
| H&E | 1 | 7 | 1 | 5 | 15 | 15 |
| PARS | 2 | 4 | 1 | 6 | 14 | 14 |
| Both | 1 | 3 | 0 | 3 | 8 | 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tweel, J.E.D.; Ecclestone, B.R.; Gaouda, H.; Dinakaran, D.; Wallace, M.P.; Bigras, G.; Mackey, J.R.; Reza, P.H. Photon Absorption Remote Sensing Imaging of Breast Needle Core Biopsies Is Diagnostically Equivalent to Gold Standard H&E Histologic Assessment. Curr. Oncol. 2023, 30, 9760-9771. https://doi.org/10.3390/curroncol30110708
Tweel JED, Ecclestone BR, Gaouda H, Dinakaran D, Wallace MP, Bigras G, Mackey JR, Reza PH. Photon Absorption Remote Sensing Imaging of Breast Needle Core Biopsies Is Diagnostically Equivalent to Gold Standard H&E Histologic Assessment. Current Oncology. 2023; 30(11):9760-9771. https://doi.org/10.3390/curroncol30110708
Chicago/Turabian StyleTweel, James E. D., Benjamin R. Ecclestone, Hager Gaouda, Deepak Dinakaran, Michael P. Wallace, Gilbert Bigras, John R. Mackey, and Parsin Haji Reza. 2023. "Photon Absorption Remote Sensing Imaging of Breast Needle Core Biopsies Is Diagnostically Equivalent to Gold Standard H&E Histologic Assessment" Current Oncology 30, no. 11: 9760-9771. https://doi.org/10.3390/curroncol30110708
APA StyleTweel, J. E. D., Ecclestone, B. R., Gaouda, H., Dinakaran, D., Wallace, M. P., Bigras, G., Mackey, J. R., & Reza, P. H. (2023). Photon Absorption Remote Sensing Imaging of Breast Needle Core Biopsies Is Diagnostically Equivalent to Gold Standard H&E Histologic Assessment. Current Oncology, 30(11), 9760-9771. https://doi.org/10.3390/curroncol30110708